
Abstract
Objectives
To describe students’ experiences as health coaches in a student-delivered Community Outreach teleheAlth program for COVID education and Health promotion (COACH).
Methods
This qualitative description study collected data from student coaches (n = 19) who engaged in a 45-to-60-min semi-structured interview conducted via one-on-one on Zoom video-conferencing calls. Most (74%) student coaches were female with an average age of 25.6 years. Fifty-eight percent were from visible minority populations, and 42% administered COACH in suburban/rural areas. Coaches were located throughout British Columbia, Canada. Interview questions focused on students’ experiences delivering COACH, their understanding of various health-related topics (eg, chronic care, virtual health, health promotion), and possible impacts on their beliefs and future practice. Interviews were transcribed verbatim and analyzed thematically. Findings were reported in accordance with the Standards for Reporting Qualitative Research guidelines.
Results
Three themes emerged from our analysis, including: (1) knowledge and skill acquisition for professional development; (2) appreciating relationship-based client-centered care; and (3) developing clinical interests and gaining clinical experiences.
Conclusion
COACH supported the development of knowledge, skill, and confidence in medical school students in areas of health promotion, virtual care, and chronic disease management. Emerging themes were found to be representative of the six domains of the Canadian Medical Education Directors for Specialists (CanMEDS) framework (Theme 1: scholar and health advocate; Theme 2: professional and collaborator; Theme 3: leader and communicator). (ClinicalTrials.gov ID: NCT04492527).
Keywords
Introduction
Student-run clinics are defined by healthcare students being integrated to take the lead in supporting the delivery of health to patients while being supervised by licensed health professionals. 1 They are increasingly being used to support medical students’ early learning and clinical practices.2,3 Patients who use student-run clinics are observed to experience positive health outcomes and report positive satisfaction comparable to care provided by certified health professionals. 4 Research highlighting the importance and benefits of student-run clinics to primary, acute health care has increased within the past few years. 2 These clinics mirror current health systems while also provide health students opportunities to gain experience in clinical settings. 1 However, student-run clinics offering health promotion and chronic disease prevention and management support services are limited. 5
Health coaching is a patient-centered approach where patients work with coaches to determine health goals, actively learn educational content helpful to meeting their goals, and self-monitor behaviours to improve management of their health condition. 6 Coaching has been shown to be effective at facilitating health behaviour change, and thus improving chronic disease risk factor profile.6,7 Moreover, existing research indicates that such coaching may contribute to students’ professional development.6–8 For example, research focusing on teaching medical students how to effectively communicate health-behaviour change to patients highlighted how they appreciate opportunities to establish therapeutic relationships with patients. 9 Thus, previous research findings highlight medical school students’ engagement and appreciation in receiving health coaching opportunities to support their own learning and clinical skill development. 9 However, more information is needed to increase our understanding on the benefits of health coaching among health professional students.
In response to an increased need for chronic disease prevention and management support among older adults during COVID-19, we developed the student-delivered Community Outreach telehealth program for COVID education and Health promotion (COACH) program. 10 The program was adapted from a previous student-led telehealth stroke coaching program and used the Chronic Care Model as a guiding framework for its development.11,12 COACH is a 2-month intervention delivered by undergraduate medical students; it is a standardized health coaching program aimed at promoting healthy living behaviours and facilitate self-management in community-living older adults (≥65 years of age). In this two-month, six session, virtual program, coaches collaboratively develop strategies (ie, step-by-step action plans) with participants to help them reach their self-identified health-related goals.10,13 Using brief action planning and motivational interviewing, 13 coaches empower and support participants through education and motivation to self-manage their behaviours, while adhering to public health restrictions (eg, physical distancing) aimed at reducing the spread of COVID-19. 10
Prior to implementing COACH, medical undergraduate students were trained on the COACH protocol. All students began their training by attending an orientation session to learn about the COACH program and become familiar with basic motivational interviewing strategies and the structured conversation rubric that guided each coaching session. Afterwards, students attended practice coaching sessions and enrolled in a certification workshop to learn about and implement brief action planning. 10 Outside of the coaching sessions, student coaches were supported by the research team and senior coaches in regular monthly meetings and fidelity checks. 12 These meetings and fidelity checks gave the student coaches the opportunity to seek advice or help from each other and the research team in how to better run their coaching sessions, ensure quality control, and confirm that their coaching is delivered as intended. 10
In our previous investigation of COACH, we quantitatively evaluated the program, among older adults (n = 75) with chronic conditions, in a single group pre-post study design. We observed statistically significant improvements in heath directed behaviour and health promotion self-efficacy among participants. 10 Moreover, subjective comments indicated a high satisfaction with the program. 10 While this previous evaluation provided insight on how COACH empowered self-management among older adult participants, we were unable to gain any understanding on the experiences of the SCs who helped to deliver COACH. The purpose of this study is to understand the perspectives of medical students who led the COACH program sessions. In this paper, we investigated: (1) what are the experiences of trained medical student coaches (SCs) delivering COACH and (2) how these experiences supported their learning as undergraduate medical students.
Methods
Findings for this qualitative descriptive study were reported in accordance with the Standards for Reporting Qualitative Research guidelines (Supplemental Digital Content 1). 14 Ethics was obtained for this study from the Behavioural Research Ethics Board (H20-01368) at the University of British Columbia.
Participants
To be included, individuals needed to: (1) be actively enrolled in an undergraduate medical program during their time as a student coach, (2) be able to provide consent, (3) have been trained on the COACH protocol, and (4) previously led at least two sessions in the COACH program. Individuals were excluded if they were unable to provide informed consent and were unable to communicate in English. Table 1 summarizes our inclusion and exclusion criteria.
Inclusion and Exclusion Criteria

Individuals were initially recruited to become health coaches via social media groups and student email lists. Medical students who were interested in becoming an SC expressed their interest via email. A total of 19 SCs were trained and led COACH sessions. At the end of the 2-month COACH program, SCs were contacted and invited to participate in the interviews via phone or email by a member of the research team. All SCs met the required criteria to participate in the study. If the individual was interested in participating, they were asked to provide their electronic consent (eConsent).
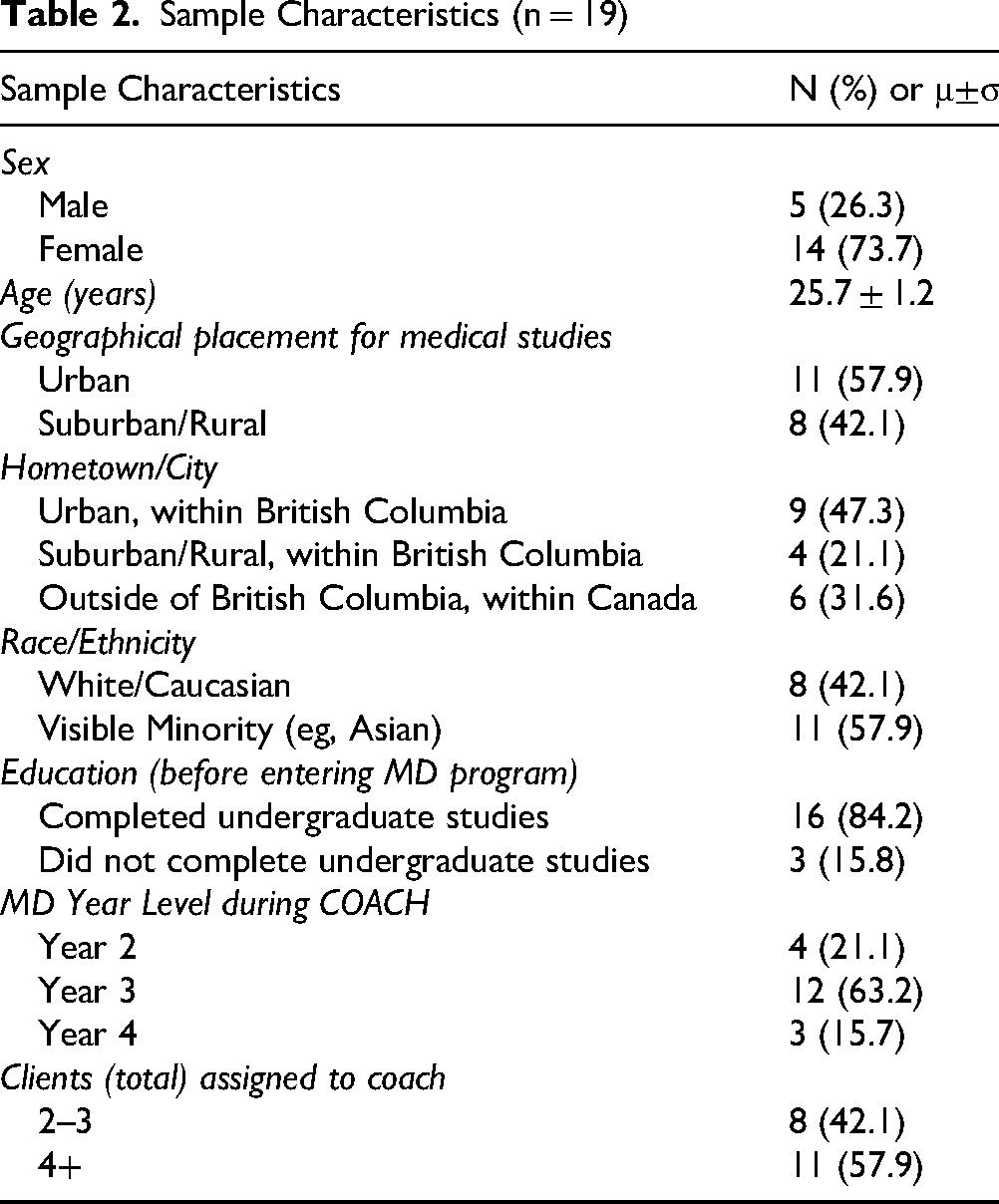
All SCs that were eligible were recruited for this study (n = 19). We recruited until data was deemed sufficient for the purposes of our study (ie, having enough data to meet minimum requirements to show similar and differing perspectives between SCs for analysis and decision making).15,16 Five male and fourteen female SCs from COACH participated in the study, with a mean age of 25.7 (SD 1.2). Fifty-eight percent of SCs were of visible minority populations, and 42.1% administered COACH while they were located and studying in rural or suburban regions of British Columbia (BC). During their time in the program, SCs were either in their second, third or fourth year of their medical undergraduate program. One SC coached up to three participants at a time, and in total SCs coached between 2 to 7 participants. Table 2 further details the sample characteristics.
Sample Characteristics (n = 19)
Period of Study
Data was collected between June 2021 and July 2021.
Data Collection
SCs were taken through a 30–45-min semi-structured interview. The interviews were conducted one-on-one via Zoom videoconferencing with a member of the research team (MY and CC). Both interviewers contributed to the development of the interview guide and had previous experiences conducting qualitative interviews. They also had previous interactions with all the SCs through coach training, program fidelity checks, and other administrative-related tasks. This familiarity allowed the interviewers to conduct more in-depth interviews, as they were familiar with the COACH protocol. Given that the interviewers’ previous experience in this field may be a source of bias, negative cases were probed while interacting with interviewees to limit both subjectivity and bias. Interviews were recorded using an audio recorder and recordings were transcribed shortly after data collection. Supplementary field notes were also written by interviewers throughout the interview process. Interviewers were trained by the study principal investigator (BMS) who has expertise in chronic disease management and prevention, health promotion, and virtual health.
A semi-structured interview guide was developed by members of our research team (BMS, CC, and MY). Interview questions focused on the medical students’ experiences participating in COACH as a health coach. Examples of questions from the interview guide included:
General knowledge/interest in chronic disease management and prevention, virtual health, etc (ie, “What was your perspective on chronic disease management and prevention prior to COACH?”); Thoughts on the training program and coaching resources that they received (ie, “How was your experience on getting trained to administer the coaching sessions?); and Overall experiences as a coach (ie, “How would you describe your overall experience in running the sessions for the COACH program?”).
The interview guide was further refined on an ongoing basis to include questions on new topics that were not originally in the interview script.
Analysis
Qualitative description was used as the guiding methodological framework for this study. Data was analyzed using a codebook thematic analysis approach.17,18 Two members of the research team (MY, GS) led the data analysis process. Initially, data was read multiple times to develop ideas and interpretations about recurring, converging, and contradictory patterns and identify key concepts, along with illustrative examples. 19 Broad categories were developed to organize and inductively code raw data using NVivo12. Coding allowed researchers to break up and recognize key elements and identify salient pieces of the data. Codes were modified or deleted throughout the analytic process.17,18 Coding began with each team member coding the same first five transcripts independently and then discussing any similar and contrasting thoughts and findings that emerged. During the coding process, a coding guide was developed to organize and manage each code. Codes were not drawn from pre-existing ideas that were developed prior to the analysis process, and the guide was modified throughout the coding process. 18 The remaining interviews were then divided and coded separately by each team member. The two team members met regularly to continue discussion of findings throughout the analysis process. After all data was coded, themes were collaboratively developed by research team members (MY, GS, BMS, CC). A theme was identified if it brought “meaning and identity to a recurrent experience and its variant manifestations” and captured something important about the objectives.20,21 By the end of analysis, themes were created, named, and defined. Table 3 summarizes the step-by-step analysis process.
Step-by-Step Analysis Process

Two study co-authors (first and second author) were involved in the data analysis process. Whereas the first author has an academic background focussing chronic disease management and prevention and virtual health, the second author has an academic background on mobile health apps for individuals living with spinal cord injury. As the first author's previous experience in COACH project evaluation activities and interaction with the SCs could create a source of bias or be influenced by pre-existing ideas, they kept track of their thought process through notetaking throughout the analysis process. Furthermore, multiple trustworthiness strategies were also implemented, including reflexivity, investigator triangulation, and member checking. 22 These steps further supported the interviewer's awareness of their own position in the research process, and thus helped to document how the interviewer's positioning shaped data interpretations. All records of raw data, field notes, and transcripts were kept for researchers to clearly systemize, relate, and cross-reference data. 22
Results
Three main themes emerged regarding medical students’ experiences in COACH: (1) knowledge and skill acquisition for professional development (ie, learning virtual care, learning health promotion strategies); (2) appreciating relationship-based client-centered care (ie, motivating clients to improve their health and wellbeing and appreciating building rapport); and (3) developing clinical interests and gaining clinical experiences (ie, developing different understandings and interest in chronic care and overcoming coaching-related challenges).
Knowledge and Skill Acquisition for Professional Development
SCs described how COACH allowed them to explore opportunities for knowledge and skill acquisition in areas that receive little attention in their medical undergraduate curriculum. Some of these included virtual care, health promotion strategies, and client-centered based care. Table 4 provides example quotes for each of the subthemes.
Theme 1: Knowledge and Skill Acquisition for Professional Development – Subthemes and Example Quotes
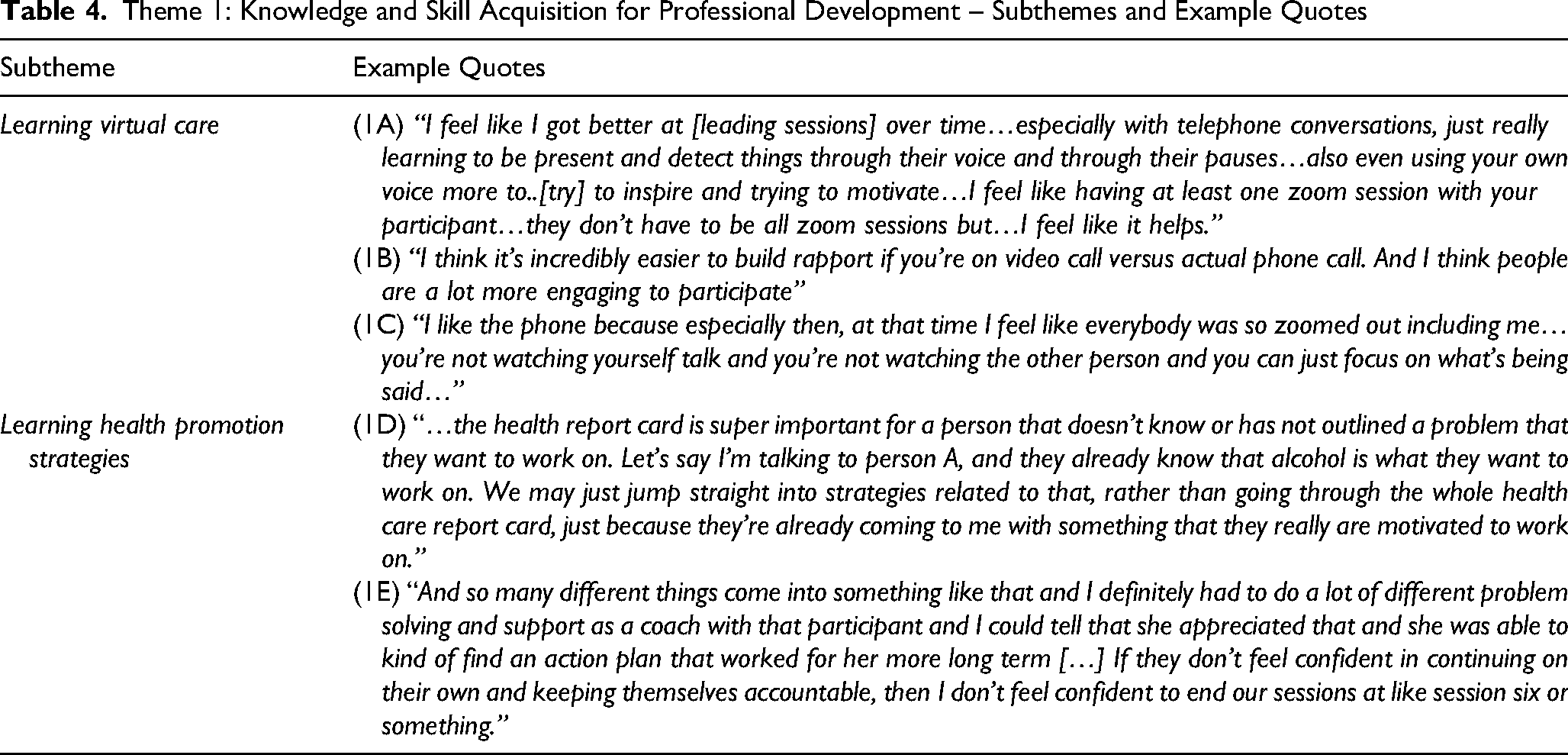
Learning Virtual Care
For some SCs, COACH was their first-time delivering care using technology. SCs had to adjust to communicating through phone or video conferencing, which may involve picking up on different social cues compared to in-person appointments (1A). Other SCs had some experiences delivering care virtually in their medical curriculum (because of COVID-19), and thus COACH allowed them to gain further experiences in delivering health promotion strategies effectively to people at a distance. SCs also learned about the advantages and disadvantages of different technologies and even developed preferences between various options. For example, some SCs preferred video conference calls because of the ability to visually see participants for additional social cues to support communication and verbal interpretations (1B). On the other hand, SCs who expressed preference for using telephones explained how telephones created less distraction and provide better focus for the conversation (1C). By the end of their coaching experiences, all SCs expressed that they would be open to using virtual care options in their future professional careers in medicine.
Learning Health Promotion Strategies
For many SCs, learning chronic disease management and prevention health promotion strategies were identified as key learning experiences during COACH. SCs highlighted how the program allowed them to learn and practice health promotion strategies, such as brief action planning and motivational interviewing techniques, be able to review health self-assessments (completed at the first session to gather information about participants’ current health situation and goals) and learn to develop and implement health promotion action plans in the context of COVID-19-related environmental restrictions. For example, one SC described the benefits of using a self-health assessment in their ability to identify health-related problem areas that can be worked on with participants (1D). The self-health assessment allowed SCs to obtain a general idea about participants’ health priorities, which then was used to help guide discussions they had with their paired participants. Similarly, another SC described how developing a step-by-step action plan with participants served as an important source of confidence among COACH participants (1E). Developing action plans not only helped participants stay organized and accountable to their goals, but it also facilitated SCs to better learn and observe ways that participant progress. Overall, learning chronic disease management and prevention health promotion strategies, such as brief action planning and motivational interviewing techniques, were deemed instrumental to SC's professional development as medical professionals.
Appreciating Relationship-Based Client-Centered Care
This second theme revolved around the relationship and rapport that SCs developed with each of their COACH participants. COACH participants had the opportunity to self-identify what health goals they wanted to focus on and collaborate with their assigned SC to received support in achieving those goals. SCs expressed how building these relationships with participants was not only instrumental in facilitating the successful pursuit of their health goals, but also helped coaches themselves with their own professional development and appreciation for client-centred care. These include: (1) motivating clients to improve their health and wellbeing, and (2) appreciating the opportunity to build rapport. Table 5 provides example quotes for each of the subthemes below.
Theme 2: Appreciating Relationship-Based Client-Centered Care – Subthemes and Example quotes
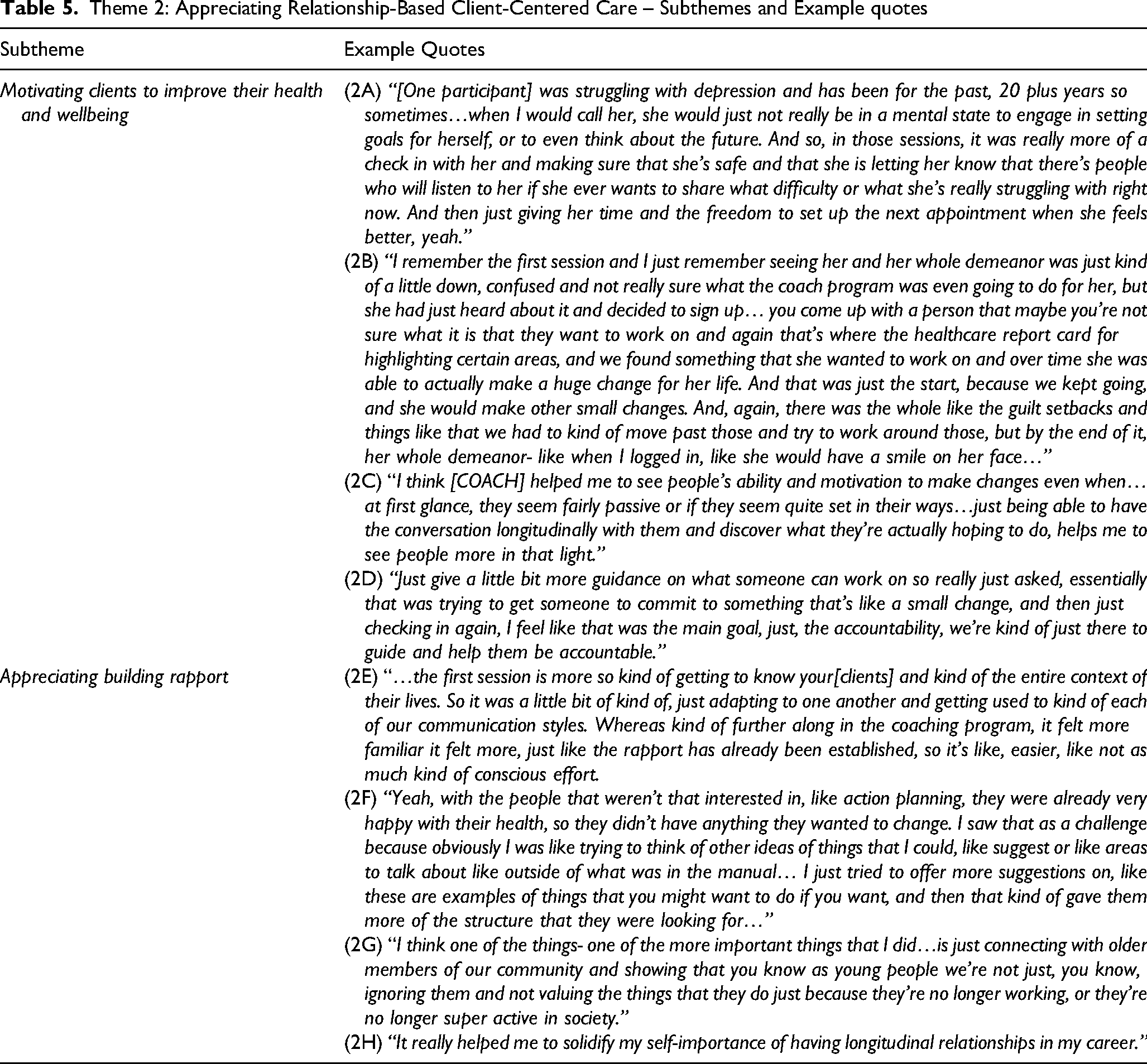
Motivating Clients to Improve Their Health and wellbeing
SCs highlighted the importance of having the opportunity to motivate their clients during the relationship-building process to improve their health and wellbeing. As part of COACH, SCs would engage in discussion to learn about the participant's self-perceived health and wellbeing, successes, and areas for improvement. Coaches highlighted how participants would not always be in the same state of motivation, and thus SCs gained experience in how to structure sessions and promote health and wellbeing among participants who were less motivated (2A). Several SCs emphasized that positive encouragement helped with motivation, particularly when participants’ reported experiences of minor setbacks or challenges in improving their health goals (2B). Moreover, SCs attempted to identify opportunities for growth among less motivated participants, which helped them figure out the best strategy to initiate motivation (2C). Additionally, SCs elaborated on how they played an important role in promoting motivation via holding participants accountable to follow their action plans (2D).
Appreciating Building Rapport
During their time in COACH, SCs grew to appreciate building rapport with their clients, which supported their understanding of the value of developing positive relationships with patients for their future clinical work. COACH gave opportunities for SCs to develop relationships with study participants that supported their development in communicating with others in a professional setting. In return, the rapport built between SCs and their assigned participants also allowed for a more personalized experience for COACH participants. For example, having enough time to get to know participants during COACH allowed SCs the chance to understand and adapt to different attitudes towards health each participant had (ie, based on personalities, the way they respond to different motivational cues and phrasing, etc), which supported the effectiveness of program content delivery (2E, 2F). This helped SCs in relating to emotional struggles that participants reported in either their current circumstances, or when trying to reach the specific health goals (2G). Overall, SCs learned how building rapport could provide both clinical benefits for themselves, and health benefits for the participant.
Developing Clinical Interests and Gaining Clinical Experiences
This theme represents SCs developing their clinical interests and gaining clinical experiences while applying health promotion and chronic care-related strategies during COACH. Two sub-themes emerged including: (1) increasing understanding in chronic care; and (2) applying clinical decision making to overcome coach-related challenges). Table 6 provides example quotes for each of the subthemes that emerged below.
Theme 3: Developing Different Understandings and Interest in Chronic Care – Subthemes and Example Quotes

Increasing Understanding in Chronic Care
SCs highlighted how the program allowed them to gain new meaning or refine their understanding of the meaning of and approach to chronic care. For example, SCs discussed how COACH contributed to their understanding that chronic care is a holistic process consisting of all physical, mental, emotional, and spiritual components (3A, 3B). In general, COACH allowed SCs to observe differing client perspectives on what is important for chronic care. Moreover, SCs highlighted how COACH contributed to their confidence in engaging with participants about their chronic care concerns through repeated practice (3C). Ultimately, SCs’ reported their experiences in the program facilitated their development of a multifaceted whole-person, and patient-centred approach to supporting patients with chronic disease.
Overcoming Coaching-Related Challenges
Challenges that arose during coaching sessions (eg, regarding how coaches delivered program content or reception of program content from the participants) gave SCs opportunities to further develop their clinical reasoning skills and experiences. Some SCs described how they experienced initial struggles when first beginning COACH. For example, some SCs had participants that struggled to identify initial health goals (eg, could not identify any goals, identified too many goals that could not be achieved within six coaching sessions). In these situations, SCs described how they would use collaborative problem solving and decision-making strategies by offering multiple evidence-based suggestions before participants could settle on an idea. This was sometimes due to participants being indecisive, or due to participants already having positive health behaviours and thus, SCs had trouble finding areas that participants could work on. These situations gave SCs the opportunity to practice delivering motivation and behaviour change strategies. SCs even mentioned taking time outside of the sessions to search through their own resources to figure out how to effectively help individual participants with crafting personalized sets of health goals (3D). By doing so, these SCs felt they were able to practice and develop clinical reasoning skills to effectively support and motivate participants to identify the health goals they wanted to achieve.
Importantly, the challenges highlighted above experienced by SCs provided them with the opportunity to practice and apply their problem solving in a virtual setting. Many of the SCs expressed appreciation for the challenges they needed to overcome, as they contributed to their own ongoing development as medical trainees (3E). COACH also gave SCs the opportunity to further develop any previous education or medical interests in settings outside of their medical curriculum (3F). Overall, by experiencing challenges during their coaching sessions, SCs had an opportunity to further their professional development outside of their studies.
Discussion
In this qualitative description study, we aimed to explore the experiences of medical undergraduate students who were trained as health coaches (SCs) to administer a chronic disease management and prevention program, COACH. Our findings suggest that COACH supported the development of knowledge and skill in SCs in the areas of health promotion, virtual care, and chronic disease management. These were reflected through themes that summarized SCs’ learning (ie, “Knowledge and skill acquisition for professional development”), relationship building with participants (ie, “Appreciating relationship-based client-centered care”), and clinical application (ie, “Developing clinical interests and gaining clinical experiences”). Within these themes, SCs also reflected on how they developed interest and appreciation in concepts or topics they experienced during their time as a coach.
While our previous research on COACH indicated health benefits of the program to older adults, in this study we also show benefits of the program to SCs. Our previous quantitative study demonstrated COACH to support health directed behaviour and health promotion self-efficacy in older adults during COVID-19. 10 This current study highlights SCs’ personal reflections on how training to deliver and delivering the COACH program benefitted their professional growth. Leading COACH sessions allowed SCs to not only experience developing rapport with patients but also gave them the opportunity to learn how to deliver health virtually for chronic disease management and prevention.
Interestingly, other student-led health programs emerged during COVID-19, to increase health service capacity with using minimal resources.23,24 For example, in the United States, a free student-led telemedicine clinics opened to serve uninsured patients in Florida and New York.23,24 Importantly, these clinics provided continuity of care for uninsured patients, which allowed for the provision of safe care to individuals with COVID-19, provided examples where health delivery via technology is a viable option, and created opportunities for medical education. Results from this study indicate that telemedicine is a viable method in providing care and enhancing service learning for medical school volunteers.23,24 We also provide evidence that the use of technology is viable for health service delivery and enhanced student experiences and learning, however, in the context of chronic disease management and prevention,.25–27 This focus highlights the program's dual benefit of meeting unmet educational needs for SCs while supporting patients with chronic conditions through virtual coaching.
Our findings are also consistent with the domains of the CanMEDS (Canadian Medical Education Directions for Specialists) competencies, an overarching educational framework developed to identify and describe the core abilities physicians require to meet the health care needs of their patients. 28 Figure 1 shows a visual representation of the framework. 28 Within the framework, required abilities are grouped into six roles: medical expert, communicator, collaborator, leader, health advocate, scholar, and professional. 28 The framework represents how an effective physician (ie, the “medical expert”) integrates all seven roles to improve the care of their patients. 28 We found each of our themes to be consistent with two CanMEDS roles: (1) scholar and health advocate (Theme 1: “Knowledge and skill acquisition for professional development”); (2) leader and communicator (Theme 2: “Appreciating relationship-based client-centered care”); and (3) professional and collaborator (Theme 3: “Developing different understandings and interest in chronic care”). Our interpretations are summarized in Table 7.
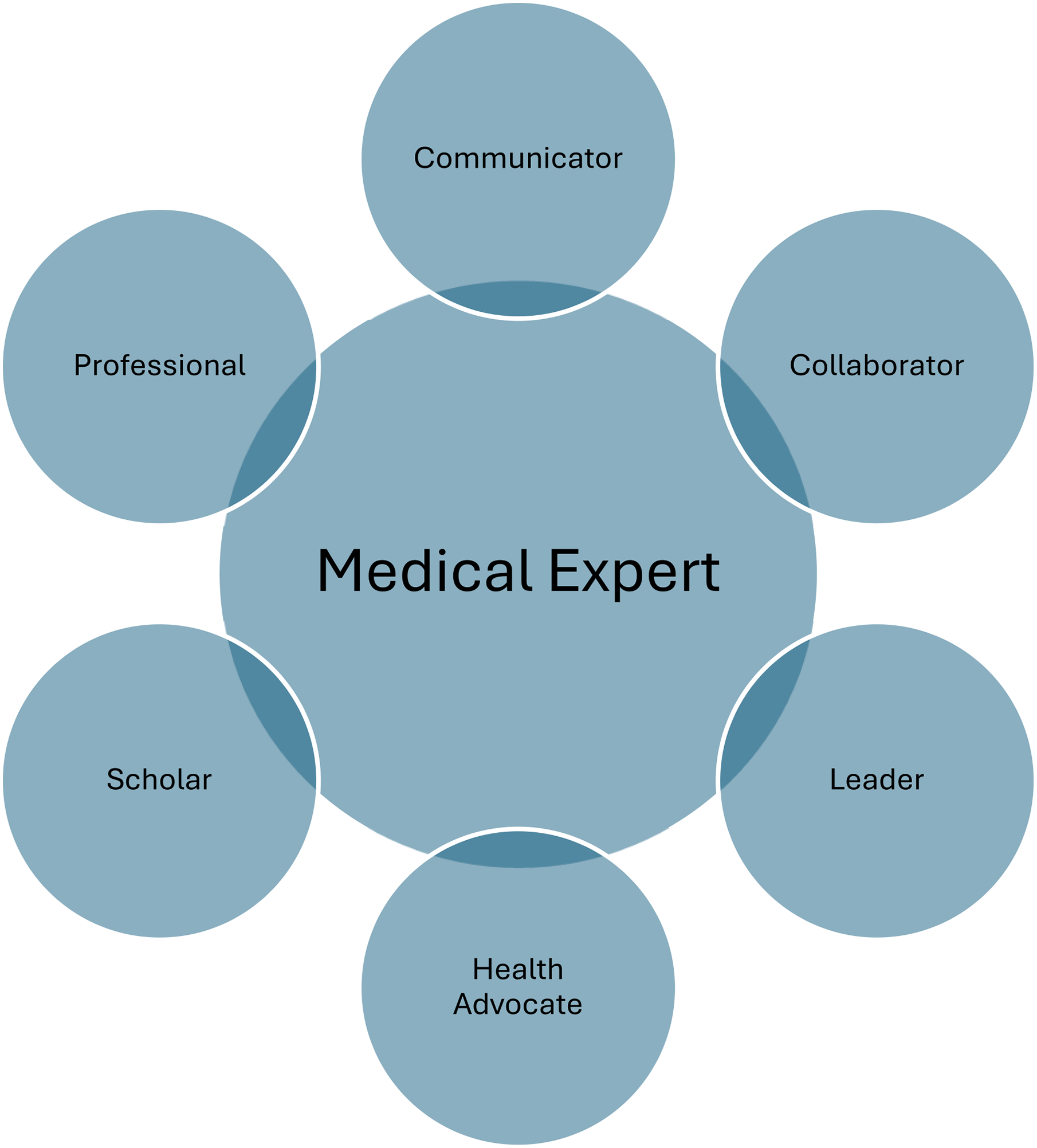
CanMEDS Framework.
Our Themes and CanMEDS Roles
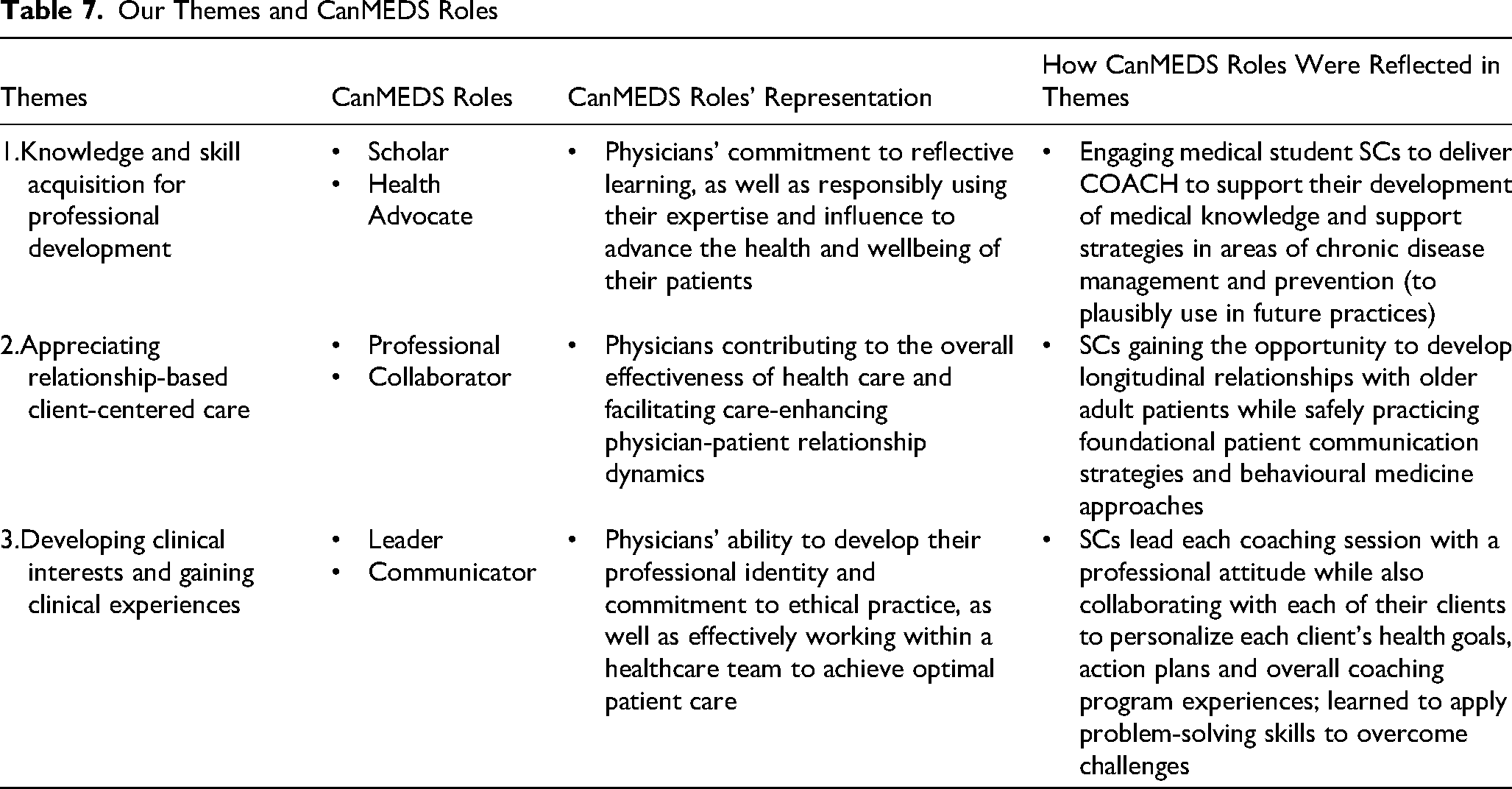
The first theme, “Knowledge and skill acquisition for professional development,” represented SCs’ experiences that allowed them to develop their scholarly and health advocacy roles. In CanMEDs, the scholar and health advocacy roles represent physicians’ commitment to reflective learning, as well as responsibly using their expertise and influence to advance the health and wellbeing of their patients. 28 Engaging medical students to deliver COACH supported their development of medical knowledge and support strategies in the areas of chronic disease management and prevention. This is of paramount importance considering that medical undergraduate programs have a minimal focus on chronic disease management and prevention, despite the increasing prevalence of chronic diseases in the older adult population.25–27 By developing the knowledge to support chronic disease management and prevention, SCs may potentially open opportunities for them to successfully support their future patients in managing and preventing their chronic diseases.25–27 Additionally, SCs were provided with opportunities to engage in virtual health, which is now emerging as a new normal in health care. 29 However, due to its recent emergence largely resulting from COVID-19 public health restrictions, training in virtual health is also lacking within the medical education system. 29 Thus, through COACH, SCs were given opportunities to practice delivering chronic disease management and prevention strategies using virtual health techniques, which they will plausibly use in their future practices. Overall, COACH was viewed as a resource among students to explore and develop highly relevant knowledge and skills that have little emphasis in their medical education.
The second theme on “Appreciating relationship-based client-centered care” emphasized relationship building with participants, where SCs were given the opportunity to develop their abilities as both a leader and a communicator. In the context of the CanMEDS framework, the leader and communicator roles represent physicians contributing to the overall effectiveness of health care and facilitating care-enhancing physician-patient relationship dynamics. 28 A core contributing element to these competencies is early clinical exposure. Early training patient interaction allows medical students to learn how to improve communication skills and begin developing their professional identity early in their medical training. 30 Unfortunately, during pre-clinical years at many institutions, there is limited patient interaction. COACH provided a means by which SCs’ could develop their first longitudinal relationships with patients and safely practice foundational patient communication strategies and behavioural medicine approaches while building rapport with adults aged 65 years or older. Many SCs appreciated the opportunities that COACH provided to improve their communication skills and practice interacting with program participants to support their future medical careers. At the same time, SCs also reported satisfaction in observing their participants being successful at improving their health behaviours through their support. Overall, COACH provided medical undergraduate students opportunities to develop as effective communicators and leaders in care, supporting their future clinical practice.
The third theme on “Developing different understandings and interest in chronic care” theme highlighted the professional development of SCs leading COACH. Findings in this theme parallel the CanMEDS roles of a professional and a collaborator, which represent physicians’ ability to develop their professional identity and commitment to ethical practice, as well as effectively working within a healthcare team to achieve optimal patient care. 28 Previous literature highlights the benefits in involving medical students in clinical practices early in their education to enhance students’ professional identity and attitude, team experience and skills, and their ability to perform various clinical tasks. 31 Furthermore, whereas mentorship and role modelling experiences through clinical practice experiences have been shown to influence professional behaviour and identity formation, curriculum adaptations due to the COVID-19 pandemic have been shown to impact the attainment of these experiences.31,32 Additionally, early involvement in clinical practices could also benefit students in improving collaborative attitudes and behaviours when working with clients. 33 In our research, SCs were presented with the opportunity to develop their clinical and professional experiences by working as a virtual health coach with older adults who have diverse chronic disease management and prevention needs. Specifically, SCs took the initiative to lead each coaching session with a professional attitude while also collaborating with each of their clients to personalize each client's health goals, action plans and overall coaching program experiences. When met with coach-related challenges, SCs learned to collaborate with their assigned participants and apply their problem-solving skills to overcome those challenges. Thus, our research contributed to the professional and collaborative development of the medical students involved by providing them these opportunities. Overall, COACH not only supported participants in managing their health behaviours, but it also supported student coaches in: (1) learning how to use key communication strategies that could be applied in clinical settings; (2) learning about lifestyle/behavioural medicine; and (3) obtaining hands-on experience to develop themselves as medical experts.
Overall, our findings suggest that student clinics can effectively deliver chronic disease management support through health promotion initiatives. Institutions may consider implementing similar virtual coaching programs that not only focuses on benefits for program participants, but also their benefits on medical students and their medical education. By providing the right training to deliver virtual programs, 34 institutions may use these to give medical students an alternative to expanding their clinical learning and experiences alongside their medical curriculum. Highlighting the program's role in providing medical students with education and hands-on experience in working with patient populations, virtual health, and chronic disease management can be a key motivator for volunteering to deliver such programs.
Limitations
There are several limitations to this study. First, social desirability bias is possible due to SCs’ knowing their responses are being audio recorded and the interviewer's presence. Second, while perspectives that we gathered are reflective of all SCs that were involved with COACH, we cannot guarantee that these experiences reflect all medical undergraduate students. This thus limits the transferability of findings. Further studies are needed to better determine the transferability of health promotion coaching experiences of medical school students that lead to similar interventions. Finally, as the majority of SCs were female (73.7% of the sample), there is underrepresentation of male medical school students and their experiences in student-led interventions. 35 Thus, future research may consider equal representation of female and male study participants to compare similarities and differences in their experiences providing chronic disease management and prevention support.
Conclusion
Findings suggest that COACH supported the development of knowledge, skill, and confidence among medical school students in areas of health promotion, virtual care, and chronic disease prevention and management. Study findings were also found to parallel six domains of the CanMEDS framework (Theme 1: scholar and health advocate; Theme 2: professional and collaborator; Theme 3: leader and communicator). COACH also provided students with opportunities to develop interest and appreciation that they may use in clinical, relationship-based patient care. Our findings support the use of medical student-led clinics for the delivery of chronic disease management and prevention programs, as it benefits both participants and students.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251335723 - Supplemental material for Experiences of Health Professional Students Delivering a Community-Outreach TeleheAlth Program for COVID Education and Health Promotion to Older Adults
Supplemental material, sj-docx-1-mde-10.1177_23821205251335723 for Experiences of Health Professional Students Delivering a Community-Outreach TeleheAlth Program for COVID Education and Health Promotion to Older Adults by Michelle C. Yang, Gurkaran Singh, Cam Clayton, Devin Harris and Brodie M. Sakakibara in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors acknowledge all students from the University of British Columbia's Doctor of Medicine (MD) undergraduate program for dedicating their time and efforts to delivering the intervention presented in this study. The authors also acknowledge the Centre for Collaboration, Motivation, and Innovation for their contribution to the coaches’ training.
Ethical Considerations
Ethical approval was obtained from the Behavioural Research Ethics Board (H20-01368) at the University of British Columbia.
Consent to Participate
All participants provided written informed consent to participate.
Author Contributions
All authors contributed to the study conception and design.
Funding
This work was supported by funding from the Interior Universities Research Coalition (IURC) for BC Interior Region Seed Grant Health Research Fund and the Michael Smith Foundation for Health Research Scholar Award (to BMS).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.