
Abstract
Objectives
Antibiotic resistance threatens global health, underscoring healthcare students’ critical role in mitigation efforts. This study evaluated their knowledge, attitudes, and practices toward antibiotic resistance and use.
Methods
A validated, self-administered, paper-based questionnaire was developed following an extensive literature review and administered to final-year medical, dental, Pharm D, and pharmacy students at the University of Jordan from October 2022 to March 2023.
Results
Descriptive, nonparametric, and logistic regression analyses were conducted on 263 eligible questionnaires. Students demonstrated adequate knowledge (4.30/5) and positive attitudes (4.19/5), but poor practices (4.78/6). Most felt responsible for resistance (89.73%) and reported efforts to combat self-medication (77.95%). However, irresponsible antibiotic use was noted (78.33%). Females scored higher in practice (5.29) than males (4.70, P = 0.01). Students using leftover antibiotics had lower attitudes (3.50) than those who obtained antibiotics via prescriptions (4.25) or directly from pharmacies (4.55). Enrollment in pharmacy and dental majors increased the odds of inadequate knowledge (P = 0.004) and poor practices (P = 0.02), respectively. Positive attitudes significantly predicted adequate knowledge (P < 0.001) and good practices (P = 0.001).
Conclusions
Knowledge and practices varied across healthcare majors, highlighting educational gaps. Systematic interdisciplinary clinical exposure paired with periodic discussions could enhance interprofessional knowledge sharing, inform decision-making, and foster trust between disciplines. Male students’ poorer practices may stem from an unmet need for career-oriented education that aligns with their career trajectories; incorporating internships could improve their engagement to education and prudent behaviors. Despite limitations in generalizability and potential sampling bias, these findings align with existing literature, suggesting relevance beyond the study sample.
Keywords
Introduction
Antibiotic resistance is accelerating at an alarming rate, and the prevalence of resistant bacterial pathogens threatens the efficacy of existing antibiotics. 1 Antibiotic-resistant infections have spread globally, 1 with approximately 700,000 annual deaths attributed to multidrug-resistant infections, 2 with severe consequences including prolonged hospitalizations, higher mortality rates, and increased reliance on costly second- and third-line treatments. This demand has led to shortages of essential antibiotics and rising healthcare costs. 3 In the healthcare sector, antibiotic resistance is fostered by the overuse and misuse of antibiotics and poor infection control.4,5 Complex scientific, economic, and licensing factors pose additional barriers to antibiotic development and innovation. 6 For instance, antibiotic discovery faces lengthy preclinical assessments, high costs, and low success rates, as only 1 in 15 preclinical candidates achieves approval. 7 Even approved antibiotics often lose efficacy within 2–3 years due to rapid resistance emergence. 7 Nontraditional approaches are prioritized, yet deemed insufficient by the World Health Organization.5,7 Currently, only 6 of 27 antibiotics in clinical trials against priority pathogens demonstrate true novelty in chemical class, target, mechanisms of action, or cross-resistance.7,8 Hence, many countries have developed National Action Plans (NAP) to delay crises or reduce their impacts. 9 Furthermore, the WHO finalized a global development and stewardship framework based on a tripartite collaboration between the Food and Agriculture Organization and the World Organization for Animal Health, which aims to preserve existing antimicrobials while developing and distributing new quality antimicrobial medicines, vaccines, and diagnostics. 10
Strengthening the healthcare system involves a set of essential pillars: infection prevention and control (IPC), patient and medicine safety, and antimicrobial stewardship (AMS). 11 The latter aims to optimize antimicrobial use regarding indication, drug choice, dosing, duration, and route while ensuring sustainable access to quality healthcare. 12 Healthcare providers serve as essential frontline stewards in the fight against antibiotic resistance. They fulfill this critical role by appropriately prescribing antibiotics based on their specialized knowledge and expertise. Additionally, they educate their patients about the proper use of these medications. 12 Furthermore, the education and training of healthcare students, including primary and continuous training, are among the core elements of AMS. 13
In the Middle Eastern and North African (MENA) region, several NAPs have been developed to tackle antibiotic resistance. 9 Despite their presence, studies have highlighted inadequate implementation due to insufficient AMS education and training among healthcare professionals14–17 and the public.18–20 Furthermore, the implementation of Universal Health Coverage (UHC), which implies the full coverage and continuum of timely access to affordable and geographically accessible quality healthcare, is also a burden in many countries across the region.21,22
Jordan's NAP
Jordan is a lower-middle-income country located in the Eastern Mediterranean region. 23 According to national mortality statistics from 2018, communicable diseases (including maternal, perinatal and nutritional conditions) represented Jordan's second leading cause of death (n = 1145), with respiratory tract infections (RSTIs) accounting for 45.2% of these fatalities (n = 518). 24 In alignment with global efforts and national priorities to address communicable diseases, Jordan has implemented an NAP to combat antimicrobial resistance (AMR). The 2018–2022 NAP identified critical gaps, including insufficient public awareness campaigns, inadequate training for healthcare providers, and weak enforcement of AMR-related policies. 25 To address these challenges, the 2023–2025 monitoring and evaluation plan, through a One Health approach, focuses on expanding public awareness initiatives, strengthening AMS programs, improving IPC measures, and reinforcing governance. 26 The existing literature underscores the urgency of these measures, particularly the need for improved AMS education and training among healthcare professionals,27–30 and for better implementation of AMS to ensure the adherence to Jordan's NAP.27,28,30
Health education research to curb antibiotic resistance
Since healthcare students are the future gateway keepers against antibiotic resistance, ensuring their optimal education and adherence to AMS principles is paramount. Therefore, several studies have been conducted worldwide to assess healthcare students’ knowledge, attitudes, and practices related to antibiotic resistance and antibiotic use.31–34 To the best of our knowledge, no study has conducted a comparative assessment of final-year healthcare students undergoing the critical transition into the workforce, a phase that imposes additional psychological burdens, 35 with comprehensive assessments based on subgroup differences, particularly in the MENA region, where evidence indicates inappropriate antibiotic use among healthcare providers. By adopting a comparative approach, this study aims to formulate targeted recommendations that foster equitable educational and professional opportunities across healthcare disciplines. These findings provide critical insights into subgroup differences among healthcare students that may shape their contributions to antibiotic resistance. Identifying gaps in knowledge, attitudes, and practices enables formulating evidence-based recommendations for curricular improvements, contributing to global efforts against antibiotic resistance.
This study explored medical, dental, Pharm D, and pharmacy students’ knowledge, attitudes, and practices related to antibiotic resistance and use in Jordan, examined their associations by sociodemographic characteristics and patterns of antibiotic use, and explored potential predictive factors for antibiotic use.
Methods
Study design and setting
A cross-sectional survey-based design was used to collect data from final-year medical, dental, Pharm D, and pharmacy students at the University of Jordan, a public institution in Amman, the capital of Jordan, and its affiliated teaching hospital, Jordan University Hospital. During the 2022–2023 academic year, the university enrolled 46,590 undergraduate students.
Population and sample
The target population comprised final-year students specializing in medicine, dentistry, Pharm D, and pharmacy at the university. No exclusion criteria were applied, and final-year students were selected because they have acquired nearly all the theoretical and practical antimicrobial knowledge necessary for transitioning into the workforce. Thus, the study findings would reflect their behaviors as future healthcare professionals, making curricular recommendations most relevant at this stage.
According to the University of Jordan's Admission and Registration Unit, the number of final-year students in medicine, dentistry, Pharm D, and pharmacy was 411, 167, 132, and 172, respectively. Males comprised 33.12% of the total population, distributed as follows: 47.93%, 29.30%, 17.42%, and 19.05% across these majors.
Although proportional stratified sampling was initially considered to ensure representative subgroup distribution, its implementation was not feasible due to time constraints and limited research staff. Consequently, a convenience sampling approach was employed within each stratum. Despite this limitation, efforts were made to maintain representativeness by stratifying participants by academic major and utilizing faculty assistance to facilitate recruitment.
The sample size was calculated from a population of 882 students based on the multivariate analysis of variance (MANOVA): Global Effects using a priori G*Power software (G*Power Software for Windows, Kiel, Germany). 36 The analysis was performed to compare students’ knowledge, attitudes, and practices across four study majors using a medium effect size of f 2 (V) = 0.0625, power of 0.8, and type-1 error (α) of 0.05. A proportion of 20% was added to the estimated sample size of 88, yielding a total of 106 to account for expected incomplete reporting, data loss, or other study-related issues. The number of participants in each stratum was determined based on their proportions in the target population, with medical, dental, Pharm D, and pharmacy students representing 46.60%, 18.93%, 14.97%, and 19.50% of the sample, respectively.
Study instrument
Two experts in public health developed the questionnaire following an extensive literature review of similar published studies that assessed the knowledge, attitudes, or practices related to antibiotic resistance and use. The literature search was confined to articles with questionnaires published in English in PubMed and Scopus. The items were supplemented by additional insights drawn from authoritative public health sources such as the Center for Disease Control.28,37–46 Only pre-validated questionnaires were included in the synthesis of questionnaire items, and the study authors developed additional items to suit the study population and objectives. The questionnaire consisted of four sections: knowledge (10 items), attitudes (eight items), practices (seven items), and sociodemographic characteristics (15 items).
The first section, “knowledge,” contains questions assessing students’ ability to define antibiotic resistance (items 1 and 2), their agreement on specific factors related to antibiotic use that are associated with resistance (items 3 to 7), and their understanding of the possible consequences related to antibiotic resistance (items 8 to 10). Answers were based on a five-point Likert agreement scale, with scores ranging from 1 (strongly disagree) to 5 (strongly agree). Three negative items (4, 5, and 9) were reverse-coded.
The second section, “attitudes,” contains questions exploring students’ views on the narrowing pipeline of antibiotic development (item 1), their attitudes toward factors related to antibiotic use that are associated with resistance (items 2 to 7), and their sense of responsibility in influencing antibiotic resistance (item 8). Answers were based on a five-point Likert agreement scale, with scores ranging from 1 (strongly disagree) to 5 (strongly agree), while item 3 was reverse-coded.
The third section, “practices,” investigates students’ behaviors related to their preference for antibiotic use in specific scenarios (items 1 and 2), the execution of their role in influencing the judicious use of antibiotics among their friends, families, and community (items 3 to 6), and their behaviors following knowledge gained on antibiotic resistance (item 7). The answers were based on a six-point Likert frequency scale, with scores ranging from 1 (never) to 6 (always). Negative items (1, 2, and 4) were reverse-coded.
The fourth section, “sociodemographic characteristics,” includes questions about a respondent's gender, income, major, paternal education, maternal education, having relatives working in healthcare, and their use of antibiotics in the past year.
Cut-off values of the knowledge, attitude, and practice mean scores
The Knowledge, Attitude, and Practice outcome variables were dichotomized using an 80% threshold of the total possible scale scores. 47 For knowledge and attitude assessments (5-point Likert scales), scores ≥4 (80% of 5 points) were classified as indicating adequate knowledge or positive attitudes, respectively. The practice scale (6-point Likert scale) used a cutoff of ≥4.8 (80% of 6 points) to define good practices. The minimum possible score was 1 and the maximum was 5 for both knowledge and attitude scales, while the practice scale ranged from a minimum of 1 to a maximum of 6.
Validity and reliability assessment of the questionnaire
The draft questionnaire was submitted to a panel of four family and community medicine and community health nursing experts at the University of Jordan to verify face and content validity. Based on constructive feedback, minor rewordings and amendments to scale items were made. The questionnaire's reliability and internal consistency were evaluated through a pilot study involving 30 participants within the same sampling frame, analyzed using SPSS (version 20). 48 The average time for questionnaire completion was 11 min. Cronbach's alpha values of 0.710 (knowledge) and 0.756 (attitudes) indicated high reliability. Given these robust consistency metrics, the pilot data were retained in the final analysis to maximize statistical power and maintain sample representativeness.
Data collection procedure and ethical considerations
Data were collected between October 2022 and March 2023 following approval from the Institutional Review Board (IRB) of the University of Jordan (Approval No. 101-2022) using self-administered, paper-based questionnaires.
Initial in-person data collection involved researchers directly approaching students in faculty buildings and hospital wards, with hospital-based recruitment conducted exclusively outside clinical sessions. However, the response rate was suboptimal due to participants’ demanding schedules. To improve participation, the administrative faculty provided formal support by:
Facilitating access to academic schedules: (including faculty-based and hospital-based lectures), ensuring data collection did not interfere with clinical training; Identifying mixed-cohort lectures: (eg, lectures attended by Pharm D/pharmacy students or by fourth-/fifth-year cohorts); and, Advising on optimized screening protocols during these lectures, where students were instructed to self-report their academic level and major on top of questionnaires, an approach that ensured only eligible final-year participants were included.
The research objectives, ethical considerations, and principal investigators’ contact details were clearly outlined in the informed consent form and through verbal communication from the research team. All participants provided verbal consent after reviewing written study information, with questionnaire return constituting final consent. During the 10- to 20-min data collection window, participants could withdraw freely. Strict anonymity was maintained (no identifiers collected). Participation was entirely voluntary, with no impact on academic standing or incentives offered, and only principal investigators collected completed questionnaires. All data collected remained secure and accessible exclusively to the research team.
Statistical analysis
The paper analyzes the associations between three endpoint variables (knowledge, attitudes, and practices) against a set of candidate determinants (ie, sociodemographic characteristics and patterns of antibiotic use in the past year). The data were analyzed using SPSS software version 20. 48 P values <0.05 were considered significant (with 95% confidence intervals [CI], two-tailed). Univariate descriptive frequency statistics were employed using counts and percentages. While in the bivariate analysis, inferential nonparametric Mann–Whitney U and Kruskal–Wallis tests were employed to assess associations between mean score outcome variables and candidate determinants, given the non-normal distribution of mean score outcome variables (Shapiro–Wilk test: (knowledge (P < 0.001), attitudes (P < 0.001), and practices (P < 0.001)). When the analyses showed significant associations, pairwise post hoc comparisons were performed using the independent samples Kruskal–Wallis one-way ANOVA test (significance level is at Adjusted P values <0.05, two-tailed). Mean scale variables were summarized with medians and interquartile ranges (IQR) in the bivariate analysis. In the univariate analysis, however, means and standard deviation (SD) were more informative, given the categorical nature of the raw data.
Significantly associated determinants were entered into the multivariate logistic regression analysis to control for confounding (enter model). Multicollinearity in each regression model was ruled out based on variance inflation factors below 2. Notably, variable categories pertaining to the source of antibiotics used in the past year were combined into “medical prescription” and “other” to address the very low sample sizes obtained in specific categories.
Handling missing values
In the total sample of 263 students, there were 15 cases with missing values in the knowledge ordinal constructs (5.70%), 4 in the attitude constructs (1.52%), and 3 in the practice constructs (1.14%). When calculating mean scores, missing values were imputed by series means using SPSS. 48 A sensitivity analysis was conducted to assess the potential bias arising from this method. This involved replacing the missing values in constructs with extreme upper-limit and lower-limit values, and then conducting bivariate and multivariate analyses for each resulting mean. The results were consistent with the original findings of this research, except for the association between “course completion” and “students’ practice mean scores”, which became statistically insignificant. However, this finding was discussed in the context of existing literature.
Results
Response rate
Of the 315 questionnaires distributed, 263 were considered eligible for inclusion, yielding a response rate of 83.49%. The ineligible questionnaires (52 respondents) were mainly collected from lectures that included students from different academic majors or levels at the faculty of pharmacy, having students from outside the target population. With data saturation achieved, the final study sample comprised 263 final-year students, distributed as follows: 56 medical (21.29%), 58 dental (22.05%), 89 Pharm D (33.84%), and 60 pharmacy students (22.81%).
Baseline characteristics
The majority of respondents were female (78.91%), with female distribution across majors as follows: 14.06% in medical, 17.58% in dental, 28.52% in Pharm D, and 18.75% in pharmacy programs. Also, 94.33% of students fell within the 20 to 25-year-old age group, and 39.53% reported having a family member working in the healthcare field, of whom 13.31% were medical healthcare professionals. Over the past year, 125 students (60.98%) had used antibiotics; 92.56% completed the treatment course, and 72.95% used antibiotics based on a medical prescription (Table 1).
Sociodemographic characteristics of last-year healthcare students at The University of Jordan, October 2022–March 2023 (N = 263).

Tawjihi: The General Secondary Education Certificate Examination in Jordan.
Knowledge, attitudes, and practices of healthcare students
Knowledge
Table 2 shows the mean knowledge score of students is adequate: 4.30 (0.54) out of 5 (cut-off value at score ≥ 4), The highest mean knowledge scores were demonstrated for items 1 (4.61 (0.81)) and 2 (4.78 (0.62)), which assess students’ ability to define antibiotic resistance. However, the lowest mean scores were seen among items underpinning students’ understanding of specific factors associated with antibiotic resistance.
Students’ answers to knowledge items related to antibiotic use and resistance, October 2022–March 2023, Jordan (N = 263).
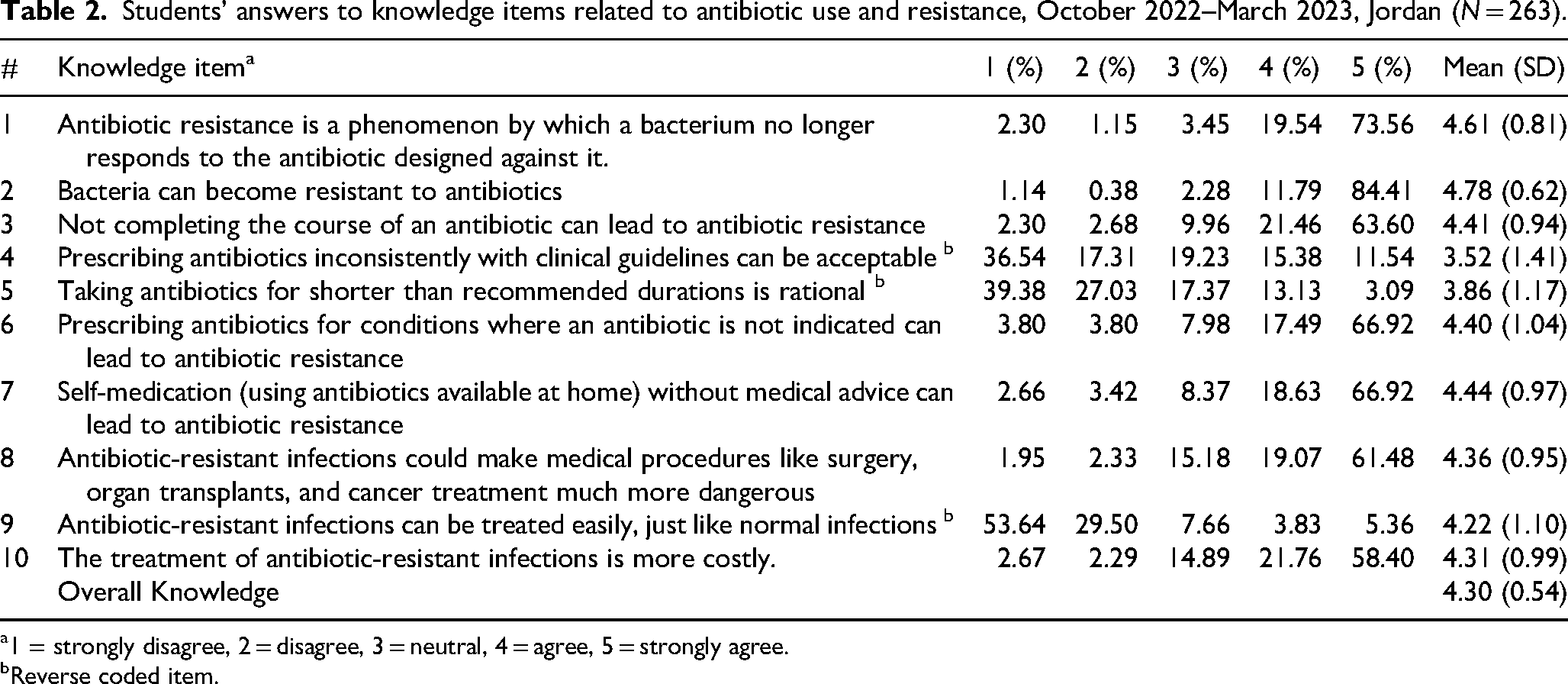
1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
Reverse coded item.
Attitudes
Table 3 shows that students demonstrated an overall positive attitude with a mean score of 4.19 (0.53) out of 5 (cut-off value at score ≥ 4). The highest attitude mean score (4.60 (0.79)) was observed for the item assessing students’ sense of responsibility in influencing antibiotic resistance. In contrast, the lowest mean score (3.48 (1.09)) was for the item concerning the narrowing pipeline of antibiotic development.
Students’ answers to attitude items related to antibiotic use and resistance, October 2022–March 2023, Jordan (N = 263).

1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
Reverse coded item.
Practices
Table 4 shows that students exhibited poor overall practices with a mean score of 4.78 (1.10) out of 6 (cut-off value at mean scores ≥ 4.80). Students demonstrated the highest practice mean score (5.11 (1.33)) for the item investigating the impact of knowledge gained about antibiotic resistance on the frequency of prudent practices. However, the lowest mean score (4.41 (1.49)) was observed for the item assessing the frequency of using antibiotics in the presence of cough and sore throat.
Students’ answers to practice items related to antibiotic use and resistance, October 2022–March 2023, Jordan (N = 263).

1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = most, 6 = always.
Reverse coded item.
Relationships between students’ knowledge, attitudes, and practices and their sociodemographic characteristics and patterns of antibiotic use in the past year
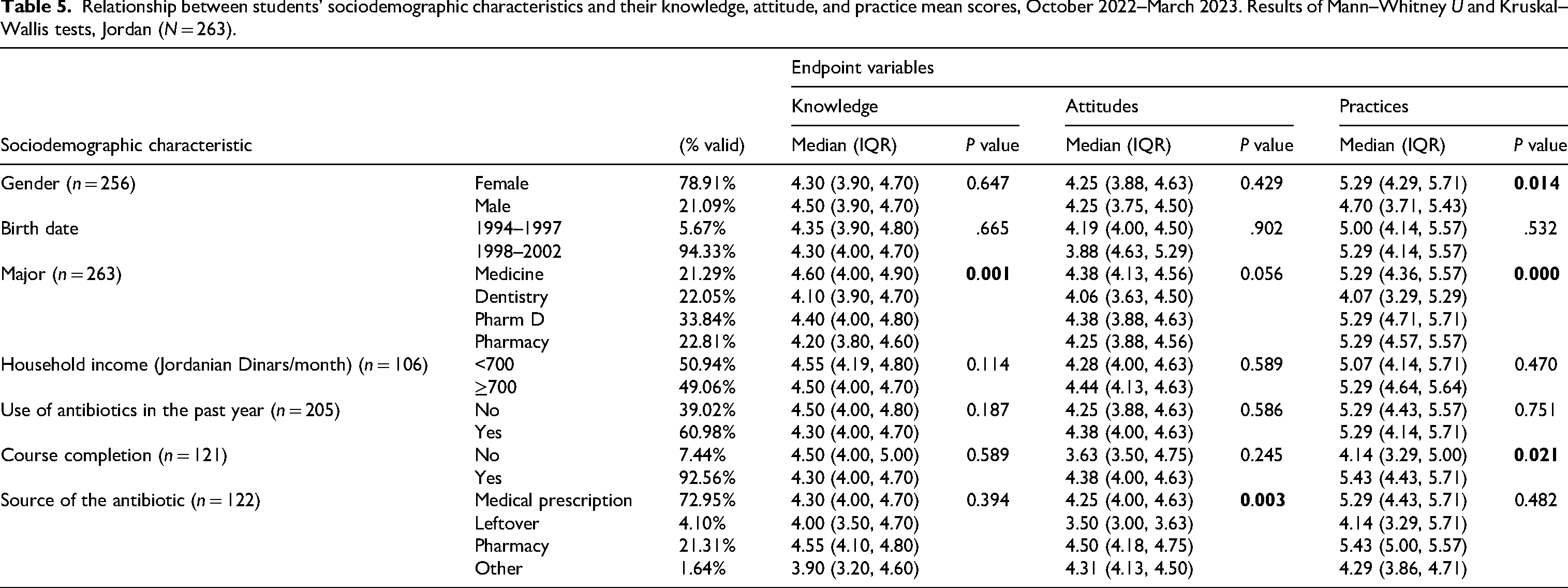
Mann–Whitney U and Kruskal–Wallis analyses were conducted to explore the associations between students’ knowledge, attitude, and practice mean scores and their sociodemographic characteristics and patterns of antibiotic use in the past year (Table 5). The Kruskal–Wallis test showed a statistically significant association between students’ knowledge and their major (P = 0.001). Post hoc pairwise comparisons revealed that medical students reported higher knowledge scores (4.60 (4.00-4.90)) than pharmacy students (4.20 (3.80-4.60), P = 0.001) and dental students (4.10 (3.90-4.70), P = 0.05). Also, post hoc pairwise comparisons showed that significantly lower attitude scores were found among students who used leftover antibiotics at home (3.50 (3.00-3.63)) compared with those who bought antibiotics directly from the pharmacy (4.50 (4.18-4.75), P = 0.001) or based on a medical prescription (4.25 (4.00-4.63), P = 0.01). Based on the Mann–Whitney U test, significantly higher practice scores were found among females (5.29 (4.29-5.71), P = 0.01) and among students who completed the course of antibiotics used in the past year (4.14 (3.29-5.00), P = 0.02). Post hoc analyses found that dental students reported significantly lower practice scores (4.07 (3.29-5.29)) than Pharm D (5.29 (4.71-5.71), P < 0.001), pharmacy (5.29 (4.57-5.57), P = 0.004), and medical students (5.29 (4.36-5.57), P = 0.02).
Relationship between students’ sociodemographic characteristics and their knowledge, attitude, and practice mean scores, October 2022–March 2023. Results of Mann–Whitney U and Kruskal–Wallis tests, Jordan (N = 263).
Predictors of knowledge, attitudes, and practices
In Table 6, the multivariate logistic regression results show, after adjusting for confounding factors, that having positive attitudes significantly increases the odds of having adequate knowledge (odds ratio [OR] = 4.56, 95% confidence interval [CI] 2.35-8.85, P < 0.001) and good practices (OR = 3.67, 95% CI 1.67-8.03, P = 0.001). Furthermore, pharmacy students had the lowest likelihood of adequate knowledge (OR = 0.25, CI 0.10-0.65, P = 0.004). Dental students had the lowest likelihood of good practices (OR = 0.33, CI 0.13-0.84, P = 0.02).
Multivariate logistic regression of factors predicting Students’ knowledge, attitudes, and practices related to antibiotic resistance and use, October 2022–March 2023, Jordan (N = 263).

The cut-off point for adequate knowledge is at mean scores ≥ 4.00 of 5; knowledge is considered deficient at values < 4.00 of 5.
The cut-off point for positive attitudes is at means scores ≥ 4.00 of 5; attitudes are considered negative at values < 4.00 of 5.
The cut-off point for good practices is at mean scores ≥ 4.80 of 6; practices are considered poor at values < 4.80 of 6.
No regression analysis was conducted between the two variables due to the lack of significant associations found based on nonparametric analyses.
Discussion
In this study, we investigated the knowledge, attitudes, and practices regarding antibiotic resistance and use among final-year medical, dental, Pharm D, and pharmacy students in Jordan. As future healthcare professionals, comparing these student groups may be a reference for future curricular enhancement.
Students’ knowledge, attitude, and practice scores
Analyses of the overall mean scores and distributions revealed that students had adequate knowledge and positive attitudes toward antibiotic resistance and use, but poor practices. The study found that 84.41% of students understood that unnecessary antibiotic prescriptions contribute to resistance, and a substantial proportion (89.73%) believed in their role in mitigating antibiotic resistance. These sentiments were highlighted in their practices, as most students frequently made efforts to protect their family and friends from antibiotic resistance (76.80%), persuaded their community not to self-medicate (77.95%), and informed them about the risks associated with irresponsible antibiotic use (78.33%). Furthermore, 57.03% of students reported that they never stopped taking antibiotics when their symptoms disappeared. Similarly, a study from Jordan reported that 61.0% of undergraduate Pharm D and pharmacy students always completed the entire course of treatment. 33 Despite these promising findings, only 28.52% and 25.86% of the students reported rarely using antibiotics for cough or sore throat, respectively, indicating the need for curricular advancements for RSTIs.
RSTIs
Regional and global patterns of inappropriate antibiotic use
Inappropriate antibiotic use for RSTIs is prevalent across the Middle East and globally. In the Middle East, two multicountry cross-sectional online surveys found inappropriate antibiotic use for RSTI indications; one observed such behaviors in around half the sample of medical students, while the other observed them in approximately a quarter of a sample of multi-level pharmacy and Pharm D students.46,49 Similarly, a multicenter study in Saudi Arabia found that around a quarter of a sample of fourth-year to sixth-year dental students and interns would prescribe antibiotics for viral infections, a practice linked to gaps in knowledge that improved with academic seniority. 50 In the global context, findings from Nepal found that almost half the sample of multilevel medical and dental students also self-medicated with antibiotics for the treatment of sore throat, accompanied by a runny nose. 51 On the contrary, A multicenter cross-sectional report found that only 8% of Colombian medical students regard antibiotics as the first-line agents in cough and sore throat, highlighting regional disparities influenced by healthcare education and policies. 31
Healthcare policies and legal frameworks
The effectiveness of antibiotic stewardship programs is intrinsically linked to national regulatory frameworks, with significant variations observed across countries. In Nepal, unregulated antibiotic dispensing has led to widespread self-medication practices, exacerbating antimicrobial resistance. 52 In contrast, both Saudi Arabia and Colombia implemented stringent regulatory measures in 2018, including prescription-only antibiotic access, comprehensive public awareness campaigns, and strict penalties for violations such as pharmacist license suspension or termination.53,54
Nevertheless, surveys in these two countries showed heterogeneous prescribing behaviors,31,50 suggesting variability in policy enforcement or the depth of educational interventions. For example, a Saudi study found that while 75% of students were aware of antibiotic resistance, only 54.7% understood its public health threat. Crucially, this deeper awareness was associated with nearly double the reduction in antibiotic misuse (51.32%) compared to basic awareness alone (27.96%). 55
Jordan's regulatory landscape and challenges
Jordan faces significant antibiotic misuse, driven by systemic gaps identified in its 2018–2022 NAP, including weak policy enforcement, insufficient healthcare training, and limited public awareness. 25 A retrospective analysis of 92,968 family medicine clinic visits (2017) revealed that antibiotics constituted 25% of all prescriptions, with 51.13% for RSTIs, yet only 28.8% were clinically justified. 27 This aligns with broader regional trends and underscores Jordan's urgent need for in-depth awareness interventions that influence collective behavioral change to mitigate antibiotic resistance within the sheets of society.
Students’ perceptions of educational influences on their practices
Educational interventions emerged as a critical but underutilized tool for improving AMS. Only 59.32% of our sample highly credited the impact of academic input on influencing their practices, a proportion similar to that from a survey of fourth-to sixth-year medical students in Warsaw (53.40%), which also indicated educational insufficiencies. 56 Curricular advancements should focus on exploring root causes that drive inappropriate behaviors, as this would likely prevent their persistence in future clinical practice. Qualitative assessments from Egypt, Spain, and Norway revealed that fear of negative therapeutic consequences contributes to inappropriate antibiotic use among healthcare practitioners,57–59 especially when a past traumatic outcome triggers these feelings. 58 To mitigate this, healthcare education must strike a balance between rigorous therapeutic training and psychological support, empowering them to navigate clinical decisions safely and effectively, especially given the high mortality rates associated with these infections. 24
Associations between baseline characteristics and mean knowledge, attitude, and practices
Gender disparities in education
In terms of sociodemographic characteristics, gender disparities were evident in this sample, with males disproportionate to the target population (21.09% in the sample compared to 33.12% in the population), particularly in the medical and dental majors (35.71% and 21.05%, respectively). Medical students may be absent due to elective rotations outside the country, making their exact representation uncertain. However, the disproportion among dental students might reflect lower engagement in education and attendance among males, which aligns with their reduced engagement in prudent antibiotic practices observed in this study. Our analysis also revealed that females exhibited significantly higher practice mean scores than males (P = 0.01). These findings align with Saudi Arabian, Middle Eastern, and Serbian surveys of healthcare students.49,60,61 In contrast, multicountry Asian and Sudanese surveys reported higher knowledge scores among male pharmacy students, potentially due to sampling biases favoring female participation.62,63
Social identity attributes provide additional insights into gender differences in academic engagement. An analysis of the Add Health dataset, 64 which tracked 20,000 adolescents until their early adulthood, found that gender gaps in attitudes are predicted by males’ perceived ‘attainable’ social identity. 65 Male students had substantive lower aspirations of attaining college, despite expressing their desire, making them less likely to enroll. These aspirations are strongly linked to male students’ social identities, suggesting that so-called “behavioral deficits” are, in fact, a consequence of an undermined social identity quest. Although the study differs in terms of age and academic discipline, its findings align with another analysis of large-scale international surveys and statistical reports,66–68 which suggests that standardized education models across genders may not sufficiently accommodate diverse learning needs across genders, and that directly addressing males’ academic weaknesses may be less effective than creating opportunities to capitalize on their strengths and interests. 69 One proposed solution is career-oriented internships, as exemplified by the University of Jordan's School of Pharmacy, which leverages stakeholder networks to provide internships across various pharmacy sectors. 70 Such experiential learning opportunities may help reduce gender disparities in both education and practice by aligning educational structures with students’ aspirations and career trajectories.
Use of antibiotics within the past year
Regarding antibiotic use in the past year, 72.95% of students used prescribed antibiotics, aligning with findings from Serbia (71.5%) 71 and Mali (81.2%) 72 among medical students. The latter study also found that self-medication was more prevalent among senior students and indicated deficient overall knowledge that may underpin overconfidence. 72 In addition, pairwise post hoc comparisons found that students who used leftover antibiotics at home had significantly lower positive attitude scores than students who bought antibiotics using a medical prescription (P = 0.01) or from the pharmacy (P = 0.001). Conversely, a Serbian study among final-year medical and nonmedical students found no association. 71 A multicenter survey among Sudanese medical students found that self-medication is inversely associated with academic year advancements and income level. 73 The latter is unsurprising given that income can facilitate access to timely and quality medical care that is affordable and geographically accessible, according to the principles of the UHC. 21 This is particularly relevant in Sudan's urban areas, where 61.80% of the population lives in poverty, driving reliance on pharmacies for self-medication due to financial, geographical, and time barriers to quality healthcare access. 74 Thus, public health policies addressing self-medication require a nuanced approach considering sociodemographic indicators, ensuring that interventions do not unintentionally marginalize disadvantaged populations from essential healthcare services.
Multivariate regression analysis
Discordance between knowledge and practice
Multivariate logistic regression analysis revealed that positive attitudes predicted adequate knowledge and good practices. However, adequate knowledge was not a predictor of good practices. This discordance is well-documented in the literature.75–77 Hence, tackling practices is better achieved by addressing attitudes and vice versa. The following paragraphs discuss how training enhancements, including early, hands-on, case-based theoretical, and interdisciplinary clinical training, might address these incompetencies. For instance, a cross-sectional survey in Colombia found that medical students who perceived their training as excellent had significantly higher knowledge, attitude, and practice scores. 31 Training enhances students’ competence by fostering critical thinking, decision-making, and interpersonal relationships, while enabling them to handle attitudinal factors (eg, fear and anxiety) prudently.78,79
Interprofessional gaps across healthcare disciplines
Medical students
Medical students achieved the highest median scores in knowledge (4.60 [4.00-4.90]), attitude (4.38 [4.13-4.56]), and practice (5.29 [4.36-5.57]), likely due to their rigorous training. At the University of Jordan, medical students undergo 40 weeks of annual clinical training starting in their fourth year, with specialty systems beginning as early as the second year.80,81 This aligns with findings from Egypt, where medical students demonstrated superior knowledge and lower self-medication rates. 76 Similar trends were observed in Colombia. 31 However, discrepancies exist in the literature. For instance, Polish medical students showed knowledge-attitude gaps, possibly due to including junior students. 56 Conversely, in Bangladesh, seniority inversely correlated with knowledge and attitudes, 77 a pattern likely influenced by context-specific systemic barriers, including inadequate IPC infrastructure (eg, clean water access), financial strains 77 (eg, high out-of-pocket costs accounting for 44.31% of healthcare expenditures), and antibiotic market dynamics ($45.08 M in Q2 2022).82,83 Such infrastructural and economic barriers may hinder optimal antibiotic practices, warranting further policy research on these linkages.
Pharm D and pharmacy students
This study found that pharmacy students were less likely to have adequate knowledge (P = 0.004). Notably, pharmacy students, unlike other students in the sample, lacked clinical training in hospital wards or outpatient clinics. Furthermore, while pharmacy and Pharm D students share foundational coursework in Therapeutics and pharmacy field training, their career pathways diverge substantially: Pharm D students receive extensive clinical training focused on patient management, including specialty clerkships during their sixth year, 84 while pharmacy students concentrate on pharmaceutical sciences and dispensing. 85 This curricular divergence likely explains pharmacy students’ inferior antibiotic stewardship knowledge versus Pharm D peers and other healthcare students.
Our finding contrasts with a multicountry Middle-Eastern survey that found an increased likelihood of adequate knowledge among pharmacy students compared to Pharm D students. Nevertheless, the study employed a different cut-off categorization and included students from all academic years. 49 In fact, surveys in Cyprus and Spain found that medical students demonstrated significantly higher knowledge of pharmacological agents 34 and antibiotic resistance 86 than other healthcare students, likely due to their infectious disease training. 86 However, pharmacy students excelled in understanding antibiotic effectiveness for specific microbes, 34 highlighting the need to integrate theoretical education with practical training for optimal competency.
The literature reported variable knowledge levels among pharmacy students, ranging from deficient62,87 to adequate, 88 and curricular enhancements have been recommended for pharmacists62,87,88 and healthcare students in general. 89 Structured clinical exposure would reinforce pharmacy students’ theoretical knowledge. The University of Toronto provided a successful example of how early, experiential clinical training, with consistent feedback, can enhance hands-on experience and decision-making skills, leading to informed prescribing practices. 78 In Jordan, Pharm D programs have begun implementing simulation labs for clinical training; 90 moreover, pharmacy students would benefit from incorporating case-based theoretical learning, expanded clinical placements, and standardized AMS modules.
Dental students
Our findings also revealed that dental students had significantly lower odds of demonstrating good antibiotic prescribing practices (P = 0.02). This aligns with global literature highlighting gaps in their education and training, including: The need for further education on antibiotic use and resistance,91,92 limited confidence,91,93 deficits in interdisciplinary training, 94 and in managing pediatric endodontic infections. 95 These professional gaps may stem from curriculum limitations inherent in traditional dental education, which maintains a strong oral health focus while providing less emphasis on systemic pharmacological principles and AMS.
A multicenter cross-sectional survey in Saudi Arabia found that dental interns exhibited poor prescribing behaviors, particularly for systemic conditions. 50 Furthermore, a scoping review on the challenges of dental education found that students rarely receive adequate performance assessments during interdisciplinary training. 94 Interdisciplinary cooperation is influenced by social dynamics, acting as either an opportunity for interprofessional learning or a barrier when peer pressure and hierarchy interfere. 96 A collaborative learning environment mimicking real-world clinical challenges can prepare students across disciplines to integrate, developing new insights while blending their knowledge. The variability of healthcare professionals’ knowledge and experience backgrounds may drive them to perceive prudent practices differently. 18 Therefore, standardized interdisciplinary education on antibiotics for all healthcare students would enhance decision-making and mutual understanding. 97
Growing evidence highlights the effectiveness of interprofessional educational workshops,97,98 e-learning modules, 99 and teamwork and knowledge sharing in enhancing AMS and healthcare outcomes. 100 At the university level, fostering interfaculty collaboration might provide valuable insights for curricular enhancement strategies, yielding better outcomes than isolated efforts. These collective efforts can focus on standardizing healthcare students’ core competencies, developing early, supervised, interdisciplinary clinical training in their syllabi to help them grow together and work together, and incorporating social support courses that emphasize the importance of solidarity and collaboration across healthcare disciplines, who are the building blocks of tomorrow's healthcare systems. 97
Limitations
This study has several limitations that should be considered when interpreting the findings. The primary limitation is potential sampling bias, particularly the underrepresentation of medical students (20.83% in the sample compared to 46.60% in the population). This discrepancy resulted from limited access to medical students relative to other healthcare student groups. However, the sample size was deliberately increased to account for subgroup differences.
Additionally, the survey-based cross-sectional design introduces the potential for self-reporting bias. This was partially mitigated by ensuring anonymous responses and triangulating data with existing literature. Furthermore, the questionnaire did not include items on students’ intravenous (IV) history or grade point average (GPA), both of which may influence knowledge, attitudes, and practices. However, given that students’ knowledge, an essential component of GPA, was discordant with their practices, attitudes may be a more significant predictor of behavior in this field.
Another limitation is the exclusion of nursing students, who play a key role in antibiotic administration and patient education. Additionally, the sampling frame was confined to final-year medical, dental, Pharm D, and pharmacy students at the University of Jordan, which may limit the generalizability of the findings. Nevertheless, the results align with broader literature, suggesting their relevance beyond this specific population.
Recommendations
A summary of recommendations based on key findings is presented in Table 7. In brief, the findings highlight students’ difficulties in translating knowledge into practice, underscoring the need for curricular improvements.
Summary of key recommendations based on major study findings.

Education
Public health policies
Research
Conclusion
This study highlights persistent gaps between healthcare students’ knowledge and clinical practices, calling for educational reforms: Early clinical rotations to bridge pharmacy students’ theory-practice divide, interdisciplinary training to strengthen dental competencies, and gender-responsive internships addressing male students’ educational needs and career aspirations. Standardizing AMS training through interfaculty collaboration and expanding partnerships between universities and the healthcare industry will develop a workforce capable of translating knowledge into practice.
Supplemental Material
sj-docx-2-mde-10.1177_23821205251344732 - Supplemental material for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study
Supplemental material, sj-docx-2-mde-10.1177_23821205251344732 for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study by Sara R. Homsi, Sireen M. Alkhaldi, Hana A. Taha and Zaid R. Homsi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251344732 - Supplemental material for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study
Supplemental material, sj-docx-4-mde-10.1177_23821205251344732 for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study by Sara R. Homsi, Sireen M. Alkhaldi, Hana A. Taha and Zaid R. Homsi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205251344732 - Supplemental material for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study
Supplemental material, sj-docx-5-mde-10.1177_23821205251344732 for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study by Sara R. Homsi, Sireen M. Alkhaldi, Hana A. Taha and Zaid R. Homsi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-sav-6-mde-10.1177_23821205251344732 - Supplemental material for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study
Supplemental material, sj-sav-6-mde-10.1177_23821205251344732 for Healthcare Students’ Knowledge, Attitudes, and Practices Related to Antibiotic Resistance and Use in Jordan: A Cross-Sectional Study by Sara R. Homsi, Sireen M. Alkhaldi, Hana A. Taha and Zaid R. Homsi in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We thank Dr Sireen Alkhaldi for the continuous guidance, support, and encouragement. The shared knowledge and expertise significantly contributed to the quality of this research. We appreciate the dissertation committee (Prof. Zeinab Hassan, Dr Lana Alhalaseh, and Dr Mamdouh El-Hneiti) for their valuable comments, insights, and guidance in improving and refining this work. The authors also acknowledge the editor and anonymous reviewers’ valued time, effort, and constructive feedback invested in the quality and depth of this manuscript. Authors deeply recognize the internal support provided by the University of Jordan faculties and staff, with special gratitude to Prof. Areej Othman, Prof. Mahmoud Alhussami, and Dr Hamza Alduraidi for their expertise and support during the validity assessment, as well as to Prof. Khawla Abu Hammour, Dr Dina Taimeh, Dr Bassam Amro, Prof. Ibrahim Al-Abbadi, Dr Oqba Al-Kuran, and Prof. Yusuf Al-Hiari for their support during data collection. We also thank Dr Nezar Al-Labadi for the valuable knowledge and expertise imparted and the statistical analysis of raw data. Acknowledgment is extended to Pharm D training supervisors for their help with data collection, and to all the students who participated in this study. We thank Elsevier Language Services for the English language editing of the manuscript. We used the STROBE cross-sectional checklist when writing our report. 101
This paper is dedicated to the memory of Prof. Mohammad Issa Saleh, whose commitment to research ethics deeply inspired me, in honor of his generous administrative guidance during data collection and technical support. His impact on my scientific journey continues to resonate.
Author Note
This paper has been edited in English by Elsevier Language Services.
Ethical Considerations
Ethical approval for this study was obtained from the University of Jordan IRB (Approval No. 101-2022, ref. 19/2022/549).
Consent to Participate
Informed consent was obtained verbally before participation.
Author Contributions
Sara R. Homsi: all tasks of research conduct and manuscript preparation. Sireen M. Alkhaldi: all tasks of research conduct and manuscript preparation. Hana A. Taha: questionnaire validation, writing—original draft, and writing—review and editing. Zaid R. Homsi: data collection, writing—original draft, and writing—review and editing. All authors have read the final manuscript draft and approved it for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.