
Abstract
Objectives
This study identified the prevalence of second victim experience (SVE) in a multidisciplinary sample of healthcare learners and explored personal experiences of trauma and desired forms of support following traumatic patient care events or situations.
Method
We used the validated SVE Support Tool-Revised and the Physician Well-Being Index (PWBI) to query healthcare learners at a large academic health system across the institution's medical, graduate medical education, and health sciences schools. The survey was open to all healthcare learners from April 8th, 2022 to May 30th, 2022. Here, we report on an analysis of respondents’ fixed responses describing the prevalence and characteristics of SVE.
Results
Of 2298 potential respondents, 206 answered at least one question (9.0% response rate). Of the 206 respondents, 205 answered questions inquiring if they had been a part of a stressful or traumatic patient care event or situation and 54.1% (111/205) answered in the affirmative. Of this group, 49.5% (51/103) reported feeling like a second victim (SV). The average PWBI of the exposed group was significantly higher (worse well-being) than the nonexposed group (3.4 vs 2.6, P = .0009). The most common forms of desired support for those exposed to a traumatic event and felt like an SV was conversation with peers 95.3% (41/43), family 81.4% (35/43), and a supervisor or manager 67.4% (29/43).
Conclusion
Findings suggest that many healthcare learners experience SVE and would benefit from connection to desired support strategies. Strategies to mitigate the impact of SVE on professional self-efficacy should be considered by education administrators. We present strategies from the literature and our institution that may be replicated for early identification and support of learners with SVE.
Introduction
The term “second victim (SV)” was coined by Wu in 2000 and encompasses psychological and physical symptoms that healthcare professionals (HCPs) experience after involvement in an adverse patient event.1,2 Since then, the term has gained international recognition and increasing scholarship relating to different medical disciplines and types of HCPs.2–4 Prior studies have focused on distinct sectors of the healthcare industry; few have examined the experiences of learners in a multidisciplinary context.2,5 While students and trainees have varying degrees of responsibility, studies on learners to-date suggest they are vulnerable to second victim experience (SVE), especially as it may be their first exposure to an adverse event or medical error.6,7 Compared to staff, learners were more likely to have experienced SVE in the previous 12 months. 7 Fear of consequences prevents medical residents from disclosing medical errors. 8 Several studies have focused on specific medical, nursing and pharmacy trainees while there is a gap in the literature with the experience of SVE of learners in different sectors of healthcare. Like nonlearners, conversations with peers after an event are strongly desired, however conversations with supervisors or preceptors play a larger role for trainees than with nonlearners.6,7 Involvement in adverse events is known to contribute to burnout and dropping out of the profession, 9 suggesting SVE should receive greater attention to its impact over a HCP's career, including during the formative period of medical education and training.
Fully understanding the prevalence and impact of SVEs in this population is important to those designing optimal learning environments. This has taken on greater relevance in the wake of COVID-19 and the evidence suggesting that learners were not exempt from its effects.10,11
We sought to identify the prevalence of SVE among diverse health care learners including those fields that have not been studied, such as perfusionists at a large teaching hospital by evaluating responses to validated instruments measuring professional and personal domains and current well-being status. The study also explored desired forms of support following involvement in traumatic patient care events or situations.
Materials and Methods
The study protocol, survey instrument, and informed consent materials were approved by the Mayo Clinic Institutional Review Board. The Mayo Clinic Institutional Review Board determined the study to be exempt (No. 21-010381). Mayo Clinic Education Research Committee provided additional review and approved distribution of the study among Mayo Clinic healthcare learners. The reporting of this study conforms to the STROBE statement 12 (Supplemental Table S6).
Study Setting
We utilized a cross-sectional survey design to query all healthcare learners at Mayo Clinic, a large multisite academic health system from April 8th to May 30th, 2022 to determine the prevalence and postevent experiences of SVE, including its impact on well-being and desired forms of support. The survey was fielded though Research Electronic Data Capture (REDCap) a secure, web-based platform used to collect and organize data. The anonymous online survey was distributed via an email with an individual link for all learners meeting inclusion criteria. Inclusion criteria for the survey included learners aged 18 or older, patient care experience, and enrollment in one of Mayo Clinic's 3 medical graduate programs: Mayo Clinic Alix School of Medicine, Mayo Clinic School of Graduate Medical Education, and Mayo Clinic School of Health Sciences. Participants were excluded from the survey invitation if they did not meet these criteria. The email invitation and beginning of the survey contained informed consent information. Respondents were informed in the email invitation and information at the beginning of the survey that by continuing with the survey they were providing written consent to have their anonymous results used for research. As responses were collected anonymously and the survey did not collect protected health information, Mayo Clinic Institutional Review Board approved this informed consent procedure. Implied written informed consent was obtained for all individuals who voluntarily completed the online survey. Responses are reported in aggregate to prevent identification of individual respondents.
Study Cohort
The survey was developed for learners of all healthcare programs with a minimum of 1-year clinical experience at Mayo Clinic. Mayo Clinic is a large academic teaching hospital and referral center that includes learners in all aspects of patient care. A system of graduated autonomy is inherent in all of its educational programs. As such, the learners surveyed ranged in clinical experience from those who are in their preclinical time to those who are about to graduate into autonomous practice. The respondents included medical students, postgraduate residents and fellows, and the School of Health Sciences which includes over 80 programs for various types of HCPs (full list available in Supplemental Table S1).
Survey Tool
The survey instrument consisted of 2 validated tools, the SVE and Support Tool-Revised (SVEST-R)13,14 and the Physician Well-Being Index (PWBI)15,16 as well as questions assessing participants’ knowledge of the term “second victim,” desired supports, and demographic questions tailored to the learner experience. The SVEST-R measures the positive and negative impact of medical errors and adverse patient events on HCPs. 14 The SVEST-R consists of 35-items within 9 categories: 7 dimensions (psychologic distress, physical distress, professional self-efficacy, supervisor support, colleague support, institutional support, resilience) and 2 outcomes (turnover intentions and absenteeism). 14 Good internal consistency is noted in the validation study for each psychosocial factor with Cronbach alpha scores ranging from .66 for colleague support to .86 for physical distress. 14 A 5-point Likert scale is used to rate these items from 1 (strongly disagree) to 5 (strongly agree). Higher mean scores indicate more SV responses, higher perceptions of inadequate support, and worse employment outcomes. Seven additional items queried different desired forms of support using a 5-point Likert scale of 1 (strongly do not desire) to 5 (strongly desire). Scores of 4 or greater were defined as desired. Responses to the SVEST-R were scored and presented according to published instructions. 14 The expanded PWBI has been validated to identify healthcare workers in severe distress using various dimensions including fatigue, depression, burnout, anxiety/stress, and mental/physical quality of life. 15 The WBI has been validated in numerous populations.16–19 During development of the PWBI, data from 2248 medical students generated a Cronbach's alpha of .68. 15 The 7 items in the PWBI were designed and validated against instruments measuring low mental quality of life, high fatigue, and recent suicidal ideation. The answers are scored as yes or no and a point awarded for each yes response. The mean score on the PWBI in a national sample of physicians was 1.85 (SD 2.74) where scores of ≥ 3 were associated with adverse outcomes such as increased suicidal ideation and burnout 16 A score of 4+ is considered “at risk” for medical students and a score of 5+ is considered “at risk” for residents/fellows.15,16
Statistical Analysis
A cross-sectional survey was conducted on the entire eligible population of healthcare learners where voluntary responses were collected. Based on a population size of 2298 healthcare learners, for a 95% confidence interval we would need 181 responses to obtain a margin of error of 7%. Standard descriptive statistics with frequency and percentages for categorical variables and means and standard deviations for the scores from the SVEST-R were utilized to summarize the data. A chi-square test or Fisher's exact test was used to compare the proportion of respondents in the 2 groups, where Fisher's was used if a cell count was 5 or less. Continuous comparisons between groups were evaluated using the 2-sample t-test. All responses were utilized that were provided, even incomplete cases. P-values <.05 were considered significant and all tests were 2 sided. Statistical analysis was performed using the SAS version 9.4 software package (SAS Institute, Inc.; Cary, NC). A separate qualitative analysis has previously been published describing the events that led to respondents’ SVE as well as their open-ended comments on their desired forms of support. 20 Here we describe statistical analysis of respondents’ fixed responses.
Results
Of the 2298 learners who received the survey invitation, 302 opened the REDCap link. Of those 302 learners who opened the link, 206 (68%) answered at least one question and were included for analysis (9.0% response rate). Of the 206 respondents that answered at least one question, one respondent did not answer any questions regarding participation in a traumatic event, leaving 205 respondents for part of the analysis.
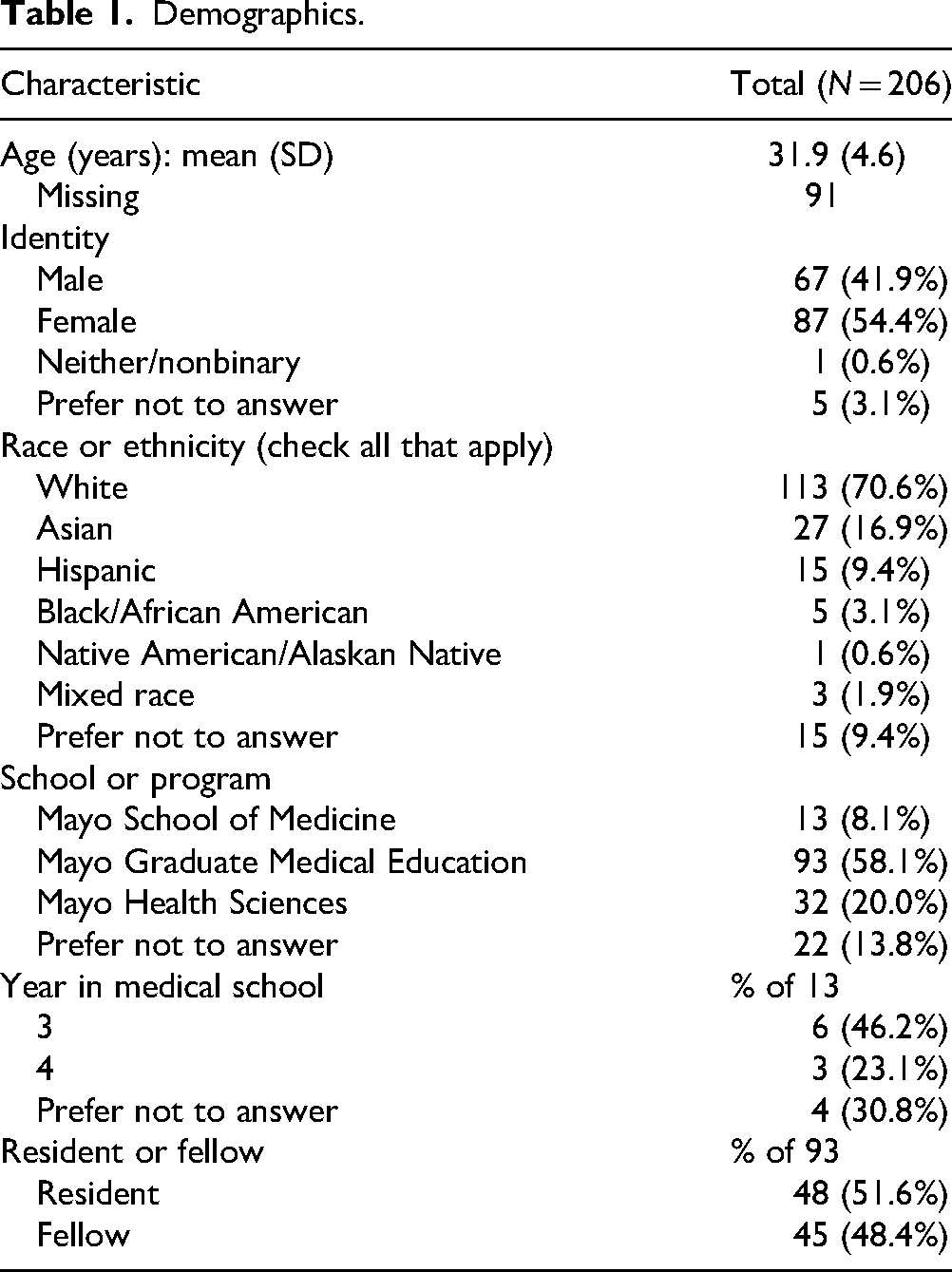
Demographics are presented in Table 1. Most participants identified as female and white. The largest category of respondents was residents and fellows accounting for 45% (93/206) of respondents. The highest response rate came from the School of Health Sciences with a rate of 15.3% (45/294), followed by medical students 8.8% (19/215), and residents/fellows at 6.2% (145/2323). Compared to the population within each learner group, respondents were slightly older (32 vs 29 years) and more likely to report their race as white (Supplemental Table S2).
Demographics.
SVE Among Learners
Prior to this survey, 31.6% (65/206) of respondents had heard of the term “second victim” with most becoming aware of the term in their current or prior education program (Supplemental Table S3). Of the 205 respondents that completed the first section of the survey which included the question regarding exposure to a traumatic care experience, 54.1% (111/205) reported that they had been a part of a stressful or traumatic patient care event or situation, while 45.9% (94/205) did not have this experience. Among participants who reported having been a part of a stressful or traumatic event, 49.5% (51/103) reported that they felt like an SV (Table 2). Learners from graduate medical education were more likely to identify as having had an SVE compared to those from the medical school or health sciences. Of those who identified as having had an SVE, 36.5% (19/52) of respondents indicated that they had considered leaving or left their position or role due to a traumatic patient care event.
Characteristics of Learners Identifying as Second Victims.

*Respondents could select more than one response.
All respondents who identified as being part of an adverse event or traumatic experience were prompted to complete the SVEST-R. For each measure of the SVEST-R, higher mean scores indicate more SV responses. The mean score on a 5-point scale of those respondents who self-identified as an SV were higher than those who did not identify as an SV on the domains of psychological distress (3.4 vs 2.4, P < .0001), physical distress (2.0 vs 1.7, P < .0001) and professional self-efficacy (3.1 vs 2.3, P = .001) (Table 3). Within the domain of professional self-efficacy, those who identified as an SV had higher mean score for feelings of inadequacy compared to those who did not identify as an SV 3.6 versus 2.8, P = .01 (Supplemental Table S4).
SVEST-R Dimensions and Outcome Variables of Second Victims.

SVEST-R, Second Victim Experience and Support Tool-Revised.
1Higher mean scores represent more second victim responses (eg, more psychological distress, less resilience), greater perceptions of inadequate support, and more second victim-related negative employment outcomes.
2The respondent's score for each factor was defined as the mean of 3 to 5 items each rated on a 5-point scale of 1 = strongly disagree and 5 = strongly agree. The second victim item was not answered by 1 of the 88 respondents.
3Two sample t-test.
4Missing value N = 1 for no.
5Missing value N = 4, N = 2 for yes.
All respondents, regardless of whether they had been part of a stressful or traumatic event, were asked about methods used to cope with a difficult patient situation. Following an adverse event, the top 3 support mechanisms selected by those who felt like an SV included conversations with peers 95.3% (41/43), family 81.4% (35/43), and supervisors or managers 67.4% (29/43) (Supplemental Table S5). When asked about desired support following a future traumatic event, the top 3 items on a Likert scale of 1 to 5 of those who identified as SVs (43/82) were the same as those who did not identify as an SV (38/79) and included a peer to discuss the event (4.5 vs 4.2, P = .15), taking time away from their unit (4.2 vs 4.1, P = .14), and counseling via an employee assistance program (3.8 vs 3.7, P = .38) (Table 4).
Desired Support of Learners Identifying as Second Victims.
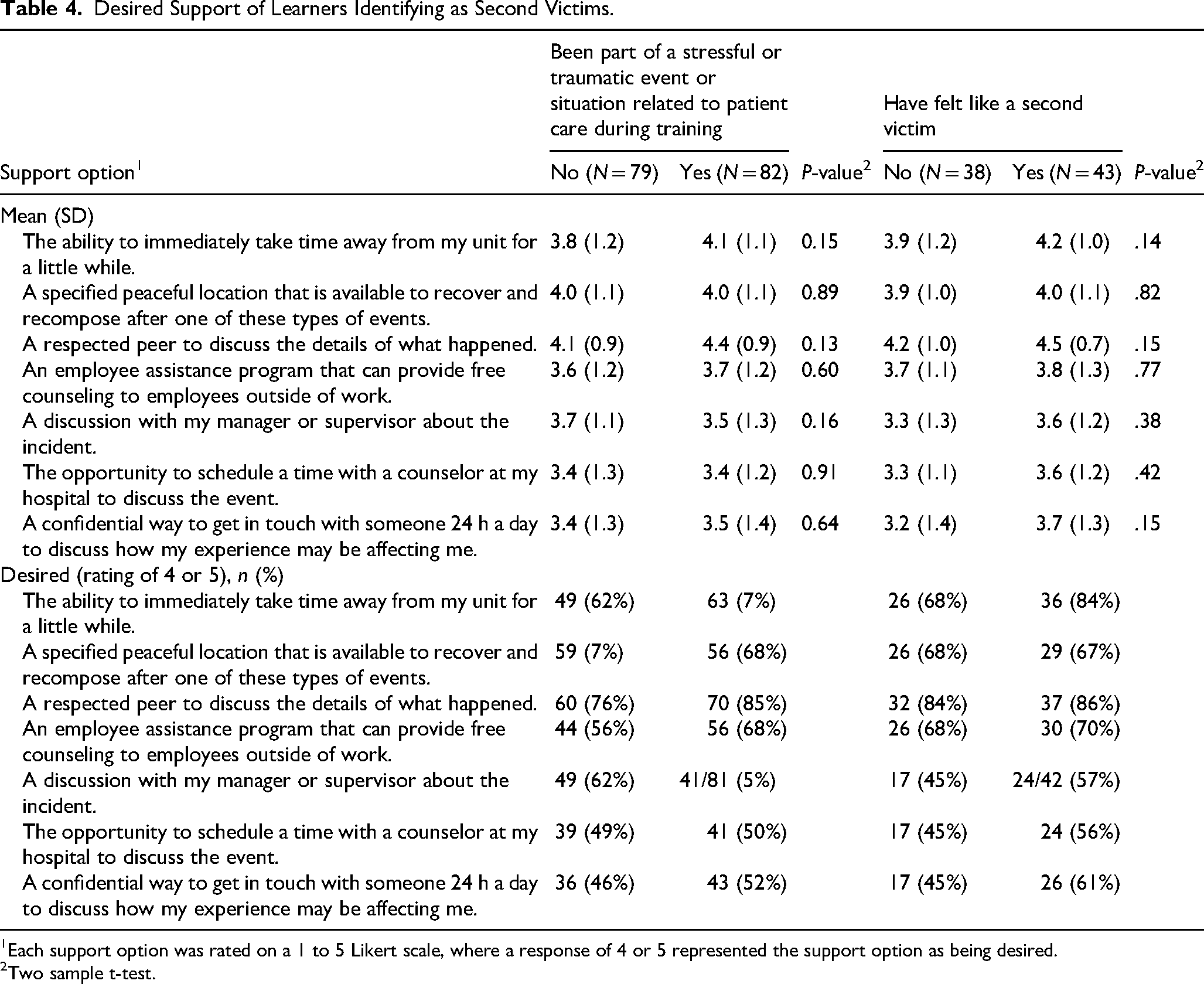
1Each support option was rated on a 1 to 5 Likert scale, where a response of 4 or 5 represented the support option as being desired.
2Two sample t-test.
Physician Well-Being Index
One hundred sixty-one respondents completed the PWBI (Table 5). For those respondents who have been a part of a stressful or traumatic patient care event, their mean well-being score was 3.4, while those who have not been part of traumatic patient care event have a mean score of 2.6 (P = .0009). Among all respondents, 4 of 13 (30.8%) medical students scored ≥4, 14 of 48 residents (29.2%) and 10 of 45 fellows (22%) scored at ≥ 5. Specific domains of the PWBI that were increased among those who had been part of a stressful or traumatic care event compared to those who did not experience an event included: “work hardening you emotionally” (P = .03), “things piling up” (P = .03) and “physical health interfering with ability to do daily work” (P = .01). Among identified SVs the question “has your physical health interfered with your ability to do your daily work at home and/or away from home” was answered in the affirmative more commonly than those who do not identify as an SV 34.9% (15/43) versus 15.85% (6/38), P = .05.
Physician Well-Being Index.

Comparisons between groups were evaluated using the sample t-test for the continuous well-being index and chi-square test for each individual item (categorical).
Discussion
We administered the SVEST-R and the PWBI to a group of multidisciplinary medical and health sciences learners to understand the prevalence of stressful or traumatic patient care events, self-identification as an SV, and their current well-being status. To the best of our knowledge, this is one of the largest multidisciplinary studies on the SVE of healthcare learners using validated instruments. Our results indicate that just over half of learners have been involved in a patient care event that they consider stressful or traumatic. This is higher than other studies where learner involvement in patient safety events varies from 20% to 30%.21,22 This may be a result of the high percentage of residents and fellows in the cohort who are likely to be involved in more high-acuity patient events. It may also be influenced by COVID-19, as this survey was fielded in Spring 2022 following the Omicron surge. Multiple studies have highlighted the anxiety of trainees and learners in response to high patient volumes, financial strain, and their ability to manage medical risk.10,11
Prevalence of SVE and Potential Impact on Learners
Of the participants in our study who have been involved in an event, 49.5% identified as feeling like an SV. In comparison, other studies report an SV prevalence of 62% and 58% among learners.7,22 While this study did not evaluate the effect of time from the event and current SV status, other work seems to suggest that trainees are more likely to encounter these experiences within the previous 12 months than nonlearners. 7 This suggests that supervisors and faculty should pay heightened attention to learners involved in situations involving medical errors or adverse patient outcomes.
The domains of the SVEST-R that were most different for those with SVE versus those that reported being involved in a traumatic event, but did not feel like an SV, were psychological distress, physical distress, and professional self-efficacy. Professional self-efficacy was the domain impacted among a greater percentage of learners identifying as SVs. A breakdown of the professional self-efficacy domain showed the largest difference between respondents who did and those who did not identify as an SV were feelings of inadequacy regarding patient care abilities postevent (Supplemental Table S4). It is presently unknown whether these feelings of inadequacy are inherent in SVE or if the role of the learner in the clinical environment and scrutiny of the trainees’ abilities after an event contributes to self-doubt and the development of SVEs.
Some symptoms of psychological and physical distress after an adverse event may be more easily recognized by those supervising or teaching the learner. However, decrease in professional self-efficacy or the belief in the ability to perform professional duties may be less visible but have lasting effects on the confidence of trainees. Learners may also be reticent to disclose such feelings out of concern about the impact it may have on their training and career. Self-efficacy may be a predictor of trainee well-being in that those who have high self-efficacy often feel prepared and capable. 23 Lower levels of self-efficacy can be a predictor of burnout. 24 Self Determination Theory is a framework for studying motivation and postulates that intrinsic motivation is heightened when individuals experience autonomy, competence, and relatedness. 25 Achievement of these 3 key components leads to increased well-being 26 and may be affected by SVE which may lead to decreasing intrinsic motivation. Educators should be aware of the potential influence of traumatic patient events on professional development and explore support mechanisms to help learners regain confidence in their skills and abilities. Although there is not much literature on improving self-efficacy after a traumatic event, educators have used many different strategies such as goal setting and action plans to improve confidence in their specific population of learners. 27 Learners with SVE may need to psychologically process the event to have increased self-efficacy. This is an area that needs more investigation.
In contrast to other studies exploring the impact of SVE on learners, one of the study's goals was to identify the well-being status of learners who had been a part of a patient safety event compared to those who had not. Using the validated PWBI, we were able to identify that the current well-being status of those participants who have been a part of a patient safety event was significantly less than those who have not. While the overall mean score of learners who identified as SVs fell under the at-risk scores of 4+ for medical students and 5+ for residents and fellows, the significant difference between learners involved in traumatic patient events and those identifying as SV versus those that have not had these experiences is concerning.
Support Needs and Desires
For healthcare learners who identify as SVs, the most utilized forms of support include conversation with peers, supervisors, and family. Similarly, among the entire sample, including learners who have not been involved in traumatic events, peer support is a highly desired means of postevent support. Many studies have shown comparable results about the desire for peer support among HCPs, including cohorts with residents and fellows.7,22,28 Implementing a trained peer support program or other formalized structures for postevent processing may be beneficial. Several programs have instituted peer support programs that show individuals receiving this intervention feel better supported by their organization.29,30 Our own institution offers trained peer support, including individual peer-to-peer and group emotional debriefing via the Mayo Clinic Healing Emotional Lives of Peers program, implemented institution-wide. 29
Guidance for Medical Educators to Identify Learners With SVE
Our data suggests that more formal systems to identify at-risk learners and connect them with postevent support should be considered by medical educators and program directors. From the literature and experiences at our own institution, we offer several suggestions as to how to better identify and support at-risk learners following an adverse patient care event. First, increased awareness of SVE through formal training among learners and educators involved in their training and supervision will improve recognition of SV symptoms among affected trainees. This may include introduction of the concept as part of orientation, with subsequent didactic sessions during medical school, residency, fellowship, or practicums to teach learners about SVE. Encouraging affected learners to self-refer to peer counseling or other support when involved in a traumatic or stressful event may facilitate improved uptake of support. Additional education for supervisors, including how to facilitate supportive debriefs and how to normalize SVE for affected learners, may also be beneficial towards developing a network of support and assist learners to regain confidence in their developing skills and competencies.
Another method to identify at risk learners is to regularly poll trainees for such experiences, using a validated instrument such as the SVEST-R to evaluate their risk of SV status. Unfortunately, HCPs are known for their low response rates to voluntary surveys and a mandatory requirement on this sensitive topic may raise concerns among learners about how such information may be used in their educational advancement.
Automatic referral of all colleagues, including learners, involved in a stressful patient care event to a trained peer support program or employee assistance program is another strategy that has been initiated at some institutions to identify potential SVs. 30 This strategy has the added benefit of avoiding stigmatization of trainees by singling them out for support, but instead demonstrates emotional processing is encouraged by the academic institution and that SVE can occur at any stage of one's career. Trained peer support is available to all employees at our institution, including learners who may be impacted by a patient event. Staff are encouraged to submit the names of affected staff to the Healing the Emotional Lives of Peers program so that a trained peer supporter can reach out for any support needs. 29 The results of this study, among others, suggest that learners may be particularly at-risk for traumatic responses and automatic referral to a peer support program by program leadership may proactively connect struggling learners with support.
Medical education programs are beginning to develop creative ways to support clinicians, trainees and students who experience a traumatic clinical event. The Association of American Medical Colleges describes several strategies that have been employed to promote healing, including story slams, role play and simulations at several institutions. 31 As the phenomenon of SVE becomes better known, solutions such as curricula to foster resident resilience, developed and shared in MedEdPortal, and an educator Toolkit on SVE will help educators to proactively address SVE and hopefully improve outcomes among affected learners.32,33
Strengths and Limitations
Strengths of our study include the large number of trainee respondents across diverse disciplines and the use of validated instruments to measure SV response and well-being. These results address an important knowledge gap about the HCP learner experience. The low response rate is a limitation, although it is consistent with other surveys that report low response rates among medical professionals 34 and recent trends of declining response rates during the COVID-19 pandemic. 35 However, the total number of learners who responded is one of the largest number of learners in a single study, to our knowledge, in the literature. Given that the survey utilized a voluntary nonprobability sample and sent to all learners, response bias is another potential limitation; respondents with more negative experiences or stronger feelings may have been more likely to complete the survey. Supplemental Table S2 shows that the respondents are slightly older and more likely to report their race as white than the surveyed population. To decrease response bias, the team sent reminders every other week for 6 weeks to encourage survey completion, with text reminding potential participants of the anonymity of the survey and goal to understand how to improve support for all learners. For maximum survey completion, we did not ask extensive details about the experience itself, such as length of time since the event occurred, however, our key findings are consistent with other studies examining SVEs. Respondent descriptions of these events is available in our qualitative analysis. 20 Additional research is needed to understand specific factors of the training experience that contribute to SVE and the long-term trajectory of trainees with these experiences early in their career.
Conclusion
In this multidisciplinary cohort of healthcare learners, nearly half of the learners reported experiencing a stressful or traumatic patient care event, with 49% of those individuals identifying as feeling like an SV. These results underscore the urgent need to identify healthcare learners affected by SVEs and connect them with appropriate support mechanisms. Peer support, particularly for emotional debriefing following a stressful patient event, was strongly preferred. This study, along with others, provides compelling evidence that trained peer support should be considered as an integral component of healthcare training programs to address the impact of adverse patient events and deliver timely interventions that promote learners’ personal and professional well-being.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251340434 - Supplemental material for Prevalence of Second Victim Experiences in a Cohort of Healthcare Learners and the Impact on Their Well-Being
Supplemental material, sj-docx-1-mde-10.1177_23821205251340434 for Prevalence of Second Victim Experiences in a Cohort of Healthcare Learners and the Impact on Their Well-Being by Vanessa E. Torbenson, Kirsten A. Riggan, Cynthia M. Stonnington, Lily Huang, Abd Moain Abu Dabrh, Adam I. Perlman, Tyler F. Vadeboncoeur, Megan A. Allyse, Robyn E. Finney and Enid Y. Rivera-Chiauzzi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251340434 - Supplemental material for Prevalence of Second Victim Experiences in a Cohort of Healthcare Learners and the Impact on Their Well-Being
Supplemental material, sj-docx-2-mde-10.1177_23821205251340434 for Prevalence of Second Victim Experiences in a Cohort of Healthcare Learners and the Impact on Their Well-Being by Vanessa E. Torbenson, Kirsten A. Riggan, Cynthia M. Stonnington, Lily Huang, Abd Moain Abu Dabrh, Adam I. Perlman, Tyler F. Vadeboncoeur, Megan A. Allyse, Robyn E. Finney and Enid Y. Rivera-Chiauzzi in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We thank Amy Weaver, Megan Branda, and Ramy Mehta for their descriptive statistical analysis. We want to thank the Mayo Clinic Education Shield for financial support for statistical analysis. We want to thank all the staff from Mayo Clinic Alix School of Medicine, Mayo Clinic School of Graduate Medical Education, and Mayo Clinic School of Health Sciences for their administrative help. Lastly, we want to thank all the learners who responded to the survey.
ORCID iD
Ethical Considerations
The study protocol, survey instrument, and informed consent materials were approved by Mayo Clinic's Institutional Review Board. This study was determined to be exempt by the Mayo Clinic Institutional Review Board (#21-010381). Mayo Clinic's Education Research Committee provided additional review and approved distribution of the study among Mayo Clinic's healthcare learners. All research was conducted in accordance with relevant guidelines and regulations.
Consent to Participate
The email invitation and beginning of the survey contained informed consent information. Respondents were informed in the email invitation and written information at the beginning of the survey that by clicking on the link and continuing with the survey they were providing written consent to have their anonymous results used for research. As responses were collected anonymously and the survey did not collect protected health information, Mayo Clinic's Institutional Review Board approved this informed consent procedure. Implied written informed consent was obtained for all individuals who voluntarily completed the online survey.
Author Contributions
Conceptualization and study design: EYRC, MAA, KAR, REF, CMS, AMA, AIP, VET, and TFV; data collection: EYRC, LH, and KAR; data analysis and interpretation: EYRC, VET, and KAR; drafting of manuscript: VET; critical revision of manuscript: all authors. All authors gave final approval of the submitted version and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by Mayo Clinic's Education Shield. This study was additionally supported by the National Center for Advancing Translational Sciences (Grant No. UL1 TR002377). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset supporting the conclusions of this article are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.