
Abstract
BACKGROUND
Domestic violence (DV) is a public health problem in the United States. Emergency physicians are often the first providers to see patients needing acute care for injuries sustained secondary to DV and are an important part of the healthcare workforce for underserved populations seeking help. While much has been published about the need for better identification and care of this population, little is known about the current prevalence and characterization of DV curricula in accredited emergency medicine residency programs.
METHODS
Cross-section survey of program directors sent to 232 Accreditation Council for Graduate Medical Education-accredited emergency medicine residency programs to learn about the presence, content, format, and barriers related to implementation of DV curriculum in their residency programs. The survey was open from May to June 2022.
RESULTS
A total of 63 programs responded (response rate: 26%). In total, 84% of programs reported having some form of DV curriculum, with the majority of respondents (81%) offering 1-5 h of content. Most programs included content on intimate partner violence (92%), child abuse (91%), and human trafficking (91%), but only 79% of programs had content on elder abuse. The most common modalities of DV curriculum implementation were didactic lectures (98%) and bedside teaching (51%). In total, 20.5% of 3-year programs had no DV curricula, while 44% of programs planned to implement improvements to their curriculum. The most common barriers to implementing additional education or further strengthening DV curriculum were lack of time in curriculum (69%) and lack of expertise in faculty (25%).
CONCLUSIONS
The majority of residency program respondents offer some formal DV curriculum with variation in the delivery modality and curriculum time dedicated to DV. There are existing solutions to address the barriers faced by the many programs that hope to improve their DV curriculum. Creative solutions, such as incorporating non-emergency medicine lectures or supporting faculty in bedside teaching, could help residencies meet the American College of Emergency Physician recommendation for integrating the DV curriculum into emergency medicine training.
Keywords
Introduction
Domestic violence (DV) is a broad term that is defined by the United Nations as a pattern of behavior in any relationship that is used to gain or maintain power and control. 1 It can include physical or sexual violence and emotional or psychological abuse. 2 While DV is often times used to describe intimate partner violence (IPV) alone, it also includes child abuse and elder abuse. According to the National Intimate Partner and Sexual Violence Survey (NISVS) in 2016/2017, 1 in 2 women in the United States (47.3% or over 61 million women) experienced some form of sexual violence, physical violence, and/or stalking by an intimate partner and reported an IPV-related impact during their lifetime. 3 Additionally, 10% of people 60 or older experience elder abuse 4 and 1 in 7 children experience abuse or neglect. 5 Many DV survivors seek care in emergency departments (EDs). For example, according to a study of the Nationwide Emergency Department Sample (NEDS) looking at almost 500 000 000 visits to EDs between 2006 and 2009, the mean average was approximately 28 000 ED visits per year that had a recorded diagnosis related to IPV. 6 Despite the prevalence of survivors seeking care in EDs, DV is often missed and likely contributes to the discrepancy between estimated rates of IPV and the number of ED visits with documentation identifying IPV.7,8 Research has shown that ED physicians only identify 4%-10% of IPV cases that present to the ED. 9 Similarly, 1/3 of children with injuries from physical abuse had previous visits where signs of abuse were not recognized on exam.10,11
Since 2018 the US Preventive Services Task Force (USPSTF) 12 has recommended that clinicians, across all settings, screen for IPV in women of reproductive age and provide or refer women who screen positive to ongoing support services. However, the USPSTF does not recommend similar screening guidelines for elder patients or children, citing a lack of evidence that outcomes are improved with routine screening in these groups. 12 Regardless of whether routine screening is recommended, physicians must know how to confidently identify potential signs of IPV, child abuse, and elder abuse; how to speak with patients about DV; and what resources are shown to be effective and available for patients in their community. Not only is there wide variability in ED provider screening frequency, but emergency physicians report varying degrees of comfort in their ability to identify and care for populations such as those affected by violence. 13 For IPV, elder abuse, and child abuse, providers often cite a lack of knowledge or discomfort talking to patients about abuse as barriers13-15. Nevertheless, research has shown that physician training and education on IPV can improve screening. 16
A 2013 WHO report found that women identify healthcare providers as the professionals they would most trust with the disclosure of abuse. 17 IPV survivors want their physician to ask “about how an injury occurred, history of violence, children's safety, support information and referrals, and follow-up appointments”. 18 Emergency medicine (EM) residents are often times the first physicians to encounter a patient who is experiencing abuse. While there has been a recent increase in available IPV curriculum geared toward medical students in response to the aforementioned USPSTF recommendations, 19 data is still limited on the quantity, quality, and implementation of IPV and broader DV curriculum specifically for EM residents. These areas highlight an opportunity for improvement and emphasize the need for a continuously evolving and survivor-focused DV curriculum, particularly within EM residency training programs. The American College of Emergency Physicians’ recommendation for a comprehensive DV curriculum in residency training is an opportunity for growth, as it highlights the need for education and training in recognition, assessment, and interventions for DV survivors. 20 For example, even brief interventions among healthcare providers have been shown to lead to significant increases in knowledge and efficacy in routine inquiry and referral services for IPV care. 21 A growing amount of evidence in the past decade has linked DV to multiple associated morbidities, including, but not limited to, HIV and other sexually transmitted infections, induced abortion, miscarriage, low birth weight or premature birth, intrauterine hemorrhage, hypertension, cancer and cardiovascular diseases, alcohol use, depression, and suicide. 22 Consequently, adequate screening and identification of at-risk patients could bolster efforts to provide resources and education that can mitigate these poor outcomes.
To characterize the present state of DV curricula in emergency medicine residency programs, we conducted a national survey of accredited EM residency programs on their existent DV curriculum. This study seeks to describe the prevalence of DV curriculum, trends in curriculum design, and any barriers to program implementation or growth. Our goal is to characterize current practices around DV curriculum requirements, to identify gaps in the DV curriculum landscape, and to identify opportunities for knowledge sharing and best practice implementation.
Methods
Study design
This study adheres to the Strengthening of Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cross-sectional studies (Supplement 1). 23 This was a cross-sectional survey of EM residency programs in the United States accredited by the Accreditation Council for Graduate Medical Education (ACGME). In May-June 2022, a 27-question online survey (Supplement 2) was distributed to 232 Emergency Medicine Residency programs whose contact information could be obtained. Only ACGME emergency residency programs whose contact information could not be found or was not otherwise up to date were excluded. Only residency program directors (PDs) were emailed the survey link, but either one PD or one associate/assistant program director (APD) per program could complete the survey. Our study was reviewed by the University's Institutional Review Board and deemed exempt from review.
Survey development and recruitment
Survey design began with the review of a similar questionnaire on disability health curricula for EM residents. 24 Items were adapted to fit this study's research focus on DV by EM faculty and researchers with content expertise in IPV. Questions included program characteristics and DV curricula presence, structure, and content. For the purposes of this study, we defined DV for respondents as “the intentional use of physical force or power, threatened or actual, that either results in, or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation” 25 which is directed towards children, elders, intimate partners, and other family members. Consequently, the survey contained questions on DV curriculum with respect to child abuse, elder abuse, and IPV. Additionally, we asked questions on human trafficking as this topic is commonly taught alongside IPV. Generally, programs operate on an 18-24 month curriculum rotation ensuring that all residents are exposed to a given topic at least once during their tenure. The survey pertained to any curriculum content in which DV education could have occurred. Face validity was assessed by EM resident review. 26
We used Qualtrics software [Qualtrics, Provo, UT] for survey distribution and data collection. In total, 232 of the 258 ACGME-accredited EM residency programs were emailed after obtaining PD or APD email addresses utilizing either the Council of Residency Directors directory, EMRA Match, or the program-specific website. Correspondence requesting study participation was sent on four separate occasions over the course of one month. The recruitment email specifically requested the survey to be completed by an individual from residency leadership who would have knowledge of their program's curriculum.
Data analysis
The primary outcome was the prevalence of DV education within the residency core curriculum. We calculated prevalence by analyzing the percent of programs that included formal content on DV, regardless of method of delivery, in their curriculum during the course of a single academic year, and the number of hours dedicated to DV content. Secondary outcomes included content areas, delivery methods, interest in expanding their DV curriculum, and barriers.
Data was cleaned and analyzed in Excel (Microsoft, Redmond, WA) and STATA (Release 18. College Station, TX). There was no missing data except for questions that were free response. Descriptive statistics were performed for each item. Univariate analysis was conducted with two-sided t-tests for continuous variables and chi-square tests for categorical variables. Significance for all statistical tests was set at P < .05.
Results
63 EM residency programs responded to the survey for a response rate of 26% (Table 1). In total, 70% (N = 44) of these were 3-year programs. In total, 84% (N = 53) of residency programs reported having some formal DV curriculum while only 16% (N = 10) specified that they did not have any formal DV curriculum. The median number of residents per program was 42 (IQR = 27).
Program Characteristics.

SANE, sexual assault nurse examiner; SART, sexual assault response team.
Description of domestic violence curriculum
The majority of responding programs provide between 1 and 5 h of dedicated DV curriculum while utilizing a variety of delivery formats (Table 2). There was no significant association between the number of hours of curriculum provided by programs and whether a program's clinical site had a sexual assault nurse examiner (SANE) or sexual assault response team (SART) onsite (P = .072). However, many programs that did have one utilized their SANE/SART team members to lead instruction on DV and IPV topics (N = 14). In total, 20.5% of 3-year programs (N = 9) reported having no DV curriculum, compared to 5.3% of 4-year programs (N = 1).
Domestic Violence Related Training Characteristics.
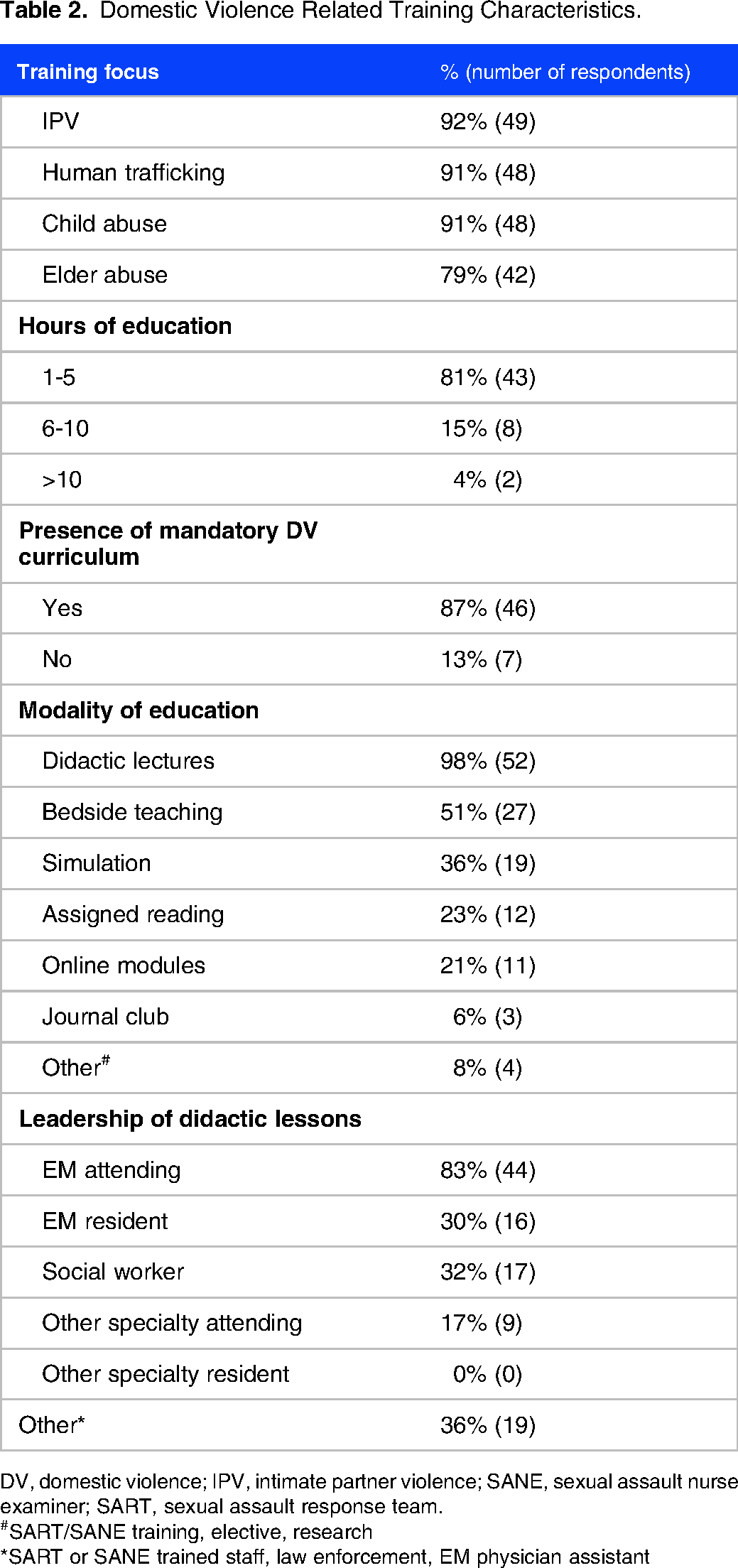
DV, domestic violence; IPV, intimate partner violence; SANE, sexual assault nurse examiner; SART, sexual assault response team.
#SART/SANE training, elective, research
*SART or SANE trained staff, law enforcement, EM physician assistant
For IPV curricula, 93% (N = 44) had content on signs/symptoms and 97% (N = 46) on recognition, whereas 68% (N = 32) included education on safety planning and state legal requirements (Figure 1). In total, 87% (N = 46) of all programs providing some form of DV curriculum describe it as a mandatory component, however only 64% (N = 28) of 3-year programs designate their DV curriculum as mandatory compared to 100% (N = 19) of 4-year programs (P = .04).

Domestic violence training curriculum content.
Description of barriers
The most common barriers to implementing or further strengthening DV education were lack of time in curriculum (69%, N = 42) and lack of expertise in faculty (25%, N = 15) (Figure 2). Only 15% (N = 9) of programs stated that they did not have any barriers to implementing DV education. When asked what future plans EM residency programs had to improve their DV education in the next three years, responses included refining and increasing the time spent on the subject matter in their curriculum, inviting community experts and SANE nurses to teach, and using simulation.
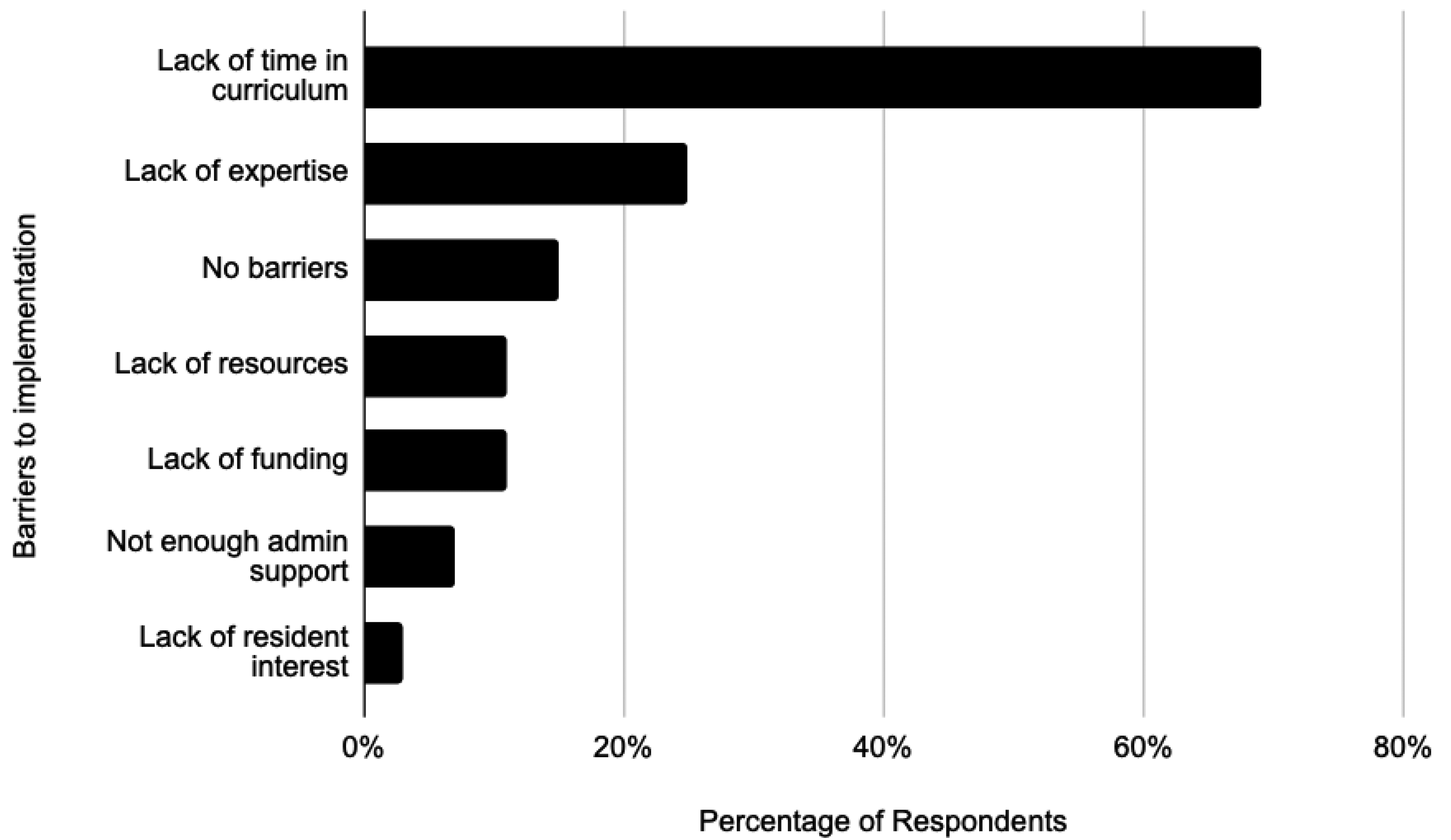
Barriers to implementation.
Discussion
Our data shows that 84% of residency programs currently offer formal DV curricula. The majority of EM residency programs that responded to the survey offer 1-5 h of curriculum. Almost all of these programs specifically include content on IPV, child abuse, and human trafficking, but fewer programs offer curriculum on elder abuse, a trend that is similarly found in other residency programs. 27 The largest barrier cited to incorporating or expanding upon current DV curriculum was lack of time, which is likely a significant contributing factor to the discrepancy between 3- and 4-year programs.
As physicians begin to address the growing needs of the global geriatric and elder populations (estimated to triple by the year 2050), 28 all EM residency programs will need to have high-quality education on elder abuse. Elder abuse is drastically underreported with an estimated 84% of cases never making its way to an adult protective service agency. 29 Yet, there is limited literature on elder abuse curricula in residency training, particularly in emergency medicine. 30 In an effort to support this growing need, educators from four California medical schools collaborated to create a modular 2-3 h curriculum that can be incorporated into emergency medicine residencies. 31 EM residency programs could benefit from similar resources and the development of specific guidance at a national level, particularly aimed at identification and screening of abuse.
Many residency programs have plans to improve upon their current DV curriculum, while still facing time restrictions to do so. Expanding DV curriculum time can be challenging, particularly for 3-year programs. Encouragingly, one study found that with even a total of 2.5 h of training on IPV, there was a significant impact on trainee knowledge, comfort, and likelihood of screening. 19 Additionally, residency programs may be able to offer training opportunities outside of traditionally dedicated didactic time during the week. Bedside teaching was cited as a way that 52% of programs provide education on DV to their residents. Ensuring that attending physicians have access to continuing medical education on DV would likely have a trickle-down effect that could benefit residents working shifts in the ED without requiring more time out of the weekly educational programming. Currently, online modules accounted for only 18% of the curriculum format provided by the residency programs, and further strengthening this delivery method could be an excellent way of implementing asynchronous learning for residents. One study on EM residents’ didactic format preferences found that asynchronous and online conferences rivaled that of in-person when taking into consideration retention of information, enjoyability, and preferability. 32 An even smaller portion (6%) of the residency programs noted that they provided journal clubs on the topic of DV. Journal clubs are a well-known way to supplement curriculum and focus on topics to better inform clinical practices, while also allowing for flexibility in delivery of curriculum. 33 The inclusion of more asynchronous learning opportunities for residents aligns with ACGME's desired shift to more individualized interactive instruction, with increased online modules and journal clubs being noted as a way to support this implementation. 34
Another commonly cited barrier was that many programs felt that they did not have the faculty or expertise available to provide DV training. Over 60% of programs answered that they have a SANE or SART program at their hospital while only 28% of programs have their onsite SANE/SART personnel lead didactic instruction on DV or IPV. Several programs indicated they have plans to start having their residents learn alongside the SANE/SART nurses while on shift. Utilizing the expertise and education opportunities of established personnel through interprofessional education (IPE), including specially trained nurses and social workers, is a resourceful way to incorporate approved ACGME milestones for EM residents and interns, and may be an additional untapped resource for many programs who may be impacted by the lack of readily available faculty expertise. 35 IPE has demonstrated improved understandings for a variety of educational opportunities including logistical learnings, scopes of practice, and team-based care, particularly in EM settings. 35 In addition to IPE instruction, there exists the possibility to supplement gaps in expertise or limited faculty availability by partnering with local DV shelters or sharing established online training modules by community-based organizations. 36 This collaboration would benefit the education of residents, and could foster long-term relationships between healthcare providers and groups that have more experience working with survivors of DV.
Limitations
The main limitations of this survey are small sample size and self-selection bias. With a response rate of 26%, there remains a large number of programs for which we have no data, making it difficult to generalize our findings. Without any information from these programs, it is difficult to fully assess the presence and characteristics of the DV curriculum in emergency medicine residencies nationally. Additionally, programs may have been less likely to respond if they do not currently have any DV curriculum available for their residents. Moreover, researchers in this study do not have specific content expertise in child or elder abuse.
Conclusion
Our survey of accredited EM residency programs reveals that while a majority of respondents incorporated formal DV curricula, significant variability exists in time dedicated to content delivery, modality of delivery, and barriers to implementation of additional DV education content. Ensuring the incorporation of elder abuse curriculum will be critical to the care of the growing geriatric population. The most cited barriers to enhancing the current state of the DV curriculum include time constraints and lack of faculty expertise, with many programs expressing plans for improvement despite these challenges. Strategies such as integrating IPEs, expanding asynchronous learning opportunities, or leveraging community partnerships could bolster curriculum delivery without imposing additional resource burdens. This study underscores the ongoing need for collaboration, innovation, and commitment among residency programs to strengthen DV education and ultimately enhance the care provided to vulnerable populations in emergency settings.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251324010 - Supplemental material for Landscape Analysis of Emergency Medicine Residency Education on Domestic Violence
Supplemental material, sj-docx-1-mde-10.1177_23821205251324010 for Landscape Analysis of Emergency Medicine Residency Education on Domestic Violence by Alana Harp, Michelle A. Gimenez, Adrené Garabedian, Maria Alejandra Ruiz and Jennifer A Newberry in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
Thank you Dr Cori Poffenberger for your guidance on our survey development.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contribution
A.H., M.G., A.G., and J.N. conceived and designed the study. A.H., M.G., A.G., and J.N. acquired and collected the data. A.H., M.G., A.G., J.N., and M.A.R. analyzed and interpreted the data. A.H., M.G., M.A.R., and J.N. drafted the manuscript. A.H., M.G., A.G., J.N., and M.A.R. provided critical revisions of the manuscript for important intellectual content. J.N. provided statistical expertise. A.H., M.G., A.G., M.A.R., and J.N. gave administrative and technical support. A.H., M.G., and J.N. supervised the study.
Data availability
Authors will consider data-sharing inquiries upon individual cases and requests.
Ethical considerations
Our study was reviewed by the Stanford University Institutional Review Board and deemed exempt from review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.