
Abstract
Many modern medical school curricula have deemphasized the study of anatomy, dedicating significantly less curricular time to student dissection of human bodies and relying instead on other resources, including digital anatomy softwares. Extracurricular student-led dissections allow learners to develop a deeper understanding of the human body, practice surgical skills, and explore clinical interests. We here provide learners and anatomy educators with practical strategies to organize and execute efficient student-led dissections. The authors include senior medical students, anatomy faculty, and clinical instructors at Harvard Medical School with experience in facilitating student-led dissections. Based on our own experience with this approach, and within the background of current developments in anatomy education, we provided ten recommendations for creating a student-led anatomy learning experience. Priorities include understanding student goals, utilizing near-peer teachers, integrating case-based clinical data, partnering with specialty interest groups, and encouraging student independence. Medical students involved in student-led dissections have offered positive feedback with regard to clinical skills, retention of anatomy, and specialty discernment. Future research should gather both students’ subjective perceptions of dissection and objective learning outcomes to quantify the impact of student-led study of anatomy.
Introduction
The study of human anatomy is essential to undergraduate medical education, and dissection of human bodies has played a crucial role in anatomy education for millennia.1–3 As medical schools have reformed curricula to meet the increasingly complex demands of modern medical practice—emphasizing interprofessionalism, social determinants of health, and patient-centered care—time spent on anatomy education has diminished and transformed. 4 Long faculty-led laboratory sessions are time intensive and compete with expanding curricular demands from other disciplines, while students face increasing pressure to maximize their research, volunteer, and work experiences to enhance their residency applications. 5 Due to these constraints and to the advent of new technology, anatomy educators no longer rely only on the conventional pedagogy of lectures, two-dimensional drawings, and many hours of dissection.6,7 Instead, many medical schools have augmented time spent in the anatomy lab with modalities such as plastinated prosections, digital anatomical libraries, virtual dissection of computed tomography (CT) and magnetic resonance imaging (MRI)-generated images, interactive augmented reality, and generative Artificial Intelligence.8–10 The COVID-19 pandemic accelerated these changes; social distancing requirements temporarily suspended in-person dissection of human bodies and forced schools to accelerate the incorporation of virtual anatomy softwares.11–14
Digital anatomical resources, though useful and ever more sophisticated, obscure the immense variability of human anatomy and cannot adequately replace the tactile experience of dissection. For example, students can read about the difference between the muscular walls of an artery and the thinner, less rigid walls of a vein, but this distinction is more meaningful when students palpate these structures in a real human body. Importantly, digital resources are also unlikely to evoke the same emotional response that occurs when working with donated human bodies, depriving students of an opportunity to learn humanistic values and practices that are relevant to caring for the living.15–19 Medical students can also miss out on opportunities for emotional and professional growth. 20
Though modern curricula allow learners to study important aspects of twenty-first century medicine, some anatomists and clinicians have raised concern that anatomy knowledge has declined to a level that is inadequate for medical practice.21–23 Medical students pursuing a surgical specialty or radiology may be disproportionately affected by current trends in anatomy education, leaving soon-to-be surgeons and radiologists particularly unprepared for residency.24–27 As a result, there has been an increasing presence of efforts that include supplementary anatomy curricula for advanced electives in procedural specialties as well as just-in-time teaching methods in residency.28–30
In the absence of required anatomical dissection, some undergraduate medical students may be interested in and benefit from extracurricular study of anatomy. Students interested in surgery or other procedural specialties—or, importantly, those still discerning their clinical specialty or interested in developing their general clinical skills—can benefit from additional study of anatomy without adding further time-consuming requirements to saturated pre-clinical curricula.
Reflecting on our own implementation of peer-led extracurricular dissection over the past three years and considering the literature on current educational trends in anatomy, we created the following ten recommendations for the creation of a dissection-based, student-led supplemental anatomy experience, with a focus on design, implementation, and improvement. Our aim is to bolster students’ knowledge of clinically relevant anatomy, develop surgical skills through hands-on learning, and build long-term retention of anatomy knowledge through iterative peer-to-peer teaching. This practical guide contributes to the existing literature by providing a detailed, replicable framework for implementing student-led dissection initiatives in modern medical curricula—an area that remains underexplored despite growing interest in peer-driven, experiential learning in anatomy education.
Body
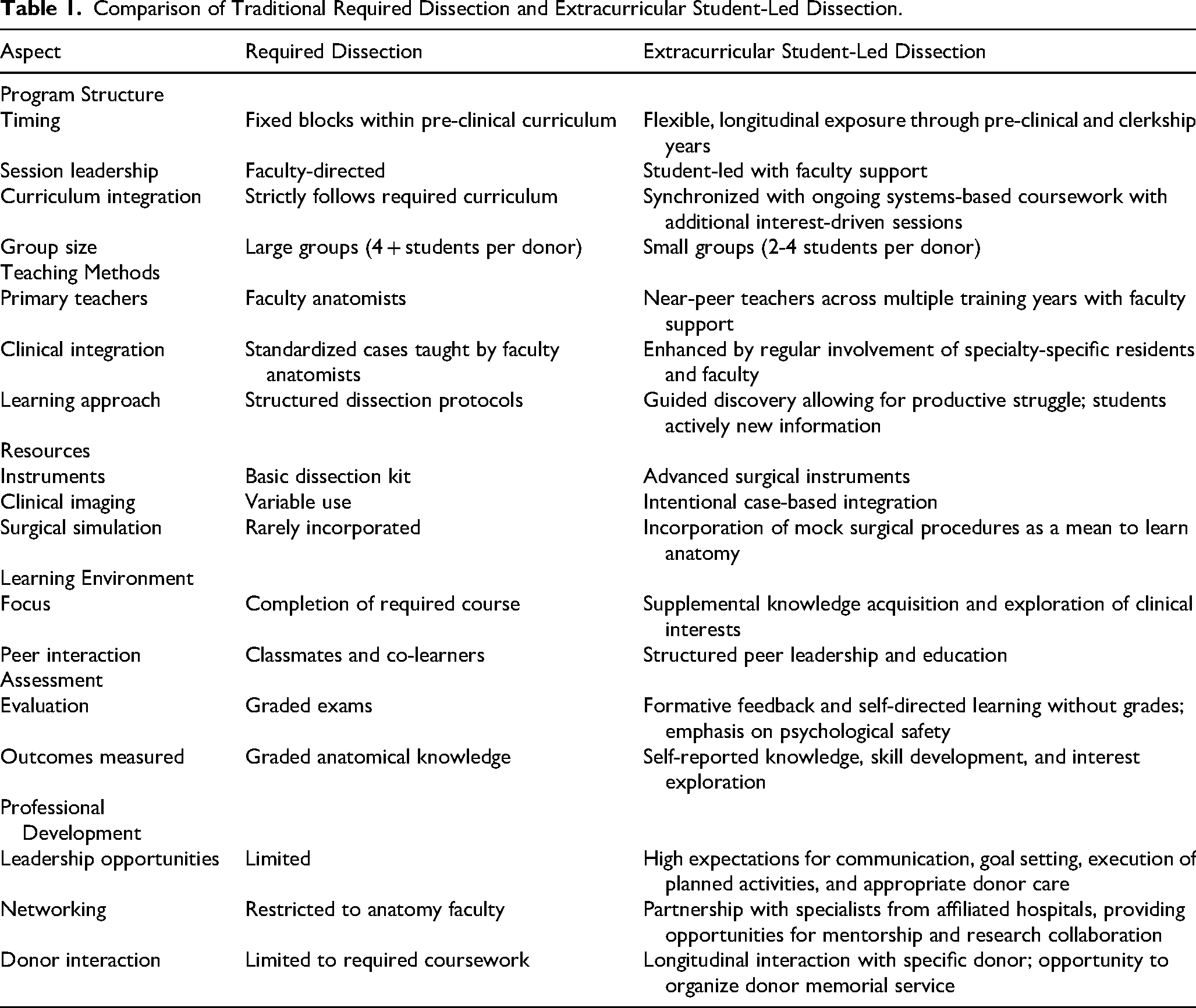
The following recommendations attempt to provide practical, actionable guidance on the design and implementation of extracurricular student-led study of anatomy. The steps are not intended to be sequential; it is most efficient, and indeed imperative, for many of them to occur in parallel. These recommendations incorporate the necessary personnel (i.e., student leadership, near-peer teachers, faculty, and human body donors), the pedagogical approaches involved in establishing and improving the student-led curriculum (i.e., motivation theory, productive struggle, and continuous improvement), and specific components of the program (i.e., semesterly schedule, case-based dissection, and practice with surgical instruments) key to the successful implementation of a student-led dissection experience. Each recommendation is paired with an example(s) embodying the experience of the authors at Harvard Medical School. Table 1 compares our novel approach to extracurricular dissection to the traditional model of anatomical dissection required by many pre-clinical curricula. While there is no single anatomy curriculum shared across all institutions, we have summarized common characteristics of required dissection as described in the literature.
Comparison of Traditional Required Dissection and Extracurricular Student-Led Dissection.
Engage Early with New Learners
When first-year students arrive at campus, there is an opportunity to capture their excitement and energy; they are often eager for experiences such as dissection or clinical observation that go beyond the biochemistry and physiology they learn in their pre-clinical curriculum. Early engagement provides an opportunity to emphasize the value of voluntary and ungraded student-led dissections that offer autonomy and self-direction that they will not often encounter in required coursework or on licensing exams.31–34 Furthermore, pre-clinical curricula are increasingly graded on a pass/no pass basis, allowing students to spend more time engaging in extracurricular pursuits such as research, volunteer, work, and extracurricular experiences. 5
We recommend introducing first-year medical students to dissection early upon arriving at campus by introducing the student organization at their first anatomy lecture and soon after hosting a dissection event aimed specifically at first-year students. Within the first month of class, it is beneficial to invite students to the anatomy lab to learn laboratory basics, emphasizing safe handling of dissection instruments and the development of basic dissection skills.
Our first dissection was the femoral triangle, which is an appropriate first dissection for several practical reasons. First, the structures are large, sturdy, and relatively easy to identify. This provides students an opportunity to familiarize themselves with the general gross appearance of arteries, nerves, and veins before progressing to finer dissection of smaller anatomy. Secondly, students can work on the bilateral extremities in tandem, effectively doubling our donor-to-student ratio and capacity for hands-on learning. Goals for these dissections include demonstrating safe handling of dissection instruments (scalpel, forceps, and scissors), defining the boundaries of the femoral triangle (inguinal ligament, sartorius muscle, and adductor longus muscle), and identifying the neurovascular structures within the femoral triangle (femoral artery, nerve, and vein, as well as lymphatic vessels and lymph nodes).
Create a Dissection Schedule That Builds upon the Required Curriculum and Incorporates Student Interests
Most pre-clinical medical curricula follow a systems-based approach that provides an excellent framework for anatomical exploration. By synchronizing the dissection schedule with their classroom experience, students can integrate their learning with hands-on applications without experiencing additional cognitive load. 35 In this model, consistent with cognitive load theory, students collaboratively explore the region of interest and use their collective reasoning to investigate the most difficult concepts as identified by faculty and previous student leaders. 36 Moreover, many dissections should ideally occur over several weeks, allowing students to practice spaced repetition and further reinforce anatomical education outside the bounds of the preexisting curriculum. 37
Students may also benefit from dissections that go beyond the scope of the pre-clinical curriculum, allowing them the opportunity to explore clinical interests and challenging anatomic regions. At the beginning of the semester, group leaders met to discuss dissections scheduled for the upcoming months, including case-based dissections that parallel the ongoing pre-clinical curriculum as well as dissections that are independent from any required coursework. For the latter, anatomic regions for dissection were chosen based on student interest, as gaged by online surveys sent to the entire group, or because a student leader volunteered to lead a specific session based on personal interest. These sessions are enhanced by collaboration with clinical specialty interest groups who invite residents and attendings to share their expertise during dissection. Allowing students the opportunity to explore their interests in this way is incredibly valuable, but it must be balanced with the limited supply of human body donors and the special educational value of synchronizing dissection with the ongoing pre-clinical curriculum.
In a break from the pre-clinical curriculum and in response to student interest in orthopedic surgery, we performed a knee dissection in collaboration with the orthopedic surgery interest group and several orthopedic surgery residents from our affiliated hospitals. The session included a case-based discussion of anterior cruciate ligament (ACL) injury and reconstruction, with special focus on identifying the ACL and structures suitable for use in reconstruction (patellar ligament, hamstring tendon, quadriceps tendon).
Table 2 demonstrates an example schedule that includes dissections related to the required curriculum and specialty-specific dissections driven by student interest.
Example Schedule for the Spring Semester. Dissections that align with the required pre-clinical curriculum are shaded gray. Other dissections were chosen by student interest and involved house staff from the relevant specialty. Student leaders are identified by their initials and are included in the authorship of this article or acknowledged as contributors.

Utilize Near-Peer Teaching
The utility of near-peer teaching (NPT) in the context of anatomy education is well documented, with authors often highlighting the development of students as teachers in addition to improving the experience of first- and second-year learners.38,39 Though NPT within a required curriculum is well established, we propose that NPT in a voluntary context offers additional value.
Consistent with contemporary motivation theory suggesting that students are motivated when they feel a sense of autonomy and competence, offering student leaders the opportunity to take greater responsibility and to be recognized for their contributions motivates them to invest additional time and energy into dissection. 40 More senior students who elect to participate in dissection beyond their first year of medical school are encouraged to learn alongside their first-year peers; they instruct as they proceed with their own dissection, identifying gaps in their existing knowledge and adding to it with new experiences. More senior students offer important connections to scenarios they have encountered in the wards and operating rooms, which is often illuminating for pre-clerkship students eager for learning about the clinical relevance of anatomical knowledge. For every dissection, a NPT should be designated to fulfill several logistical responsibilities: preparation of any necessary special equipment (eg, rib cutters for thorax dissection), presentation of the dissection approach (ie, skin incision, target structures, and structures at risk of damage), and supervision of proper donor care and laboratory clean up.
NPT is also essential to the logistics of an extracurricular anatomy group because they allow guided dissection to occur outside of required class times (eg, in the evenings or on weekends) without putting undue burden on anatomy faculty. In addition, having students from multiple classes is necessary to coordinate across different schedules and design dissections appropriate for students of all levels.
Near-peer teachers should be selected by anatomy faculty and senior medical students involved in the extracurricular study of anatomy. We suggest a written application that includes questions related to the applicants’ interests, commitment, and plans. This selection process identifies NPTs who are passionate about anatomy, knowledgeable of a variety of anatomic regions, and committed to learning alongside their peers. We also recommend an in-person group discussion of the group's interests and goals that involves experienced student leaders, new student leaders, and anatomy faculty members.
Why do you want to lead this group? If given the opportunity to lead any dissection, what would you choose and why? What specialties are you considering at this stage of your education? Are you able to commit to approximately four hours of dissection per week?
NPTs were selected by senior students based on answers to the written application. We prioritized building a leadership team with enthusiastic students with varied clinical interests, understanding that these interests will evolve over time.
Integrate Course Content and Structure Dissection with Clinical Vignettes
Case-based learning models are ubiquitous in medical education, including the study of anatomy, and allow students to apply medical knowledge to clinical scenarios they will encounter on the wards.41,42 Student-led elective dissections should revisit cases from the ongoing pre-clinical curriculum, which provide important clinical context for dissection. The clinical vignette serves as a scaffold for understanding anatomical structures relevant to patients they may encounter in the clinic, in the hospital, or on exams.35,43 We recommend trying to incorporate a case-based approach to dissection sessions when possible, maintaining the overall focus on anatomical learning. Student leaders should identify cases appropriate for dissection in collaboration with faculty based on student interest, relevance to the pre-clinical curriculum, and availability of donors. Student leaders, serving as NPTs, are encouraged to take the lead in presenting cases to learners. They are responsible for revisiting and expanding upon cases studied in the classroom, or using patients they encountered in the clinical setting to create new cases.
Incorporate Clinically Relevant Imaging
Imaging studies are also an important consideration in choosing appropriate cases to accompany dissection. As radiologic imaging techniques have evolved to be more effective, affordable, and expedient, physicians in all specialties must be able to identify normal and abnormal anatomical structures as they are seen on CT, MRI, bedside ultrasound (US), and other modalities. Incorporating imaging studies into anatomy education is well established and has been shown to enhance students’ learning.44–46 We found it valuable to incorporate imaging studies into our dissections to both enhance the dissection experience and to improve proficiency in interpreting radiologic studies. For imaging studies such as CT and MRI, it is important for students to actively scroll through the complete series of cross-sectional images to build a three-dimensional understanding of anatomy, as passively showing a critical finding on a single slice of an MRI is less effective for both teaching anatomy and for building radiologic proficiency. 47
Reviewing imaging studies before and during dissection, even though the images do not reflect the exact anatomy of the donor, also prepares students for the hospital wards, where imaging studies often provide the basis for clinical decision-making. Consideration should be given to the use of imaging studies of known provenance, provided by patients with their consent, as is often the case in teaching hospitals. Other resources such as Radiopaedia, a peer-reviewed open-edit radiology resource, are well-suited for this purpose, though the provenance of the images is not easily discernable. 48
We recommend that student leaders have relevant imaging studies on computers positioned near the dissection stations before the start of the session. NPTs should review the imaging study with the group before beginning dissection, highlighting important structures that students will identify during dissection. Learners should revisit the imaging studies during dissection to better understand anatomic relationships and to guide dissection.
Use Clinically Relevant Surgical Tools and Materials
We sought to perform dissections and mock procedures with techniques that closely resemble those that students will encounter in the operating room. 49 This often requires using surgical instruments beyond forceps and scissors. Retired surgical instruments and expired suture from affiliated hospitals prevent waste and allow students to name and use instruments such as Metzenbaum scissors, DeBakey forceps, Kelly clamps, Weitlaner retractors, Army-Navy retractors, and linear staplers, which are frequently used in surgery. Students should be resourceful when finding materials for dissection: ask anatomy faculty what tools are available, partner with surgical faculty to obtain expired or reusable equipment from the hospital, and use available funding to purchase expired materials when they are unavailable from affiliated hospitals. Learning how to handle instruments safely and effectively with faculty supervision will build practical skills in spatial cognition and manual dexterity that will benefit them in the operating room and in other procedural contexts. Table 3 summarizes the instruments most used during dissection as well as special equipment used for certain dissections.
Surgical Instruments Used in Dissections And/Or Surgical Simulations.

In addition to using and maintaining proper care of surgical instruments, learners can also model best practices in care for the body donors during and after each dissection period. This includes handling the donors with respect, always wearing gloves when handling donors, maintaining appropriate temperature and humidity conditions, preventing any unnecessary damage or contamination, and leaving the laboratory space clean and orderly. Good donor care foreshadows good patient care.
Foster a Safe Learning Environment That Encourages Productive Struggle
Student leaders should be responsible for determining not only the goals of the session but also how to get there: where to incise the skin, what structures to identify, and how to troubleshoot. This can be uncomfortable for students early in their medical training. Student leaders can identify resources within the laboratory workspace, including textbooks, online resources, and near-peer teachers, and encourage their classmates to take advantage of these options before seeking assistance from faculty. Struggling through a dissection can be uncomfortable but productive, allowing students to identify structures with both their eyes and hands and to gain problem-solving skills that are otherwise difficult to simulate. 36 Students become self-sufficient in dissection only after a period of productive struggle. 50 To this end, we cannot understate the importance of establishing a culture of consistency and sustained effort: demonstrate enthusiasm, be welcoming and inclusive, and congratulate students’ progress.
Establishing psychological safety is crucial to creating an environment for students to learn and grow. 51 Students report significant stress in response to dissection of human bodies, regardless of whether sessions are faculty or student-led, often verbalizing a connection between making mistakes in dissection and wasting the generous gift of donors. 52 Faculty and NPTs should emphasize that it was the expressed wishes of the donors to have medical students learn from them, and that by participating in sessions like these, they are making the most of the body donors’ generous gifts. When mistakes inevitably arise, student leaders should be vocal in providing support; giving examples of our own mistakes and lessons learned led to a tight-knit, supportive community of learners. Furthermore, given students’ various backgrounds and experiences prior to dissection, it is important to assess individual and group needs when providing student support. Emphasizing the active positive role students can take in good donor care can be helpful here, as well as other strategies cited in the literature, which include written reflections, modules on the history and ethics of anatomy, and elective life-body drawing. 51
The structure you’re looking for isn’t where you expected it to be; what structures are you seeing and where should you look next? What spacial relationships are guiding you? What type of structure do you think you are feeling (e.g., vessel or nerve)? Based on this, do you think you need to protect it or is this connective tissue that you can dissect bluntly? Can we use an image or drawing to help us determine what structure we are seeing?
Measure Student Satisfaction, Academic Performance, and Interest in Surgical Specialties
To develop an effective dissection program, educators must assess students' subjective experiences with dissection activities. Understanding these perceptions is essential for enhancing program quality and adapting curricula to meet students' evolving educational needs.53,54 This can be accomplished by developing surveys and facilitating group discussions. To date, we have not formally collected data on students’ experience, though informal feedback has been uniformly positive. In addition to studying students’ reaction to the dissections, it would be beneficial to measure objective learning outcomes such as student performance on anatomy practical exams, pre-clinical test scores, or clerkship evaluations. Student-reported experience measures and objective learning data regarding dissection may have notable ceiling effects, as learners who choose to engage in optional dissection may already enjoy and excel in anatomy. Similarly, early opportunities to practice technical skills in surgery have been shown to improve student performance on their surgery rotations, 55 though it is likely that students motivated to participate in dissections are also motivated to perform well on their surgery clerkship. Finally, students often change career preferences throughout medical school. 56 As these experiences evolve, it will be important to examine the influence of early procedural exposure in the context of anatomical dissection on students’ ultimate choice of medical specialty. These data can help better quantify the effect of dissection on the retention of anatomical knowledge and identify areas for improvement in the anatomy curriculum.
Consider Formalizing Anatomical Dissection as an Optional Longitudinal Course
While we maintain that there is an important role for extracurricular self-guided study of anatomy, medical schools could consider formalizing supplemental dissection experience as a longitudinal elective course. This would improve access to faculty who could guide specialty-specific dissections, increase funding for surgical materials (eg, instruments, implants, suturing material), and validate the efforts of involved students (ie, on residency applications). We propose a year- or semester-long elective course in which students meet for 2–4 hours weekly to perform advanced dissection and mock surgeries with faculty guidance at an earlier point in their medical curriculum. This structure has been useful for other longitudinal courses such as courses in medical education, medical device innovation, and medical languages.57,58
Honor the Donors and Their Invaluable Gift to Medical Education
Whole body donors serve as medical students’ first patients or “silent teachers,” who in death remain deserving of respect, care, and meticulous attention.59,60 For many learners, donors are their first up-close encounter with death and dying, grounding them in the complex ethical and emotional demands of the profession.61–64 Apart from the regular duties of appropriate and respectful donor care in the laboratories, it has become common practice for medical students to organize an annual donor memorial service or ceremony of appreciation to honor those who donated their bodies to medical education.65–67 The event may include written reflections, poetry, musical performances, visual art, or other expressions of gratitude, responsibility, and growth. A supplemental anatomy curriculum is only possible because of the generosity and selflessness of donors, and students who choose to engage in additional study of anatomy should express special gratitude for those who make it possible.
I am in awe of our donors for their selflessness and commitment to medical education. Sometimes during a dissection, I linger on a donor's military tattoo or ruby red painted fingernail and wonder what lessons they learned in the course of their life. I hope that they know, somehow, just how much their gift means to me.
Generalizability
The specific examples described in these ten recommendations are based on the authors’ experience at Harvard Medical School, an institution with extensive financial resources, specialized anatomy faculty, affiliations with large hospital systems, and a robust Anatomical Gift Program. We recognize that these resources may not be readily available at other medical schools. The underlying principles and strategies we present, however, can likely be adapted at all institutions. The emphasis on student-led dissections, integration of clinical data, and fostering independence are fundamental approaches that can be implemented in various educational settings. However, smaller medical schools may need to adjust their strategies to account for limited resources, such as by partnering with nearby institutions or leveraging digital tools to supplement hands-on learning experiences. Ultimately, the goal is to create a rich and engaging environment for studying anatomy that equips learners with the knowledge and skills necessary for a successful medical career.
Discussion
The recent trend away from anatomical dissection in medical education raises concerns that medical students may graduate with inadequate anatomical knowledge, limited skills in handling surgical instruments, and inadequate experience with the ethical and humanistic considerations of the profession as required by working with human bodies in life and death.4,6,7,15,18,22 The proposed supplemental anatomy curriculum addresses these concerns and aligns with broader trends in medical education that emphasize the importance of active learning, clinical integration, NPT, and student-centered approaches.32,38,41,42
This initiative also builds on a growing body of work supporting the efficacy of peer-assisted learning in medical education. Medical students benefit from NPT, which is most relevant for practical skills. (REF) In anatomy specifically, peer-led programs have been implemented successfully in both gross anatomy and neuroanatomy, helping to create learning environments that promote student autonomy, collaboration, and deeper understanding of anatomical relationships (REF). Our model expands this literature by describing a longitudinal, dissection-based, student-run initiative with dedicated peer leadership and a clinical and practical emphasis.
Forming and maintaining a supplemental anatomy curriculum depends on the involved students’ motivation to learn anatomy. Contemporary motivation theories highlight several concepts essential to initiating and continuing goal-directed activities, including self-efficacy, autonomy, perceived value of the task, short- and long-term goals, affective response, and an intrinsic interest in gaining knowledge and skills. 40 By providing students with opportunities for self-directed learning and leadership, a supplemental anatomy curriculum develops autonomous learners and allows students to make progress on their individual goals. This is particularly important in the context of busy pre-clinical curricula and competitive residency applications on the horizon. Not all students will elect to participate in anatomical dissection, instead choosing to invest time in research, community engagement, early clinical experience, or other pursuits. We maintain that there is a desire and a need for additional study of anatomy that can best be addressed in a student-led, collaborative learning environment.
The value of integration of clinical vignettes and imaging studies in the study of anatomy is well documented. Encouraging medical students to generate or adapt these cases themselves introduces an added layer of active learning that promotes synthesis of knowledge. This approach helps students—both as first-time learners and as near-peer teachers—connect their anatomical knowledge to real-world clinical scenarios, improving their understanding and retention. Additionally, the use of clinically relevant surgical tools and materials provides students with practical, tactile experience that can be applied in future clinical settings.
The curriculum also addresses the ethical and emotional dimensions of anatomy education. Students who elect to participate in elective dissection spend far more time with donors than their peers, and by doing so they learn important lessons in empathy, responsibility, and professionalism. By emphasizing the importance of caring for and honoring donors, as well as creating a psychologically safe learning environment, the authors recognize that anatomy is more than just a subject to be studied; it is a deeply personal and meaningful experience. 68
We recognize there are limitations to our program and to our recommendations. Although our program is intentionally student-driven, there are logistical considerations that require faculty involvement. Depending on institutional policy, varying degrees of faculty oversight will likely be required to implement extracurricular study of anatomy effectively, from supervision in the laboratory space or to troubleshooting complicated dissections. This voluntary contribution would likely be in addition to other responsibilities within the anatomy curriculum, medical school, or clinical department for faculty anatomists.
Laboratory resources—namely whole body donors—are typically used as much as possible to maximize education for medical students and trainees at affiliated medical centers. This can present challenges with donor availability for extracurricular dissection, as institutions are unlikely to have additional donors readily available solely for this purpose. Student-led extracurricular dissection may also raise unique ethical considerations regarding donor intent and appropriate supervision, even if the intent is to magnify the impact of the donors’ gifts. It is therefore paramount that students recognize the immense privilege of working with the donors in this manner. We maintain, however, that with active leadership by experienced medical students and clear faculty-student communication, these challenges can be surmounted, thus increasing the magnitude of donors’ gift to future generations of physicians and improving learners’ experience with anatomic education.
While our program offers a promising approach to anatomy education, it is important to note that further research is needed to evaluate its effectiveness. Studies should examine the impact of extracurricular study of anatomy on student learning outcomes, their satisfaction with the program, and their career choices. Additionally, exploring the long-term effects of this approach on the development of clinical skills and knowledge would be valuable.
The supplemental anatomy curriculum presented in this paper represents an opportunity to fill an emerging gap in undergraduate medical education. By incorporating evidence-based strategies from the literature on NPT, active learning, and experiential anatomy instruction, it complements traditional curricula and meets the needs of contemporary learners. By emphasizing student motivation, clinical relevance, NPT, and the ethical dimensions of anatomy learning, this initiative contributes to the growing literature on active, student-centered approaches to medical education and offers a flexible, scalable model for institutions seeking to enrich their anatomy instruction.
Conclusion
As medical schools transition away from required dissection-based anatomy curricula, student-led dissection opportunities have proven valuable for medical students across class years. These experiences offer irreplaceable tactile knowledge and problem-solving skills that digital resources cannot replicate, while maximizing the generous gift of body donors and fostering collaboration with surgical departments. Our student-led dissection experiences have been intellectually stimulating and rewarding for all participants.
We call upon medical educators and institutions to develop curricula supporting student-led anatomical exploration with appropriate ethical oversight. We also encourage students passionate about deepening their anatomical knowledge to advocate for these experiences. Through either formal integration into existing curricula or clear guidelines for self-directed learning, expanding access to dissection experiences both honors donor legacy and equips future clinicians with essential anatomical knowledge and reasoning, preserving an invaluable and historic component of medical education.
Footnotes
Acknowledgments
We thank fellow student leaders Lois Owolabi, Donald Fejfar, Michelle Bosche, Matt Knerr, Valeria Robayo, Zoe Ingram, and Massoud Sharif for their outstanding contributions to the Harvard Medical School Student Anatomy Team. We are grateful to Cynthia McDermott for sharing her exceptional knowledge and skills throughout our student-driven anatomical dissections. We also express our unwavering gratitude to the donors and their families for their support of our medical education.
Ethical Considerations
There are no human participants in this article and informed consent is not required.
Author Contributions
EKW, JG, and SM cofounded the Harvard Medical School Student Anatomy Team and continue to lead anatomical dissections. EKW and KF conceived of the presented manuscript. EKW wrote the manuscript with support from JG. KF and SH provided important guidance on literature review. All authors provided critical feedback and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Notes on Contributors
Ellery Koelker-Wolfe, BA, Justin Gelman, BS, and Stephen Moye, BS, are fourth-year medical students at Harvard Medical School. Together they cofounded the Harvard Medical School Student Anatomy Team and continue to serve on the organization's leadership council. Their clinical interests include obstetrics/gynecology, anesthesiology, and orthopedic surgery, respectively.
Dana Stearns, MD, is an assistant professor of Emergency Medicine and Surgery at Massachusetts General Hospital. He also serves as the faculty director of Anatomy Education for the Pathways Curriculum for the Program in Medical Education at Harvard Medical School.
Sabine Hildebrandt, MD, FAAA, is a researcher and associate professor of pediatrics at Boston Children's Hospital, Harvard Medical School. She teaches anatomy and history and ethics of anatomy at Harvard Medical School and Harvard College. She serves as associate editor of Anatomical Sciences Education for the areas of history and ethics.
Dennis Cullinane, PhD, is the co-director of the Anatomy Curriculum Theme for the Program in Medical Education at Harvard Medical School.
Krisztina Fischer, MD, PhD, MMSc, is an assistant professor in Radiology at the Brigham and Women's Hospital, Harvard Medical School, Boston, MA, US. She is also the faculty director of the Master of Medical Sciences in Medical Education Program at Harvard Medical School.