
Abstract
Although global prevalence of autism has grown substantially, researchers still report inequity in access to evidence-based interventions in many low-resource settings where majority of world’s children live. Capacity building of diverse stakeholders in low-resource settings has been suggested to be a potential way to mitigate low levels of access to resources; however, little is known about what these stakeholders consider as helpful strategies in capacity building. In this qualitative research, we conducted five focus groups with 30 Mongolian caregivers of children with autism and 15 individual interviews with professionals in Mongolia. Three themes emerged from this study, including (a) partnership, (b) advocacy, and (c) empowerment. Each theme also contained several categories. For example, partnerships included enhancing collaboration among stakeholders and collaboration with international development agencies; advocacy included parental and legislative advocacy; and empowerment included training for diverse stakeholders, including caregivers and professionals. Implications and directions for future research are also suggested.
Lay abstract
Prevalence of autism is increasing all around the globe, but there is still great inequity in accessing evidence-based interventions. Although the field of autism research has made great strides in identifying and establishing evidence-based interventions, dissemination and implementation of these interventions have been reported as inequitable. This inequity is especially highlighted in many low-resource settings, such as Mongolia. As a field, there is still much to be learned about what strategies are used by stakeholders in low-resource settings to build capacity and to mitigate the hardships. To gain a deeper understanding of strategies for capacity building within a low-resource setting, we conducted five focus groups with 30 Mongolian caregivers of children with autism and 15 individual interviews with various professionals who work in Mongolia. These stakeholders reported three main strategies, including (a) partnership, (b) advocacy, and (c) empowerment, which included several strategies and implications on capacity-building practices. Furthermore, the findings from this study may suggest important implications for future intervention research.
Autism presents in millions of individuals worldwide regardless of their demographic characteristics. The prevalence of autism worldwide has been fairly understudied, which varies with an estimate of one in 100 (1%; Zeidan et al., 2022) to one in 270 individuals (.37%; World Health Organization [WHO], 2021). As it is practically difficult to conclude with an exact prevalence of autism due to the methodological variances in each country (Chiarotti & Venerosi, 2020; Wallace et al., 2012), researchers around the world have reported varying prevalence, including 0.39% in China (F. Wang et al., 2018), 0.87% in Mexico (Fombonne et al., 2016), 0.23% in India (Rudra et al., 2017), and 2.27% in the United States (Maenner et al., 2021). Such discrepancy may be contributed to by multiple factors, including availability of culturally sensitive diagnostic tools and personnel, sampling bias, mental health infrastructure, and public health policies (Elsabbagh et al., 2012). Regardless of these variations, the consensus is that these numbers may be an underrepresentation of true prevalence and that autism has become a global health concern (Divan et al., 2021).
Kieling et al. (2011) addressed a common concern with research disparity and underrepresentation of many low- to middle-income countries (LMICs) in global mental health and suggested that only 10% of relevant studies were conducted in LMICs where 90% of children and adolescents live. This inequity in both research and practice is exacerbated in low-resource settings (LRSs; Lee & Meadan, 2021) where there are limited resources for stakeholders of children with autism, such as family members. Furthermore, many children with autism in LRSs have little access to services and treatment options largely due to their national infrastructure in mental health (Divan et al., 2021). As a result, children with developmental disabilities (DD), including autism, are often excluded from educational opportunities (Mizunoya et al., 2018). Moreover, even if they are physically placed in schools, they often receive special education services in segregated settings (Wang, 2008). There is also a chronic shortage of qualified personnel who can provide individualized, high-quality special education or psychoeducational interventions to children with autism in LRSs (Harrison et al., 2016).
Efforts of the international communities
The international communities have long promoted the ideal of equitable education for all. For example, as early as in 1959, the Declaration of the Rights of the Child was adopted by the United Nations (UN) General Assembly, which specifically emphasized the rights of children with disabilities and their rights to be “given special treatment, education and care required by his particular condition” (UN, 1959). This principle then evolved over time and the rights of children with disabilities were again addressed in the Convention on the Rights of the Child in 1989 by the United Nations Children’s Fund (UNICEF, 1989), which specifically emphasized children’s well-being and rights to receive proper education for the “fullest possible social integration and individual development.” In the UN Standard Rules on the Equalisation of Opportunities for Persons with Disabilities of 1993, the language was further extended to very young children with disabilities and it promoted UN Member States’ responsibilities in providing inclusive educational opportunities. Most recently, the United Nations Educational, Scientific, and Cultural Organization (UNESCO, 2021) emphasized the importance of inclusive early childhood education for children with DD as a priority in achieving the UN’s 2030 Sustainable Development Goals. In response to the challenges faced by many families of children with DD, the UNESCO (2021) also recognized the vital roles that various non-governmental organizations (NGOs) play in many LRSs, including service delivery for marginalized and minoritized populations.
Despite the prolonged emphasis worldwide, however, relevant literature unfortunately reflects the arduous reality that children with autism and DD are still not being provided with proper treatment or meaningful inclusion in educational or community settings (UNESCO, 2021). There are still institutional, systemic, and societal barriers in many LRSs that prevent meaningful inclusion or treatment for children with autism. Furthermore, families of children with autism in LRSs have also reported their experiences of severe hardship due to various factors, including social isolation, financial burden, and limited resources (An et al., 2020; Lee & Meadan, 2021). Stakeholders in these studies described similar difficulties despite being in different countries, which indicates the need to further investigate strategies for capacity building and what would benefit these stakeholders in LRSs.
Mongolia as an example of an LRS
One example of an LRS is Mongolia, a landlocked LMIC in East and Central Asia neighboring China, Russia, and Kazakhstan. Mongolia may be an example to other LRSs in this region due to the geographical and cultural proximity. Furthermore, there is very limited autism research on Mongolia, which may lead to invisibility and limited access to evidence-based interventions (EBI; Lee & Meadan, 2021). As a result, many caregivers of children with autism are left with limited choices for unsubstantiated or alternative treatment, which are not based on evidence or scientific background (An et al., 2020). Researchers have reported various types of syncretic care being prevalent for children with autism in many LRSs, which often involves (a) indigenous, culturally traditional biomedical interventions, such as mixed herbs or oriental medicine (Ha et al., 2014); (b) modern biomedical supplements, such as vitamin B12, omega-3 fatty acid, and zinc (An et al., 2020); (c) physiologically oriented interventions, such as acupuncture and acupressure massages (Ha et al., 2014); or (d) spiritual, faith-based “healing” approaches, such as shamanic rituals, animal sacrifices, or a traditional, religious “healer” (Gona et al., 2015). The efficacy of these treatments remains unknown and some biomedical practices without any research evidence may even be physically harmful. As An et al. (2020) argued, however, it is notable that these potentially dangerous or ineffective choices are not reflective of a family’s choice; rather, these are often the only approaches that are available and a reflection of parents’ desperate attempts to “try anything” (p. 1822). Although a majority of these treatments have already been challenged extensively in the scientific communities, these seem to be especially prevalent in LRSs, including Mongolia, due to limited access to EBI. Therefore, it is necessary to seek effective strategies to increase capacity of a community in response to the low level of resources around the globe.
Capacity building
As seen in the literature, there is a combination of difficulties for stakeholders of children with autism who live in LRSs, which may be alleviated by increased capacity of these communities. Capacity building may also be a necessity in response to the low levels of access to resources, such as EBI for children with autism. However, little is known what stakeholders in LRSs report as useful and potentially viable strategies for capacity building. Therefore, there is a critical need for examining stakeholders’ perceptions of current and future strategies to achieve capacity building on a larger scale. There are various definitions and approaches to community capacity building. The WHO defined capacity building as “development of knowledge, skills, commitment, structures, systems, and leadership to enable effective health promotion,” which includes “the advancement of knowledge and skills among practitioners; the expansion of support and infrastructure for health promotion in organizations, and, the development of cohesiveness and partnerships for health in communities” (Smith et al., 2006, p. 341). Evidently, emphases are being placed on increasing the stakeholders within the community to promote empowerment. This aligns with community–academic partnership that is promoted through the use of community-partnered participatory research (Henrick et al., 2017), which was suggested as a gap and a future direction in autism research (Vivanti et al., 2018).
Current qualitative research on autism globally is mostly focused on negative experiences, barriers, and needs of stakeholders of children with autism in LRSs (e.g. An et al., 2020; Lee & Meadan, 2021). Although understanding these perceptions can be very informative in developing socially valid interventions and proper policies, it is also important to acknowledge what these stakeholders report as effective strategies and their perceptions of potential strategies for capacity building in their communities. For example, Mongolian caregivers of children with autism reported exchanging information and supporting each other within the NGOs as a positive aspect (Lee & Meadan, 2021). Such strategies (e.g. caregiver peer support) may be culturally and socially valid strategies to increase a community’s capacity in response to the very low levels of resources in Mongolia. Despite the limited resources in many LRSs globally available to stakeholders, very little is known in autism research about what strategies these stakeholders report as positive, necessary, or potentially helpful to increase the capacity of their communities. Therefore, this study was conducted to examine various stakeholders’ perceptions of current and potential strategies for capacity building in Mongolia. The stakeholders in this study included (a) Mongolian caregivers of children with autism and (b) professionals in various fields related to working with Mongolian children and their families.
Method
Participants
Following approval from the institutional review board (IRB) of the University of Illinois, recruitment activities were carried out by the Autism Association of Mongolia (AAM), a caregiver-led NGO for Mongolian children with autism and their families. Caregivers and professionals were recruited with a flyer in Mongolian that was posted on the AAM’s social media and by verbal announcements. A caregiver participant had to be (a) a caregiver of a child with autism and (b) willing to complete the demographic questionnaire and participate in a focus group interview. Participants’ eligibility was screened by the AAM when the participants called to express their interest in participating in the study. Inclusion criteria for professional participants included (a) working with children with autism and their families in any capacity and (b) willing to complete a demographic questionnaire and participate in an individual interview. No incentive was offered for participation. Five focus group sessions with a total of 30 Mongolian caregivers of children with autism were conducted and individual semi-structured interviews were conducted with 15 professionals who worked in the field of child development, international development, and special education in Mongolia.
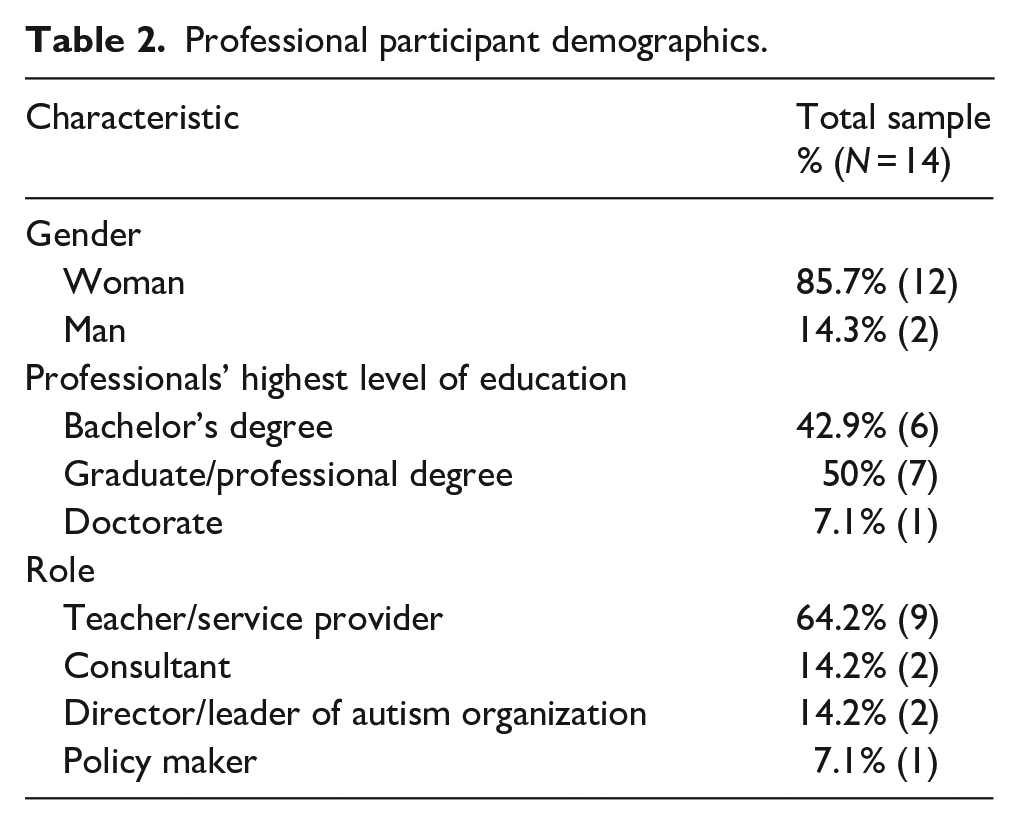
Of the 30 caregiver participants, 77% (n = 23) were mothers and 17% (n = 5) were fathers. In addition, one grandparent and one extended family member participated. More than 90% of the caregivers (n = 27) reported having at least some college education and more than 66% of the caregivers (n = 20) reported household incomes higher than the average monthly Mongolian household of US$400 (Asian Development Bank, 2019). Most children were 8 years old or younger (83%, n = 25; see Table 1). Of the 15 professional participants, 87% were women (n = 13) and 13% were men (n = 2). All professional participants held college degrees, including 40% (n = 6) with a bachelor’s degree, 46.6% (n = 7) with a graduate or professional degree, and 6.7% (n = 1) with a doctorate. One participant did not respond to this question. The professionals had various occupations, including teacher, researcher, psychologist, pediatrician, director/leader of an autism NGO, and international development or government agency personnel, and they worked with children with disabilities and their families in different capacities (see Table 2).
Caregiver participant demographics.
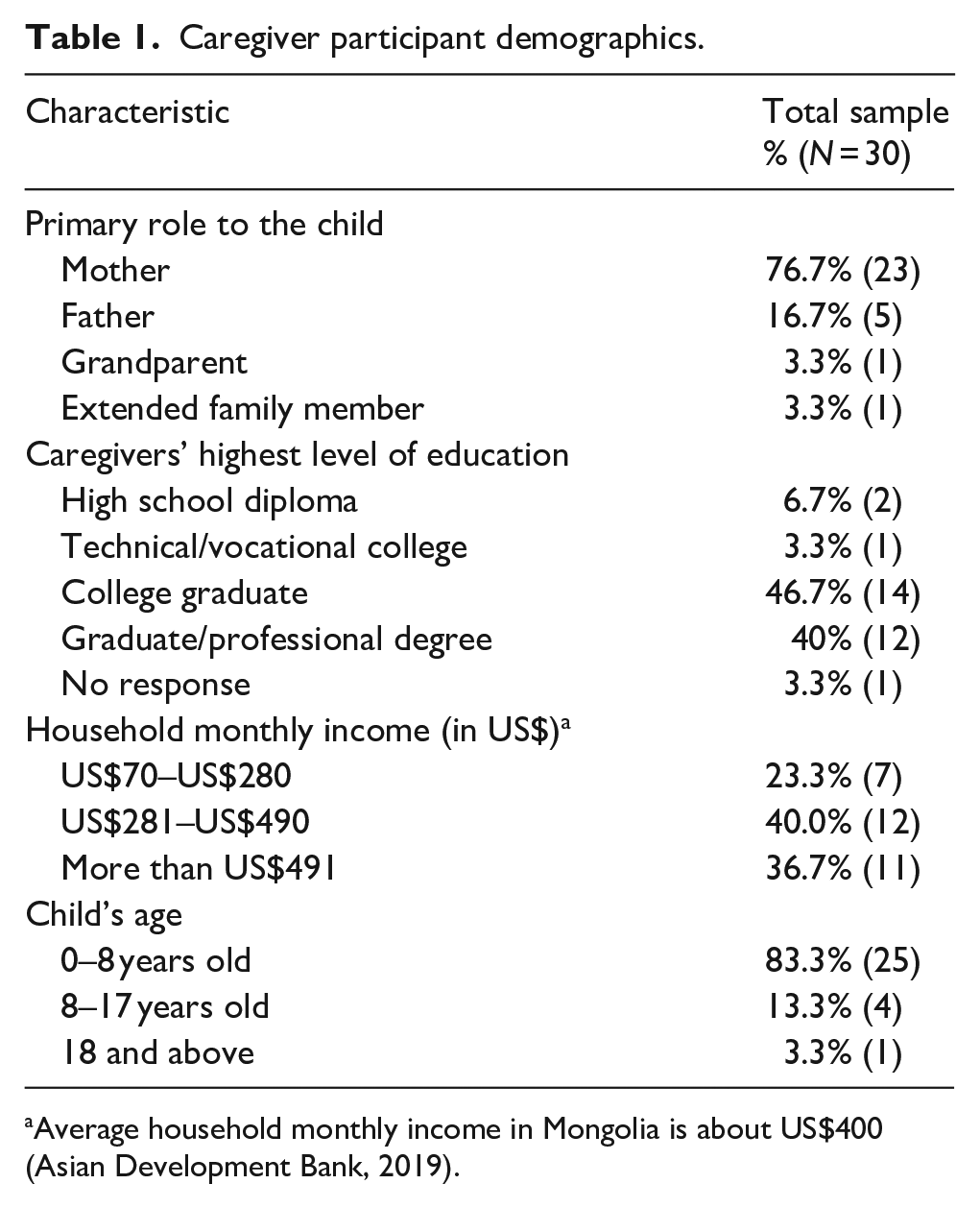
Average household monthly income in Mongolia is about US$400 (Asian Development Bank, 2019).
Professional participant demographics.
Community engagement
This study was conducted using principles of community-partnered participatory research in attempts to promote community–academic partnership, which involves the process of researchers and community stakeholders jointly addressing shared priorities and research agendas (Clark & Ventres, 2016). The first and second authors were a doctoral student and a faculty member in special education at a US university who had several years of experience working with children with autism and their families. The third author was a Mongolian who studied in the United States and earned a bachelor’s degree in health sciences; he helped with data collection, translation, and data analysis. The fourth author was a Mongolian who had background experience in NGO management and fundraising; she helped with recruitment, logistics, and data collection in Mongolia. The partnership between the AAM and the US-based research team has been in place since 2018 to promote sustainable changes for stakeholders of children with autism in Mongolia.
Data collection and measures
Focus groups and semi-structured individual interviews were conducted to explore the experiences and perspectives of caregiver and professional participants (Nyumba et al., 2018). Conducting qualitative research in an LRS with little extant research allowed us to enhance our understanding of caregivers’ and professionals’ perceptions. Both focus groups and individual interviews have been frequently utilized in autism-related studies and were reported to be effective in gaining insight into stakeholders’ experiences (Koffer Miller et al., 2018; Lee & Meadan, 2021). Four in-person focus group sessions and an online focus group session were conducted with Mongolian caregivers and 15 individual, in-person interviews were conducted with professionals in Mongolia. Prior to participating in an interview or focus group session, each participant completed a short demographic questionnaire specific to their role. The questionnaires were developed in English, translated to Mongolian, and then sent to a few native Mongolian speakers to ensure they were culturally appropriate. In addition, interview protocols developed for the focus group sessions and the individual interviews were utilized to encourage conversations that captured a wide range of perspectives. The four in-person focus group sessions were conducted in the NGO office by the first author and the individual interviews with professionals occurred in the professionals’ respective offices. Each focus group included five to seven caregivers. The first author facilitated all interviews and focus groups and encouraged participants to share their experiences and voice their thoughts.
This study was part of a larger study (Lee & Meadan, 2021) and reports data specific to strategies for capacity building. Interview questions were related to the caregivers’ or professionals’ experiences, needs, barriers, and strategies related to supporting children with autism and their families. For example, caregivers were asked, “Are you satisfied with the current supports and services? If not, what is missing?” “What additional support do you think will benefit your child and family?” and “Do you feel like you can lead changes for your own child’s services or other children’s through the system?” For the individual interviews, professionals were asked, “What can a parent of a newly diagnosed child do to get support in Mongolia?” and “What strategies or advice would you give to stakeholders from other developing countries based on what worked or didn’t work in Mongolia?” Interview protocol was uploaded as a supplementary file.
Procedures
AAM staff members, who were fluent in both Mongolian and English, served as interpreters during the focus group sessions and interviews when needed. See Lee & Meadan (2021) for detailed descriptions of the procedures for the focus groups. For the individual interviews with professionals, 40% (n = 6) of the interviews were conducted in English without an interpreter, 53% (n = 8) were conducted in Mongolian with an interpreter, and one interview was conducted in Korean without an interpreter. Interviews with professional lasted from 16 to 71 min (mean duration: 40 min) and focus group sessions lasted from 40 to 50 min (mean duration: 44 min).
Transcriptions and translations
A few Mongolian-English bilingual speakers assisted with transcribing and translating the interviews. See Lee & Meadan (2021) for the procedure for the focus groups. The transcripts for individual interviews were translated and sent to each individual for member check process (Brantlinger et al., 2005). One participant requested a few minor changes related to organization of the data.
Data analysis
Data related to the demographic information were analyzed to provide participants’ descriptive information. Thematic analysis (Vaismoradi et al., 2013) was used in which the researchers (a) familiarized themselves with the data by reading the transcripts carefully, (b) started with an open-coding process whereby they identified units independently, (c) labeled these codes as they emerged within the data, (d) compared the new codes with the existing ones to examine whether they warranted new code labels, (e) met and discussed the codes, (f) reached consensus on each code, (g) organized codes into categories, and (h) further grouped categories into themes. There were two sources of data (i.e. focus groups and interviews), which we sought to compare and contrast across transcripts.
Credibility and trustworthiness
We have taken measures to promote credibility and trustworthiness of this study according to Brantlinger et al.’s (2005) recommendations in qualitative research. For example, we have (a) utilized field notes from the individual interviews and focus groups, (b) provided rich descriptions of the data including the participants’ demographic information as much as possible, and (c) collaborated with multiple stakeholders when collecting and analyzing the data.
Findings
The findings are derived from five focus group sessions conducted with 30 Mongolian caregivers of children with autism and 15 individual interviews with professionals in Mongolia. Three main themes related to strategies for capacity building were identified, including (a) partnership, (b) advocacy, and (c) empowerment (see Figure 1).
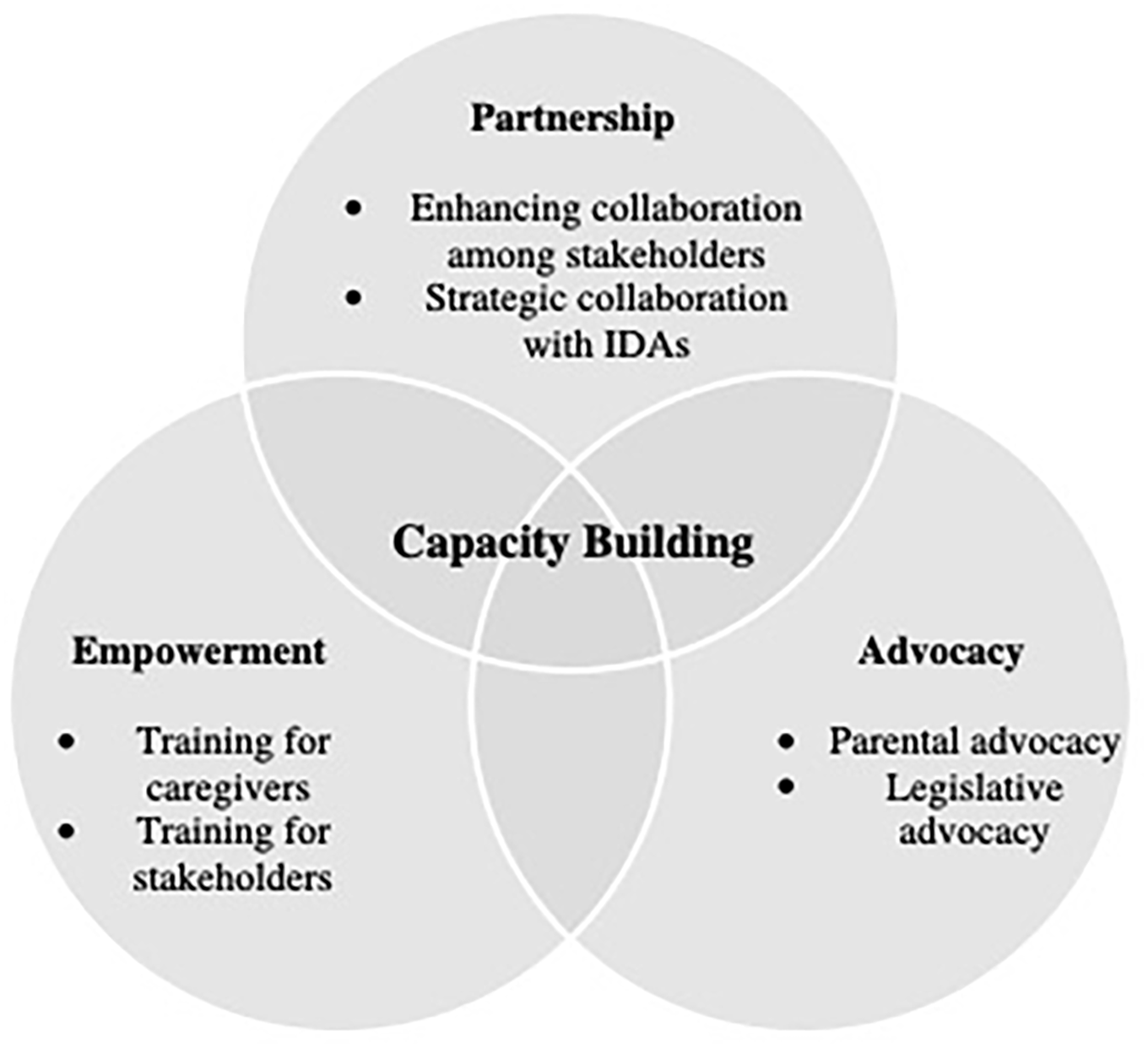
List of themes and categories on capacity-building strategies.
Partnership
Partnership refers to forming reciprocal and collaborative relationships with each other. Stakeholders emphasized partnerships among various entities as a strategy to promote capacity building in their communities. These entities included the Mongolian government and its agencies, international development agencies (IDAs), and Mongolian and international NGOs, including stakeholder groups such as the NGO. Stakeholders suggested that partnership between these entities may catalyze changes at both broader societal and individual levels, and they also shared some existing and effective strategies.
Enhancing collaboration among stakeholders
Both groups identified forming partnership with various stakeholders, including the government, IDAs, and local NGOs, as an important strategy they were currently using and a potentially effective strategy for increasing stakeholders’ capacity. As an IDA staff member, P1001 shared, The government should be more active in this matter [inclusion of children with autism]. After all, it should be the governmental efforts to include children with disabilities.
P1003, also an IDA staff member, similarly said, As an NGO, we are telling the government that NGOs are the experts [in autism], so the government needs to cooperate and collaborate with the NGO.
An NGO director, P1012, also shared the practical importance of collaboration between the government and the NGO: The government can’t be experts on everything. But NGOs can focus only on autism. . . NGOs don’t need to be at the national scale or too big but could be more of a resource center for the government and other international agencies.
As an IDA staff member, P1014 highlighted the importance of coordination among stakeholders and reported, We started this coordination for special education where we have stakeholders, including the government agencies, some teacher trainers, and NGOs . . . come together and learn why we are doing this [coordination], what kind of issues there are [at the government level].
A few stakeholders also highlighted the efforts and initiatives undertaken by the government. For example, P1003 shared, [The Mongolian government] passed a new law in 2016 about the protection of the rights of disabled persons, to support them and children with disabilities.
P1013 also stated, Parents and professionals should work together. In this case, it can bring changes. Sometimes it seems like the reality is not [there] yet, of course, but it’s better now that the attitude [toward autism] is getting better.
Strategic collaboration with IDAs
A few caregivers discussed the importance of partnering with IDAs and foreign volunteers as an effective strategy for capacity building of local stakeholders. For example, a caregiver shared, Parents are doing as much as possible for their child but don’t know the right method. There isn’t any support from the government, so NGOs should contact foreign organizations and request support and funds [to support parents].
Another caregiver said, We, as parents, should submit a proposal to the government and request them to send professionals to get proper training from abroad, and they would plant seed here and train many parents.
Some professionals reported that main function of IDAs and foreign volunteers is to support local stakeholders to promote inclusion of children with autism rather than providing direct services. P1001 reported, I observe, train, and consult [Mongolian] teachers. I also teach a foundational course in special education for teachers. I teach them why some children exhibit challenging behaviors, how to improve behaviors, or just model for the teachers, and they imitate.
P1012 also shared, We invite professionals from foreign countries because there are not many professionals in Mongolia who can teach parents.
A psychologist, P1002, similarly shared, There were three foreign professionals at my kindergarten, and they taught the kids, have classes [for local teachers]. . . After they left, local teachers were continuing to do everything [they learned].
Notably, some professionals also acknowledged the limitation in the scope of practice of many IDAs in Mongolia. For example, P1001 shared, The biggest barrier is that children with disabilities are not in schools, and because they stay at home, they are invisible [to IDA]. They don’t know that these kids exist because children with disabilities are generally invisible in Mongolia. They would have to look for children in certain areas, and actively recruit them to participate [in their programs].
Advocacy
Another strategy that emerged from the interviews was advocacy, which was divided into parental advocacy and legislative advocacy. In this study, advocacy refers to activities that are in support of other caregivers in increasing their capacity. Of the two categories, parental advocacy refers to specific advocacy activities for and by caregivers, and legislative advocacy refers to advocacy activities to promote equity for stakeholders of children with autism.
Parental advocacy
Increasing autism awareness
Both caregiver and professional groups emphasized increasing autism awareness as an important strategy. For example, a parent shared, To promote awareness [on autism], the government should do more work, but we should also let the public know more about what autism is.
Professionals also shared the importance of advocating for greater awareness on autism. For example, in response to a question that asked how to better support Mongolian caregivers who are new to autism, P1007, who was a pediatrician, answered, Raising public awareness. [For example] we have done a lot of work on raising awareness about cerebral palsy, so now everybody recognizes that cerebral palsy is a disability. Awareness is very important.
Similarly, another NGO director, P1010, shared, You inform the community, the society, and you eventually will have success. . . We have to change the attitude and community perceptions toward people with autism. If everybody starts thinking like us, that will be a big change. . . Barriers stem from community awareness, the lack of awareness, lack of information. If you can go and disseminate the information [on autism], I’m sure the barriers will disappear. So that just means we need to do a lot of awareness work through social media, through all kinds of channels to make this better.
As an NGO director who has wide experience with advocacy and awareness, P1012 shared, We can’t “fix” our children to make them “typical” and adjust to the society, but the society should adjust to our children. That’s why we needed to raise public awareness on autism, and we wanted other people to know about autism and to accept our children. . . NGOs are like the voice here, the voice of the autism community.
Notably, some professionals also acknowledged the limitation in the scope of practice of many IDAs in Mongolia and the importance of advocacy. For example, P1001 shared, The biggest barrier is that children with disabilities are not in schools, and because they stay at home, they are invisible. They don’t know that these kids exist because children with disabilities are generally invisible in Mongolia. They would have to look for children in certain areas, and actively recruit them to participate [in their programs].
Parent-to-parent support
Stakeholders also discussed a more specific advocacy strategy in which parents provide and receive support from each other (i.e. parent-to-parent support). One caregiver said,
After we joined the NGO, we started getting support from [other parents] here.
Another caregiver similarly shared, I was able to get a lot of information [related to autism] because of [other caregivers of] this association, and we are working hard both at home and kindergarten with my child.
Professionals also suggested parent-to-parent as one of unique form of advocacy in LRSs. P1003 suggested, One of the most resourceful groups is associations like the Autism Association of Mongolia, rather than the local government agencies. It’s peer counseling, and they can give newly diagnosed mothers very useful advice as more experienced mothers.
P1014 said, Our general training for parents includes classes where they can actually mingle with other parents.
P1012 explained, Although we cannot provide professional help, we instead provide consultation services to parents each week. We share our experiences and what we know about autism and try to help each other and guide parents. . . We support our parents, and they can share their experiences, what they know, and provide psychological support as a community. That’s why we started this organization.
Legislative advocacy
Caregivers expressed their concerns and existing or potential strategies related to raising awareness of legislation on disability and anti-discrimination in Mongolia. One caregiver shared, There are laws that passed, which are written nicely on paper, but it is not working for us, and nothing happens on the ground. People who are supposed to implement these laws do not know anything about them.
Professionals also pointed out that because this legislation exists, advocating for its implementation and enforcement can be an effective strategy. P1010 shared, We actually have good laws, which say that children with disability should go to the same school, same class [as their peers] . . . this is like the law on the paper, but it doesn’t get implemented. . . But we are trying to push it and change the legislation. We will have to interact with the people on top [politicians] regarding the legislation.
P1014 corroborated and said, These laws are not familiar to people, so the government doesn’t urge schools [to follow]. . . So they don’t actually understand the law. Besides, there are no practical guidelines of how to implement the law, how the schools and NGOs should [work together]. This link is missing. It’s written and adopted in a way that pleases the Parliament but doesn’t necessarily reflect the voice of the wider community.
P1006, who is also a parent of a child with disability, shared, We must know the law. If we don’t know it, schools say, “No, your child is not supposed to be here. Your child is supposed to be in [segregated] special school.” We need to then show this legislation. . . As parents, we are angry. Not angry, more than angry. That’s why we would really like to push this government so they would understand implementation [of laws].
Collective efforts to legislative advocacy
Stakeholders further discussed potential strategies to respond to the lack of enforcement of the laws. One parent shared, We may be able to start making progress by enlightening people [about the laws].
Another parent shared, Parents who have children with autism should join and talk to the government together. Current laws are enough to support and defend our children’s rights. In public schools, these children have lawful rights to be enrolled without any problem. If we talk to the government, we can succeed in solving our problem.
P1006 stated, They [parents] can empower [each other]. Power comes from inside, and as this group of people come together, they will be powerful. If we’re alone at home, we’re not powerful.
P1010 also commented, We try to raise our voice and raise it to the government, to the state, so that they can make our lives a bit easier. But we have to work together. We want them to cooperate with us, give resources.
P1012 similarly emphasized the importance of stakeholders’ collective advocacy, It’s good to have many NGOs, but they have to be together and have one voice. Parents need to talk, and NGOs should always work together. . . We try to be close to other NGOs because disability is one thing.
Empowerment
Stakeholders also reported empowerment as a strategy for capacity building to respond to the low levels of resources available in Mongolia, which includes training for caregivers and other stakeholders to increase their ability to provide better services for children with autism. They also emphasized the importance of gaining knowledge and competence in EBI that will likely lead to feeling empowered. In this study, empowerment refers to the process of helping others to develop competence.
Training for caregivers
Both groups emphasized the importance of increasing caregivers’ capacity to enhance their own children’s developmental outcomes largely due to the limited resources available in Mongolia. One parent said, We need to be taught proper methods. . . There needs to be government-funded classes that are free to the public. Parents are struggling to figure out how to raise their children, and we’re trying to make it happen all on our own.
Another parent shared, We need proper training for our children. It doesn’t matter whether it’s free or not. If it’s free, it’s great, but professionals are needed.
Another parent also emphasized, Parents need to get trained and gain skills. The difficulty is in finding someone to teach us. How to do the most basic things, how to raise awareness.
Most professionals likewise emphasized the importance of caregiver training opportunities. For example, P1002 said, I work with the kids, but I want the parents to participate. I tell them how they should do things, what to tell their teachers.
She also mentioned the need for parent training on a specific topic: If the child is being aggressive, they [parents] just start to get stressed and depressed. We would talk to them that “we did this, so maybe you should do the same at home.”
P1006 similarly shared, Our main purpose is not directly teaching children because it would be impossible [to teach effectively] with just 1 hour, 2 hours a week. Our goal is to teach parents, to guide parents.
P1003 explained that parent training is integrated in their organization and shared, It’s a family education program. We are not intervening directly with children; we ask parents questions and we make suggestions. We give advice to the parents on how to teach their children at home.
P1012 similarly said, We have this handbook that we give to parents each month, and parents have “homework” to work on with their children. . . We try to share what we know about behavior analysis and how to work [with the children], especially about challenging behaviors. Not everybody is a teacher here, and not everybody can be a trainer [for other parents]. That’s why we need support, professionals for parents. They may work with their child at home, but they need someone to guide them. Not just getting one training here and try to do something [with their child], professional people who guide them.
Training for stakeholders
While emphasizing the importance of training for caregivers, participants emphasized professional development for other stakeholders as well, including teachers in public schools and other therapists. One parent said, Teachers were not taught anything about special education to begin with. Teachers don’t get any training when it comes to educating children with autism. Because teachers don’t understand it, it may seem reasonable for them to ask the parents to take their kids away.
Another parent shared, A teacher doesn’t get more salary [even if they work with autistic children], so the teacher says, “Why don’t you go to the [segregated] special education school?” We don’t know what to do next.
A parent expressed her frustration with systemic barriers in education: Even if we organize trainings, teachers in public kindergarten or schools will not attend. . . So they do not get paid enough to do professional development. They do not understand even the basic signs of autism, and even the more senior teachers do not understand autism. . . Teachers should take courses and receive training.
Professionals provided some specific strategies being used to increase teachers’ capacity. P1001 explained, Some schools send special education teachers to Russia, Japan, or Korea during breaks so that they can visit the schools abroad and learn things.
P1005 shared, Teachers use the methods that they learned in trainings. For example, JICA provided training and a Japanese teacher provides advice to teachers.
Similarly, P1012 shared how the NGOs train stakeholders: If this community doesn’t know about autism, it’s not enough for parents to know everything. That’s why we provide trainings to professionals like teachers, other NGOs, doctors, and social workers. We try to talk to everyone who could be working with a child with autism so everybody can know what it is, and how to understand them better. . . We can do it without too much funding because it’s more about the commitment. For training professionals, it requires time, and professionals should be motivated themselves.
Finally, some also emphasized the importance of minimizing the reliance on foreign professionals by increasing the capacity of local stakeholders. P1003, a foreign national in Mongolia, reflected, We are simply foreigners. We come to Mongolia for a limited period of time, but the NGOs are Mongolians. They know the context, know the culture, and they don’t go away. So parents rely or feel closer to the local NGOs rather than foreigners like myself.
Discussion
The purpose of this study was to examine the perceptions of stakeholders of children with autism on strategies for capacity building in Mongolia. Examining existing and potential strategies to increase stakeholders’ capacity is crucial in many LRSs where there is very limited infrastructure for autism, from screening and diagnosis to necessary treatment. The findings revealed that both groups of stakeholders suggested partnership, advocacy, and empowerment as potentially effective strategies to increase the capacity of Mongolian autism communities. For example, partnership was suggested as a strategy that includes promoting collaboration among diverse stakeholders of children with autism, such as government agencies, schools, or IDAs. Advocacy was related to how stakeholders may advocate for their own children, other caregivers, and the autism community in general. Finally, empowerment through increasing stakeholders’ knowledge and experiences was suggested mostly due to the low levels of resources for stakeholders of children with autism in Mongolia.
The findings of this study, including these themes, also confirm the current literature. For example, community–academic partnership which encompasses all three themes has been identified as an integral component of building the capacity of stakeholders in autism research (e.g. Maye et al., 2021). Pearson et al. (2019) similarly identified partnership, advocacy, and empowerment as principles of family capacity-building practices as these are important strategies that promote more responsive, positive services to families. Some of the strategies are also consistent with autism research in various LRSs. Also, this study extends the findings from extant autism research that identified different strategies to increase capacity within an LRS. For example, Lee et al. (2022) provided a culturally adapted training and coaching program to parent mentors in Mongolia via telepractice. As suggested in this article, both parent mentors and mentees reported high levels of satisfaction and feasibility of providing and receiving peer support in delivering EBI to their children. This could be contributed to by utilizing the existing infrastructure of the NGO and strengthening their current program of parent support.
Limitations and implications
There are some limitations that should be considered when interpreting the findings of this study. First is the risk of misinterpretation or mistranslation during the process of data collection and transcription. Second, recruitment for this study was primarily conducted through the NGO’s social media and network, which may have limited the number or types of stakeholders during the recruitment process. Despite our efforts to widen recruitment, it is possible that stakeholders with little access to NGO’s social media due to poverty or other extraneous variables were not able to participate.
There are also several notable implications for research that emerged from this study. For example, both caregiver and professional groups emphasized the importance of training as a strategy to empower them and increase their capacity. This is partly due to the limited evidence-based resources, including providers who could delivery direct services (e.g. behavioral interventions). Thus, effective task sharing, including nonspecialist-delivered intervention, may be potentially useful in the LRS context (Divan et al., 2021). The WHO developed the Caregiver Skills Training to be adapted and disseminated in various LRSs across the globe (Salomone et al., 2019), which is a parent-mediated early intervention based on the theoretical frameworks influenced by applied behavior analysis and developmental science. It was developed to support caregivers of young children with DD, including autism, via dissemination by nonspecialists who are supported by experts. Such programs are highly malleable to be adapted to increase the contextual fit of the intervention and researchers have reported its feasibility and effectiveness in LRSs such as India (Sengupta et al., 2021) and Ethiopia (Tekola et al., 2020). Therefore, such programs have the potential to be helpful in increasing capacity of diverse stakeholders when properly adapted. Developing and examining more resources that are contextually fit to LRSs is another direction for future research. Although many strategies suggested by the stakeholders may be immediately useful, building infrastructure for care of children with autism (e.g. more professionals) is warranted for a long-term strategy.
Autism research has been reported to have limited representation in terms of participants’ demographics, such as race, ethnicity, or socioeconomic status (Maye et al., 2021). Such phenomenon is especially apparent in global autism research, which may perpetuate marginalization of minoritized populations. Therefore, autism researchers must solicit partnership from underrepresented stakeholders to develop more sound and socially valid interventions that can have lasting impact on building the capacity of their communities.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221127077 – Supplemental material for Strategies for capacity building in a low-resource setting: Stakeholders’ voices
Supplemental material, sj-docx-1-aut-10.1177_13623613221127077 for Strategies for capacity building in a low-resource setting: Stakeholders’ voices by James D Lee, Hedda Meadan, Enkhjin Oyunbaatar and Amarbuyan Amar in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.