
Abstract
Objective
We describe a novel evaluation of attitudes toward engagement with a required medical school course from the perspective of the participating community organizations. We then consider lessons learned about sustained community engagement from this longstanding community–academic partnership and potential implications for public health and research partnerships. The aim of this observational study is to assess facilitators of community engagement to improve engagement with community organizations.
Methods
Data collection consisted of end-of-course evaluations collected from community mentors of the student teams. Surveys were completed at the end of each course and they used a common set of questions across cohorts. Data from the Class of 2019 through the Class of 2026 were analyzed using a qualitative framework and descriptive statistics.
Results
One hundred mentors completed surveys across 7 years of measurement. The most frequently cited reasons for participating are interest in influencing the training of health professionals, needing additional help, and wanting a relationship with the university. Community organizations agreed or strongly agreed that the community/people served benefitted from projects and that the relationships will continue. Organizations reported a wide variety of benefits, and current and planned uses for project findings, ranging from internal program evaluation and planning to external outreach, education, and advocacy.
Conclusions
Facilitators and drivers of successful partnerships are essential for project success and sustained community engagement. Our data and experience suggest that documented community benefit is essential for long-term engagement, adding to the current literature for community engagement in medical education and research.
Introduction
Numerous articles highlight community engagement in medical education as an essential educational strategy to respond to community health and social priorities.1-8
Such educational approaches also align with strategies to engage communities in research and improve population health.9-12 Recent references identify strategies to enhance partnerships in education and research.1,9,12 However, substantial gaps remain, including a need for intentional focus on the community perspective in developing sustained community–academic partnerships.3,8 We describe a novel evaluation of attitudes toward professional education with a required medical school course from the perspective of the participating community organizations, suggesting implications for public health and research partnerships. The aim of this study is to assess facilitators of community engagement to improve how our medical school engages with community organizations.
Methods
Public Health Projects is a required medical school course in which community organizations submit proposals for projects, and students respond to identified health needs in a structured and mentored semester-long framework. We have previously described project methods and community benefits.5,6 Additionally, prior to the start of the course, students participate in an orientation session, match to a topic area (eg, social determinants of health, health policy, and advocacy) and community agency, have their first meeting as a group, and complete e-learning modules on key aspects of research ethics and best practices, literature searching, and basic qualitative and quantitative methods. At the start of the course and with the guidance of the community and faculty mentors, the teams develop a public health project question and identify appropriate methods, including quality improvement, program evaluation, and/or public health practice. Teams must collect some form of data to address the project question, which typically is related to a community-identified need. Projects culminate with a poster session attended by community partners and faculty, with many teams going on to present their work at national public health meetings.
This partnership began in 2004, reflecting a hub and spoke model, with the United Way of Northwest Vermont, serving as the hub and the spokes referring to approximately 150 community nonprofit organizations, the source of the projects. Sixteen annual projects include a mix of prior partners and new organizations, varying according to community-identified needs, framed in the national Healthy People categories. Our previous reports describe this process5,6 and UVM ScholarWorks serves as a repository for project abstracts and posters. 13 This project was reviewed by the University of Vermont Institutional Review Board (IRB), and it was determined that the study was exempt from review under Exemption Category 1 Educational Research 45 CFR 46.104(d)(1).
In this multimethods study, we utilized historical de-identified data from community mentor assessments of student group process and project quality. Community feedback about student group performance, engagement, reasons for participation, and project uses were gathered in electronic surveys.
Data collection consisted of end-of-course evaluations collected from community mentors of the student teams. Surveys were completed at the end of each course and they used a common set of questions across cohorts. All available mentor data from the Class of 2019 through the Class of 2026 were analyzed using a qualitative framework and descriptive statistics. Data was not available for the Class of 2023, as in-person community projects were briefly suspended during the COVID-19 pandemic. A thematic coding approach was applied to mentors’ narrative responses.
Qualitative data analysis used a published framework.14,15 Responses were independently coded by the authors and following coding reconciliation, common themes were identified. This study conforms with the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for observational studies. 16
Results
One hundred community mentors (89% of the total) completed surveys across 7 years of measurement. The most frequently cited reasons for participating are presented in Figure 1.
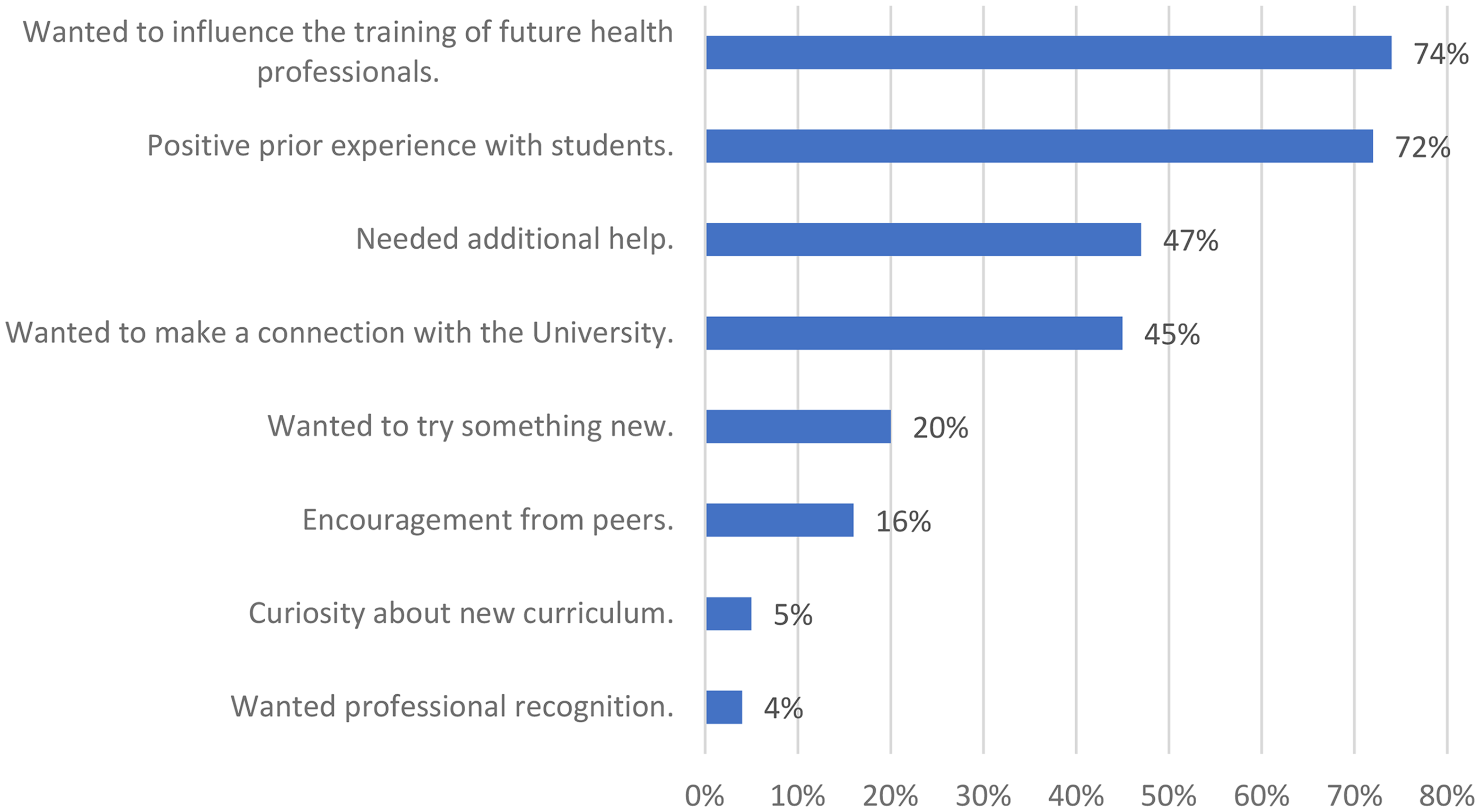
Reasons for Community Organization's Participation.
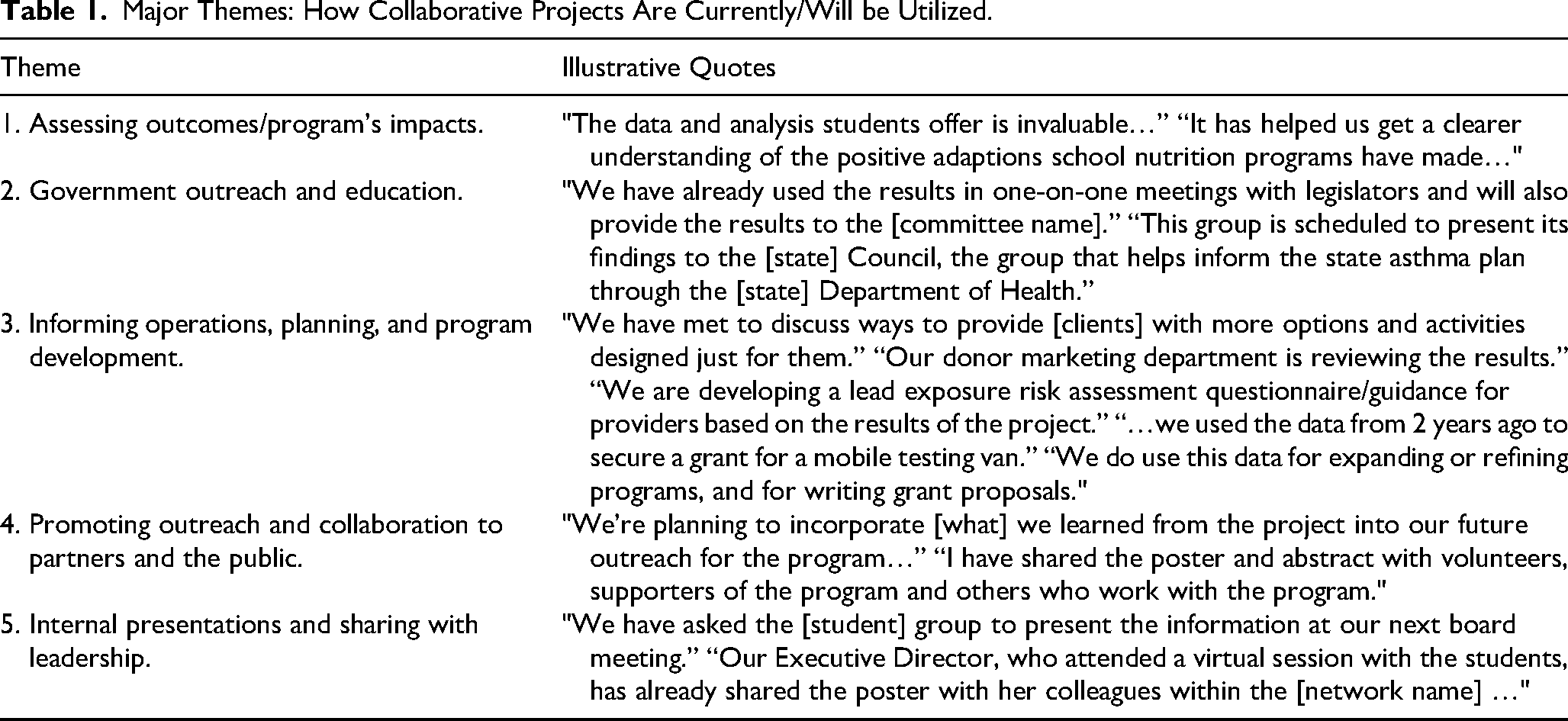
Additionally, using a 4-point Likert-like scale for agreement (4 = strongly agree, 1 = strongly disagree), we asked about aspects of their involvement that would identify the strength of relationships and engagement between students, faculty, and community organizations, and the benefit to the people and communities served by these organizations. Figure 2 illustrates the agreement with relationships between the community organization and students and faculty. This figure demonstrates the strength of agreement with the community and individual benefits from these projects. Figure 3 illustrates the strength of agreement with the perceived mentoring role of the community organization to students. Additionally, this figure illustrates the strength of agreement with the potential for continuing relationships between the organization and the university. Fifty-seven of the participating community mentors provided narrative responses to the (open-ended) item “Please list or describe in any general or specific ways you have already used the project or expect to use it” which are summarized in Table 1. Table 1 illustrates major themes for how community organizations utilize project findings, across a range of outcomes, with specific quotes illustrating the use of specific project findings.

Community Mentor Ratings for Relationships and Community Benefit.
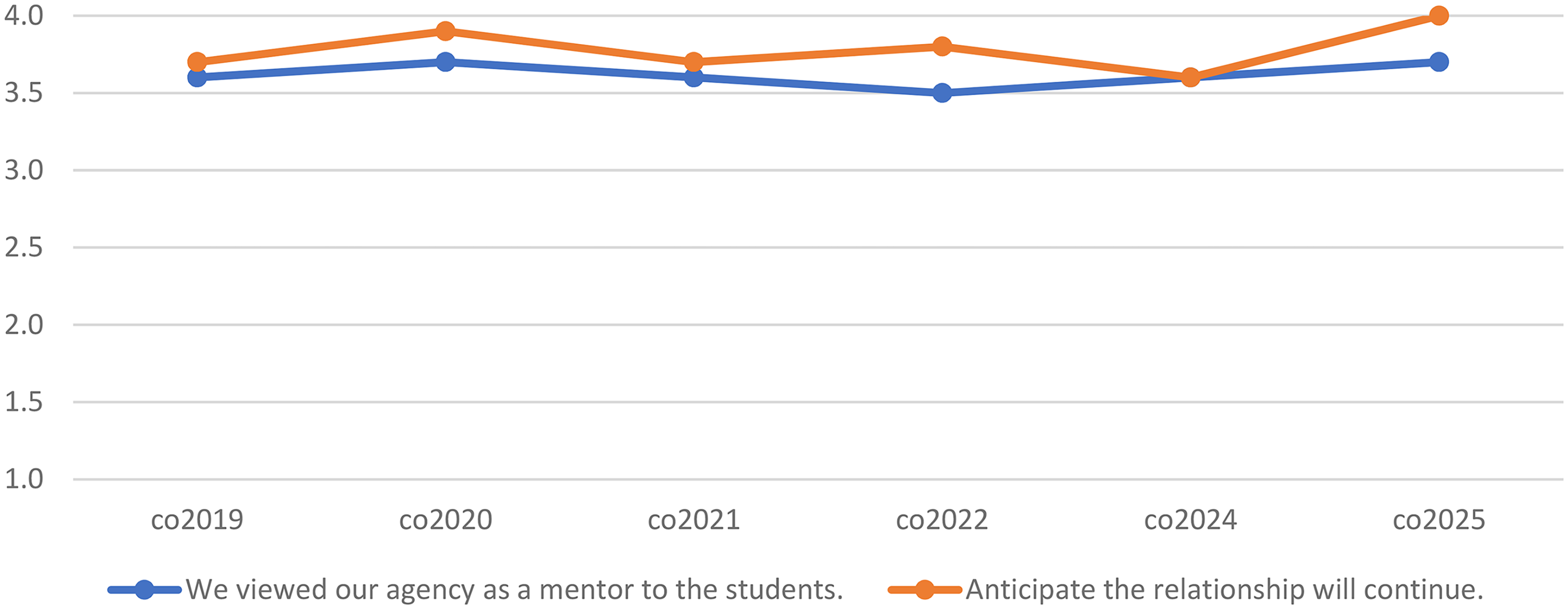
Community Mentor Ratings for Perceived Mentoring and Continuing Relationship.
Major Themes: How Collaborative Projects Are Currently/Will be Utilized.
Discussion
This paper expands on our prior work5,6 and highlights potential opportunities from our lessons learned for partnerships in settings beyond medical education, such as public health practice and research. The most cited reasons for engaging with the university in public health projects were to influence the training of health professionals (74% of respondents) and positive prior experience with our students (72%). These reasons are consistent with agencies’ views of their relationships with faculty and students and their mentoring roles with students (Figures 2 and 3). Limitations of the study included not all mentors completing the end-of-course surveys and that implementation of the course is in a single institution.
Statewide, Vermont has more than 6400 nonprofit organizations, requiring organizational strategies to garner significant resources (including technology), create partnerships, and ensure ongoing training and volunteer capacity, while meeting growing health and social needs in communities.17,18 In our experience, nearly half of participating community organizations cited the need for additional help, consistent with community health and social needs in the context of limited resources; a similar percentage wanted to have a relationship with the university.
Community organizations reported a wide variety of current and planned uses for project findings, from internal program evaluation and planning to external outreach, education, and advocacy (Table 1). These specific benefits and documented uses, along with reported plans for future projects, further support strong and sustained engagement between community organizations and the university.
Cultural humility and community engagement are essential for partnerships in public health and medicine, education, and research. CDC and others cite the importance of cultural humility in this process.19,20 Other authors describe strategies to teach community engagement, focusing on students, communities, equity, and sustainability.7,11,21 Applying community engagement principles in research is a priority for the National Institutes of Health 22 and other academic institutions.23-28 Our projects begin with community-initiated needs, ongoing collaboration, and focus on project outcomes benefiting communities and the organizations that serve them.
Facilitators and drivers of successful partnerships are essential for project success and sustained community engagement. This work builds on our prior work in the understanding of community benefits and identifying strategies that facilitate sustained engagement. Our data and experience suggest that documented community benefit is essential for long-term engagement, adding to the literature on community engagement in medical education. Community-identified health needs vary over time, reflecting changing public health priorities and organizational needs. Each year, 16 projects and organizations participate out of a potential number of about 150 readily available organizations through our longstanding United Way partner. Organizations in our partnership with the United Way network have worked with us for multiple years to well over a decade, depending on the specific public health need identified, its scope, and complexity. During our study period, 46 different organizations participated, with 29 (63%) participating more than once during the study period or previously. Our prior works5,6 highlight the importance of a “community-first” mindset in developing projects and the importance of community benefits. This remains consistent with our more recent finding in which nearly half (47%) of respondents cited that they “needed additional help” and 72% cited “positive prior experience” as reasons for participation (Figure 1). Responding to identified community needs with deliverable products, such as abstracts and posters, in a semester-long timeframe, serves as concrete and responsive contributions to a variety of identified needs (Table 1). Our broad and sustained partnership with the United Way of Northwest Vermont and partner organizations began over 20 years ago and remains strong today, as community health needs evolve over time.
Additionally, our lessons learned from this longstanding community–academic partnership may have additional relevance to individuals and organizations building and sustaining community–academic partnerships for public health practice and research. What we have learned from our experience in sustaining engagement in our community–academic partnership additionally potentially relates to principles of community engagement for research and public health practice. 27 Utilizing existing resources to reduce disparities, facilitating research translation into practice, and using shared knowledge and expertise are all potential benefits. 27 Lessons from our experiences may benefit others in engaging with communities in education, practice, and research.
Conclusion
We describe a novel evaluation of attitudes toward community engagement from our perspective of a required medical school course and a longstanding community–academic partnership. Using 7 years of completed surveys from community organizations serving as project mentors, we identified the most cited reasons for participating, the importance of identified benefits from partnerships, and an intent to continue in the future as important. In our experiences, project uses such as internal program planning, external outreach, education, and advocacy, were all noted. In addition to further strengthening community–academic partnerships in medical education, lessons learned about sustained community engagement also suggest potential implications for public health practice and research partnerships by providing additional insights for developing and sustaining these relationships. These findings may be useful to other institutions and organizations in other geographic settings.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251353070 - Supplemental material for Sustaining Community Engagement: Lessons Learned From Medical Education for Community–Academic Partnerships
Supplemental material, sj-docx-1-mde-10.1177_23821205251353070 for Sustaining Community Engagement: Lessons Learned From Medical Education for Community–Academic Partnerships by Jan Kirk Carney and Thomas V. Delaney in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251353070 - Supplemental material for Sustaining Community Engagement: Lessons Learned From Medical Education for Community–Academic Partnerships
Supplemental material, sj-docx-2-mde-10.1177_23821205251353070 for Sustaining Community Engagement: Lessons Learned From Medical Education for Community–Academic Partnerships by Jan Kirk Carney and Thomas V. Delaney in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors want to acknowledge the assistance of Deja Murray, Audree Frey, and Jessie Raven for their support of the course and for assisting with data collection.
Ethical Considerations
This project was reviewed by the University of Vermont IRB, and it was determined that the study was exempt from review under Exemption Category 1 Educational Research 45 CFR 46.104(d)(1). This exemption category is for research conducted in established or commonly accepted educational settings, involving normal educational practices. (Both the procedures involve normal education practices, and the objectives of the research involve normal educational practices). Consent, Health Insurance Portability and Accountability (HIPPA), and waiver determinations are not applicable or required under this IRB determination.
Author Contributions
JKC contributed to the conception or design of the work; the acquisition and interpretation of data for the work; drafting the work and reviewing it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. TVD contributed to the conception or design of the work; the analysis, and interpretation of data for the work; drafting the work and reviewing it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant U54 GM115516 from the National Institutes of Health for the Northern New England Clinical and Translational Research Network.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JKC receives annual textbook royalties from Jones & Bartlett Learning for Controversies in Public Health & Health Policy (ISBN: 9781284049299; 2016) and A History of Public Health: From Past to Present (ISBN: 9781284111774; 2023).TVD has no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.