
Abstract
OBJECTIVES
While there has been increasing awareness of the importance of social determinants of health (SDOH) learning for internal medicine residents and physicians, only a few residency programs have incorporated training into their curricula. For those who did, the curricula were often didactic and lacked action-driven components or community partnership. Therefore, we built an experiential SDOH curriculum with an action-driven element and emphasis on community partnerships in a newly established residency program in rural New York.
METHODS
Over 24 months, 22 internal medicine residents were engaged in SDOH lectures, workshops, and action-driven learning through implementing screening tools in residency clinics and working with community partners. After the curriculum, residents’ competency in addressing SDOH needs was assessed through Likert-scale questionnaires. Focused interviews were conducted among participating residents and faculty to obtain qualitative feedback on the curriculum.
RESULTS
Participating resident physicians demonstrated competency in recognizing and addressing SDOH needs after curriculum completion (mean competency score = 4.04). A significant increase in residents’ self-rated confidence in addressing SDOH was observed after training (P = .002). Residents reported enhanced relationships with patients, effective utilization of community resources, and readiness to apply SDOH knowledge and skills to their future practice. Residents and faculty also discussed the SDOH challenges unique to rural primary care through their experiences.
CONCLUSION
This curriculum provides insights into an educational framework that improves residents’ SDOH awareness, integrates SDOH into resident physicians’ daily practice, and facilitates community collaboration. While challenges unique to rural primary care exist, this curriculum demonstrated the feasibility of longitudinal, action-driven, and community-centered SDOH education in rural areas that may inform future programs’ curricular design.
Introduction
The World Health Organization defines social determinants of health (SDOH) as “the conditions in which people are born, grow, work, live, and age and the wider set of forces and systems shaping the conditions of daily life”. 1 Influence from social circumstances has been shown to exceed healthcare factors in determining health outcomes such as early mortality, chronic disease prevalence, and overall life expectancy expectancies. 2 While SDOHs are critical drivers of health outcomes, the inability to adequately address them has exacerbated health inequities across populations. 3 Since 2021, the Association of American Medical Colleges (AAMC) has called upon the mission to incorporate community-oriented primary care and community-engaged health care with academic health centers to improve equity in the surrounding communities. 4 In response, medical training programs have started to incorporate SDOH education into their curricula.5–9
Existing SDOH curricula vary significantly in content, implementation, and evaluation methods. Three key challenges exist with existing SDOH training: 1) the lack of action-driven components, 2) the limitation of community resource referral and collaboration, and 3) the limitation of both healthcare and social resources in rural communities.
First, current SDOH curricula are mostly didactic in style with educators providing pamphlets or lecturing students on selective SDOH topics.6–10 For instance, Gard et al surveyed 43 SDOH curricula in the United States from 2007 to 2017, among which they found over 74% of the programs used a didactic teaching style and 47% occurred in a one-time session or less than six months time frame. 6 While traditional SDOH training had a positive outcome on students’ declarative knowledge of the meaning and implication of SDOH, it lacks procedural training for residents to take actions that alleviate those issues. For example, a recent systematic review of existing SDOH curricula by Nour et al, found that students preferred interactive, experiential learning teaching methods over traditional classroom teaching methods. 11 Similarly, the McMaster University Internal Medicine residency program implemented a social medicine elective rotation for residents to learn the SDOH needs of the community through programs such as an anti-racist practice and a transitional beds program for patients with housing needs. A key feedback from participants was that the addition of the experiential learning component enhanced the applicability of SDOH in future practices. 12 Therefore, the incorporation of action-driven components, when combined with traditional teaching, is crucial in enhancing learners’ SDOH knowledge and confidence to address SDOH in practice.6,11,13
Second, existing SDOH programs lacked integration with local resources and community partnerships to support SDOH need referrals. Residents are often aware of social domains that cause health risks for their patients but do not feel comfortable accessing resources for their patients with health disparities until they have formal training on health disparities and community resources. 14 In a study that surveyed family medicine residency program directors, they identified a lack of training in SDOH as a barrier to addressing them and believe there is a need for a longitudinal relationship between the community and the healthcare institution. 15
Nour et al surveyed eight programs and found that the ones that involved community engagement and resource referral provided the most meaningful experiences. 11 Additionally, Boutin-Foster et al 16 found that community advocates from organizations provided a link to underserved populations and revealed diverse perspectives that helped healthcare members tailor their care and strengthen their relationships with the community. 17 Therefore, developing an SDOH curriculum that is both action-driven and community-focused is of significant importance.
Third, addressing the SDOH needs of rural communities is particularly challenging compared to its urban counterpart. 17 One key challenge is the gap between the healthcare needs of rural communities and available resources. For example, one study evaluated the differences in attributes between rural and non-rural counties across the United States between 2015 and 2019 and found that rural counties had worse measures of SDOH at the county level and the disparity gap widened as the years progressed. 18 Given the substantial demand for primary care in rural areas in the United States and globally, addressing SDOH and teaching rurally located physicians to address SDOH are key goals for numerous primary care training programs. Furthermore, there is currently no known research on implementing an SDOH curriculum tailored to rural populations.
This study utilizes the experiential learning theory as the framework for developing the curriculum. David Kolb's experiential learning theory has four stages in the cycle: concrete experiences, reflective observation, abstract conceptualization, and active experimentation. 19 By manifesting these stages into the residents’ learnings, we hope to distill abstract concepts, such as addressing SDOH for patients, into actionable experiences.
This study aims to evaluate the feasibility of integrating action-driven components and community engagement into the residency SDOH curriculum that would promote effective and practical SDOH learning. We designed, implemented, and assessed a multi-dimensional curriculum, with an emphasis on experiential training, for training internal medicine residents on addressing SDOH in rural areas.
Methods and Materials
Participants
23 internal medicine residents who rotated in the resident-run primary care clinic from July 2020 to July 2022 were recruited. This resident-run primary care clinic is located in rural central New York, mainly serving patients who do not have regular primary care physicians in central New York. 22 residents (3 PGY3, 10 PGY2, and 9 PGY1) who worked in this clinic site were eventually enrolled in the study. The only inclusion criterion was active enrollment in the internal medicine residency program at Cayuga Medical Center; there were no prespecified exclusions for this study. The Institutional Review Board at Cayuga Medical Center at Ithaca (0924KD) approved it as an exempt study from ethical review, and the need for informed consent was waived.
Curricular development
There was no SDOH curriculum in this residency program before this study. The curriculum was developed by faculty and residents in a newly established internal medicine residency program in central New York to cultivate community-engaged primary care providers and future physician leaders. The curricular framework was based on the textbook A Framework for Educating Health Professionals to Address the Social Determinants of Health, which describes education, community, and organization as the three pillars for lifelong learning in understanding and addressing SDOH. 20 The curriculum is focused on experiential and collaborative learning through applied learning and community engagement. Multiple perspectives from resident feedback, faculty opinions, and input from community partners were also adopted in the development of the curriculum. The objective of the curriculum was to increase residents’ awareness of SDOH, empower residents to recognize and address unmet social needs that may affect patients’ health and increase residents’ confidence in addressing SDOH by utilizing community resources.
The 2-year longitudinal curriculum involved didactics, experiential training, and community resource navigation and referral (Figure 1).
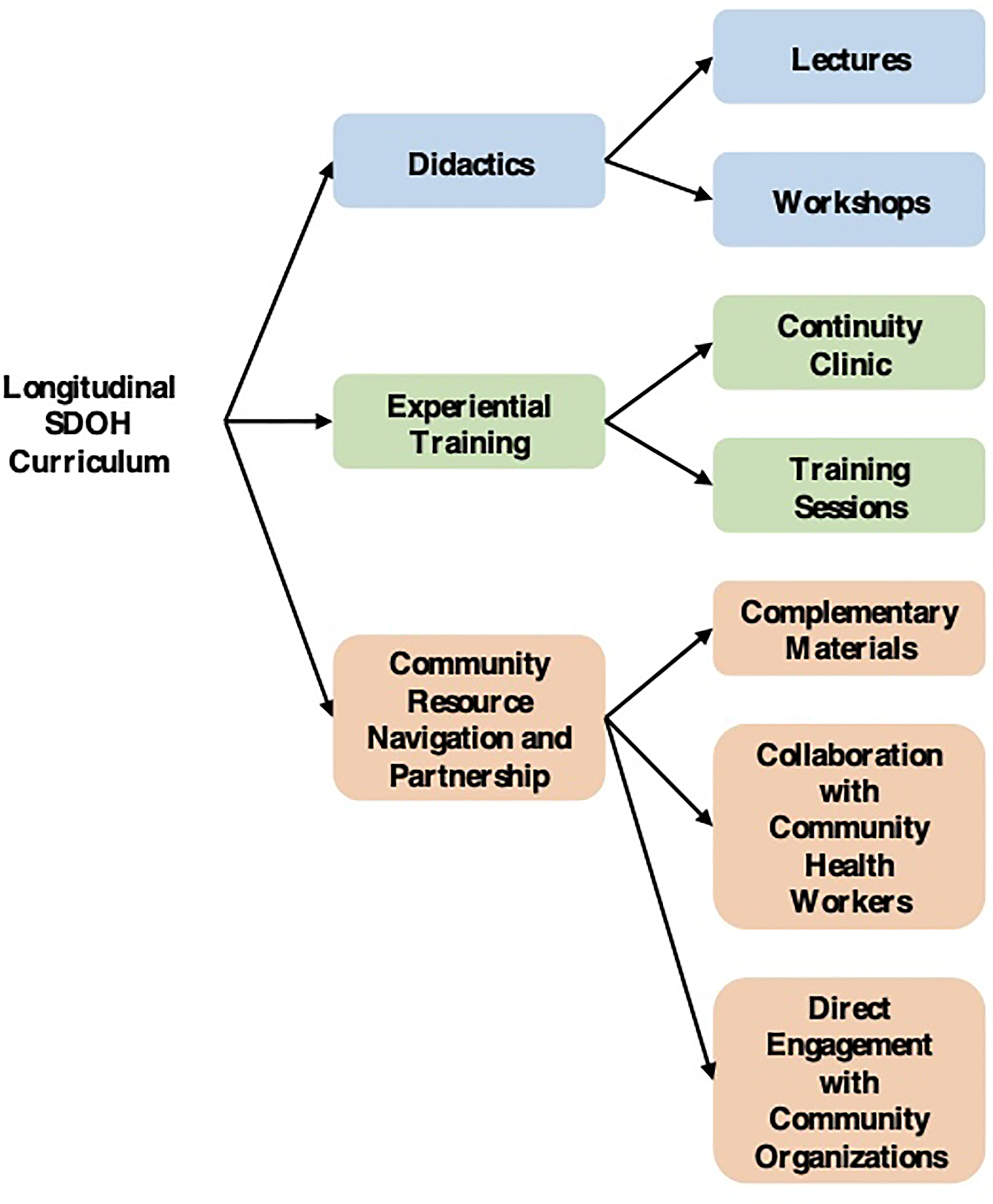
Curriculum overview. The longitudinal SDOH curriculum was specifically developed for the internal medicine residency program at Cayuga Medical Center in rural New York.
The didactic component included lecture series and workshops. A list of lecture and workshop topics can be found in Supplementary Table 1. Workshops consisted of 5-10 residents and involved discussions of real-life clinical cases and interactions with community partners, including community health workers and community-based organization leaders. Each instructor provided discussion questions and prompts for the residents and educational resources and readings. Workshop topics were selected to achieve the goal of helping residents develop an understanding of SDOH and fostering the formation of attitudes and knowledge to help them interact effectively with patients and the community.
For the experiential training, residents were placed in a resident-run primary care clinic. Resident physicians learned to use the SDOH screening tool as part of their patient intake process (Supplementary Figure 1). In two training sessions, residents were taught how to incorporate this tool into their daily workflow, identify SDOH, and work with onsite community health workers along with offsite community organizations to address specific SDOH needs.
Residents learned how to use three different strategies to support patients with community resource navigation. The first strategy was to offer complementary materials. These included a community resource brochure with 3-4 resources for each social needs domain and posters displayed in locations visible to all patients. These materials were created with the help of Cornell University's Master of Public Health Program and the Cornell Center for Health Equity Student Chapter to enhance patient and resident physician education. Examples can be found in Supplementary Figure 2 and Figure 3. The second strategy for community resource navigation was collaboration with onsite community health workers. Patients who identified one or more unmet social needs on the SDOH screening form and agreed to additional assistance were referred to onsite community health workers. Community health workers would work with the patients to better understand their unmet needs and connect them with the most appropriate community organizations to solve their specific SDOH concerns. The third strategy employed by residents was direct engagement with community organizations. For example, several residents referred patients with diet-related chronic diseases and food insecurity to a community organization that offered vouchers for free fruits and vegetables. Other residents gained expertise in community organizations that supported specific populations such as inmates and immigrant farmers.
Development of SDOH screening protocol
Building a comprehensive and effective SDOH screening tool and integrating it into the clinic workflow served as the foundation for the SDOH curricular development. As a newly established clinic and residency program, no SDOH screening protocol or community engagement protocol existed before the curriculum. The SDOH questionnaire from the Health Leads screening toolkit 21 was adapted and 8 domains of SDOH were selected based on the local county data, including food security, utility, housing, childcare, finances, transportation, literacy, and social support. The questionnaire was integrated into the electronic medical record system for easy access and documentation. All new and returning clinic patients were asked to complete SDOH screening questionnaires every six months, and resident physicians reviewed SDOH screening results during their encounters. When patients screened positive (ie, had at least one unmet social need), they were offered one of the 3 community resource navigation options described above.
Curriculum implementation and assessment
The new curriculum was implemented in July 2020. All primary care residents (3 PGY3, 10 PGY2, and 9 PGY1) participated in all educational activities outlined in the previous section. The training length ranged from a minimum of 12 months to a maximum of 24 months depending on the participant's PGY level. The reporting of this study conforms to the SQUIRE-EDU publication guidelines 22 (Supplementary File 2).
Currently, there is no validated way to measure medical trainees’ SDOH competencies. Existing post-curriculum evaluations were all developed based on team consensus.6,11,23,24 In this study, a self-assessed quantitative, non-validated questionnaire was developed by adapting items from similar SDOH curricula that assessed relevant physician competencies.11,25 The questions on the questionnaire assessed teamwork in addressing SDOH, community partnership, and resource utilization. Several faculty members reviewed the questionnaire to ensure face validity. The questionnaire contained two parts: 1) an Evaluation of residents’ confidence and competency in understanding and addressing SDOH in practice (Table 1), and 2) an Evaluation of the effectiveness of the SDOH curriculum in training residents to screen and address SDOH (Table 2). The assessment utilized a 5-point Likert scale, where 1 = Not Confident at all / Never / Strongly disagree and 5 = Very confident / Always / Strongly agree. Upon completion of the curriculum, 19 out of 22 resident participants completed the questionnaire. Faculty evaluation and feedback on SDOH competency were also integrated into the residents’ clinic rotation assessment. Due to the nature of continuous learning through feedback in medical training and different training levels among trainees, those data were not used for further analysis.
Retrospective assessment of residents’ competency in understanding and addressing SDOH.

Retrospective assessment of the effectiveness of the curriculum in training residents to screen and address SDOH in practice.

Focused interviews were conducted with resident participants and faculty voluntarily to understand individual experiences, gains of participation, and areas of improvement. Interviews were guided by questions reviewed by faculty members with an emphasis on open-ended feedback and discussion. Guiding interview questions and representative answers are listed in Table 3. A total of 2 residents and 2 faculty volunteers participated in the interviews.
Resident and faculty interview questions and sample answers.

Data analysis
A mixed-methods approach was used to combine quantitative data collected from surveys and qualitative data from interviews to explore the dynamics of participants’ experiences with SDOH. For quantitative data obtained from the questionnaires, descriptive statistics were calculated to summarize the responses to all survey items (Tables 1 and 2). A paired t-test was used to examine residents’ perceived confidence before and after training, both assessed retrospectively post-curriculum. P-values of .05 were considered significant for all statistical testing. Data were analyzed using SAS, version 9.4 (SAS Institute; Cary, NC). For qualitative data obtained from interviews, key points from interviewees were quoted in Table 3. No further analysis was done due to the small sample size.
Results
The results between July 2020 and July 2022 after the initial implementation of this new curriculum in a newly established internal medicine residency program were analyzed. Currently, this SDOH curriculum is still actively used in the residency program with more residents’ participation.
Participating resident physicians demonstrated overall competency in recognizing and addressing SDOH by self-survey and faculty evaluation. Residents were rated on average a 4.04 out of 5 among the main competencies assessed for this curriculum. Residents reported a significant increase in perceived confidence in addressing SDOH before and after the curriculum, which was both assessed retrospectively post-curriculum (before: M = 2.7, SD = 1.3; after: M = 3.8, SD = 0.9). Paired t-test indicated that there is a significant difference in residents’ confidence levels (P = .002). Residents demonstrated strong motivation to learn SDOH and commitment to future learning on SDOH. They were also noted to be able to recognize SDOH in practice quickly and consistently after receiving SDOH education, both through survey and faculty feedback.
The effectiveness of the SDOH curriculum in teaching residents how to screen and address SDOH was also assessed. Residents reported that SDOH activities helped them screen patients for social challenges that affect their health (average score 4.3) and better take care of patients (average score 3.9). The effectiveness of the SDOH questionnaire and tool utilization received average scores of 3.8 and 3.9, respectively. More effort needs to be placed in guiding residents on “how to work with an interdisciplinary team and local resources to address social determinants of health,” which received an average response of 3.7. The full results of the resident survey can be reviewed in Tables 1 and 2.
The results of resident surveys served as the foundation for in-depth discussion during 1-1 focused interviews. Qualitative data was collected from 2 residents and 2 faculty, who provided insights into their individual experiences with the SDOH curriculum. All 4 interviewees recognized the importance of SDOH training and integration into primary care practices. All reported that the curriculum was effective in helping residents recognize barriers to patients’ SDOH needs and develop essential skills to provide resources. Both residents reported that having direct patient interactions and being able to take actions to address SDOH were beneficial in their learning and development as physicians. 3 out of 4 interviewees reported frustrations stemming from not having resources readily available to help patients when SDOH domains were screened positive (Table 3).
Discussion
Disparities in health outcomes often arise from unequal access to SDOH resources such as housing, food, and transportation. Primary care clinics serving as sentinel stations for communities are ideal places to address health disparities related to SDOH. 17 Successful implementation of the SDOH curriculum in internal medicine residency may reduce early mortality, enhance patient-physician relationships, and improve community-wide health outcomes. 3 A mixed-method, longitudinal SDOH curriculum focused on incorporating SDOH knowledge into daily practice and community collaborations in a rural residency program was developed. This feasibility study demonstrates that a residency SDOH curriculum with an emphasis on action-driven learning and community partnerships yields promising results. To our knowledge, this is the first study of the SDOH curriculum for residency training that took place in a rural setting.
Following A Framework for Educating Health Professionals to Address the Social Determinants of Health, our SDOH curricular framework combines the traditional teaching style of faculty-led sessions and workshops with novel experiential components of applying the screening tool and partnering with community organizations. 20 The multidimensional format of our training allows the study to span the cognitive, affective, and psychomotor domains of learning described in Bloom's taxonomy, with complexity from the basic level of remembering knowledge to the metacognitive level of evaluation and creation.25,26 The immediate application of learnings from the workshops and curriculum to their daily routine in the clinic allows residents to remember, understand, and apply their skills. The reflections on their experiences afterward, whether that is through workshops or interviews, reinforce their knowledge and skill set. The format also applies Kolb's theory of experiential learning, with a focus on the steps of active experimentation and concrete experience through developing the learner's internal cognitive process. 27 These unique components enhance long-term educational outcomes and reinforce residents’ behavioral changes to address SDOH in practice. The ability for residents to apply their skills to patients with different health needs allows them to actively experiment with solutions that have worked in the past and newer ones that have potential, based on their experiences. Once they gain confidence in their skills, they can create their paths and build upon existing knowledge.
Collaboration and local adaptation are essential to ensure success in the implementation of SDOH in diverse communities. 28 Our curriculum focuses on collective effort by patients’ healthcare teams and community-based personnel. By bringing together physicians, community health workers, and community organizations in a highly coordinated manner, our educational module emphasizes the importance of team-based efforts with the local community and aims to equip residents with the skills to collaborate with various community partners. Our curriculum is designed to be easily adaptable to any primary care setting our resident physicians may encounter after graduation.
The combined results of quantitative surveys and interviews provided valuable insights into the educational benefits of our SDOH training. Before training, residents demonstrated strong motivation to learn SDOH but relatively low confidence in addressing SDOH, which provided intrinsic motivation for their participation. After the training, residents felt significantly more confident in their ability to recognize, identify, and take action to address SDOH in their everyday practices, as reflected by both the survey results and participant interviews. The increase in resident confidence and abilities will encourage future primary care physicians to establish routine behaviors surrounding SDOH. This training will contribute to the improvement of community health and holistic healthcare in our county. Current methods for incorporating SDOH, such as the elective rotation in the McMaster University Internal Medicine residency program, are optional for residents, which means that only residents who are highly motivated will join the two-to-four-week program. 4 Our curriculum is integrated with the residency program for all three years, which forces all the residents to gain and practice this skill set longitudinally. Furthermore, long-term integration of SDOH education helps establish routine behaviors and encourages changes on an institutional level, thereby providing positive reinforcement for optimal educational outcomes.
The findings echo the national and international trends of SDOH curricula for medical trainees, which help enhance students’ SDOH attitudes, knowledge, confidence, and competencies in recognizing and addressing patients’ social needs.4,6,11 The positive feedback on the experiential components of the training aligned with the result by Nour et al that action-driven learning and community engagement experiences were the highest-rated modalities of SDOH curricula. 11 In addition, our approach for curriculum evaluation using focused interviews enriches existing literature. Currently, knowledge quizzes and self-reported surveys are the two most used evaluation tools for the SDOH curriculum. 6 Few studies used videotaped clinical encounters or focus group interviews. 6 The interviews gave more insights into a new curriculum and allowed for constructive feedback without being constrained by the grading system.
While the results of this study indicated an overall success of the curriculum in an internal medicine residency program, challenges specific to rural primary care were reflected during our curricular implementation. Dauner et al discussed barriers to addressing SDOH in rural communities, which included a lack of systematic screening process across various healthcare players, a lack of follow-up system for referrals made to community organizations, and documentation inconsistency. 29 Although our study achieved a streamlined workflow across different healthcare players, electronic integration to enhance documentation, other barriers that are common in rural healthcare, such as a perceived lack of social resources, staffing shortage, and inadequate follow-up for referrals made to community organizations, were experienced by our residents.17,29 Advocacy for policy changes, therefore, is crucial in achieving long-term success in SDOH screening and referral, in which resources and staff are readily available to navigate patients’ SDOH needs. 29 These policy changes in the public health system can lead to a significant improvement in the health status of the rural populations, as indicated in Huang & et al's study. 30
One limitation of this study includes the size of our study; this curriculum was in a newly established residency with only 22 residents participating. With that said, this curriculum was designed for small community-based primary care programs, which typically have only 15-30 learners. Though most of the residents were able to fill out the survey, we were only able to gather qualitative data from 4 individuals due to time constraints and scheduling. In the future, we would want to interview and gather data from more if not all the residents involved in the curriculum. Secondly, there is no standardized test to evaluate learning outcomes for the SDOH curriculum. Our outcome assessment was largely based on self-assessments, which may be subject to reporting bias. Thirdly, the tool developed focused on the main SDOH challenges tailored to our local community. We decreased the number of SDOH domains to make screening easier to administer and less time-consuming. Some important SDOH topics may be overlooked, such as employment and educational attainment, and the residents wouldn’t be able to actively practice addressing those needs. Moving forward, we want to incorporate most if not all the knowledge topics and behavioral learning goals that were identified in the Delphi Study so that we can adequately train the residents in addressing SDOH knowledge that is relevant to primary care specialties. 31 Fourthly, there was a lack of clinical data on the usage of the screening tool and its effectiveness in addressing the health concerns patients faced. Because the tool was recently implemented, it required a training period for the healthcare professionals. There were also updates and changes to the wayflow of how the tool was incorporated so there was no standardized way to collect clinic data. In the future, a retrospective chart review should be conducted to determine whether the tool and training were effective in improving health outcomes in the community.
Conclusion
In summary, we successfully established a longitudinal, community-centered, and action-driven SDOH curriculum by using Kolb's theory in a newly established internal medicine residency program in a resource-limited area. Future residency programs can adapt our SDOH training model to meet the specific needs of their communities. We continued to implement our curriculum in our residency program while actively improving it based on current results and feedback. We have also expanded SDOH screening and training to other primary care offices nearby. Currently, at least 3 primary care offices in our network have adopted our SDOH screening and training model with success. Future studies may aim to assess the extended implementation of our curriculum and develop validated assessments to examine its impact on residents’ learning. Integration of community health workers after the screening process remains challenging due to low human resources. The future direction for this SDOH curriculum is to include advocacy training for residents to help facilitate institutional changes that address challenges faced by rural primary care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241312756 - Supplemental material for Learning by Doing, and Doing it Right – Building a Multi-Dimensional Social Determinants of Health Curriculum in a Rural Internal Medicine Residency
Supplemental material, sj-docx-1-mde-10.1177_23821205241312756 for Learning by Doing, and Doing it Right – Building a Multi-Dimensional Social Determinants of Health Curriculum in a Rural Internal Medicine Residency by Sophia Zhang, Yibei Zhu, Lara Parrilla and Kaili Du in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241312756 - Supplemental material for Learning by Doing, and Doing it Right – Building a Multi-Dimensional Social Determinants of Health Curriculum in a Rural Internal Medicine Residency
Supplemental material, sj-docx-2-mde-10.1177_23821205241312756 for Learning by Doing, and Doing it Right – Building a Multi-Dimensional Social Determinants of Health Curriculum in a Rural Internal Medicine Residency by Sophia Zhang, Yibei Zhu, Lara Parrilla and Kaili Du in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors would like to thank all the residents who took the time to participate in the study, answer questions in the interview, and fill out the questionnaires.
Author's Contributions
KD designed the experimental studies, contributed to the longitudinal study design, data collection, analysis, manuscript preparation, and revisions. YZ and SZ performed the literature review, analyzed the data, and prepared the primary manuscript and revisions. LP oversaw the longitudinal study design, conducted literature review, and manuscript revisions. All authors read and approved the final manuscript.
Author's Note
This work was presented on 5/17/2024 at the Society of General Internal Medicine annual meeting in Boston, MA as the Hamolsky Award Finalist.
FUNDING
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the David M. Einhorn Center for Community Engagement (grant number: EOG 20.071); the Rural Health Equity Training Collaborative (grant number: T0BHP33100).
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The Institutional Review Board at Cayuga Medical Center at Ithaca (0924KD) approved it as an exempt study from ethical review, and the need for informed consent was waived.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.