
Abstract
Background
Diversifying the healthcare workforce is critical to achieving a healthier, more equitable society.
Objectives
The objective of this literature review was to examine and synthesize the literature on interventions to promote diversity, equity, and inclusion (DEI) in people who are currently enrolled in the workforce or in a terminal degree/training program and who are located in the following institution types: medical centers; healthcare organizations; and schools of dentistry, medicine, nursing, nurse practitioners, physician assistants, and public health.
Methods
A literature search was performed on November 2, 2023 in Ovid MEDLINE®. We reviewed titles and abstracts of all retrieved articles from 2000 forward and the full text of articles included in the final review. We included English-language articles published in peer-reviewed journals that detailed 1 or more interventions to promote DEI in the United States and United States territories. All data included in the final review was extracted by a single investigator and charted using an Excel spreadsheet.
Results
The authors identified 55 articles for inclusion, 4 of which aggregated and analyzed data from many interventions. The remainder detailed 52 interventions across 25 states and Puerto Rico. Most articles did not include a comparison group (38, 69%). The types of interventions identified were: institutional change (14, 27%), mentorship (13, 25%), development programs (13, 25%), pathway programs (5, 10%), financial support (2, 4%), and workshops (2, 4%). Three (6%) interventions could not be categorized. Most studies detailed interventions in medicine (28, 54%) and nursing (11, 21%), focused on racial and ethnic (42, 81%) and/or sex (12, 23%) diversity, and targeted students (33, 64%) and/or faculty/staff (28, 54%).
Conclusion
Many different types of interventions have been trialed to promote workforce DEI in the United States healthcare workforce. These efforts must continue to achieve a diverse and equitable healthcare workforce.
Keywords
Introduction
Diversifying the healthcare workforce is critical to achieving a healthier, more equitable society. Among other examples, workforce diversity is associated with better patient care,1–6 high-quality research,7–11 and increased health equity.12–16 Despite the crucial benefits that diversity provides, people from minoritized groups remain underrepresented at all career levels in medicine,17–19 nursing,20,21 and other health professions. 21
In light of the recent Supreme Court decision banning affirmative action, attention has focused on increasing recruitment of minoritized groups into health education programs.22,23 Although these efforts are both laudable and necessary, it is also necessary to address diversity after recruitment into educational programs.19,21,24–29 Even after entry into the workforce, minoritized candidates often face a high level of attrition, and representation of minoritized groups decreases with each step up the career ladder.19,21,24–29
Diversity, equity, and inclusion (DEI) in the existing workforce is particularly important because faculty, staff, and leaders at healthcare organizations and health professional schools may have disproportionate power over their organization's culture and priorities. 30 Additionally, minoritized staff and faculty can be critical in recruiting minoritized students and junior staff, which may create of virtuous cycle of increased DEI over time. 22 Promoting DEI in the existing healthcare workforce is therefore an urgent priority.
Unfortunately, many of the interventions used to recruit minoritized students into health professional schools may not work to increase DEI after matriculation. The challenges and obstacles that minoritized workers face after entry into terminal degree programs and/or after entry into the workforce itself likely differ from those that minoritized people face when applying for health professional programs. Therefore, many of the interventions designed to increase recruitment of minoritized students into health professional schools may not be applicable to people who have already entered a terminal degree program or the workforce. For example, holistic admission models that decrease the emphasis on standardized testing show promise in increasing recruitment of minoritized medical students and residents. 22 However, admission models are unlikely to be helpful for faculty and staff recruitment, which follows an entirely different process and does not involve standardized testing.
Current literature reviews have focused on recruitment into health professional schools. 22 Not much is known about the existing literature on interventions to increase DEI in students currently enrolled in a health professional program or people who are already working in their chosen health profession. Some past literature reviews have focused on a single type of intervention, such as mentorship,31,32 or interventions in a specific field.31–33 However, to our knowledge, no previous reviews have examined multiple types of interventions to promote DEI across multiple fields including dentistry, medicine, nursing, nurse practitioners, physician assistants, and public health.
Because so little is known about the existing literature on interventions to promote DEI in these fields, a scoping review of existing research is necessary. A scoping review allows for an examination the strengths and weaknesses of prior studies and literature gaps in the field. This exploration of existing research and research gaps is critical for future researchers looking to contribute to the field.
To fill this gap, we performed a scoping review of interventions to promote DEI in medical centers, healthcare organizations, and health education programs. The objective of this literature review was to examine and synthesize the literature on interventions to promote DEI in people who are currently enrolled in the workforce or in a terminal degree/training program and who are located in the following types of institutions: academic and nonacademic medical centers; healthcare organizations; and schools of dentistry, medicine, nursing, nurse practitioners, physician assistants, and public health. Terminal degree/training program was defined as the final program that students need to complete before they can work in their chosen health profession.
Methods
This literature review was performed following the PRISMA reporting guidelines for scoping reviews (Supplement 1). 34 A review protocol does not exist. However, the literature review was performed as described below.
Literature Search
A literature search was performed by a medical librarian (LCH) in Ovid MEDLINE® (1946+ and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Ovid MEDLINE® Daily) on November 3, 2023. The date range was later further restricted to articles published on or after 1/1/2000. The search was limited to English-language articles from 1990 forward. Medical subject headings as well as keywords were used to identify articles on interventions related to DEI in medical centers, healthcare organizations, and schools of dentistry, medicine, nursing, nurse practitioners, physician assistants, and public health. The full search strategy is included in Supplement 2.
Results were imported into Endnote. In addition to original research, the search also retrieved several prior literature reviews. One researcher (KAH) reviewed the reference lists of all potentially relevant prior literature reviews to identify additional articles that fit the inclusion criteria.
Study Selection
Study selection was performed by one researcher (KAH). Articles were screened first by title and abstract to determine whether they met inclusion criteria. For articles that did not clearly meet inclusion or exclusion criteria, the researcher performed a full-text review.
Inclusion and Exclusion Criteria
Articles were included if they were published in a peer-reviewed journal, used original data, and detailed 1 or more concrete interventions to promote workforce DEI in the following types of institutions: academic and nonacademic medical centers; healthcare organizations; and schools of dentistry, medicine, nursing, nurse practitioners, physician assistants, and public health. Other health professions were not included in the search strategy or in the final review. These professions include but are not limited to social workers, pharmacists, physical/occupational therapists, and mental health professionals other than psychiatrists. Articles were retained if the intervention targeted a single profession or multiple professions, at least one of which was within the scope of this review.
Articles were excluded if the intervention was designed to promote DEI in patients, society at large, or any population other than the workforce. For example, interventions designed to teach students about health disparities and social mission interventions were excluded. However, articles were retained if they detailed an intervention that included multiple goals or elements, at least one of which targeted workforce DEI. For example, an intervention to promote health disparities research and recruit minoritized faculty members would be retained. However, the authors only extracted data for intervention elements pertinent to workforce DEI.
Articles were only included if the intervention detailed was targeted toward promoting DEI among people who had already entered their terminal degree/training program or the workforce at any level (eg, postgraduate, faculty, leadership). The terminal degree/training program was defined as the final program that students need to complete before they can work at the highest level in their chosen field.
The terminal degree/training program included by field is as follows: medical residents for medicine, masters-level nursing students for nursing, dental students for dentistry, masters or doctorate students for all other fields. MD and DO students were excluded from this review because, unlike doctoral students in other fields, they need to complete another training program that uses a standardized application process (residency) before they can work in their chosen field. Previous reviews have already examined interventions to promote DEI by altering an educational program's admission process. 22 The purpose of this review was instead to examine interventions that occur after the completion of all educational/training program application and admission processes.
Articles were included if the intervention was targeted toward participants at multiple career stages, including career stages lower than those of interest to this paper. For example, interventions that targeted both medical students and residents or interventions that aimed to increase both recruitment of minoritized candidates for a masters-level nursing program and retention of those candidates following enrollment. However, the authors only extracted the data for participants and/or intervention elements relevant to the career levels of interest for this review.
Articles were excluded if they did not include information on an intervention targeting participants in the United States or United States territories. The geographic restriction was chosen because the target audience of this literature review is United States investigators, health professional workers, and health professional leadership. Because of the large social, culture, and political differences in DEI between different countries, interventions to promote DEI performed outside the United States are unlikely to be relevant to readers in the United States.
In several cases, we identified articles that included participants in both the United States another country. Articles that included participants from the United States and another country were included in the final literature review. In all of the cases that we identified where an article included participants in both the United States and another country, the other country included in the intervention was Canada. No articles were identified that included participants from both the United States and a country other than Canada.
We excluded pre-existing literature reviews from the final literature. However, we reviewed the citations of all potentially relevant pre-existing literature in order to identify additional articles that met inclusion criteria. We excluded theory, position, and opinion articles. We excluded articles with suggestions for possible interventions but no clear plan for implementation. We excluded articles that were commentaries on other articles that discussed a DEI intervention. We did include commentaries on original interventions that were designed/implemented by the authors of the commentary, even if the commentary did not include information on outcomes of the intervention.
During the literature review process, we identified 4 articles that were not literature reviews but that aggregated and analyzed data from many interventions at different locations.35–38 Of the 4 articles, only 1 included any nonaggregated data on specific interventions. 35 None of the 4 articles included enough specifics on individual interventions for a full analysis of intervention characteristics. 35 Therefore, these 4 articles were not included in analyses of intervention characteristics. However, the authors thought that the 4 articles may be of interest to readers interested in the subject of DEI interventions. Therefore, the 4 articles were included in the table detailing all articles/interventions included in the final review (Table 1) and were also included in analyses of article characteristics.
Characteristics of Interventions Identified in the Final Literature Review.

Data Charting
One researcher (KAH) extracted all data and charted data using an Excel spreadsheet. The researcher extracted data on year published, profession (eg, medicine, nursing), training level(s) of participants or people targeted by the intervention, type(s) of diversity targeted by the intervention, organization that performed the intervention, location, specific name of the intervention (if any), goal(s) of the intervention, type of intervention, sample size, whether there was a comparison group, and type of study performed. Unfortunately, most articles did not include information on the type of study performed and researchers were not confident in their ability to extrapolate this information from the article itself. Therefore, information on study type was not included in the final analysis.
Data Categorization
Intervention types were categorized as follows: development program (development or training programs, internships, fellowships), mentorship, institutional change (any institutional change, large or small, such as creating a strategic plan or a new chief diversity officer position), pathway program (program that follows participants across multiple career stages in order to increase recruitment and/or retention), financial support (scholarship or grant), workshops, and other interventions that did not fit into one of the preceding categories. These categories were chosen posthoc by reviewing the interventions included in the final literature review and identifying common themes.
Many development programs include a mentorship component, and some mentorship programs include educational opportunities or other elements more typically associated with development programs. Interventions were classified as mentorship programs if mentorship was the main or only program element. Additionally, whenever possible, we used the intervention organizer's own categorization of their intervention as mentorship versus a development program.
Career stage was divided into 3 categories: student (residents, graduate and postgraduate students, and junior researchers), faculty/staff, and leadership. Leadership was defined based on self-categorization by individual articles. Any article that reported the intervention targeted “leaders” or “leadership” was included in the leadership category.
Profession was categorized as: medicine, nursing, dentistry, public health, or health science (researchers from multiple backgrounds or profession types engaged in health sciences research). No articles on physician assistants were identified.
The type of diversity targeted was categorized as: race or ethnicity, sex, LGBTQIA status, disability, socioeconomic status, religion, age, culture, and career interest. Interventions targeting a specific diversity type did not necessarily include only participants minoritized based on that diversity type. For example, an intervention designed to teach White participants about implicit racial bias would be categorized under the race or ethnicity diversity type.
Statistics
Descriptive statistics were calculated for all variables. Mann–Kendall test was used to determine whether a trend existed for the number of articles published by year. All descriptive statistics and analyses were obtained using R version 4.3.0 and RStudio version 2023.09.1.
Results
Article Characteristics
The initial search identified 3398 articles published on or after 1/1/2000 (Figure 1). After initial screen, 43 articles were reviewed, of which 32 met inclusion criteria. One of the reviewed articles 90 was a commentary on an original research article that did meet inclusion criteria. 51 The commentary was excluded, but the research article was added to the review. An additional 22 articles were identified following review of 4 pre-existing literature reviews identified by the search,22,31–33 for a total of 55 articles in the final review (Table 1). The maximum number of articles published in a single year was 6, in 2006 and 2009 (Figure 2). Mann–Kendall test showed an increase in the number of articles published per year from 2000 through 2023 (P = .004).
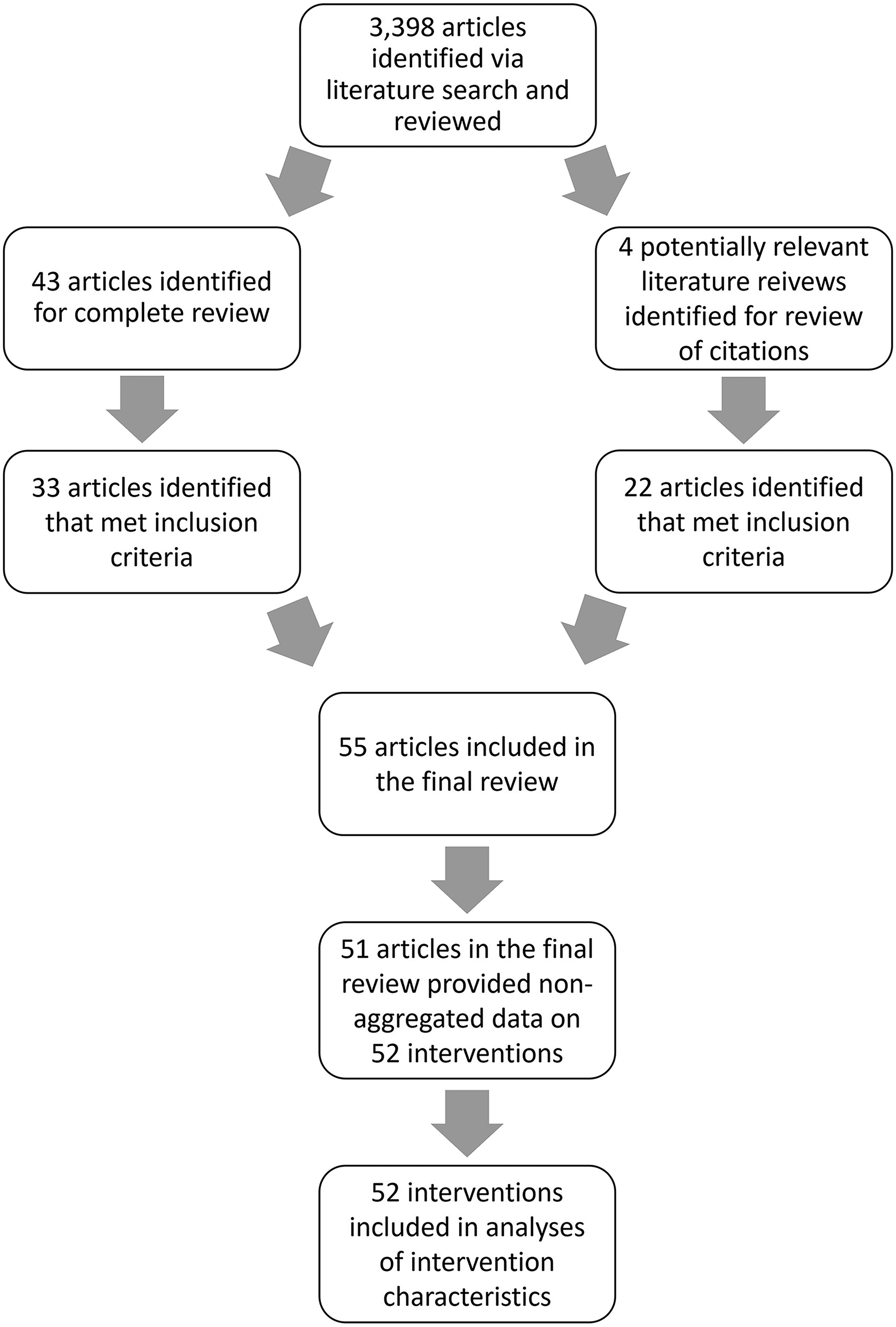
Flowchart of Study Selection.

Number of Articles Included in the Final Literature Review Published by Year.
Most articles (38, 69%) included no comparison group (Table 1). Eight (15%) articles included a comparison of before versus after the intervention,39,41,50,56,58,77,78,85 3 (6%) included a comparison between the intervention group and at least one other group,37,38,60 3 (6%) included both.48,49,54 One article detailed a randomized controlled trial 64 that included 3 intervention groups and one control group. One (2%) article 51 tested for deviation from a race and sex-neutral model and 1 (2%) article 91 used a retrospective design where pre- and post-intervention surveys were completed at the same time. Of the 55 articles, 4 aggregated and analyzed data from many interventions at different locations.35–38 These 4 articles did not include sufficient deaggregated data on individual interventions to be included in analyses of intervention characteristics. The remaining 51 articles detailed 52 interventions to promote workforce DEI.
Intervention Characteristics
The 52 interventions identified ranged in size from a single participant 53 to an entire healthcare system. 45 The interventions were implemented by multiple different types of organizations including academic and medical institutions,39,41–56,58–61,63–68,70–80,82–85,87,92,93 professional organizations,69,81,88,89 government agencies,40,53,67 and an academic journal that developed an internship for “racially minoritized physicians and PhD-trained medical educators living in the United States.” 86 Nine (17%) interventions included participants from across the United States.39,40,61,62,69,73,74,81,88,89 The remaining 43 (83%) interventions were spread across 25 states and Puerto Rico. The professions impacted by each intervention were: 28 (54%) medicine,39,44,47–51,58,61–63,65,66,70,71,74,75,77–79,82–84,86,88,89,92 11 (21%) nursing,41,46,52,53,55,56,67–69,72,80 8 (15%) health science,40,42,43,54,59,76,85,87 1 (2%) dentistry, 81 1 (2%) public health, 60 and 3 (6%) that involved multiple professions.45,64,73 Of interventions that involved multiple professions, 1 was designed to impact every employee in a healthcare system 45 ; 1 involved participants from health professions (eg, nursing, medicine) and nonhealth professions 64 ; and 1 involved primarily the medical profession, with some participants from professions including nursing, public health, health science, and pharmacy. 73
Three (6%) interventions did not specify the career stage of participants76,81,89 and 16 (27%) included participants from multiple career stages.45,46,50,55,64,66,73,77,82,84,85,87,94 Students were included in 33 (64%),39,40,42,43,45,46,50,52,55,56,59,60,64–68,70,72–75,77–79,82–85,87,88,92,94 faculty/staff in 28 (54%),44–51,53–55,58,61–64,66,71,73,77,80,82,84–87 and leadership in 5 (10%)41,45,49,69,73 interventions. Six (12%) interventions did not specify the type of diversity targeted48,69,76,79,83,84 and 10 (19%) specified multiple types of diversity.44,51,54,64,65,71–73,75,78 Types of diversity targeted were: 42 (81%) race or ethnicity,39–56,58–65,67,68,70–75,77,78,80–82,85–89 12 (23%) sex,44,51,58,64–66,71,73,75,78,92 4 (8%) disability status,54,64,65,75 2 (4%) age,65,73 2 (4%) LGBTQIA status,65,75 2 (4%) socioeconomic status,64,72 1 (2%) culture, 73 1 (2%) religion, 65 and 1 (2%) career interest. 73 The article that included career interest as a type of diversity did not give any further clarification of what was meant by the term “career interest.” 73
Types of Interventions
The most common intervention type was institutional change.45,46,50,61,62,65,71,78,82–84,92,95 We identified 14 (27%) interventions in the category of institutional change. Institutional interventions included any change, large or small, in the structure or workings of an institution designed to promote workforce DEI. These included the creation of a strategic plan,45,46,49,50,71,78,84 committee,45,49,50,61,78,83,93,96 department,46,49,71,82 or position 65 to promote workforce DEI or changes in the structure39,46,49,71,78 or selection process39,45,46,49,71,78,92 for existing departments and positions. These programs ranged in scope from the addition of peer nominations in the process for selecting a chief resident, 92 to multipronged interventions intended to effect changes throughout an entire healthcare system. 45
After institutional change, the next most common intervention types were mentorship40,41,58,63,64,69,74,76,85,88 and development programs,42–44,47,48,53,54,59,60,75,77,81,86,87 with 13 (25%) interventions each. Mentorship programs ranged in size, scope, and institutional support. Some papers described self-directed and self-organized mentorship groups with fewer than 10 participants.44,55 Other mentorship programs had greater than 1000 participants 40 or support from specific offices or programs at their institution.58,69,74,85,88 Some mentorship programs included other elements in addition to mentoring, such as educational opportunities41,85 and travel grants.74,85
Development programs included a variety of different internships, 86 fellowships, 53 and training programs.42,43,48,54,59,60,77,79,87 They ranged in size from a single fellow 53 to 120 participants. 77 Development programs included a variety of different elements, such as mentorship,42,43,47,48,53,54,59,60,75,81,86,87 educational opportunities,42,43,47,48,53,54,59,60,75,77,81,86,87 administrative or technical support,47,48,87 and financial support.53,59
We identified 5 (10%) pathway programs, which followed participants across multiple career stages to increase recruitment and/or retention.52,56,67,68,79 Four of the 5 identified pathway programs were designed to increase recruitment and retention of minoritized students in graduate level nursing programs.52,56,67,68 The fifth was designed to increase the recruitment and retention of minoritized medical students, residents, and faculty in academic medicine. 79
Two (4%) interventions provided financial support to participants48,72 and 2 (4%) consisted entirely of workshops.73,80 Three (6%) interventions did not fit neatly in a single category: the creation of an award to honor the academic work of scholars studying equity, diversity, and inclusion 89 ; the solicitation of individualized pledges to fight gender inequality 66 ; and the development of a toolkits to assist program directors in preparing for new graduate medical education diversity standards. 70
Discussion
Underrepresentation of minoritized groups in the healthcare workforce is an urgent problem that requires aggressive and sustained intervention from multiple stakeholders including healthcare systems, academic institutions, and governmental agencies. This literature review represents a collection of potential interventions and strategies to increase workforce DEI.
We identified interventions from across the United States and United States territories in fields including medicine, nursing, and health science. We also found interventions that were spearheaded by multiple different types of organizations, such as academic institutions, professional organizations, government agencies, and an academic journal. This demonstrates that interest and motivation to promote workforce diversity already exists across multiple fields and relevant stakeholders. The increase in the number of articles published yearly from 2000 to 2023 may also show increasing recognition of the importance of workforce diversity and interest in finding solutions.
The existing literature is also diverse in terms of career stage, with all career stages represented from students through leadership and type of intervention. We identified 6 different categories of intervention and 4 interventions that were too unique to categorize. Even within individual intervention categories, there was significant diversity in terms of intervention goal, scope, and specific elements. For example, development programs often included multiple elements, such as mentorship,42,43,47,48,53,54,59,60,75,81,86,87 educational opportunities,42,43,47,48,53,54,59,60,75,77,81,86,87 administrative or technical support,47,48,87 and financial support.53,59
The interventions included in this review also varied dramatically in terms of scope, effort, and resources required. Some interventions included only a single participant 53 or alteration in an existing process. 92 Others attempted to overhaul entire healthcare systems. 45
Although the interventions included in this review varied widely in characteristics such as intervention type, sponsoring organization, and scope, other characteristics showed considerably less diversity. For example, medicine was far overrepresented in the literature review as compared to other professions included in the review, such as dentistry. We did not identify any articles on interventions to promote DEI among physician assistants. It is unclear whether the underrepresentation of certain professions was due to a problem with the search criteria used to identify literature for this review or for a different reason.
Although we identified interventions aimed at all career stages from students through leadership, the number of interventions identified dwindled in leadership positions. We only identified 5 interventions designed to promote DEI in leadership positions. This oversight is crucial because leadership remains the least diverse part of the workforce.19,24–29,97–100 Additionally, leadership may have disproportionate control over their organizations’ culture, priorities, and resource allocation. 30 Minoritized leaders may be more likely to prioritize DEI, creating a virtuous cycle in which DEI among leadership begets more DEI throughout the entire organization.
Most articles focused on racial or ethnic diversity and, to a lesser extent, sex diversity. There is no doubt that these types of diversity are critically important. Women and people of color remain underrepresented in medical centers, healthcare organizations, and health professional schools, particularly in leadership positions.19,21,24–29 In particular, people minoritized based on race or ethnicity face many unique and pressing challenges. For example, the “minority tax,” which describes the extra responsibilities, such as mentorship and committee work, that underrepresented minorities are expected to shoulder.101,102 These extra responsibilities take time away from research and other activities necessary for career advancement.101,102 Because of these unique barriers, efforts to promote diversity in race, ethnicity, and sex are necessary to create a more just and equitable workforce and support for interventions must continue to expand.
In addition, many other minoritized groups also face unique challenges while progressing through the workforce hierarchy. These minoritized groups include, but are not limited to, sexual and gender minorities, people with disabilities, people from low socioeconomic status backgrounds, and certain religious groups. For example, sexual and gender minorities often need to decide when and if it is safe to disclose their identities15,103 and historically, many people with disabilities have been barred outright from entering medicine and nursing due to discriminatory technical standards.104,105 These additional types of diversity were unfortunately not well represented in articles found through this review. Going forward, we must expand our definition of DEI to include people from all minoritized backgrounds and design interventions tailored to their unique experiences.
Limitations
This study had several limitations. Only literature published in English was included in this review, which may have excluded relevant articles. There was overlap between many of the categories for intervention type. For example, development programs often included mentorship and/or financial support and mentorship programs sometimes included workshops or other resources in addition to mentorship. In cases where categorization was unclear, we deferred to the description of the intervention used by authors of the article.
The search strategy only included schools of dentistry, medicine, nursing, nurse practitioners, physician assistants, and public health. Other health professions were not included in the search strategy or in the final review. These professions include but are not limited to social workers, pharmacists, physical/occupational therapists, and mental health professionals other than psychiatrists. Additionally, dental schools were included in the search strategy, but dental clinics and dental centers were not included, which may have caused the exclusion of relevant papers on the dental field. Future researchers should examine the existing literature on interventions to promote DEI in these fields.
There may be articles that met inclusion criteria for this review but were not included in the final sample because they were not identified by the search criteria, because they were not included in the databases that were searched, or because of human error during the article review process. A single person completed all aspects of the review, including screening for article inclusion/exclusion, which introduces a risk of bias. An even larger number of interventions to promote DEI likely went unidentified because information on these interventions exists only in gray literature and has never been published in an academic journal.
Only articles published after 1/1/2000 were included in the final review. This date was not chosen based on a specific sociocultural or other demarcating event and is therefore somewhat arbitrary. There may have been articles published before 1/1/2000 that remain relevant in the current sociocultural climate or articles published after 1/1/2000 that are no longer relevant.
For articles that were included in the review, no information was collected on funding source. This is a major limitation because the interventions described in the articles were almost certainly influenced by their funding sources. However, without information on the funders, it is difficult to know how funding source influenced each intervention.
Despite these limitations, this review contains information on over 50 interventions from multiple professions, organizations, career stages, and types of diversity. Therefore, this review may represent a useful starting place for individuals, institutions, agencies, or other stakeholders interested in promoting DEI in the healthcare workforce.
Conclusion
Over the past 23 years, many different types of interventions have been trialed to promote workforce DEI in the healthcare workforce. These interventions have been diverse in terms of type, scope, location, field, institution, and career stage. However, some types of interventions remain underrepresented in the literature. Specifically, long-term, sustained interventions and interventions involving leadership; professions other than medicine; and types of diversity other than race, ethnicity, and sex. Despite these limitations, existing interventions represent a laudable effort to advance workplace equity. To achieve a diverse and equitable healthcare workforce, we must continue to support, study, and refine new and existing DEI interventions.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251333034 - Supplemental material for A Scoping Review of Interventions to Promote Diversity, Equity, and Inclusion in the United States Healthcare Workforce
Supplemental material, sj-docx-1-mde-10.1177_23821205251333034 for A Scoping Review of Interventions to Promote Diversity, Equity, and Inclusion in the United States Healthcare Workforce by Katherine A. Hill, Andrew W. Austin and Felicity T. Enders in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251333034 - Supplemental material for A Scoping Review of Interventions to Promote Diversity, Equity, and Inclusion in the United States Healthcare Workforce
Supplemental material, sj-docx-2-mde-10.1177_23821205251333034 for A Scoping Review of Interventions to Promote Diversity, Equity, and Inclusion in the United States Healthcare Workforce by Katherine A. Hill, Andrew W. Austin and Felicity T. Enders in Journal of Medical Education and Curricular Development
Footnotes
Authors’ Note
Preprint Server Disclosure: No preliminary report of this work has been previously published. Abstract Presentation: The content of this manuscript was previously presented at the Social Mission Alliance Conference in Durham, NC on 4/9/2024.
Acknowledgements
Thank you to Leslie C. Hassett MLIS for creating and performing the literature search used for this review.
Author Contributions
Katherine A. Hill: conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, and visualization. Andrew W. Austin: conceptualization, methodology, writing—review and editing, and visualization. Felicity T. Enders: conceptualization, methodology, resources, writing—review and editing, visualization, and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FTE has received grants from National Institutes of Health and Agency for Healthcare Quality Research in the form of payments to her institution. FTE has received honoraria from the following institutions: Mount Sinai, University of Washington, University of Minnesota, University of Rochester, Cincinnati University, the National Institutes of Health, Duke University, Wake Forest University, the Patient Centered Outcomes Research Institute, Johns Hopkins University. FTE has received support for attending meetings from the following institutions: The Association for Clinical and Translational Science, Cold Spring Harbor Laboratories. FTE has an unpaid fiduciary role for the Board of Directors, Association for Clinical and Translational Science. KAH received an education small grant from Mayo Clinic in the form of payment research materials. AWA declared none.
Data Availability Statement
All articles included in this review are available via Ovid MEDLINE®. The full search strategy is included in Supplemental file 1.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.