
Abstract
OBJECTIVES
To identify community preceptors’ views on the qualities and abilities required of physicians in community medicine, the education to acquire those qualities and abilities, and the factors affecting preceptors’ involvement in community-based teaching.
METHODS
We conducted semi-structured interviews with 13 male community preceptors in northern Japan who had at least 5 years of experience in community medicine and prior teaching experience with preclinical students. Participants were selected using purposive sampling to ensure diversity in clinical roles and institutional affiliations. A thematic analysis was conducted on verbatim transcripts to identify recurring themes.
RESULTS
Participants emphasized “communication skills,” “understanding the perspectives and backgrounds of patients and their families,” and “love for the community and its people” among the essential qualities and abilities for community physicians. They cited deepening relationships with and fostering an attachment to the community as necessary to cultivate these skills. The factors identified as facilitating community-based teaching included “positive emotions felt throughout the teaching experience,” “supporting hospitals and the wider community,” and “devotion to students.” Factors that hindered involvement included “perceived difficulty of teaching preclinical students” and “education-related issues at universities assigning students on placement,” such as the lack of opportunities for community-based teaching within the curriculum.
CONCLUSIONS
In line with the “social axis” in Worley's four Rs model, deep community involvement is essential to developing communication skills and patient-centered medicine. This study identified the qualities and abilities required for community physicians, as well as the educational activities needed to cultivate them from the early years of medical school. Strengthening collaboration between universities and community preceptors is vital to advancing community-engaged medical education (CEME). Cross-cultural studies could further explore how CEME operates in diverse contexts, contributing to socially accountable and community-responsive medical education.
Keywords
Introduction
Community-based medical education (CBME) was designed to provide teaching rooted in the local community in order to address the health needs of individuals together with those of their community, and has played a wide role in modern medical education.1,2 Defined as “medical education that is conducted outside a tertiary or large secondary level hospital,” 3 CBME aimed to engage with the local community and its health problems in a creative way while teaching medical students the key attitudes and skills that are applicable to both the local hospital and local people. 4
However, CBME has traditionally placed communities in a passive role, an approach drawing criticism because it neglects valuable local health perspectives and community input in shaping medical education. 5 ,6 As a consequence, the concept of “community-engaged medical education” (CEME) emerged. CEME represents a shift in the focus of medical education, moving from social responsibility, defined as an awareness of the duty to respond to the needs of society, 7 toward social accountability, defined as “the obligation of medical schools to direct their education, research and service activities towards addressing the priority health needs of the community, region, and/or nation they have a mandate to serve.” 8 This shift aligns with calls for medical institutions to address their social accountability, facilitating medical education that not only serves the institution but also directly benefits the health and well-being of the broader community.9,10
Building trusting and cooperative relationships between stakeholders (students, medical institutions) and the community is an important component of CEME that is fostered through authentic partnership.11–14 The key to this partnership is community preceptors (i.e., physician-educators who provide clinical training and mentoring in the community health care setting), who act as a bridge between the medical school and the community. In traditional CBME, preceptors were expected to serve as mentors and role models, encouraging students to reflect on morals, ethics, and values15,16 and to support the acquisition of foundational skills in holistic medicine, effective communication, and interprofessional collaboration.4,17 However, the voices of local people became lost in the education process amid an imbalance of power between the medical school and the local community. 5 The CEME model repositions communities as active contributors to the educational process, aiming for greater social accountability and responsiveness.5,12 Yet the role of preceptors in this model is not clearly defined.
Given the indispensable role that preceptors play in teaching students these community-oriented skills, as well as essential competencies such as patient-centered care and empathy,12,14 particular value should be placed on the unique insights of preceptors when developing and advancing CEME programs.
The commitment of preceptors to their teaching role in community-focused educational frameworks is driven by various intrinsic motivations. 18 Preceptors are often motivated by opportunities to update their own knowledge and contribute to developing future medical professionals, finding a sense of joy in education itself.19–22 However, the current community teaching structure relies heavily on altruism and lacks adequate institutional support. 23 Due to the increasing demands on preceptors, including clinical productivity pressures and challenges such as the transition to electronic health records, this reliance on voluntary support may be unsustainable.24,25 Barriers such as increased working hours for the preceptors themselves, conflicts in work–life balance, and a diminished relationship with the university have resulted in instances of physicians withdrawing entirely from community-based teaching (including CBME and/or CEME). 26 To date, most reports on community preceptors’ views about factors influencing community teaching have been in relation to clinical education,19–22,24,25,27 in which the factors relevant to preclinical students with limited medical knowledge were not identified.
Preceptors’ insights are currently underrepresented in the CBME and CEME literature. We therefore believe there is a need to explore preceptors’ views on the qualities and abilities required by physicians for effective community medicine, and the education that should be provided from the early years of medical school to cultivate these qualities and abilities. To bridge these gaps and to better understand the educational needs within community settings, this study focuses on two main research questions:
Research Question 1: From the perspective of community preceptors, what are the qualities and abilities required of community physicians, and what education should be provided from the early years of medical school for students to acquire and develop those qualities and abilities? Research Question 2: What do community preceptors perceive to be the factors that facilitate and hinder community-based teaching?
By elucidating preceptors’ viewpoints on these questions, this study aims to determine how CEME can be designed to balance educational goals with community needs, ultimately creating a more socially accountable, collaborative, and mutually beneficial framework for medical training. The findings may offer valuable insights for medical schools to achieve the shift from traditional CBME to CEME, fostering an educational model that not only strengthens the partnership between academia and community preceptors but also enhances community well-being.
Methods
Research approach and design
This study adopted a qualitative research approach rooted in an interpretive paradigm, allowing for an in-depth exploration of community preceptors’ perspectives on community-based teaching. We employed a descriptive and exploratory qualitative design, as it was well-suited to uncovering and describing the nuanced views and experiences of preceptors in the context of medical education in the community context. This approach was chosen to provide a foundational understanding that could inform future research in similar educational and healthcare settings.
Data collection
This study was targeted at physicians (preceptors) responsible for conducting community medicine training for medical students at community medical institutions in a prefecture in northern Japan. On the basis of the study's scope and the practical limitations of recruitment, we initially targeted 10–15 participants. The participants were selected to prioritize physicians with practical and educational experience of community medicine. Our selection criteria were: (1) a minimum of 5 years of experience in community medicine; and (2) prior experience of teaching early-year medical students in community settings. Of the 13 community preceptors we contacted, all 13 consented to participate in the study. The participants had clinical experience ranging from 10 to 48 years, with a mean of 32 years and a median of 38 years. The participants are affiliated with local clinics and hospitals, serving in roles ranging from staff physicians to senior leadership, such as clinic directors. This diversity of roles allowed us to capture a range of perspectives on community medical education. Each participant had worked at their respective community medical institution for between 3 and 30 years and had experience of responding to the 2011 Great East Japan Earthquake. It is important to note that the participant population was all male. This gender imbalance was reflective of the demographic characteristics of the target population involved in community teaching at the participating institutions.
We conducted semi-structured interviews with participants between May and August 2021. The primary author conducted all interviews face-to-face at locations chosen by the participants, ensuring a comfortable environment for open dialogue. Each participant took part in one interview session. Interview durations ranged from 30 to 70 min, and the conversations were recorded with a digital voice recorder after obtaining permission from the participants. We used the recordings to prepare verbatim interview transcripts. This study was conducted with the approval of the Ethics Review Committees of Gifu University School of Medicine (approval number: 2021-A216) and Fukushima Medical University (approval number: General 2021-330).
The interview included questions on the nature of the participants’ current involvement in community-based teaching, perceptions of factors facilitating or hindering their teaching activities, their relationship with the university, the qualities and abilities they consider most important for physicians working in community medicine, and the education that should be provided to students for those qualities and abilities to be cultivated. The first author created the interview question guide while referring to previous qualitative studies on factors affecting the implementation of medical teaching in the community,26,28,29 and the research team then reviewed the validity of the guide's contents. The finalized interview guide comprised of the following questions:
Please describe the nature of the education provided to medical students at your institution (including community placements and clinical clerkships). How are you currently involved in student education? Do you have any good experiences of teaching students from the early years of medical school? If so, please give specific details. Have you ever encountered any difficulties or had any trouble in teaching preclinical students? If so, please give specific details. What, if any, are the gaps between the demands of the university and the realities of the clinical setting in terms of student education? What qualities and abilities do you want students to acquire to become physicians in community medicine? What education do you think should be provided to medical students from the early years to cultivate these qualities and abilities? As a community physician, what message would you most like to convey to medical students?
Data analysis
In this study, we employed Braun and Clarke's thematic analysis, 30 following an inductive approach to explore the interview data. The research team comprised of four researchers from diverse backgrounds: an internist (YM), an education researcher (RI), and two medical educators (TS, CK). This multidisciplinary composition allowed for a broad range of perspectives. The analysis was conducted systematically using Braun and Clarke's six-phase process, 30 and a range of strategies were implemented to ensure rigor throughout each phase.
First, all researchers systematically reviewed the transcribed data to gain a comprehensive understanding of its content. This phase involved detailed reading and annotation of the text data to identify preliminary insights. Next, the text data were broken down into smaller units. Two researchers (YM and RI) independently performed the initial coding for a subset of the data to ensure diverse perspectives were captured. A codebook was developed iteratively during the initial coding process to standardize the coding scheme and promote consistency. Each unit was assigned a descriptive code, preserving its semantic meaning, and the codebook was updated to reflect emerging patterns. Following this, the research team collaboratively compared the results of the initial coding to identify broader patterns of meaning, generating preliminary themes. YM then applied these themes to code the remaining transcribed data, grouping the smaller units into more abstract categories.
All researchers reviewed and refined the initial themes to ensure they accurately represented the data. This involved cross-checking the themes against the original transcripts to confirm their alignment with the participants’ perspectives. We actively incorporated reflexivity into the process, maintaining reflective journals to document assumptions, biases, and decision-making processes throughout the analysis. The final themes were defined and named through collaborative discussions. This process included developing detailed analyses, identifying the focus of each theme, and articulating their overall narrative. Finally, we contextualized the analysis within the existing literature, employing data triangulation by comparing the interview data with field notes and relevant literature to enhance the credibility and reliability of the findings. The report was prepared in line with the Standards for Reporting Qualitative Research (SRQR) 31 (Supplementary Table: Checklist standards for reporting qualitative research). This ensured that the findings were presented in a rigorous and transparent manner.
Results
Qualities and abilities required of physicians in community medicine
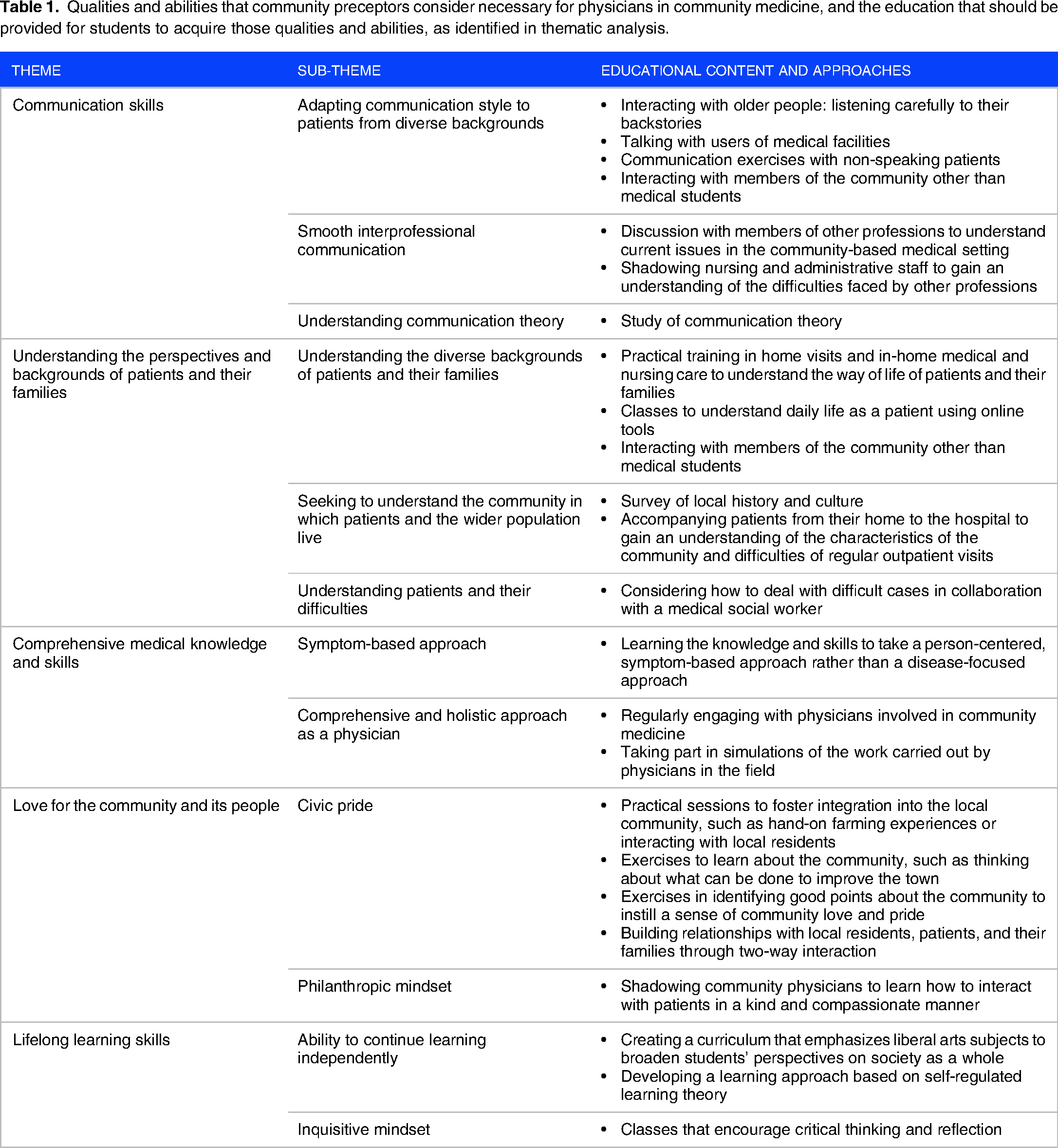
We identified five themes and 12 sub-themes relating to the qualities and abilities that participants consider necessary for physicians engaged in community medicine. The five core themes that emerged were: “communication skills,” “understanding the perspectives and backgrounds of patients and their families,” “comprehensive medical knowledge and skills,” “love for the community and its people,” and “lifelong learning skills.” In addition, we identified participants’ views on the type of education that should be offered from the early years of medical school to enable students to acquire these qualities and abilities. The themes, sub-themes, and proposals for related educational activities are described in Table 1.
Qualities and abilities that community preceptors consider necessary for physicians in community medicine, and the education that should be provided for students to acquire those qualities and abilities, as identified in thematic analysis.
Communication skills
Participants emphasized the importance of developing communication skills tailored to individual needs through diverse experiences and structured learning in community medicine. Developing the ability to communicate with patients from a diverse range of backgrounds is crucial for delivering care tailored to their individual needs. Because preclinical students are yet to acquire sufficient medical knowledge, participants instead wanted them to focus on learning the importance of interacting with people as human beings rather than solely as patients, such as through dialogue with older people living in care facilities. The participants believed that this would enable students to gain an understanding of the background of each patient and develop the communication skills appropriate for individual cases. [I told the students to] properly sit down with the user [patient] and listen to what they have to say. Basically, be friendly and talk to them for 30 minutes, without taking notes or anything, and then come back and present what kind of person they are. (Participant 2)
In addition, participants highlighted the importance of encouraging students to engage with professionals from other fields early in their medical education. They suggested that by interacting with other healthcare professionals such as nurses, dieticians, and pharmacists, students would develop a broader perspective on healthcare collaboration and learn how effective communication operates across disciplines. Talk to the nurses, dieticians, pharmacists, and so on … I think it would be great if [the students] became able to do that. (Participant 8)
Another participant pointed out the significance of introducing students to communication theory as a way to develop communication skills based on structured frameworks. They believed that such theoretical knowledge would enable students to approach communication more systematically and effectively in their future clinical practice. There is a thing called communication science – with proper theoretical frameworks and so on. By using that, they [the students] will be able to learn [to communicate] more effectively. (Participant 5)
Understanding the perspectives and backgrounds of patients and their families
Participants recognized that building relationships of trust with patients and their families is essential in providing patient-centered care, and that understanding the diverse backgrounds of patients and families is an important part of this. They believed that the most effective way for students in the early years of medical school to deepen their understanding was to accompany patients during home nursing or home medical visits. Such visits enable students to directly observe the patient's home environment, their way of life, and the way healthcare professionals interact with patients and their families. It's a rare experience to go into [a patient's] home. You get a completely different impression compared to a hospital room. You get a sense of their daily life. Whether it's pictures or other objects out on display, if you see something unusual and ask “What's this?” you can learn a lot about their history that you weren’t expecting. (Participant 12)
In addition, participants were concerned that interactions among the medical student community tended to be with people of a similar age and home environment, resulting in a lack of insight into the backgrounds of patients. Participants expected students to develop their communication skills and broaden their viewpoints through actively taking part in the local community, thereby interacting with people of different ages and varying social backgrounds. It's not good to stay in the confines of the university or school – things that you take for granted as a student become the norm. I think it's probably helpful to experience a few social settings away from the university – it doesn’t have to be a part-time job; it could be volunteering or even playing sports at a local club. (Participant 4)
Furthermore, participants believed that students would better understand the social backgrounds of patients and their families by cultivating a better grasp of the community, its history, and its culture. For these reasons, participants were aware of the importance of understanding patients with particular social and psychological issues, and therefore felt that it was necessary for students to examine complex cases of this type together with medical social workers. If you’re a physician who can properly take sociability, regionality, and local, religious, and social aspects into account, you’ll be popular… although I suppose ‘popular’ is a strange way of putting it… anyway, if you can do those things, you’ll also naturally gain the trust of patients, and I think people will think of you as providing reliable medical care. I think this helps you to better appreciate the joys of community medicine, and gets you more excited about the prospect of doing more of it. (Participant 9)
Comprehensive medical knowledge and skills
Participants noted the importance of acquiring the comprehensive medical knowledge and skills needed to view patients from a holistic, generalist perspective. For this purpose, they believed that it was necessary to incorporate a patient-centered, symptom-based approach, rather than an organ-specific, disease-focused approach. The patient-centered approach should be covered from the early years of medical school, in lectures and practical training both at the university and in community placements. The participants felt that students would expand their medical knowledge through such an approach, allowing an increase in the scope of medical care students could perform. In turn, this would allow students to move closer to becoming the type of physicians sought by patients in the community setting. The first thing is to initially examine the symptoms. In other words, from the point when the patient arrives and says they have this or that symptom, and asks what they should do, you don’t focus straightaway on a specific organ: you ask more about it and think about where the symptoms might be coming from. By repeatedly studying that approach, you’ll probably come to realize that this is what good physicians should do. (Participant 12)
Furthermore, to make students aware of the importance of acquiring the necessary comprehensive medical knowledge and skills, the participants believed that it was necessary for students to be exposed to physicians actively engaged in community medicine on a regular basis. I think the best way of developing students is to take them out into the community and regularly expose them to physicians who practice with the mindset of seeing and treating everyone and everything. (Participant 13)
Love for the community and its people
Participants perceived that it is important not only to be familiar with a community's culture and history, but also to show a deep understanding and empathy for the issues faced by its residents. This extends to having a love for the community as a whole and a desire to improve it. The participants believed that students should deepen their direct interactions with local residents and experience the realities of the community firsthand through participating in local events and community volunteering activities from an early stage of medical school. The participants hoped that students would, through this process, develop a sense of attachment to the community, discover how rewarding community medicine can be, and at the same time, explore what they can do to contribute to the community. Even though it's called community medicine, I think an important part of the experience is for [students] to establish whether or not they like the area and want to settle there. I think it would be even better if we could build a system or create chances for [students] to get to know and like the local area, rather than just attending classroom-based lectures at the university. And if there were opportunities to interact directly with patients, students would get a better understanding of how rewarding community medicine can be, and how much it's needed by local people. (Participant 13)
Furthermore, having deep empathy and kindness toward not only patients but the whole community is an essential quality for all medical professionals. The participants believed that the presence of role models who provide health care rooted in compassion and love for humanity would have a major impact on medical students and how they carry out their duties in the community in the future. They hoped that such experiences and meeting such role models would make students aware of their own potential role in community medicine, laying the foundation for their development as community-rooted medical professionals. In the long term – not one or two years, but 10 or 20 years or more – working as a community physician requires [kindness and compassion], and I want students to develop those qualities… There are a lot of community physicians working really hard, and I want students to look at them [as role models] and to take a similar – but not necessarily the same – approach to their own work” (Participant 8)
Lifelong learning skills
Participants emphasized the importance of actively updating knowledge and skills in line with advances in medicine, as well as improving humanity through learning gained from everyday life. They believed that it is important to foster a proactive attitude toward learning through liberal arts education, starting in the early years of medical school, to break away from the tendency toward the cramming of medical knowledge into medical education. I do worry that there is more and more early exposure [to medical knowledge] entering the curriculum, and that this neglects the need to give students opportunities to learn broader life lessons… I wonder if more time should be spent on this, whether you think of it as basic education or advanced education. (Participant 5)
Through their long careers as physicians, participants recognized the importance of maintaining an inquisitive mindset, constantly questioning, and refining critical thinking skills. They emphasized that critical thinking, reflexivity, and self-reflection are essential for lifelong learning, enabling physicians to adapt to the evolving challenges of community medicine. Critical thinking involves analyzing and evaluating information to make reasoned judgments, which participants believed is essential for navigating the complexities of community medicine. Reflexivity, on the other hand, was described as the ability to examine one's own assumptions, biases, and roles within a given context, allowing for a deeper understanding of one's influence on decision-making processes. Self-reflection complements these skills by encouraging individuals to look inward and assess their own values and motivations, enabling socially responsive and contextually relevant solutions in community medicine.
Participants noted that fostering these skills—critical thinking, reflexivity, and self-reflection—requires a cultural shift in medical education from focusing solely on knowledge acquisition to promoting inquiry and introspection. They hoped that students would develop an interest in the community and acquire the ability to engage in these practices from the early years of medical school to support their lifelong learning and adaptability. I want [students] to always start by asking ‘why?’ That includes, first of all, asking themselves why they want to be a physician. And then, if they say they want to work in community medicine, asking themselves ‘why community medicine?’ I feel that leads to more in-depth learning and deeper understanding… [For preclinical students,] I think it’s fine to talk to them about finding their own questions for themselves. (Participant 1)
Factors facilitating community-based teaching for preclinical students
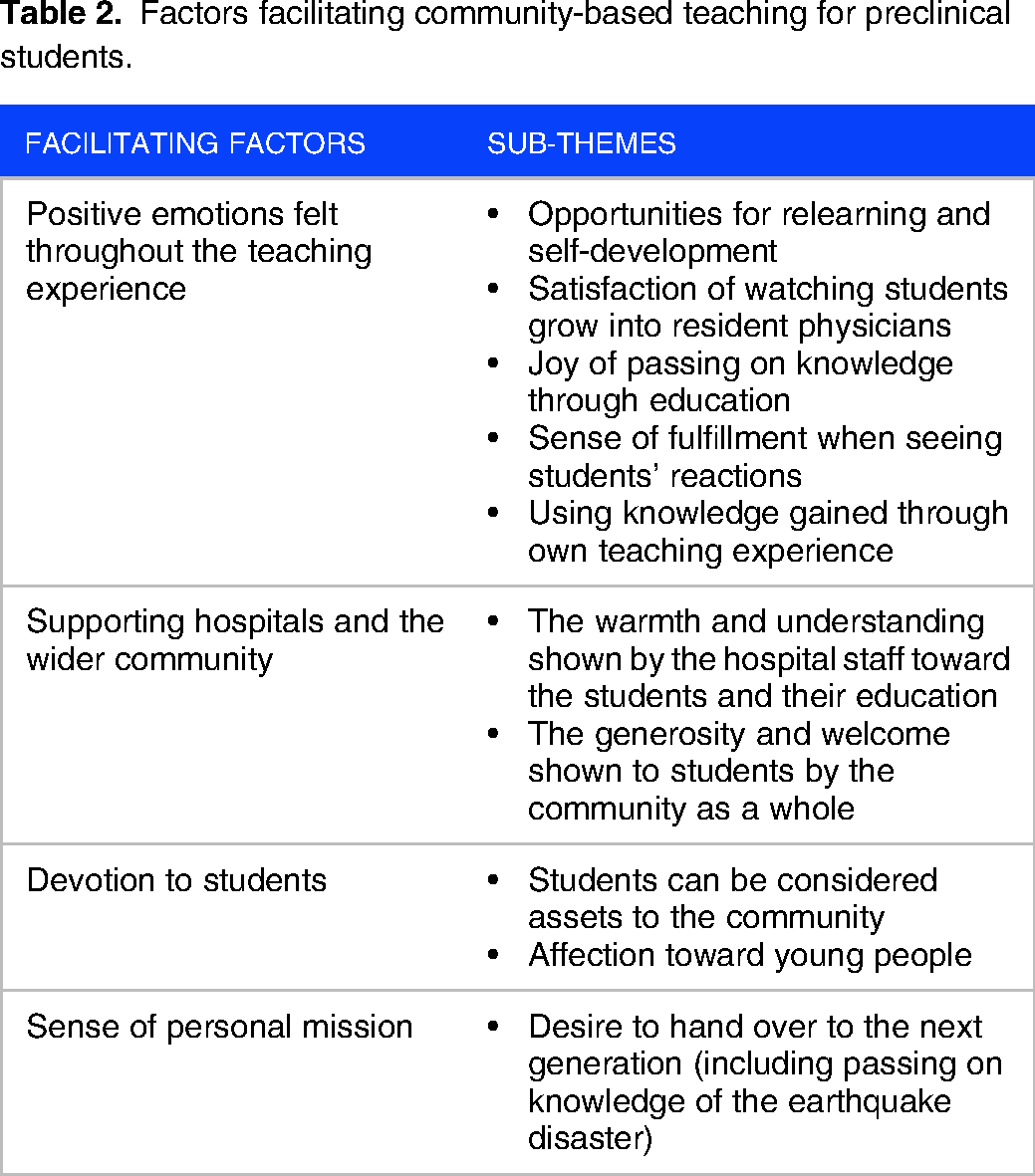
The factors that community preceptors believed to facilitate community-based teaching for preclinical students were categorized into four themes: “positive emotions felt throughout the teaching experience,” “supporting hospitals and the wider community,” “devotion to students,” and “sense of personal mission.” The four identified themes and their sub-themes are presented in Table 2.
Factors facilitating community-based teaching for preclinical students.
Positive emotions felt throughout the teaching experience
Positive emotions experienced when educating students was one of the strongest motivators for participants involved in community-based teaching. The participants themselves needed to search for and explore new information in order to impart knowledge to the students, and considered educating to be a valuable opportunity for self-development as a physician. The positive reactions and attitudes shown by students during the teaching process increased the participants’ motivation to be involved in community-based teaching. It's a good thing to have some external pressure, to know that someone else is watching you, as it makes you want to stay up-to-date; hence it's good for doctors and nurses to have student trainees come to the hospital regularly. (Participant 4; Sub-theme: Opportunities for relearning and self-development)
In addition, participants found it highly rewarding to watch medical students they had taught from the early grades develop into resident physicians, and to have the opportunity to pass on ethics and values to the next generation through working together. I’m really happy that the number of younger colleagues who understand and positively view the [community medicine] work I do is increasing. It's great to see them develop. (Participant 9; Sub-theme: Joy of passing on knowledge through education)
Participants felt that these experiences were often opportunities to apply the knowledge they had gained through their own teaching experience, and that taking part in teaching was a way to give back to and further develop the community, which contributed to increasing their passion for education. I think that there are difficulties and joys [in community medicine] that students wouldn’t experience if they just passively observed our work rather than trying it for themselves, and seeing their reactions is so rewarding – their satisfaction of having done it, and their desire to carry on doing it. (Participant 11; Sub-theme: Sense of fulfillment when seeing students’ reactions)
Supporting hospitals and the wider community
Participants recognized that community-based teaching cannot succeed through the efforts of individuals alone, but relies on the support of a multidisciplinary medical team, including administrative staff, as well as the wider community. In fact, staff at many community hospitals came together to warmly welcome students starting placements, and there were even instances of local municipal authorities holding events to make students feel welcome. Basically, the students are really welcome, so just by coming to the hospital they get a warm reception, and when the other staff hear that we’ll have students on placement they always make an effort to say ‘good morning’ to them and so on… We try to make sure that we foster that kind of atmosphere. (Participant 1; Sub-theme: The warmth and understanding shown by the hospital staff toward the students and their education)
Local residents were also positive about medical students being educated in their community, showing a generous and tolerant attitude toward community-based teaching. Such support from hospitals and wider communities was a key factor in encouraging preceptors to engage in educational activities. A lot of local people are really cooperative, treating [the students] as doctors for the community. I think it might be a regional thing – they’re really warm and accepting. (Participant 8; Sub-theme: The generosity and welcome shown to students by the community as a whole)
Devotion to students
Participants stated that a deep affection for and devotion to students was an important motivator for their active involvement in community-based teaching. They believed that this affection was the reason for their strong desire to deepen their relationship with students through education, and that this deepened their own passion for the teaching activities themselves. I do find myself saying how great it would be if the students who have been here on placement come back to do their initial training and go on to become duty physicians here later on. It takes time to reach that point of course, but I really feel that students are assets [to community medicine]. (Participant 1; Sub-theme: Students can be considered assets to the community)
Moreover, participants felt a sense of responsibility to carefully nurture young people to achieve their potential, viewing students as a “treasure” of the local community. I love students and young people; unfortunately, I’m often too busy to spend as much time with them as I’d like, but when they come on placement, I try to have lunch with them and so on. (Participant 11; Sub-theme: Affection toward young people)
Sense of personal mission
The participants saw it as their responsibility to ensure that their experiences—particularly of the Great East Japan Earthquake and nuclear disaster, and their continuing work in the rehabilitation and transformation of the community since—were passed on to students, who are future leaders in the field of medicine. In their role as guardians of the local community, participants felt that passing on this knowledge to the next generation was an important motivating factor for their teaching work. I’ve been watching things change in community medicine in this area for many years. I’d like to share my experience with the next generation, and if at least some of the students can benefit from that knowledge in their lives as physicians, I’ll be glad. (Participant 5; Sub-theme: Desire to hand over to the next generation, including passing on knowledge of the earthquake disaster)
Factors hindering community-based teaching for preclinical students
Five themes emerged for factors that community preceptors believed to hinder or inhibit community-based teaching for preclinical students: “impacts of COVID-19,” “perceived difficulty of teaching preclinical students,” “issues with students’ approach to thinking and attitude to learning,” “lack of resources at medical facilities taking on students,” and “education-related issues at universities assigning students on placement.” The five themes and their sub-themes are listed in Table 3.
Factors hindering community-based teaching for preclinical students.

Impacts of COVID-19
The COVID-19 pandemic, which began in early 2020, brought about marked changes to the format of medical student teaching. At the time of data collection, the impacts of the pandemic were still being strongly felt, forcing a change from face-to-face training to an alternative format featuring online hospital tours and lectures. I tried to set up a placement in home nursing care for students, but was told it wasn’t possible because of COVID-19. (Participant 1; Sub-theme: Changes in the format of practical training)
The participants recognized the inherent dangers not only in the limited direct contact between students and patients, but also in the significantly reduced opportunities to interact and communicate with local residents. For the participants, who place great importance on direct face-to-face interaction with patients and the wider community, the impacts of the pandemic were particularly severe and presented a major obstacle to achieving their ideal form of community-based teaching. It would be good for the students to have the chance to talk with a range of different people, but we’re totally stuck because of the pandemic. (Participant 7; Sub-theme: Reduced opportunity for direct communication)
Perceived difficulty of teaching preclinical students
Participants were accustomed to teaching knowledge of diseases and clinical skills to students through programs such as the clinical clerkship. However, many were unsure how to teach preclinical students appropriately, given the lack of medical knowledge possessed in the early years of medical school. The participants also raised feelings of unfamiliarity with teaching preclinical students because of the lack of opportunities to interact with those students within the preclinical curriculum. Everyone is now worried about what to do when preclinical students come on placement… I think fifth- and sixth-year students can be taught things like medical procedures and how to read tests, but preclinical students probably can’t. (Participant 7; Sub-theme: Difficulty of practical teaching activities suited to the readiness level of preclinical students)
Furthermore, participants felt that their values and the education they had received in the past were not necessarily compatible with today's students, resulting in a perceived gap in mindsets and a sense of loneliness. You tell students stories about your time training as a doctor [such as staying all night at the hospital to care for a patient], but they tell you very clearly that their generation wouldn’t do things like that. When you talk directly to young students you soon realize they have a different mindset. (Participant 11; Sub-theme: Generation gap between students and their supervisors in terms of their views and beliefs about learning)
Issues with students’ approach to thinking and attitude to learning
Participants perceived one of the barriers to community-based teaching to be the passive attitude and lack of reaction or enthusiasm from students on placement. They were also concerned that students tended to judge situations in terms of simple “right or wrong” and lacked the flexibility to take patients’ social backgrounds into account. There are some students who only think of things in terms of good or bad, right or wrong – just two choices… When I tell students that you have to give a patient the treatment they want, there are some who say ‘no, no, you can’t do that – isn’t that wrong?’… It's really hard to mentor and develop them if they’re inflexible like that. (Participant 1; Sub-theme: Lack of flexibility)
In particular, participants raised concerns that medical students were too fixated on a formulaic approach during medical interviews, overlooking the importance of seeing the patient as a person. [I say to the students] let's just listen to what the patient has to say, or let's just show some interest in the patient, as that's enough for the moment. After all, patients can sense when you’re not genuinely interested, even though it's natural for students to be nervous. But if you don’t show any interest, or don’t try to find out more about the patient, you won’t get anywhere. (Participant 12; Sub-theme: Lack of interest in the patient as a person)
Participants also felt that medical students’ lack of deep interest in and concern for others hindered students’ own development and inhibited cultivation of the altruism and empathy needed to become a good medical professional in the future. Students are rather passive; they respond if I tell them what to do, but they don’t really say what they want to do for themselves. (Participant 8; Sub-theme: Passive response and lack of inquisitiveness)
Lack of resources at medical facilities taking on students
Budgetary constraints at the medical facilities accepting students on placement, as well as limitations on human resources, including medical faculty who could act as preceptors, created a gap between the participants’ ideal teaching content and the education that could be offered in practice. I go to people's homes to provide home medical care at short notice, so if I were told to go and look after a patient while taking a couple of students with me, it would be pretty challenging. The families would find it hard too, so many people turning up at once. (Participant 2; Sub-theme: Limitations on the number of students who can be accepted)
Participants also cited constraints on the university side as a factor causing this issue. Similarly, participants noted that it was necessary to conduct teaching within the limited time available to fully carry out their clinical responsibilities, and highlighted their frustrations at being unable to provide adequate instruction to their students as a result. If possible, I’d want the students to speak with patients more and to do proper medical interviews with them, but you still have to do all your usual medical examinations during that time, so when it's really busy, you end up just neglecting the students. (Participant 4; Sub-theme: Difficulty in securing teaching time during clinical practice)
In addition, the lack of staff within their hospitals who shared their enthusiasm for education made the participants feel isolated in their role as preceptors, increasing their anxiety about teaching work. In hospitals like ours, not all the doctors see the point of teaching others or have much enthusiasm for it. (Participant 11; Sub-theme: Lack of staff with enthusiasm for education) Because I’m community-based, I’m not a member of the medical faculty and don’t get to spend time in the office with other physicians or anything, so it can sometimes feel a little lonely and isolated. I think that if I was allowed to be part of the Medical Education and Development Center, or be involved in something like that, I’d be able to do more self-development and study…. (Participant 9; Sub-theme: Sense of loneliness)
Education-related issues at universities assigning students on placement
Participants were concerned about the lack of opportunities for community-based teaching created by universities and the ongoing shift toward increasingly advanced and specialized education. They were also concerned that the shortened period available for education before the start of the clinical clerkship would create a trend toward cramming medical knowledge into the lower grades of medical school, resulting in a further decline in students’ interest in community medicine. Participants also acknowledged the proposal that medical students in the lower grades should be given more community-based education opportunities, particularly for those interested in community medicine, to compensate for the general lack of such teaching in the pre-clinical clerkship curriculum. Although doing a series of clinical lectures to third-year medical students probably helps them retain some knowledge [of community medicine], during the rest of medical school they get more and more specialized, and I’m honestly concerned that they will end up forgetting it. (Participant 9; Sub-theme: Lack of opportunities for community-based teaching) There's far more time given to education within the university hospital, but in reality, the specialized medical care provided at university hospitals is only a very small part of the overall medical care across Japan. Really, the majority of educational time should be spent in community medicine. I think that gap between actual clinical practice and medical education is, for better or worse, coloring the views of the next generation of physicians. (Participant 13; Sub-theme: Decrease in students’ interest in community medicine owing to high degree of specialization in curriculum)
In addition, participants identified the lack of a formal education system for physicians to follow in the clinical setting as an issue, and noted that teaching is left to the preceptors at individual medical facilities without adequate support from the university. I think there are some community physicians in the field who don’t really know how to give good feedback or to properly review students in educational terms. (Participant 4; Sub-theme: Insufficient education and backup systems for physicians working in the field)
Furthermore, participants cited the lack of proper evaluation of the teaching provided as a barrier to community teaching activities. It gives me a real headache. It seems strange to say that education work doesn’t really marry up with clinical practice, but teaching doesn’t seem to be treated as a positive in our line of work. (Participant 8; Sub-theme: Educational work not evaluated fairly)
Discussion
Qualities and abilities required of physicians in community medicine
The first part of this study, relating to Research Question 1, focused on the qualities and abilities that are required of community physicians from the perspective of preceptors. Through interviews with preceptors, we identified five themes: “communication skills,” “understanding the perspectives and backgrounds of patients and their families,” “comprehensive medical knowledge and skills,” “love for the community and its people,” and “lifelong learning skills.” These results reflect the qualities and abilities that preceptors consider most important in the context of community medicine, and we were therefore able to extract items that differ from the qualities and abilities listed by general medical education organizations.32–34
Three of the five core themes that emerged can be considered to fit within the framework of patient-centered medicine. 35 Specifically, the themes “communication skills,” “understanding the perspectives and backgrounds of patients and their families,” and “comprehensive medical knowledge and skills” overlap with the four interrelated components of the patient-centered clinical method defined by Stewart et al. 35 : (1) exploring health, disease, and the illness experience (i.e., understanding not only the medical condition but also how it affects the patient's life and personal experiences); (2) understanding the whole person (i.e., considering the patient's life history, social context, and psychological needs, and viewing them as a whole rather than as isolated symptoms); (3) finding common ground (shared decision-making to align the medical approach with the patient's values, preferences, and expectations in diagnosis and treatment); and (4) enhancing the patient–physician relationship (i.e., building a trusting, respectful relationship that fosters open communication and empathy). 35 Our participants believed that “communication skills” are closely related to “understanding the perspectives and backgrounds of patients and their families,” and that without a full understanding of the patient's background, which is rooted in good communication, it is not possible to provide the right treatment. Communication with the patient is essential across all four components of the patient-centered clinical method. 35 One-way instructions from the medical provider or a conversation that does not extend much beyond a greeting does not allow for a deep understanding of the patient's background, and risks leading the patient toward a treatment that they do not want, which in turn could have a negative impact on their health.36,37 The community preceptors recognized the importance of communicating with patients and their families to understand their family relationships, roles at home, and their daily life within their community, thereby allowing patients to share what is important in their lives, which can then inform the course of their medical care. The preceptors also believed that it is important to take an approach that considers both the family members and the wider community surrounding the patient. This aligns with the view of McDaniel et al. 38 that the primary care physician should always consider the patient's “family tree.” 38 This suggests that the participants believed this approach would lead to a more comprehensive understanding of, and ability to provide care to, each individual patient.
Perhaps the most distinctive of our results is the theme “love for the community and its people,” which we consider to be essential for physicians with a deep involvement in their community over the long term. The World Health Organization considers “social capital” to be an important social determinant of health. 39 In the context of community medicine, it is important for medical institutions, local residents, government, and other related organizations to work together to form and develop social capital. 40 This study suggests that the ability to form a deep love and affection for one's community and to continuously look for ways to improve it is extremely important in community medicine.
This study additionally reveals that preceptors place importance on educating preclinical students in a way that includes active involvement with the community. Worley15,41 proposes the “four Rs model” as a comprehensive framework for education, focusing on four central relationship axes to achieve a successful CBME curriculum: (1) clinicians and patients (“clinical axis”); (2) health service and university research (“institutional axis”); (3) government and community (“social axis”); and (4) personal principles and professional expectations (“personal axis”).15,41 In this model, particular emphasis is placed on the social axis, which is defined as “the relationship between government policy, law, funding constraints and initiatives on the one hand, and the demographic, geographic, cultural and epidemiological needs and determinants of society on the other,” 15 and is closely related to the CEME philosophy. 5 In other words, community medicine is built upon completely different social contexts in each community, and it is therefore important to learn about the community outside the confines of the medical institution. 15 In this study, preceptors raised “interacting with members of the community other than medical students,” “practical sessions to foster integration into the local community, such as hands-on farming experiences or interacting with local residents,” and “exercises in identifying good points about the community to instill a sense of community love and pride” as educational activities that they would like to provide to students in the early years of medical school. All these activities can be considered to fall within the social axis of the four Rs model, supporting the idea that preceptors act as a bridge between the medical school and the community.
Furthermore, while home nursing visits and home medical care include aspects of Worley's clinical axis (clinician–student–patient) and personal axis (personal principles–student–professional practice), community preceptors also wanted students to learn about the daily life, culture, and social background of patients through these activities. It is therefore clear that the social axis is also an important aspect of these lessons. For preclinical students with limited medical knowledge, even if they are unable to fully understand the patient's medical condition, such opportunities to gain a micro-level perspective of an individual patient's daily life can be considered to foster a macro-level perspective of the wider community in which the patient lives. Learning that falls within the social axis is also in line with the view of Frenk et al. 42 that there should be “Expansion from academic centres to academic systems, extending the traditional discovery-care-education continuum in schools and hospitals into primary care settings and communities, strengthened through external collaboration.” 42 It became clear that preceptors working in community medicine also believe that education should be centered around the social axis from the early years of medical school. If there is no intentional emphasis placed on the social axis, there is a risk that students will solely focus on the clinical axis or personal axis. 15 It is therefore necessary for educators to actively communicate the micro and macro perspectives of community medicine to students, which is an important part of social accountability. Achieving a more socially accountable curriculum is one of the key drivers of the shift toward CEME.
Factors facilitating and hindering community-based teaching
The second part of this study, relating to Research Question 2, identified factors that community preceptors believed to facilitate or hinder their involvement in community-based teaching activities for preclinical students. Four themes emerged as facilitating factors: “positive emotions felt throughout the teaching experience,” “supporting hospitals and the wider community,” “devotion to students,” and “sense of personal mission.”
Similarly to previous studies,19–22 preceptors often cited “the joy of educating” as a major motivator, but a notable finding of the present study was their motivation to watch students grow and develop from the early grades of medical school. This suggests the importance of regular educational opportunities to interact with students. Furthermore, this study revealed that the local community's tolerant attitude toward students and the warm welcome given by hospital staff and the whole community to students on placement were important facilitating factors for community teaching. The willingness of local residents to accept medical students in spite of their limited medical knowledge is indispensable and of great value not only to students but also to preceptors. Takamura et al. 6 reported a case in which the active involvement of local residents in education had a positive effect on both the residents and the learners. 6 The future development of educational approaches in which the local community can be actively involved is also desirable from the perspective of CEME. 5
The following five themes emerged as factors hindering the implementation of community-based teaching: “impacts of COVID-19,” “perceived difficulty of teaching preclinical students,” “issues with students’ approach to thinking and attitude to learning,” “lack of resources at medical facilities taking on students,” and “education-related issues at universities assigning students on placement.” Many of the factors cited by preceptors relate to the institutional axis (health service–student–university research) of Worley's four Rs model. 15 The present study revealed that some preceptors currently feel a sense of loneliness and isolation as they balance their community-based clinical and teaching responsibilities, either working with only a small team or sometimes entirely alone. In addition, the results suggest that the dominance of the “urban, technologically intensive, and specialty-dominant” medical school culture, 43 which does not give a positive impression of community medicine and general practice in medical education, also amplifies the sense of loneliness among community preceptors. Regarding the perceived difficulty of teaching preclinical students with limited medical knowledge, the university side also holds some responsibility for this issue through its outsourcing of education activities to community-based physicians without adequate assistance. To better support community preceptors, it is necessary for the university to provide fair evaluation, to develop a closer relationship, to take responsibility for giving feedback, to provide sufficient resources to mentor preceptors with educational advice and guidance, and to conduct appropriate faculty development based on these measures. 22 Preceptors also identified other important measures, including support for and fair evaluation of preceptors, strengthening relationships with universities, and building networks of preceptors across communities. Incorporating such measures within CEME would enable more effective implementation of the education needed for students to acquire the qualities and abilities of community physicians, as raised by the preceptors who participated in this study.
Limitations
This qualitative study has several limitations. First, while qualitative research does not aim to generalize findings in the same way as quantitative research, it does provide valuable, in-depth insights into preceptors’ perceptions of community medicine within the specific region studied. These findings contribute to a rich understanding of CEME that can inform similar initiatives in comparable contexts. Future studies—quantitative, qualitative, or mixed methods—could expand upon these results to further explore the broader applications of CEME. Additionally, further research could benefit from detailing the wider social and healthcare context within which this study was conducted to enhance relevance to other settings.
Moreover, while the interviewers in this study were university faculty members, which may have introduced a degree of participant reticence in discussing sensitive issues related to university policies or barriers to community-based teaching, we took several steps to encourage openness. We assured participants of the confidentiality of their responses, and the study emphasized its focus on gathering insights to improve community teaching practices rather than evaluating individual experiences. Future studies could enhance transparency in these interactions by considering third-party interviewers or anonymous feedback options to further support open dialogue.
Finally, the participant population in this study was entirely male, which may limit the ability to capture a diverse range of views. This limitation highlights the need for future research to include a more gender-balanced sample to ensure a broader and more representative range of perspectives.
Conclusion
We explored the qualities and abilities necessary for community physicians, the educational activities required during the early years of medical school to develop these qualities, and the factors influencing community preceptors’ involvement in teaching. Early years community-based teaching is driven by preceptors’ intrinsic motivations, such as their commitment to student growth, and supported by the broader community. However, preceptors faced challenges balancing clinical and teaching responsibilities and noted limited opportunities for students to engage in community-based learning.
To address these challenges, strengthening ties between universities and preceptors is essential. Faculty development programs and networking initiatives can foster collaboration and mutual support. Future research on CEME, such as cross-cultural studies drawing on social theoretical concepts such as those in Worley's four Rs model, could offer valuable insights into how CEME functions across systems. These studies would support inclusive, community-responsive medical education and sustainable partnerships between medical institutions and communities.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251317152 - Supplemental material for Community Preceptors’ Views on the Training Needs of Medical Students and Factors Affecting Medical Education in the Community Setting: An Exploratory Study
Supplemental material, sj-docx-1-mde-10.1177_23821205251317152 for Community Preceptors’ Views on the Training Needs of Medical Students and Factors Affecting Medical Education in the Community Setting: An Exploratory Study by Megumi Yasuda, Takuya Saiki, Chihiro Kawakami and Rintaro Imafuku in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to express our gratitude to Dr Yasuyuki Suzuki for his invaluable contributions to the research design and conceptualization of this study. We also thank Oliver Stanyon for translating and editing this paper, and Dr Maham Stanyon for their insightful feedback and suggestions, which greatly improved the manuscript.
Authors’ contributions
MY contributed to conceptualization, methodology, investigation, data analysis and interpretation, and writing the manuscript. TS contributed to methodology, data analysis and interpretation, review, and editing. CK contributed to data analysis and interpretation, review, and editing. RI contributed to conceptualization, methodology, data analysis and interpretation, review, editing, and supervision. All authors have read and approved the final manuscript. They also agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number: MO19K21726.
Author's note
Rintaro Imafuku is currently affiliated with the Nursing Research Promotion Center, Graduate School of Nursing, Nagoya City University, Aichi, Japan..
Ethical considerations
This study was conducted with the approval of the Ethics Review Committees of Gifu University School of Medicine (approval number: 2021-A216) and Fukushima Medical University (approval number: General 2021-330).
Consent to participate
Informed consent was obtained from all participants, and the ethics review committees approved this consent process. The process followed the policies and guidelines of the Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.