
Abstract
Purpose
Implementing Objective Structured Clinical Examinations (OSCEs) as formative educational activities significantly affects postgraduate trainees but could involve challenges to human and financial resources. This study explored senior pediatric residents’ experiences in developing and conducting OSCE stations for their junior peers to elucidate the reciprocal benefits of involving senior residents in this educational partnership.
Design and methods
This qualitative study employed a thematic analysis approach in training senior residents to develop and administer OSCEs following adequate training and supervision. After the OSCE implementation, residents reflected on their experiences. In-depth interviews were conducted using a semi-structured interview guide with the 19 senior pediatric residents who had completed the study. Audio recordings of the interviews were transcribed using a descriptive method, and thematic analysis of the data was performed using NVivo software.
Results
Thematic analysis revealed four interrelated themes: 1) the development of OSCE stations, 2) their conduction, 3) self-reflection, and 4) the Canadian Medical Education Directives for Specialties (CanMEDS) roles. Senior residents described the experience as novel and valuable, significantly enhancing their knowledge, skills, and attitudes. They recognized the benefits of teamwork, teaching skills, and increased confidence across various domains. The activities are aligned with the CanMEDS framework, contributing to their development as medical experts.
Conclusion
This study highlights how and when senior residents empowered as partners in OSCE design can enhance their development and residency programs.
Introduction
The Objective Structured Clinical Examination (OSCE) is a well-known evaluation instrument that doctors use in medical education systems to assess the clinical skills of medical students and residents.1–3 The OSCE started in undergraduate and postgraduate residency programs and medical licensing examinations to evaluate trainee competencies with high reliability and validity. 4 The educational transformation of the OSCE has delivered substantial educational effects that learners value because it enables them to receive constructive feedback about their clinical capabilities. 5 Teaching hospital-administered formative OSCEs improve learner results on summative OSCEs and develop assessment and teaching competencies for students and faculty. 6 Residency training programs should adopt formative OSCEs as a recommendation for curriculum enrichment and feedback delivery to medical residents. 7
Studies have thoroughly documented the high expenses associated with formative OSCEs, particularly in station development, faculty workshop costs, and logistics coordination and implementation expenses. These are standardized patient honoraria, skills lab scores, audiovisual facilities, and personnel time to coordinate and carry out the OSCE tasks. These logistical demands highlight the need for strategic planning and efficient resource use to ensure the sustainability of formative assessments in residency programs.8,9 Cost is a crucial obstacle for many educational institutions, especially those facing budget constraints. 10 The implementation of OSCEs has high costs, which are a significant impediment to many institutions. Besides the logistical and resource-related expenses, a considerable amount of costs is the time faculty spend. Loss of clinical revenue at the institution takes the form of faculty who are involved in the design of clinical cases, checklist writing, and delivery of OSCE, taken out of their clinical duties. Furthermore, the faculty does not receive any additional compensation for these academic activities; it is simply a responsibility inherent in their teaching role. Such a combination of both the lost clinical revenue and the unpaid academic workload highlights the immense financial and operational strain of maintaining OSCEs. The educational value of OSCEs can be preserved through peer teaching (PT) as an alternative system that reduces faculty expenditures and time requirements. 11 Multiple authors combine the definitions of peer teaching with near-peer teachers (NPT) without distinction. 12 The medical education community adopted, from Whitman and Fife, the definition of NPT as an advanced learner compared to other students. 13
Meanwhile, the term PT describes when learners maintain similar academic levels. This educational approach has become a common practice that has enhanced student knowledge and professional growth and strengthened career opportunities for both groups of students.13,14 The peer teaching approach proves effective and secure for building teacher and learner self-confidence and learning experiences in health education settings. 12 Research demonstrates that peer evaluators in OSCEs maintain feasibility and receive positive feedback from participants, primarily when used in NPT programs, because students value high-quality feedback within supportive environments. 15 Senior students who conducted mock OSCE assessments with their junior colleagues produced better confidence development in the learners and better teaching abilities in the instructors. 16 Students’ development of OSCE stations lead to better exam performance, demonstrating their educational worth. 17 This aligns with constructivist theory, which suggests that teaching others deepens one's understanding of concepts. Piaget argued that knowledge is actively constructed through engagement, and students fortify their learning by teaching.18,19 The research data demonstrates Vygotsky's scaffolding theory principle through resident teaching and assessment practices, which promote expertise enhancement and junior resident guidance in an environment built on mutual growth and respect rather than unidirectional usefulness.18,19
However, there is a lack of research assessing peer teaching in developing OSCE stations within medical residency programs, including those in Saudi Arabia. This gap is particularly relevant, given recent updates from the Saudi Commission for Health Specialties (SCFHS), which mandates only one summative OSCE at the end of the final year of pediatric residency training. Therefore, our study explored the experiences of senior pediatric residents in developing and conducting OSCE stations for their junior peers after providing adequate training and supervision to elucidate how senior residents can both enhance their abilities and gain advantages through their involvement in leading OSCE activities.
The setting uses just one OSCE assessment during pediatrician certification, but our team determined that this method provides an insufficient examination of clinical resident abilities. The assessment consists primarily of summative evaluation, although it provides minimal opportunities to offer feedback that helps residents develop their skills. A single OSCE assessment fails to measure the extensive set of abilities needed for autonomous practice in pediatric care scenarios. The educational team identified the requirement for structured extra evaluations because these tests would support resident clinical growth. The primary purpose behind adding more OSCEs was to provide residents with purpose-built opportunities to develop their clinical reasoning abilities and enhance their procedural skills and communication techniques. The added OSCEs functioned as low-stakes learning experiences to build clinical skills, as they offered feedback opportunities, whereas the existing OSCE operated as a summative assessment test. The goal was to increase clinical scenario diversity to guarantee resident competency across essential domains before their final certification assessment.
The study objectives are as follows:
To explore the perceived impact of the OSCE training experience on senior pediatric residents’ preparedness for future OSCEs and their effectiveness in teaching during daily rounds. To examine the feasibility and perceived authenticity of the formative OSCE experience as perceived by senior pediatric residents.
Materials and Methods
Design and Setting
The study employed an exploratory qualitative design and received ethical approval from the Institutional Review Board of King Abdullah International Medical Research Center (Reference No. IRBC/SP22R/227/10). The study was conducted at King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Western Region, Saudi Arabia. This tertiary hospital in Jeddah has 751 beds and hosts various postgraduate programs and subspecialties. The pediatric residency program, approved by the SCFHS, follows a four-year competency-based curriculum aligned with the SCE stations, their implementation, self-reflection, and Canadian Medical Education Directives for Specialties (CanMEDS) framework, outlining the generic competencies expected of pediatricians. 20 Assessments included formative evaluations using work-based assessments, summative evaluations employing multiple-choice questions, and OSCEs after the final residency year, leading to the Saudi Board Credential in Pediatrics award.
Sampling Strategy
At the time of the study, the pediatric residency program had enrolled 56 residents across all four levels: junior (training levels 1 and 2) and senior (training levels 3 and 4). Twenty-six senior residents and 30 junior residents participated in the program. Junior residents received invitations to participate in the OSCE assessment voluntarily, during which they could practice their clinical skills while receiving peer feedback. The program scheduled clinical coverage for participants while they worked within regular hours to maintain uninterrupted services. Written informed consent was obtained from all participants at the beginning of the study. An in-person invitation was made to senior residents (n = 26) during an educational session that was protected from clinical duties, followed by email confirmation. Participation became optional because the program offered neither rewards nor penalties for those who refused to participate. The workshop attendance rate was 76.9%, as 20 out of 26 invited participants attended. Nineteen attendees (73.1% of participants and 95% of workshop finishers) participated in the interviews. The observed participant drop-out rate was attributed to usual scheduling challenges instead of refusal to participate.
The purposive sampling technique was employed to select the participants in relation to their relevance to the research question, but the theoretical sampling of the grounded theory was not utilized.
No formal sample size calculation had been done before the study. The study sample was established according to the feasibility and availability of the pediatric residency program. It is a method that is aligned with the exploratory qualitative research, in which in-depth understanding takes precedence over statistical representability. Nevertheless, the lack of a priori estimation of the sample size is recognized as a methodological weakness.
Intervention
To support senior residents with the necessary skills to develop and conduct OSCE stations with their junior peers, a two-part workshop was conducted over two half-day sessions, one week apart. Two faculty members, both holding master's degrees in medical education and experienced in developing OSCE stations, facilitated sessions with senior residents. They role-modeled the teaching methodology, including OSCE station design, facilitation, and providing effective feedback, while guiding the residents through the process. Over time, the senior residents assumed a greater role in station development and facilitation, fostering a sense of responsibility and ownership, while the faculty gradually transitioned to a supervisory and mentorship role. The workshop taught senior residents about OSCE development while building their competence as future clinicians and educators. We engaged residents through station construction, feedback delivery, and assessment to strengthen their clinical abilities, teaching skills, and understanding of the OSCE format, which aligns with their upcoming summative OSCE assessment and future professional duties. The workshop focused on the key aspects of OSCE station development, implementation, and effective feedback delivery, utilizing the modified Pendleton feedback model known for its educational value. The model is comprehensive yet straightforward, promotes dialog-based, learner-centered discussions, and is easy to replicate. 21 The objectives of the workshop are outlined in Appendices 1 and 2. The sessions were led by two medical educators, HG and MS. During the first half of the academic day, senior residents were divided into four groups, each tasked with developing an OSCE station for specific domains: history taking, physical examination, data interpretation, and patient management or counseling. The blueprint design for station development is linked to six essential pediatric competencies: (1) history-taking, (2) physical examination, (3) data interpretation, (4) management planning, (5) counselling, and (6) procedural skills. The stations matched both the SCFHS curriculum aims and CanMEDS role requirements. Each group selected its subjects from pre-established pediatric curriculum objectives under the guidance of its designated leader to fulfill program requirements. Faculty involvement took the form of oversight of the station development process as well as final reviews of the OSCE cases and checklists to ensure clinical accuracy and relevance to educational objectives and curricular goals. It was through this supervisory role that the faculty shifted the direct case writing role into quality assurance and mentorship functions. The medical educators (HG, MS) evaluated each station for clinical significance, domain coverage, and learning objective compliance. Medical educators (HG, MS) dedicated one week to evaluating and enhancing the stations after the development phase. The second half of the academic day, conducted one week later, was dedicated to providing effective feedback and included a pilot trial of the OSCE stations among senior residents. This session served not only as a rehearsal but also to validate consistency among resident evaluators. Senior residents under the guidance of medical teachers observed the process of feedback delivery and assessment performance to ensure a consistent standard of evaluation and competent performance across the stations. This session enabled senior residents to actively participate in the OSCE process and refine their feedback delivery skills. The medical educators supervised the pilot trial, ensured its proper execution, and offered guidance to the senior residents throughout the process. To illustrate the pedagogical value of resident-driven development of OSCEs, one station created by a senior resident is provided as Supplemental Material 1. This station focuses on the general cardiac evaluation of an 8-week-old infant presenting with difficulty feeding and poor weight gain. It contains organized instructions to the candidates, a moderate script for examiners, and a critical checklist with specific marking criteria. The structured domains found in the checklist are greeting and hygiene, explanation and consent, vital signs, inspection, palpation, auscultation, and interpretation of findings. Every product is marked according to the level of performance, which contributes to a total score of 31. The station was revised by faculty to enhance clinical accuracy and educational relevance.
OSCE Day
In the third week, the OSCE was successfully conducted at the clinical simulation center, and eight junior residents were examined simultaneously. The venue and the time used by the organizing staff were donated by the Clinical Simulation Center of the King Saud bin Abdulaziz University for Health Sciences. This institutional sponsorship enabled the initiation of OSCE activities without incurring any additional financial burden to the residency program. None of the videography services or complex technological arrangements was applied throughout the OSCE. The simulation center provided vital facilities, including high-fidelity mannequins, and did not charge an additional fee for them. OSCE stations were equipped with basic materials used to simulate the actual clinical condition. These involved a chair and a table where the examiner would sit, a couch on which the simulated patient would lie, a high-fidelity manikin that had the heart sounds to use during the physical examination activities, pens, clipboards, marking sheets, instructions of the station, instructions of the simulated patient, and an electronic device that would help maintain the time limitation of the station. These materials were provided by the Clinical Simulation Center and the educational fund of the residency program, ensuring an efficient and educationally sound setup. Moreover, staffing intensity was achieved within the budget of the residency program in education, without incurring any additional personnel costs. This affordable model has been achieved due to institutional backing and strategic time allocations; hence, the program should not be a heavy financial burden. The residents were randomly assigned to various OSCE circuits, with each station structured to allow seven minutes for task completion, followed by three minutes for constructive feedback. An alarm signaled each station's start, the conclusion of the task, and the overall end of the station. Each junior resident enthusiastically participated in four different OSCE stations, enhancing their learning experience. Standardized patients were not utilized in this OSCE scheme. Instead, history-taking and communication with patients were simulated by medical students and interns, whereas a high-fidelity mannequin was placed to demonstrate physical findings (eg, cardiac sounds). The cardiovascular examination station did not need a standardized patient (SP) because it was performed on the high-fidelity manikin. Supplemental File 1 also provides candidate instructions and examiner instructions, as well as a comprehensive checklist, which collectively form the operational guide for this station. The intervention was conducted in October 2022, with 20 senior residents completing all workshop sessions and participating in the OSCE. The participants (senior and junior residents) obtained protected clinical time through program coverage, which was funded by the residency program's educational budget, during OSCE activities to enable their participation. OSCE received a core educational priority through these measures, maintaining its voluntary nature. Following the intervention, the senior residents were invited to engage in interviews, having provided written informed consent voluntarily.
Data Collection
We conducted 1:1 in-depth interviews with 19 senior pediatric residents who developed and conducted OSCE stations for the junior residents. The interviews took place in a quiet office at the hospital, conducted either face-to-face or via Zoom meetings, using a semi-structured interview question guide (Appendix 3). The research guide used open-ended questions with neutral probes to prevent influencing participant responses. The interviewers received training on how to pause after responses and then ask “What else?” to obtain natural, spontaneous answers. The questions were developed based on a literature review and with inputs from several medical educators. The language used for all interviews was English, and audio recordings were maintained with the participants’ permission. A combination of an HG (pediatrician) and a research assistant (RA) who received qualitative training conducted the interviews to reduce power differences between the interviewer and interviewee. The RA conducted 12 out of 19 interviews, while HG interviewed 7 participants. Every interviewer clarified that they occupied a dual position of researcher and learner who needed truthful program feedback to enhance the program. The participants received confirmation that their responses would not influence evaluation results for the training program and that their information would remain anonymous throughout the analysis process. The interview process was explained to the participants, and confidentiality was assured. The interviews were conducted between October 20, 2022, and November 16, 2022, each session lasting 30-40 min. We understood our position as medical educators (HG, SA, AA) and clinicians actively involved in residency training while performing the roles of researchers and program stakeholders. The researchers used two independent authors (SA, AA) to verify coding and thematic analysis while conducting negative case analysis as a bias mitigation strategy. Senior residents involved in our study worked on developing and testing the intervention design by bringing their on-site understanding to the process.
Qualitative Data Analysis
HG transcribed the recordings verbatim after each interview. After the transcription, NVivo (QSR International) version 12 was used to code the data. SA and AA assisted with the data analysis. The data were analyzed thematically, adhering to the six steps of thematic analysis described by Braun and Clarke, 22 to generate themes, as illustrated in Figure 1. The diagram illustrates thematic categories derived from Braun and Clarke's analysis, not grounded theory constructs.

Six Phases of Thematic Analysis, as Described by Braun and Clarke.
Even though the grounded theory has been initially viewed, the completion of analysis followed the thematic analysis framework by Braun and Clarke. As such, the use of grounded theory processes like open coding, axial coding, and theoretical sampling was not utilized. Thematic analysis was selected due to its flexibility and applicability to the recognition of patterns across qualitative data without the necessity to produce an actual theory.
Coding was primarily performed inductively. HG and SA read the text multiple times to familiarize themselves with the data. Codes representing common patterns in the data were organized under candidate themes. The themes were reviewed, and the data were exported to a Word document. Subsequently, the themes were assessed alongside the relevant codes to ensure data consistency before interpretation and report generation.
The study did not carry out any statistical analysis because it had a qualitative thematic methodology, which aimed at inductive coding and the development of interpretive themes.
Results
Nineteen senior residents who completed all study phases (attended half academic days and conducted the OSCE station) were interviewed for this study; we reached saturation after the fifteenth interview and conducted four more interviews to ensure no new data would emerge (Appendix 4: Table A1). We identified four interrelated themes, which we organized under the development of the OSCE station, the conduct of the OSCE station, self-reflection, and CanMEDS roles, as shown in Figure 2.
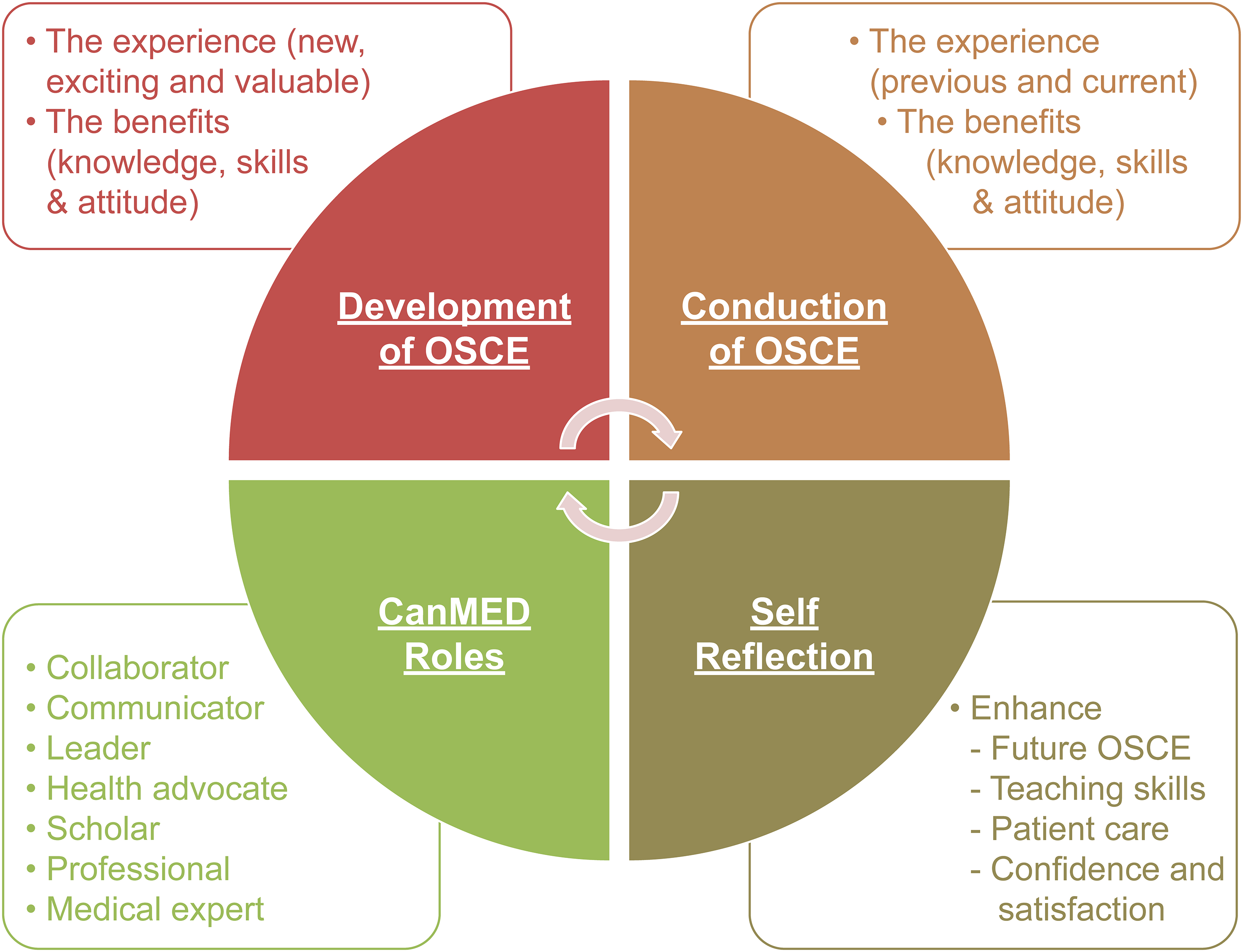
Illustration of the Four Thematic Analysis Diagrams.
Theme 1: Development of the OSCE Station
Experience of Developing an OSCE Station
Developing an OSCE station was a novel experience that elicited excitement and curiosity from all the senior residents. It provided them with a unique opportunity to explore the underlying structure and mechanics of an OSCE station, which piqued their interest. As one senior resident expressed, “It was a new experience for me, and it was interesting to see what is behind the OSCE station” (S2). The team quickly understood that developing the task would prove difficult. Developing an OSCE station required a complete examination of topic selection, learning objective alignment, task suitability, and candidate training standards. The team established a marking scale and designed tasks matching each station's available time slot. The group acknowledged the learning value of their work even though they faced numerous obstacles as they understood the time commitment they made, as expressed by the comment “The development process with my colleagues at the station was enjoyable, and I found it valuable despite the time commitment” (S10).
Benefits of Developing an OSCE Station (Knowledge, Skills, and Attitudes)
Participating in OSCE station development significantly improved senior residents’ understanding of the subject matter. The participants acquired better insights into how OSCE functions as an assessment tool while learning its structure and requirements for clear candidate directions and simplified marking systems. Medical knowledge update and expansion became essential for the residents to become experts in their selected OSCE station topics. The OSCE exam selection rationale and station components became clear to the senior resident (S7). The development process affected their competencies, most notably through teamwork development. Creating multiple pieces of an OSCE station required participants to maintain excellent communication skills together with their ability to manage time alongside mutual respect and teamwork. Residents gained insight into time management efficiency and learned why showing respect toward fellow colleagues during this development period matters. A senior resident explained, “We had to finish the station at a specific time while also ensuring that the station fit within the seven minutes allowed for the performance. That taught us how we needed to manage our time” (S3).
Additionally, they valued the discussions during the station development process, recognizing the role of mutual respect and collaboration. A resident shared, “I appreciate the discussions that happen while developing the station; as seniors, we respect each other” (S2).
Theme 2: Conducting an OSCE
Experience in Conducting an OSCE Station
For many senior residents, this study marked their first comprehensive experience conducting an OSCE. Previous encounters during medical school had been limited and often involved unsupervised practice, with no involvement in station development. Consequently, they were unfamiliar with the key components and overall utility of the OSCE. Participants who developed and conducted the stations under supervision received a more immersive experience. As one senior resident explained, “The previous experience was for practice; the station was already developed, and it was for the medical students to get used to the type of OSCE examination” (S4). The implementation of the OSCE itself received positive feedback from most senior residents, who found the process well-organized and professional. Conducting the OSCE in a setting that closely resembled real-world scenarios enhanced the authenticity of the experience. A resident noted, “The OSCE day was organized and well-structured; it resembled the real OSCE setting” (S6). Moreover, the formative nature of the OSCE contributed to a low-stress environment, allowing senior residents to engage more comfortably with the activities. A resident shared, “Knowing this is a formative OSCE gives us a safe environment to practice without much stress” (S7).
Benefits of Conducting the OSCE Station (Skills and Attitudes)
Engaging in the role of examiner provided senior residents with an opportunity to develop and practice various skills for the first time. Key learning outcomes included objectively assessing candidates and maintaining professionalism during station operation. A resident noted, “Assessing juniors is a skill that requires keen observation, which I had not paid attention to before” (S19). A key aspect of this role was understanding how to provide objective feedback without intimidating candidates. Another resident explained, “I understand the examiner's role now, which is to objectively assess the candidates’ performance using the marking scale, without aiming to intimidate the candidate” (S12). However, some senior residents found it challenging to separate personal relationships and collegiality from the evaluation process, particularly given their familiarity with the junior residents’ performances. A senior resident explained, “It was challenging to take the human factor out of it. As a senior examining my junior colleagues, there is some subjectivity, as I know their performance and believe they could do better” (S13).
Theme 3: Self-Reflection by Senior Residents
Residents’ Performance in Future OSCEs
Observing junior residents’ performance during the OSCE provided senior residents with valuable insights into their future performances. They learned the importance of organization, a systematic approach, task focus, broad differential diagnosis, verbalization of actions, and time management. Witnessing the diverse approaches of junior residents enriched their understanding, allowing them to adopt new skills that would benefit them in future OSCEs. One senior resident noted, “Observing multiple juniors performing differently was a valuable experience. Their organizational abilities and responses to questions allowed me to learn new skills that will benefit me the next time I am a candidate at an OSCE station” (S11).
Moreover, senior residents identified strategies for mitigating stress in future OSCEs. Understanding the different types of stations, being involved in station development, conducting stations, and observing multiple candidates all contributed to their preparation and orientation. One resident shared, “Understanding the different types of OSCE stations will make me less stressed and better able to anticipate what to expect in the exam” (S17). Taking on the assessor role and adhering to the marking scales also helped reduce stress and dispel misconceptions about examiners. A senior resident reflected, “I used to fear the OSCE, thinking the examiner would fail me if they did not like me. Also, when the examiner behaved professionally (not talking or gesturing to me), I thought they were rude and did not like my performance. However, now, I realize that not all is true and is part of being fair and professional to all candidates” (S15).
Teaching Juniors in Daily Work
Participation in this activity enhanced senior residents’ teaching abilities and increased their awareness of their own knowledge and skills. Recognizing areas where improvement was needed, they aimed to support the growth of junior residents by focusing on these deficiencies. A senior resident noted, “Now, I know the level of my juniors’ knowledge and skills; I will try to focus on their deficiencies and dedicate more time to teaching them” (S13). Reflecting on their teaching methods, they emphasized the importance of organized clinical skills, understanding clinical encounters, and stimulating critical thinking. One resident stated, “I must check my juniors’ current knowledge and where they are to build upon that” (S14). They also acknowledged the need to adjust their teaching strategies to match junior residents’ comprehension levels and stimulate independent thinking. One participant explained, “The needs of seniors are different from those of juniors, and I began to consider that” (S9).
Overall, this activity increased their confidence in assisting, teaching, encountering patients, and performing future OSCEs. A senior resident shared, “I will be more confident in assisting juniors, as well as in dealing with patients presenting with the same problem as the station I developed” (S10). In conclusion, senior residents expressed satisfaction with the activity, appreciating its contribution to enhancing their knowledge, skills, and attitudes. This finding highlights the value of using OSCE as an assessment tool for advancing medical education. As one resident noted, “It enhanced my teaching skills; I will use some of the strategies in my daily work, and it will enhance my skills during future summative OSCEs” (S18).
Theme 4: CanMEDS Roles
Senior residents recognized the significance of the activity in enhancing several essential roles outlined in the CanMEDS framework for physicians, which helped develop their capabilities across a range of competencies. In their role as collaborators, they valued the teamwork involved in developing OSCE stations, acknowledging the importance of collaboration in creating meaningful educational experiences for their junior colleagues. A senior resident stated, “I appreciate the collaboration with the OSCE team members to develop the station and how important it is to make this educational session successful for juniors” (S16).
As communicators, senior residents observed patient-doctor interactions during station evaluations, gaining valuable insights into effective communication with patients and families. One senior resident noted, “As my station was for history taking, I was observing the interaction between the candidate (doctor) and the simulator (patient); this gave me insights into how I could better communicate with my patients on regular days” (S12). The activity also provided opportunities for senior residents to exercise their leadership skills. By acting as team leaders, they coordinated station development, delegated tasks, resolved conflicts, and ensured the timely completion of stations. A resident explained, “Developing the station made me play the leader role effectively, as I needed my team to choose the topic, distribute the tasks, and ensure each member of my team was on the same page to finish the OSCE station within the given timeline” (S9).
Moreover, involvement in a counseling station underscored the importance of advocacy and clear communication in patient care, further strengthening their role as health advocates. One senior resident shared, “Teaching parents how to give the inhaler to their child, using clear steps and demonstrations, enhanced this role, and I would spend more time with families in real life to ensure their understanding” (S8). As scholars, senior residents engaged in research and knowledge acquisition to develop station content, demonstrating a commitment to continuous learning. One resident remarked, “I was reading different articles to update my knowledge on the topic of our station because I needed to master the topic before leaving the station's conduct to my junior” (S3).
Finally, the study emphasized adherence to professionalism, reflecting the importance of maintaining high standards and ethical guidelines in medical education. A senior resident stated, “I tried to be professional with my senior colleagues while developing the station and with the juniors while conducting the OSCE station” (S2).
Discussion
The research provides preliminary findings regarding resident feedback about the workshop and its potential impact on OSCE development. Despite its role as an exploratory qualitative study, the research approach does not establish definitive measures of effectiveness. This study highlights the feasibility and acceptance of involving senior pediatric residents in developing and conducting OSCE stations for their junior colleagues. The positive feedback and active participation from senior residents suggest good enthusiasm and engagement with the activity. This finding aligns with previous research on peer-assessed OSCEs in undergraduate medical education.15,22 Our initiative sought to resolve two essential weaknesses: first, the absence of formative OSCEs for skill reinforcement, and second, the underutilization of senior residents for educational roles. Our residency program uses other formative assessments, but they do not include the standardized and multisource feedback aspects present in OSCEs. The OSCE development process, which included senior residents, delivered two important outcomes: it prepared them for summative assessments and established a continuous assessment mechanism for junior residents. Constructivism-based education supports this practice, as teaching others helps learners solidify their skills.18,23
The research method differed by delivering extensive training to senior residents through a series of precisely prepared workshops by knowledgeable medical educators. The training methodology provided systematic education that prepared senior residents to perform their duties in developing OSCE stations and conducting assessments. The training approach improved their knowledge of OSCE methodologies while developing their ability to create stations and evaluate candidates. Evidence shows that thorough preparation enhances the OSCE assessment quality and validity.24,25
The study design featured a distinctive method that allowed participating senior residents take an active role in selecting station topic, empowering and motivating them. Adult learning theory shows that learners typically become more dedicated to their activities when they gain control over their learning process. 26
The involvement of senior residents in topic selection helped them enhance their educational value and deepen their understanding of the subject matter. Senior residents gained valuable benefits through developing and running OSCE stations because this experience served beyond assessment duties to become their professional and personal advancement platforms. The design and evaluation of OSCE stations enabled senior residents to develop their assessment abilities while learning practical feedback approaches and improving their medical teaching skills and knowledge retention. The observed outcomes match research results, which demonstrate that peer teaching and peer assessment activities substantially improve teaching abilities and clinical skill evaluation.27,28
Our study revealed that senior residents rapidly enhanced their confidence regarding patient care and assessment abilities, teaching competence, and ability to perform well in upcoming OSCE examinations. Residents demonstrated significant confidence growth for multiple reasons. By participating in the development process of the OSCE, residents acquired exposure to diverse clinical scenarios that developed their diagnostic and decision-making capabilities. Through multiple OSCE station exposures, participants mastered both the testing format and learned to use theoretical knowledge within strict time frames, which will benefit their upcoming clinical practice. Additionally, the act of teaching junior residents, coupled with the responsibility of evaluating their skills, reinforced their self-efficacy and validated their expertise. This aligns with research by Ytterberg et al and Burgess et al, who found that teaching activities significantly boost confidence, particularly in complex, high-stakes environments like OSCE.29,30
Notably, the increase in confidence among senior residents was not confined to only the technical aspects of OSCE; it extended to their broader professional identity as clinicians and educators. By taking on leadership roles in the educational process, senior residents gained a sense of empowerment that positively influenced their self-perception as educators and clinicians. The organizers designed this activity to advance the clinical abilities of senior residents. The stations used curricular guidelines to assist residents in reviewing pediatric competencies while building their professional expertise. Junior assessment required evaluative competencies matching those needed for their future summative OSCE examination, thus helping them feel more comfortable with the process. Burgess et al's research verifies this discovery by finding that peer assessment improves residents’ self-confidence and prepares them better for examinations. 29 The progressive change in self-confidence is a fundamental factor in developing their competence as future independent practitioners and medical educators, so they can transition from residency to specialist status. Their ability to offer appropriate feedback grew through their experience with peer assessment because they learned to think critically and empathize while assessing their peers. This skill serves both professional growth and lifelong learning. The study demonstrates how medical education works through an interdependent process between teaching and learning because junior residents learn better from teaching activities while senior residents experience professional growth. Medical professionals sustain professional growth using a self-assessment cycle, which extends advantages to each practitioner and their medical colleagues.
The OSCE activity benefited from being linked to the CanMEDS framework, which helped residents develop essential competencies. The experience contributed to their professional growth across multiple domains, including collaboration, communication, leadership, advocacy, scholarship, and professionalism, which are central to developing well-rounded medical professionals. 31
Despite the numerous benefits, the development and implementation of OSCEs can incur substantial costs and require significant staffing resources. Although scale comes into consideration regarding cost, no formal calculations of cost were performed in this study. Future versions would be improved by integrating a financial evaluation to enable wider usage. However, involving senior residents under appropriate supervision could help mitigate these challenges while maintaining the quality of the educational experience.28,32,33 The residents surveyed demonstrated a willingness to sustain co-design activities for OSCEs (12/19) yet demanded structured time management systems. A proposed scheduling concept merged station creation activities with academic half-day sessions to decrease non-curricular obligations. By decentralizing the responsibility for station development and execution, residency programs may foster peer-led initiatives that reduce logistical burdens and enhance the educational experience for senior and junior residents.
Strengths and Limitations
This study makes a valuable contribution to the growing body of literature on peer teaching in medical education, particularly within the context of residency training programs. While much of the existing research has focused on undergraduate medical education, our study stands out as one of the few to explore peer teaching at the postgraduate level, specifically within pediatric residency programs in Saudi Arabia. This context is significant, as it expands the understanding of how senior residents could contribute to and benefit from peer-led educational activities in a clinical training environment. A significant strength of our study is its focus on the importance of comprehensive training for senior residents. The study demonstrates that with proper preparation, senior pediatric residents can not only participate in but also lead and design OSCE stations, an area that has been underexplored in previous literature. This highlights the untapped potential of senior residents as both educators and learners, offering valuable insights into how structured peer teaching could enhance their clinical skills while benefiting junior residents.
However, there are certain limitations to consider. One key limitation is the relatively small sample size. Also, the formal sample size computation was not performed before the research. The sample size was determined by the possibility and presence of the participants in the residency program. Although this method is typical of the exploratory research of a qualitative nature, it can reduce the statistical strength and generalizability of the results. The sample size estimates should be included in future studies to increase the methodological rigor. While the responses from participants were rich and revealed consistent themes, a larger sample size would enhance the generalizability of the findings and provide a more diverse range of perspectives. Additionally, while this study presents qualitative data on senior residents’ experiences, it lacks objective measures to assess how participation in the OSCE activity directly influenced their performance in subsequent OSCEs. Including such objective data would provide a clearer understanding of the activity's efficacy, as demonstrated in previous studies. 17 Future research should consider integrating quantitative assessments to evaluate the long-term impact of the OSCE experience on residents’ clinical skills and subsequent performance in OSCEs.
Another limitation is the lack of data on the perceptions of junior residents regarding the feedback they received and their experiences with the OSCE. While this study focused on the experiences of senior residents, understanding how junior residents perceive both the feedback process and the impact of peer-assessed OSCEs on their learning would provide important insights into the effectiveness of the peer teaching model. Implementing power dynamic reduction methods (mixed interviewers and anonymization) did not eliminate social desirability bias because participants interacted with researchers connected to the program. Future research should use interviewers from outside the program to decrease potential bias effects. Future research will investigate junior residents’ evaluation of the OSCE's value. However, their spontaneous commitment to the assessment and allocated time demonstrates their view of this activity as professionally applicable. The absence of official rewards seems to have affected the extent to which junior residents participated. This aspect of the study will be addressed in future publications. However, it remains a critical factor for a more comprehensive evaluation of the peer teaching approach and its influence on both junior and senior residents’ learning outcomes.
Conclusions
This qualitative investigation revealed multiple benefits that result from using senior pediatric residents to create formative OSCEs for their junior colleagues. It demonstrates that appropriately trained senior residents can create valuable assessments and simultaneously improve their professional abilities through protected work time. The thematic evaluation showed that residents developed expertise in (1) OSCE station design (2) assessment methods and feedback techniques, (3) reflective teaching methodology, and (4) improved CanMEDS scholar, leadership, and communication competencies. The successful outcomes stemmed from how the intervention uses adult learning principles and social constructivist theory together. Residents’ active selection and design work regarding clinical scenarios produced a genuine sense of ownership in the learning process, as observed in participant comments such as “Development of the station helped us review essential foundations we had missed” (S4). The teaching practice follows Whitman's near-peer approach, allowing experienced learners to teach new knowledge through mentoring students. The 73% voluntary participation rate, or 19 out of 26 eligible senior residents, along with the dedication of 3.5hours of preparation time, indicates their strong intrinsic motivation as educational partners instead of passive students.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251393853 - Supplemental material for Empowering Tomorrow's Trainers: Engaging Senior Pediatric Residents as Co-Developers of OSCEs for Junior Peers
Supplemental material, sj-docx-1-mde-10.1177_23821205251393853 for Empowering Tomorrow's Trainers: Engaging Senior Pediatric Residents as Co-Developers of OSCEs for Junior Peers by Hasan Ghandourah, Sami Al-Nasser and Abdullah Alzahem in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251393853 - Supplemental material for Empowering Tomorrow's Trainers: Engaging Senior Pediatric Residents as Co-Developers of OSCEs for Junior Peers
Supplemental material, sj-docx-2-mde-10.1177_23821205251393853 for Empowering Tomorrow's Trainers: Engaging Senior Pediatric Residents as Co-Developers of OSCEs for Junior Peers by Hasan Ghandourah, Sami Al-Nasser and Abdullah Alzahem in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors thank all pediatric residents of the 2022–2023 batch at MNGHA-Jeddah for their participation in this study. We are grateful to Dr Mesbah Al-Shamrani (MS) for teaching the senior residents; Dr Sami Al Thubaiti (Assistant Dean, Clinical Simulation Center, King Saud Bin Abdul-Aziz University College of Medicine, Jeddah) for providing access to the clinical simulation center; and Dr Shada Shesha, Pediatric Program Director, for her involvement in the residents’ educational activities. We also thank Editage (![]() ) for English language editing and journal submission support. The authors have authorized the submission of this manuscript through Editage.
) for English language editing and journal submission support. The authors have authorized the submission of this manuscript through Editage.
Ethical Considerations
The study employed an exploratory qualitative design and received ethical approval from the Institutional Review Board of King Abdullah International Medical Research Center (Reference No. IRBC/SP22R/227/10).
Consent to Participate
The participants provided their written informed consent to participate in this study.
Consent for Publication
Not applicable.
Author Contributions
HG: Conducted the interviews, recorded the interviews, recorded the transcript thematic analysis, and wrote the manuscript. SA and AA: reviewed the transcription, thematic analysis, and manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix 1
Appendix 2
Appendix 3
Appendix 4
Participants’ Characteristics.

| Characteristics | Number | Percentage (%) |
|---|---|---|
| Gender | ||
| Male | 13 | 68.4 |
| Female | 6 | 31.5 |
| Level* | ||
| R3 | 10 | 52.6 |
| R4 | 9 | 47.3 |
| Total number of Seniors | 19 | 100 |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.