
Abstract
Background:
In an obesity epidemic, physicians are unprepared to treat patients with obesity. The objective of this study was to understand how obesity is currently addressed in United States (U.S.) Internal Medicine (IM) residency programs and benchmark the degree to which curricula incorporate topics pertaining to the recently developed Obesity Medicine Education Collaborative (OMEC) competencies.
Methods:
Invitations to complete an online survey were sent via postal mail to U.S IM residency programs in 2018. Descriptive analyzes were performed.
Results:
Directors/associate directors from 81 IM residencies completed the online survey out of 501 programs (16.2%). Although obesity was an intentional educational objective for most programs (66.7%), only 2.5% of respondents believed their residents are “very prepared” to manage obesity. Formal rotation opportunities in obesity are limited, and at best, only one-third (34.6%) of programs reported any one of the core obesity competencies are covered to “a great extent.” Many programs reported psychosocial components of obesity (40.7%), weight stigma (44.4%), etiological aspects of obesity (64.2%) and pharmacological treatment of obesity (43.2%) were covered to “very little extent” or “not at all.” Lack of room in the curriculum and lack of faculty expertise are the greatest barriers to integrating obesity education; only 39.5% of residency programs have discussed incorporating or expanding formal obesity education.
Conclusions:
Our study found the current obesity curricula within U.S. IM residency programs do not adequately cover important aspects that address the growing obesity epidemic, suggesting that obesity education is not enough of a priority for IM residency programs to formalize and implement within their curricula.
Background
Obesity is the number 1 public health crisis in the United States (U.S.); it currently affects more than one-third of adults, and prevalence is increasing faster than estimated.1,2 It either causes, exacerbates, or accelerates a myriad of complex chronic diseases that internists often diagnose and treat, including type 2 diabetes, hyperlipidemia, and hypertension, as well as contributes to increased risk of cancer and mortality.3,4 Internists are particularly well-suited to care for patients with obesity given the high prevalence of the disease and their role as adult primary care providers. In addition, internal medicine (IM) forms the foundation for medical subspecialties such as gastroenterology, cardiology and endocrinology that treat many of the weight-related complications such as fatty liver disease, atherosclerotic heart disease, and type 2 diabetes.
Despite recognition by the American College of Physicians of the importance of addressing obesity and its impact on public health, 5 obesity is not being managed effectively in the primary care setting.6-11 Studies have shown IM residents fail to recognize obesity, lack knowledge and comfort with assessment and management of obesity, and spend little time in clinic treating obesity.12-17
To help address the challenges of incorporating a consistent approach to obesity education in undergraduate education and graduate medical education, the Obesity Medicine Education Collaborative (OMEC), a partnership between the Obesity Medicine Association (OMA), The Obesity Society (TOS), and the American Society of Metabolic and Bariatric Surgery (ASMBS), has created obesity-related competencies and associated benchmarks based on the Six Core Competency domains of the Accreditation Council for Graduate Medical Education (ACGME). 18 Endorsed by 17 organizations, including the Society of General Internal Medicine (SGIM), the competencies focus on key components in obesity care. 18 Many of these topics are particularly pertinent to internists, such as use of patient-centered communication when working with patients with obesity, strategies to minimize bias against patients with obesity, evidence-based obesity treatments, and understanding the benefits of working with an interprofessional health team. 19
To our knowledge, there is currently no literature systematically examining the state of obesity education within internal medicine residency programs. The aim of this study is to understand how topics regarding obesity are addressed in U.S. IM residency programs and provide a benchmark by which progress can be assessed. Specific goals were to understand inconsistencies between the OMEC provider competencies and current internal medicine curricula and barriers to implementing core competencies in obesity.
Methods
Between August and September 2018, program directors from 501 IM residency programs, identified through the ACGME public directory, 20 were invited to voluntarily participate in this cross-sectional, anonymous study. Institutional qualification was limited to categorical or preliminary/categorical combination (preliminary programs offer 1 to 2 years of training prior to advanced specialty programs; categorical programs offer full training required for board certification) IM residency programs in the U.S., excluding Puerto Rico, with responses restricted to 1 representative per program to ensure consistent data and representation across institutions. Further web searches identified a total of 1112 directors, associate directors, and assistant directors of these residency programs. Potential respondents received a postal mailing with a letter identifying the study sponsor (Novo Nordisk) and key collaborator (Dr. W. Scott Butsch), study objectives, participation requirements, along with a modest prepaid incentive of $65 in the form of a check. A second mailed invitation with the prepaid incentive, along with follow-up faxes and emails were sent to remind non-responders to participate. Inclusion criteria required respondents to confirm their role in graduate medical education and knowledge of their program’s overall learning objectives. Ethical approval was waived (exempted) by Western Institutional Review Board, 30 July 2018, reference number 1-1098135-1. Prior to completing surveys, respondents provided informed consent electronically.
The online survey was comprised of 33 questions addressing the structure, format, content, and setting of obesity education and included multiple choice, scalar, and numeric text questions. Using a 4-point Likert scale (“great extent,” “some extent,” “very little extent,” and “not at all”) respondents were asked to assess the degree to which their curricula addresses core competencies; topics of obesity education were chosen before the finalization of the OMEC obesity competencies but were closely aligned. Respondents were also asked about how obesity is taught in their program, their expectations regarding future incorporation of obesity in the curriculum, and barriers to doing so. See
We performed descriptive statistical analysis (means, frequencies) using SPSS Statistics for Windows 23 (SPSS, Chicago, Illinois). Data are presented as number and percentage for categorical variables, and continuous data expressed as the mean ± standard deviation (SD) unless otherwise specified.
Results
Characteristics of respondents
Eighty-one IM residency programs out of a potential 501 programs (response rate of 16.2% of invited programs) responded and completed the survey. Median length of time to complete survey was 8 minutes. These programs were a geographically representative group of medical school-based, medical school-affiliated, and community-based hospital internal medicine residency programs. Approximately half of the participating IM residency programs were categorical, and the remaining programs were combination categorical and preliminary programs. Nearly all respondents were either program directors or associate/co-program directors; average time in their current role was 6 years. Almost all (98.8%) were very or extremely familiar with the overall learning objectives of the 3-year internal medicine residency program; all contribute to the decisions regarding the curriculum at their institution and teach/train residents. See Table 1 for sample characteristics.
Characteristics of 2018 Internal Medicine Residency Online Survey Respondents and their Institutions (n = 81).

Abbreviations: SD; standard deviation.
Percentages may not sum to 100% due to rounding.
Reference characteristics of regional and affiliation ACGME programs, American Medical Association’s FREIDA database. 21
When asked about their own preparedness in managing obesity, more than two-thirds (70.4%) of program directors felt “very prepared” making a diagnosis of obesity. However, only about one-third felt “very prepared” giving physical activity advice (37.0%) and nutritional advice (29.6%) to patients with obesity. Very few respondents (11.1%) felt “very prepared” prescribing pharmacotherapy for obesity, while one-quarter (25.9%) felt “not at all prepared.”
Perceived need for education
Despite obesity being an intentional educational objective for two-thirds (66.7%) of the programs surveyed, a majority (63.0%) of respondents reported that their residents are at most “somewhat prepared” to treat patients with obesity, and only 2.5% of reported their residents as “very prepared.” When rating the importance of education on various weight-related topics, respondents chose discussing the relationship between weight and comorbidities (88.9%), bringing up the topic of weight (82.7%) and discussing weight and well-being (77.8%) as “very important.” More than two-thirds (69.1%) rated patient-centered treatment of weight and goal setting “very important”; other topics were reported as “very important” by fewer respondents, such as comfort with referrals for weight loss surgery (51.9%) and pharmacotherapy (35.8%) (Figure 1).
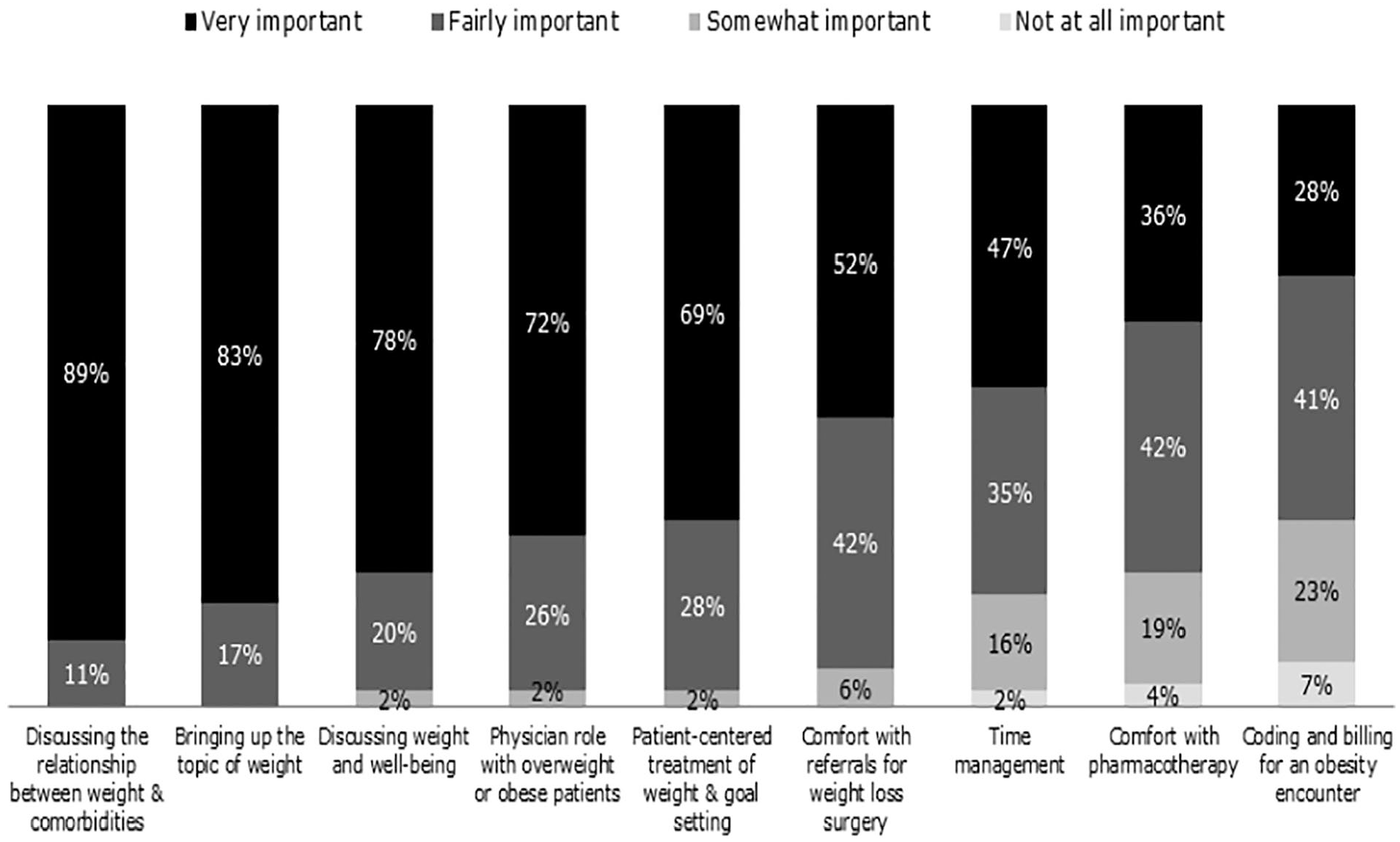
Started importance of education on weight- related topics 2018 internal medicine residency curriculum online survey respondents (n = 81).
Obesity in the curriculum
An average of 3.4 hours of textbook education specifically on obesity was reported among IM programs, with MKSAP used by most programs (95%); however, 20% of programs reported zero hours of obesity textbook education. Hands-on education focused on obesity was more common, with an average of 12.2 hours across the residency. Among the topics related to obesity included in the survey, only physical activity and nutrition interventions were covered to a “great extent” by more than a quarter of the programs. Less than one-tenth of programs covered weight stigma and discrimination (8.6%), physiology of obesity (8.6%), etiologic aspects of obesity (8.6%), and pharmacologic treatment of obesity (6.2%) well, making them the least covered obesity competencies (Figure 2).

Extent to which obesity competencies are addressed 2018 internal medicine residency curriculum online survey respondents (n = 81).
Obesity was almost as likely to be covered in dedicated seminars (66.7%) as during teaching rounds and informal teachings (both 75.9%). However, the most commonly addressed topic in a dedicated seminar was bariatric surgery, while physical examination skills specific to patients with obesity (eg, waist circumference, acanthosis nigricans) and weight stigma and discrimination were the least likely to be covered in this form. Almost two-thirds (64.2%) of programs offer the opportunity to work with non-medical providers such as dietitians and psychologists who care for patients with obesity. Far fewer programs offer formal bariatric surgical (17.3%) or non-surgical (eg, weight management clinics, 25.9%) clinical rotation opportunities in obesity.
Priority to incorporate obesity education in curriculum
Expanding obesity education was a low priority in 41% of surveyed residency programs with more than 50% respondents reporting there were no discussions to incorporate or expand obesity education in their programs. Only 9.9% of program directors and co-directors noted expansion of obesity education was a high priority for their program. Of the 39.5% of programs that have discussed incorporating or expanding formal obesity education, 43.8% planned to do so within a year, and almost all (9.8%) planned to do so within 2 years. Lack of room in the curriculum and lack of faculty expertise are reported to be the greatest barriers to integrating obesity education into the curriculum (Figure 3).

Barriers to integrating obesity education into curriculum 2018 internal medicine residency curriculum online survey respondents (n = 81).
Discussion
We believe this is the first study to comprehensively assess the state of obesity education in internal medicine residency programs in the U.S. This Internal Medicine Curriculum Benchmark Study survey revealed an inconsistent and inadequate approach in training future internists in the leading health epidemic in the U.S. In addition to poor coverage of core competencies in obesity, the results of this study highlight the under-prioritization to develop future residency curricula in obesity. This underscores the lack of progress over the past ten years despite recognition of a need for better and more comprehensive education and training in obesity management among medical school students, internal medicine residents, and internists.15,16,22-25
Although residency programs have a responsibility to train residents to practically apply their knowledge to patient care, 18 IM residents, according to IM program directors, are still not adequately prepared to treat obesity and, like many primary care practitioners, lack knowledge of evidence-based obesity treatment guidelines. 26 The majority of program directors state obesity is an intentional learning objective, yet few programs are covering relevant obesity competencies to a great extent, and some programs omit them entirely from the residency curriculum. Some studies suggest that a lack of knowledge and comfort providing guidance on behavior modification and a healthy lifestyle may play a role in limiting counseling on lifestyle interventions for patients with obesity. There remains a consistent disconnect despite the recognition for obesity education, leaving internists inadequately equipped with the skills needed to diagnose and treat obesity. Lifestyle interventions remain the foundation of effective, evidence-based treatment of obesity; 27 however, primary care physicians, including internists, are not providing weight-related counseling for patients with obesity or systematically tracking intervention behaviors.28,29
Unfortunately, but not surprising, very few (less than 10%) internal residency program directors reported that expanding obesity in the curriculum was a “high priority,” noting a lack of room in the curriculum and lack of or limited faculty expertise as the greatest barriers (the former is likely a proxy for lack of prioritization). In fact, IM residency programs are prioritizing education on the associated comorbidities for patients with obesity, rather than obesity itself. Expertise in treating these comorbidities is important, but it is also critical to have a deeper understanding of obesity as a disease. A larger concern is the lack of faculty expertise and personal preparedness of program directors and associate directors to provide obesity care, which can perpetuate the cycle of low levels of obesity knowledge and inadequately skilled physicians in treating obesity at all levels of training. This highlights the need for a more consistent approach in internal medicine residency programs with guidance to maximize both the impact of current obesity-related content and expansion of content of particular importance for internists and that are not currently well-addressed.
Internal medicine residency programs seeking to develop a more consistent approach to obesity education should first consider aligning the OMEC competencies to existing or planned residency curricula as well as the assessment of learners within a training program. However, several IM residency programs have already introduced their own unique programs or modules incorporating obesity training into an already crowded curriculum.30-32 Rather than addressing the challenges of recruiting faculty with expertise in obesity medicine, programs should utilize the strengths and expertise of individual faculty members including multidisciplinary members of the obesity care team such as registered dietitian nutritionists, health psychologists and clinical pharmacists, who may be suited to assess specific competencies. To improve obesity education within existing structures, faculty development programs to improve faculty’s clinical skills and resident teaching about obesity management can be implemented. Lastly, identifying external resources, such as shared curricula from institutions already excelling in obesity education or existing online CME courses and training modules in obesity can be incorporated to provide comprehensive training in obesity.
Limitations
This study has several limitations worth noting. Foremost, this research is limited by the relatively small sample size, a response rate of approximately 16%, and the extent to which these 81 programs represent the broader population of categorical IM residency programs in the U.S. Although the sample is fairly representative at the regional level, there is under-representation in 2 key states; only 4 of the 40 invited programs located in California and one of the 26 programs located in Texas participated. Characteristics specific to individual institutions may also be less representative. Larger programs/programs affiliated with larger institutions had a greater opportunity for participation; they are more likely to have multiple faculty members eligible to participate or more easily accessible contact information. In addition to the geographic distribution, the sample is also representative of the types of institutions with which programs are affiliated. Thus, we believe the study sample represents the overall population of IM residency programs in the U.S.
Additionally, it is possible that non-responder bias could have resulted in a favorable evaluation of obesity education in IM residency programs. Given the reported low priority of obesity education, it is unlikely that this in the case. It may also be that participants’ personal interest in obesity and obesity education played a role in the decision to participate. Programs led by internists who feel strongly about obesity education have an increased likelihood of participation and may be over-represented, while programs whose leadership prioritizes other areas of education may choose not to participate. In this case, the results would be understated.
Overall, we believe that participants were candid when describing their obesity curriculum and that results are generalizable. Responder bias here would likely result in “better” programs, or at least fewer poorly performing ones, from responding, but our data show significant room for improvement.
Conclusion
Internal medicine residents are not prepared to combat the obesity epidemic in the United States, and internal medicine residency programs are not prioritizing training in obesity. Training in nutrition, behavioral, and pharmacological treatments of obesity as well as awareness of weight stigma represent key areas of opportunity. Internal medicine residency programs should use the existing core competencies in obesity to assess and guide didactic and clinical practice education in obesity. Resident training in obesity management should be prioritized and may be more easily introduced in the context of cardiometabolic disease. If residency program directors prioritize obesity education and take advantage of resources provided by organizations such as OMEC, internists will be more competent and confident to address this major public health concern in primary care settings across the U.S.
Supplemental Material
sj-pdf-1-mde-10.1177_2382120520973206 – Supplemental material for Medicine Residents are Unprepared to Effectively Treat Patients with Obesity: Results from a U.S. Internal Medicine Residency Survey
Supplemental material, sj-pdf-1-mde-10.1177_2382120520973206 for Medicine Residents are Unprepared to Effectively Treat Patients with Obesity: Results from a U.S. Internal Medicine Residency Survey by W Scott Butsch, Kathryn Robison, Ranita Sharma, Julianne Knecht and B. Gabriel Smolarz in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank Lauren-Spirko Burns, Assistant Professor of Instruction, Statistical Science and Pallavi Chitturi, Research Professor and Director at the Center for Statistical Analysis, Fox School of Business, Temple University for their analytical support. Additionally, the authors would also like to thank Rebecca Hahn of KJT Group, Inc. for medical writing assistance and support (funding provided by Novo Nordisk).
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Novo Nordisk Inc. financed the development of the study design, third-party blinded data collection, analysis, and interpretation of data as well as writing support of the manuscript. Both Dr. Smolarz and Dr. Knecht, employees of Novo Nordisk, co-designed the study, interpreted the data and generated reported conclusions.
Declaration of conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Butsch is a health consultant for Novo Nordisk Inc. and on an advisory board for Rhythm Pharmaceuticals, Inc.; Dr. R. Sharma has no conflicts of interest to disclose; Dr. K. Robison has no conflicts of interest to disclose; Dr. Knecht is an employee of Novo Nordisk and owns stock in Novo Nordisk.; Dr. Smolarz is an employee of Novo Nordisk and owns stock in Novo Nordisk.
Author contributions
WSB, JK, BGS designed the study and developed the study materials. All authors provided input into the data analyses, contributed to writing the manuscript, and read and approved the final manuscript.
Ethics approval and consent to participate
Ethical approval has been waived (exempted) by Western Institutional Review Board, July 30, 2018, reference number 1-1098135-1. Prior to completing surveys, respondents provided informed consent electronically.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.