
Abstract
OBJECTIVES
Pediatric residency trainees interface with electrocardiograms (EKG) as part of routine clinical care. Depending on workflow and availability of support staff, trainees may be required to obtain EKGs on patients, though training on this skill varies. Our intervention seeks to train incoming pediatric residents on obtaining EKGs from pediatric patients and identifying common problems that may result in acquisition of low-fidelity EKGs.
METHODS
A team of physicians, EKG technicians, and simulation educators designed a 30-min didactic and experiential learning opportunity for incoming pediatric trainees held prior to their start of clinical responsibilities. During the session, trainees were introduced to the basics of EKG acquisition and common quality issues that arise. Afterwards, they practiced placing EKG leads on a mannequin and a live model. A pre- and post-session survey was utilized to assess the session's utility and participant's learning.
RESULTS
The intervention was perceived as a valuable experience by participants over the course of 2 years. We found increased participant comfort with performing and troubleshooting EKGs (P<.001). There was a 33% improvement in quality assessment of EKG rhythm strips after the session (P<.001).
CONCLUSION
Given the importance of EKGs to the care of pediatric patients, it is essential that pediatricians receive adequate training in acquiring and assessing EKG quality. This intervention was deemed to be highly useful with a demonstrated improvement in EKG troubleshooting skills among first year pediatric residents. This session improves learner comfort with essential clinical responsibilities and identification of low-quality EKGs that often warrant repeat testing.
Introduction
General pediatric residents are often required to interpret electrocardiograms (EKG) as part of a diagnostic workup in the evaluation and management of cardiovascular diseases. However, pediatric physicians often lack the necessary competency to accurately interpret EKG results. 1 While some trainees enter residency with EKG interpretation and acquisition experience, their comfort and skill level varies based on their prior medical school curriculum and clinical training. To establish a common skillset among a group of first year pediatric trainees at a large quaternary training center, our residency program developed a formal, longitudinal EKG acquisition and interpretation curriculum that spans across 3 years of general pediatric residency training. This educational summary report describes the acquisition portion of the curriculum that focuses on the skills required to perform an EKG and troubleshoot common issues.
Existing literature has described the gaps in knowledge of EKG interpretation across pediatric trainees of all levels from medical students to attending cardiologists.2-4 Deficiencies in EKG interpretation are amplified when physicians are interpreting poor quality EKGs, and one study in a pediatric emergency department found that of all the EKGs obtained, 14% were found to be performed incorrectly. 5 Poor quality EKGs may limit diagnostic utility, influence a provider's interpretation and clinical decision making, and lead to unnecessary consultations and repeat studies; therefore, it is imperative that trainees feel comfortable obtaining high-fidelity EKGs on pediatric patients and troubleshooting common acquisition mistakes. Due to the variable availability of care team members who are trained in obtaining high-fidelity EKGs across different care settings, resident physicians may be expected to acquire EKGs overnight, on weekends, or in urgent clinical scenarios. However, as formal training in EKG acquisition may be lacking, the quality of these EKGs is variable.
To address the need for improved EKG training in pediatric resident physicians, several studies have examined the effectiveness of various training interventions. A recent study by Smith et al. found that a simulated training program significantly improved the EKG interpretation skills of pediatric residents. 6 Another meta-analysis demonstrated that experiential learning methods are more effective at improving learning outcomes than didactic learning alone. 7 We sought to optimize EKG acquisition skills by combining experiential learning with didactics to mitigate the potential for acquisition of low-fidelity EKGs. While educational interventions have shown improvement in first-year pediatric residents’ abilities to correctly diagnose EKG findings, 8 no interventions have focused on residents’ acquisition in obtaining high quality EKGs. Our curriculum seeks to train each first-year resident in basic EKG acquisition skills that may be utilized when other staff members are unavailable. This curriculum consists of an in-person didactic lecture, hands-on workshop, and pre- and post-session testing via e-mailed survey. We implemented the curriculum as a 30-min session held during new intern orientation prior to the residents starting their clinical responsibilities as part of a quality improvement project.
Methods
Place and nature
Our intervention consisted of a 30-min, in-person educational didactic session followed by hands-on practice for all interns during their 2-week orientation prior to starting their residency training. This session occurred prior to any trainee having clinical time in the hospital or in outpatient clinic settings. All materials were developed and reviewed prior to the session by a chief year resident, second year resident, cardiology attending, EKG technician, and simulation educator. Exposure to the basic concepts of EKG interpretation during medical school is widespread; however, the curriculum was developed with the assumption that learners may have had no experience placing leads on a patient and obtaining an EKG with the use of an EKG machine. We did not ask learners to do prework prior to our session. We utilized the GE MAC 5550 EKG machines available at our institution, but we did not tailor the lecture portion of the session towards this specific EKG machine, as with the goal to teach general principles without reliance on utilizing any specific manufacturer's device. With regards to acquisition quality, based on clinical experience of the development team, we focused on 3 common pitfalls leading to suboptimal EKG quality: movement artifact, poor lead contact, and upper limb lead reversal. We were able to offer this session with a cohort of incoming interns in 2021 and repeated it in the subsequent year of incoming interns in 2022 with full participation across both classes. This was intended to be a quality improvement project, and it did not warrant ethics approval as it fell within our institution's published guidelines as to what encompasses a quality improvement project. All participants provided written informed consent that their involvement and responses to the surveys would be analyzed, shared, and utilized to improve future sessions.
Equipment/environment
The 30-min session was part of a larger clinical skills day that the residents participated in; however, the curriculum was developed to function as a standalone experience. All participants were emailed a link to a pre-survey that they were asked to complete prior to the session. The survey included questions on training background, self-reported comfort with various EKG acquisition skills, and sample rhythm strips. During the session, a lecture was given to introduce the trainees to the basics of the EKG machines (Appendix A and Appendix B). This didactic portion had a PowerPoint accompaniment that outlined how to order an EKG, place EKG leads on a patient, and examples of the 3 most common acquisition issues: motion artifact, poor lead contact/missing leads, and upper limb lead reversal (Appendix B). Rhythm strips of these findings, along with an example of a high-fidelity normal sinus rhythm EKG, were included on the pre- and post-surveys (Appendix C and Appendix D).
In addition to requiring a projector for the PowerPoint, our session required additional supplies, provided by our hospital's simulation team and the EKG technician team. We had 2 functional EKG machines, EKG stickers, scissors, an infant sized mannequin, and an adolescent sized mannequin for the hands-on portion of the session. We conducted the sessions in a conference room with a functional projector, tables set up on one side for lead placement practice, and a table on the other side for troubleshooting practice using a live model. EKG machines were placed at the end of the table with the mannequins nearby for ease of EKG lead placement.
Personnel
A senior resident, chief resident, or EKG technician was responsible for leading the session. The session was led by a chief resident and EKG technician the first year, and a senior resident and EKG technician the following year. Each leader was given all the didactic materials ahead of the session and arrived early to set up the EKG machine and mannequins prior to the session. Additionally, we had an adult volunteer who agreed to be a live model to practice placing leads on and obtaining EKGs. The volunteer was instructed to sit with their chest appropriately exposed for EKG sticker lead placement. Once leads were placed during the session, the volunteer was asked to either stay still or move in accordance with demonstrating various EKG acquisition issues that may arise within a real patient encounter.
Implementation
All materials were set up prior to the didactic session and the PowerPoint (Appendix B) was displayed on a projector. Once the trainees arrived, brief introductions and goals of the educational session were discussed. After ensuring that all participants had a chance to complete the pre-survey, the presenter oriented the trainees to the EKG machines and went through the PowerPoint for the didactic portion. During this presentation, participants were familiarized with the EKG machine, principles of EKG lead placement, and how to order an EKG using the institution's electronic medical record system. Afterwards, the instructor demonstrated how to operate the EKG machine, cut stickers to appropriate patient size, and place stickers on a mannequin. The trainees then split into 2 groups and had an opportunity to practice placing stickers on each pediatric sized mannequin. The instructor helped guide placement and answered any questions that came up.
After all parties practiced placing EKG leads on a mannequin, the instructor focused the participants’ attention on the volunteer and demonstrated how to obtain a high-fidelity EKG in real time. The first year, these occurred in parallel due to extra support staff; however, these occurred in sequence the following year. Afterwards, the common acquisition issues (poor lead contact/missing leads, motion artifact, and limb lead reversal) were simulated while an EKG rhythm strip printed to demonstrate the findings. Finally, the instructor demonstrated how to correct these issues. Final questions were answered, and all participants were thanked for their engagement.
Debriefing/assessment
After the hands-on portion of the session, trainees were encouraged to practice placing EKG leads on the mannequins and each other. Questions were fielded as they arose, and each participant was asked to fill out the post-survey later that evening when it was emailed to them. All participants were informed that surveys were de-identified, optional, and could be published and analyzed for the purpose of improving future sessions.
Data
Both groups of participants (year 1 and year 2) were provided with the same pre- and post-session survey (Appendix C and Appendix D). The survey assessed respondents’ comfort with performing EKGs and troubleshooting EKGs before and after the session on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). 9 It also asked whether the sessions were deemed to be valuable or recommended for future trainees with the same Likert scale. Finally, each survey had 4 EKG rhythm strips for interpretation depicting either: normal sinus rhythm, baseline artifact, poor lead contact/missing lead, or limb lead reversal. Participants were asked if each rhythm strip was a high-quality EKG, and if not, they were then asked to free-text the problem with the EKG. The rhythm strips were the same on both surveys, but they were presented in a different sequence. Each participant would be given a point for correctly identifying whether the rhythm was high quality or not, and an additional point for correctly describing the problem with each of the 3 poor quality rhythms. The total maximum score was 7 for the pre- and post-survey.
Statistical analysis
We performed a paired t-test of the mean Likert scale responses of participant comfort performing EKGs, participant comfort troubleshooting common EKG issues, and total correct score on EKG rhythm analysis. All statistical analyses were performed with Stata 17 (College, Texas).
Results
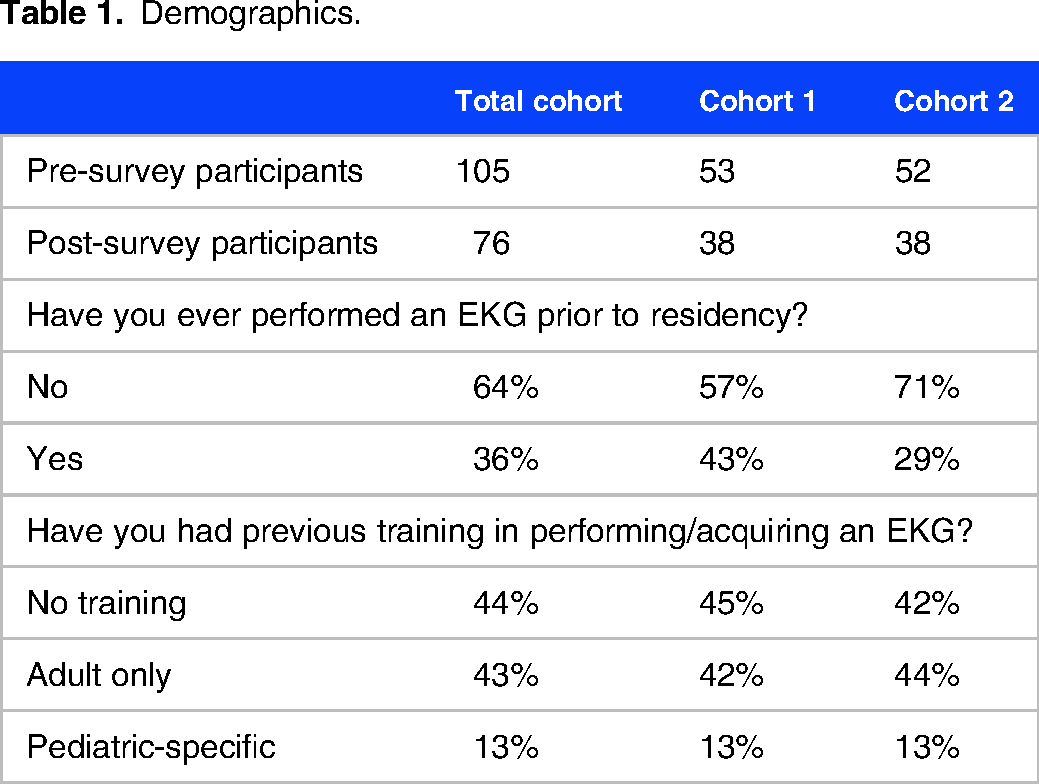
Over the 2 years, we had a total of 105 residents participate in the session and complete the pre-session survey. All participants completed the pre-session survey. Only 76 participants completed the post-session survey, of which 38 residents in each year responded to both surveys (Table 1). 36% of the all residents participating in the session had experience obtaining an EKG prior to this session. 44% had no prior formal training in acquiring EKG, 43% had prior training on EKG acquisition in adult patients, and 13% had prior training on EKG acquisition specific to pediatric patients.
Demographics.
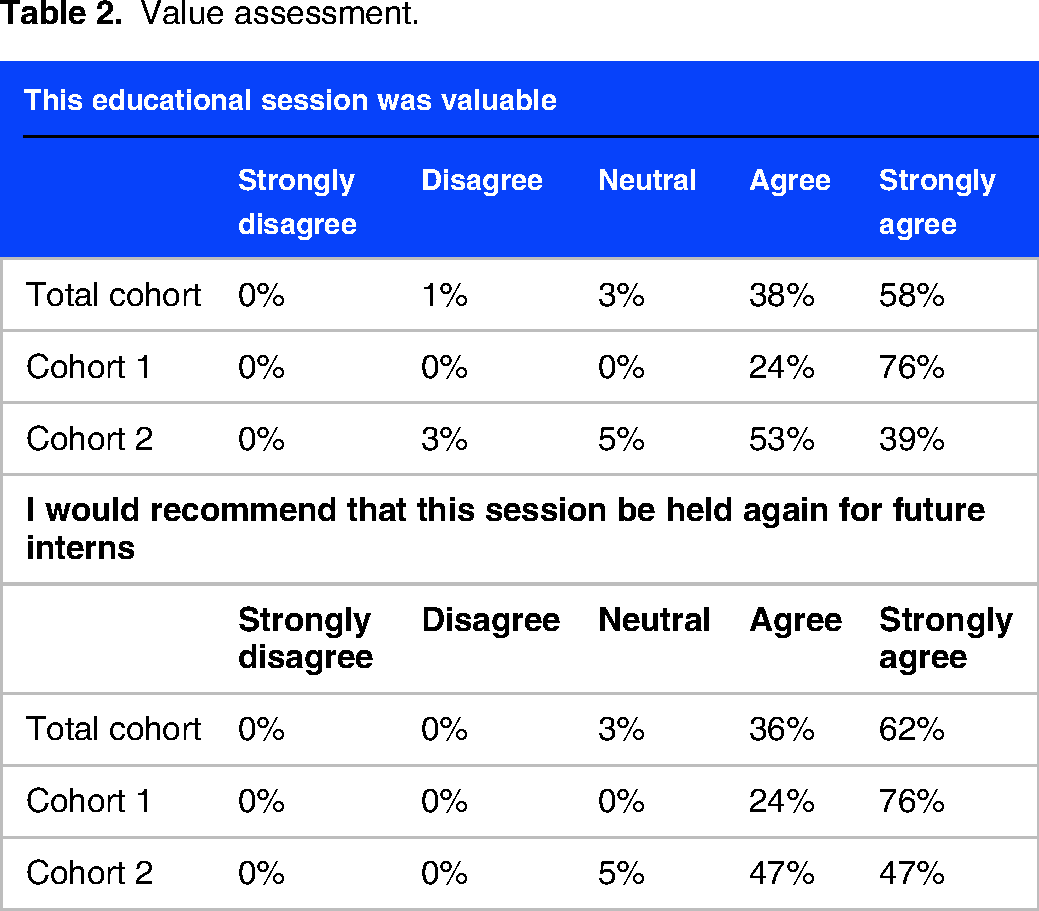
The majority of participants “disagreed” (53%) or “strongly disagreed” (19%) that they felt comfortable performing EKGs prior to the session (Figure 1). After the session, 62% “agreed” with that statement (Likert scale average of 2.13 pre-session and 3.92 post-session, P<.001). A similar trend was seen with participant comfort troubleshooting common EKG problems (Likert scale average of 1.63 pre-session and 3.85 post-session, P<.001) (Figure 2). When asked about utility of the orientation session, 96% of participants “agreed” or “strongly agreed” that the educational session was valuable and 97% “agreed” or “strongly agreed” that they would recommend the session to be held again for future (Table 2). In response to the optional descriptive question of “What was helpful about this session?” in the post-survey, many participants cited “hands-on experience placing leads on the mannequins/volunteer” and “explanation of how to turn on the EKG machine.” In response to the optional descriptive question of “What could be improved?” in the post-survey, participants requested having more than 2 EKG machines available.

Self reported comfort performing ECGs before and after the session.

Self reported comfort troubleshooting ECGs before and after the session.
Value assessment.
The results of EKG rhythm strip quality assessments are presented for the total cohort in Table 3. There was a statistically significant improvement in correct identification of all 3 EKG acquisition problems on the post-session survey. When the cohorts are analyzed separately, the same trends persist for the second year cohort for the same 3 problems; however, there was no significant change in correct identification of poor lead contact in the first year cohort. Of note, there was a decrease in correct identification of the other 3 EKG issues, with a significant decrease in identification of baseline artifact and limb lead reversal (Table 3). When comparing means between those who had prior teaching or experience compared to those that did not have any prior teaching or experience, there were no statistically significant differences in total pre-survey scores. There was also no difference among groups in their correct identification of high quality EKGs, upper limb lead reversal, baseline artifact, or poor contact one the pre- or post-survey. The only statistically significant difference was within the total post-survey scores, with those who had prior teaching scoring higher overall (“Yes teaching” 5.9/7 compared to “No teaching” 5.3/7, P = .04). Finally, the total average mean of correct identification and quality assessment increased by 33% from 4.2/7 to 5.6/7 (P < .001).
Interpretation analysis.

Discussion
Our EKG acquisition curriculum seeks to provide resident trainees a formal training on how to obtain EKG rhythm strips on pediatric patients of all ages and sizes. An interprofessional team convened to design a curriculum that can be taught within a 30-min period to multiple providers at once and combines a didactic portion with a hands-on experiential learning opportunity. It allows for direct interaction between the teacher and the learner in a safe environment separate from patient care.
The limitations of our project include need for EKG machines and mannequins to be available for the session, which may not be possible at all institutions. Furthermore, our teaching was based on the EKG machine models in our facility and may not be applicable to older or newer models. An additional limitation may be that this curriculum is early in the residency training and there may be some time before individuals apply it to clinical practice based on their rotation schedule. Although our curriculum focused on identifying motion artifact, missing leads, and limb lead reversal, there are other EKG acquisition issues that our project did not focus on, such as precordial lead reversal, and all learners should be made aware of these when continuing to hone their skills. Furthermore, our learners were only educated on upper limb lead reversal and the results do not indicate improvement in ability to identify lower limb reversal. There was no power analysis performed, as this was a pilot curriculum and the sample size equated to the total number of participating residents. Finally, due to the voluntary nature of the survey, favorable reception of the session and improvement in identification of EKG acquisition issues may be partly secondary to a selection bias in those who chose to respond to the post-survey.
To better ascertain retention of knowledge, a follow-up survey at a later date could be obtained. Despite these limitations, we designed and implemented a brief and effective curricular intervention to train pediatric resident physicians in EKG acquisition. With the broad applicability of EKG acquisition skills, this curriculum may benefit a wide audience of medical professionals to enhance patient care in settings requiring in-time acquisition of high-quality EKGs.
Conclusion
Our results demonstrate that low confidence in acquisition skills and inconsistent ability in assessing EKG quality were common among residents. As residents are expected to acquire EKGs overnight and on weekends with overall low levels of comfort, formal early training to decrease cognitive load and improve clinical care delivery further advocates for formalized EKG acquisition training. Our survey found that this curriculum was overwhelmingly valuable and popular among our cohort across 2 years. It also found that the general trends of EKG troubleshooting skills before and after the session were similar across the 2 cohorts in our program despite having different instructors each year. Overall comfort with obtaining an EKG improved after the session, and trainees showed improvement in appropriate identification of high-fidelity EKGs while recognizing common EKG acquisition problems quality interpretation after the intervention.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231204758 - Supplemental material for EKG Acquisition Curriculum for Pediatric Trainees
Supplemental material, sj-docx-1-mde-10.1177_23821205231204758 for EKG Acquisition Curriculum for Pediatric Trainees by Vladislav Obsekov, Christopher Teng and Dorene F Balmer in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pptx-2-mde-10.1177_23821205231204758 - Supplemental material for EKG Acquisition Curriculum for Pediatric Trainees
Supplemental material, sj-pptx-2-mde-10.1177_23821205231204758 for EKG Acquisition Curriculum for Pediatric Trainees by Vladislav Obsekov, Christopher Teng and Dorene F Balmer in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205231204758 - Supplemental material for EKG Acquisition Curriculum for Pediatric Trainees
Supplemental material, sj-docx-3-mde-10.1177_23821205231204758 for EKG Acquisition Curriculum for Pediatric Trainees by Vladislav Obsekov, Christopher Teng and Dorene F Balmer in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205231204758 - Supplemental material for EKG Acquisition Curriculum for Pediatric Trainees
Supplemental material, sj-docx-4-mde-10.1177_23821205231204758 for EKG Acquisition Curriculum for Pediatric Trainees by Vladislav Obsekov, Christopher Teng and Dorene F Balmer in Journal of Medical Education and Curricular Development
Footnotes
Author contributions
Vladislav Obsekov: drafted and revised the manuscript, conducted data analysis, assisted with planning the sessions both years. Christopher Teng: revised the manuscript and organized the first year's session. Dorene Balmer: revised the manuscript and provided guidance for planning the curriculum.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.