
Abstract
Introduction
The cost, high resource demands, and psychological significance of in-person cadaveric labs are barriers to their use. Computer-assisted instruction (CAI) of gross anatomy is widely available as an alternative option. However, student engagement, reflections, and expectations of learning anatomy with CAI instead of in-person labs may influence their learning experience and outcomes.
Purpose
To evaluate students’ critical self-reflection and perceptions of learning using online self-guided anatomy modules with video-based pro-section CAI.
Methods
A prospective observational cross-sectional study was conducted with first-year occupational therapy students who received anatomy education using CAI involving online self-guided anatomy modules with video-based pro-section instruction. Critical self-reflection was measured using Kember's Critical Self-Reflection Questionnaire scores and open-ended comments. Paired analysis of self-reported Kember nonreflective and reflective actions was conducted followed by quantitative (correlation, Student t-tests) and qualitative (directed content analysis) exploration of factors associated with critical self-reflection.
Results
Of the 126 students enrolled in the study, 97 consented and completed the study. The students’ Kember Understanding (U) subscale mean score was significantly higher than the Habitual Action (HA), Reflection, and Critical Self-Reflection subscales. The largest effect size was found between the U and HA subscales (ds = 1.3, 95% CI [1.0, 1.5]). Academic outcomes (anatomy quiz sum score, term grade) did not correlate with the Kember scores. Overall, students felt that video-based anatomy pro-section CAI was best used in a supplementary manner and opportunities for hands-on learning of anatomy were needed.
Conclusion
Video-based anatomy pro-section CAI helped students understand anatomy but did not readily engage students in critical self-reflection. Strategic course and curriculum design with integrated and hands-on learning opportunities are needed to optimize student anatomy learning experience and academic outcomes while using this type of CAI.
Introduction
Computer-assisted instruction (CAI) such as videos and three-dimensional (3D) applications (apps) have been shown to be effective in improving student anatomy knowledge and academic outcomes.1–4 In addition to self-paced learning, the visual capabilities of CAI are a major strength of this pedagogical approach.5,6 This is important as students learn best using methods that foster 3D visualization of anatomical structures.3,7,8 Furthermore, digital applications may be used to teach with cadaveric images or 3D models. Online education videos of dissection and 3D models of pro-section specimens are widely available through institutional and public domains. An example of such resources is Acland's Video Atlas of Human Anatomy. 9 This is an online video series of anatomy lessons taught by a clinical anatomist, Dr Robert Acland, using a 360-degree view of anatomical pro-sections. As the cost, high resource demands, and psychological concerns of in-person cadaveric labs are barriers to their use, CAI such as Acland's Video Atlas is a desired alternative for many anatomy instructors. Furthermore, the COVID-19 pandemic caused a necessary shift to online pedagogies which has led to ongoing expectations of online education options from all stakeholders (e.g., administrators, students).
However, the literature indicates that CAI is less impactful on student gains in anatomy knowledge when used in replace of traditional methods. Specifically, Wilson et al conducted a meta-analysis to synthesize the effects of CAI on student performance in anatomy. In this comparison of 2570 students who engaged in CAI with 1362 students who received traditional teacher-centred instruction, CAI used to supplement existing teaching approaches were most effective. 10 The authors bring to question whether the overall positive effect of CAI is simply a byproduct of having access to additional resources when digital technologies are offered. As such, a blended learning approach that combines CAI with traditional methods is recommended. However, if academic outcomes of CAI are always evaluated in this context, insights on how to optimize student experiences with these technologies may not be fully understood.
Wilson et al's review may also indicate that CAI as a standalone method is inferior because it lacks hands-on learning opportunities compared to the tactile and kinesthetic learning offered through in-person methods. Some CAI platforms may include features that encourage students to actively participate (e.g., apps, virtual reality), while others may be more passive (e.g., videos). The degree of user interaction during CAI influences student experience and learning. 11 Therefore, CAI of cadaveric instruction that does not encourage user participation such as Acland's Video Atlas, may not foster the same learning outcomes as a highly interactive CAI.
Another consideration of Wilson et al's findings is that user preference and technological literacy may influence student's CAI experience. McNutty et al evaluated the use of CAI to teach gross anatomy over a 6-year period and found significant variability in students’ use of different types of CAI. A relationship between the type of CAI and the students’ learning style, personality traits, and gender (i.e., females had higher use on some applications) was observed. 12 In addition, student expectations regarding learning anatomy with cadaveric specimens via CAI should be explored as in-person laboratory approaches have been the longstanding “gold standard” of anatomy education. Students who perceive traditional cadaveric methods as the favoured approach for anatomy education may have preconceived notions about the effectiveness of CAI. This may negatively influence their engagement with cadaveric-based CAI. Furthermore, there is evidence that students have greater interest, self-perceived learning, and satisfaction with traditional anatomy labs compared with cadaveric-based CAI. 13
Student preferences and expectations may influence their use of digital technologies and subsequent learning outcomes. At present, we have an understanding of the type of 3D digital technologies and content students prefer (e.g., model explanations, surface anatomy),14,15 but there is a gap in our knowledge of the learning processes that occur while students engage with video-based CAI. Seeking their reflections on how they learn while using CAI is important. Student critical self-reflection is essential to the education of health professionals. 16 This type of reflection considers the meta-cognitive process of understanding the self, situation, and environment to inform future interactions and processes.17,18 In this way, critical self-reflection considers the connection students make between their present learning experience and its value and application to the larger curriculum context and future clinical practice. As such, an evaluation of critical self-reflection must come from the students themselves.
In summary, the supplementary use of anatomy CAI is recommended. However, increased barriers to in-person cadaveric labs create the need to use CAI in place of these traditional methods. Other classroom pedagogies such as lectures and clinical skills labs may be used to supplement cadaveric-based CAI, but student engagement, reflections, and expectations may influence their learning experiences and outcomes. Yet, an evaluation of students’ critical self-reflection while using cadaveric-based CAI has not been conducted. Understanding how these digital technologies are perceived and used by students to support their learning when in-person cadaveric labs are not offered is important. Therefore, the purpose of this study was to evaluate students’ critical self-reflection and perceptions of learning using cadaveric-based CAI.
Methods
An observational cross-sectional study was conducted to evaluate student critical self-reflection while being taught gross anatomy with cadaveric-based CAI. CAI was used to supplement traditional anatomy lectures and clinical skills labs. The primary objective of this study was to determine if student occupational therapists (OTs) engage in more critical self-reflective actions than nonreflective actions while using cadaveric-based CAI. The secondary objective was to determine the factors that relate to students’ critical self-reflection and perceptions of using video-based pro-section CAI to learn anatomy. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement was followed to report this research. 19
All students enrolled in the musculoskeletal foundations for occupational therapy practice course in the first year of the 2021–22 Master of Science in Occupational Therapy (MScOT) program at the University of Toronto were eligible for inclusion in the study. Students who completed an undergraduate or graduate degree in anatomy were concurrently enrolled in any postsecondary anatomy or kinesiology course, or those who withdrew from the MScOT program prior to December 31, 2021, were excluded. Consenting students completed a critical self-reflection questionnaire and released their de-identified course assessments for analysis.
This study was conducted in the first of the course which ran from September to December and focused on gross anatomy and foundational musculoskeletal clinical skills. In 2021, the restrictions posed by the COVID-19 pandemic did not allow in-person teaching with cadaveric labs that were previously offered in the course. Instead, cadaveric-based methods were taught using CAI via online self-guided anatomy modules and student-led graded discussion forums. The online self-guided modules were designed around the weekly lecture topics and used Acland's Video Atlas of Human Anatomy pro-section instruction, as a main teaching tool. 9 Each module included gross anatomy information through text, diagrams, and video links to the relevant structures in the online atlas. Each module also included applied anatomy in the format of occupational therapy case-based scenarios and practice knowledge information. As video-based digital technology (i.e., Acland's Video Atlas) was chosen as the primary CAI, student-led graded online discussion forums were added to foster active learning. Approval for this study was obtained from the University of Toronto Research Ethics Board (Approval number: 41315) and informed consent was received from the students who participated in this study.
The primary outcome of this study was critical self-reflection. The Kember's Critical Self-Reflection Questionnaire (Kember) is a tool designed to measure critical self-reflection 17 (Appendix). This tool that has been validated and psychometrically tested on a cohort of health sciences faculty students, including occupational therapy.17,18 Theoretically, this questionnaire is grounded in Mezirow's transformative learning theory which distinguishes students’ reflective from nonreflective action during learning. It is organized into reflective from nonreflective action and has four scales: Habitual Action (HA), Understanding (U), Reflection (R), and Critical Reflection (CR). 17 The HA and U scales are nonreflective, while R and CR scales are reflective. The Kember was used to evaluate students’ critical self-reflection while learning using Acland's Video Atlas of Human Anatomy within the online modules. 9 Students’ perceptions of this CAI were elicited through an opportunity to provide comments (i.e., free text) at the end of the Kember questionnaire. The Kember questionnaire was administered to students at the end of Term 1.
Variables collected to explore factors associated with student critical self-reflection included course assessment grades and previous anatomy coursework. Term 1 course assessments included seven formative online anatomy quizzes (7%) which corresponded with the topics covered in the lectures and online self-guided anatomy modules, an anatomy reflection assignment (8%), two clinical skills labs assignments (10%), and a culminating practical exam (15%). Gross anatomy academic outcomes were defined as the sum score of the student's performance on the seven anatomy quizzes. Overall academic outcome was defined by the students’ composite grade on all Term 1 assessment items which was a total of 40% of the overall course grade. Students’ previous anatomy coursework was determined through self-report and was cross-referenced with the documented entry degree at the time of their application to the program.
Statistical analysis
The quantitative data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) statistical analysis software v.29. 20 After the normality of the data was evaluated and established, the students’ responses on the Kember were analyzed parametrically. Paired samples t-tests were conducted to evaluate within student differences on Kember's nonreflective and reflective items. Exploration of factors associated with critical self-reflection was conducted using student t-tests to compare Kember subscale scores between students with and without previous anatomy coursework. Pearson's correlations were used to describe the relationship between the Kember and student academic outcomes (anatomy quiz sum score, Term 1 grade). Following, directed content analysis was used to analyze students’ free text comments by the first author [EH] and verified by a second researcher [ED]. 21 Our reporting of these data followed a data saturation approach that was consistent with our descriptive purpose in analyzing these text-based responses. 22 The key purpose in reviewing these comments was to determine whether the students were in favour of using the Acland Video's Atlas and explore their perceptions of the strengths and weaknesses of this CAI.
Results
Ninety-seven of the 126 students (77%) enrolled in the MScOT program consented to participate in the study. There were no students who were excluded or withdrawn based on our criteria. All participants completed all data points of the study; there were no missing data. Demographic information, including gender, was not collected to maintain the anonymity of the learners, as there is traditionally a small proportion of male students in the University of Toronto MScOT program. Sixty-seven (69%) of the students had previous anatomy coursework and 30 (31%) had not taken an undergraduate course in human anatomy prior to admission in the MScOT program.
The results of Kember's Critical Self-reflection Questionnaire of the entire cohort are shown in the first column of Table 1. For each subscale, the highest score achievable is 20. The mean and standard deviation for each Kember subscale and the total score of the nonreflective subscales (i.e., HA and U) and reflective subscales (i.e., R and CR) are shown. The Understanding (U) subscale mean score was higher than all other subscales, while the Habitual Action (HA) subscale was the lowest. Table 2 summarizes the comparative analysis and effect size between Kember subscales using paired t-tests. All comparisons between subscales were found to be significantly different (p < .001). As such, the largest effect size was found between the U and HA subscales (ds = 1.3, 95% CI [1.0, 1.5]) which is very strong. 23 The low mean HA subscale score (10.1 ± 2.8) and moderate to very strong effect sizes between HA and the other subscales indicate that HA was not readily used during CAI.
Kember's Critical Self-Reflection Questionnaire outcomes.

Note. Maximum score per subscale is 20; higher scores represent stronger representation of the respective type of learning.
Comparison of Kember's nonreflective and reflective subscales.

Abbreviations: HA, Habitual Action, U, Understanding, R,Reflection, CR, Critical Reflection.
Significant at the α = 0.05 level (two-tailed).
Next, an exploratory look at the factors associated with students’ critical self-reflection was conducted. In the latter columns of Table 1, the Kember results are broken down between students with and without previous anatomy coursework. There was no significant difference between groups on all aspects of the Kember. Then, the academic outcome was evaluated. The average (mean ± standard deviation) Anatomy Quiz sum score of the cohort was 37.1 ± 6.7 (range: 17–50) out of a possible 56 points. The average term 1 grades were 83.8 ± 7.4% (range: 49.9–96.4). The Pearson correlations between anatomy quiz sum score, term 1 grades, and Kember's subscales are shown in Table 3. Directionally, the Kember Understanding (U) subscale demonstrated a positive relationship with academic outcomes (i.e., anatomy quiz sum score, term 1 grades), while all other subscales were negative. There were no significant correlations found among these data.
Relationship between Kember's subscales and academic outcome

Note. α = 0.05 level (two-tailed).
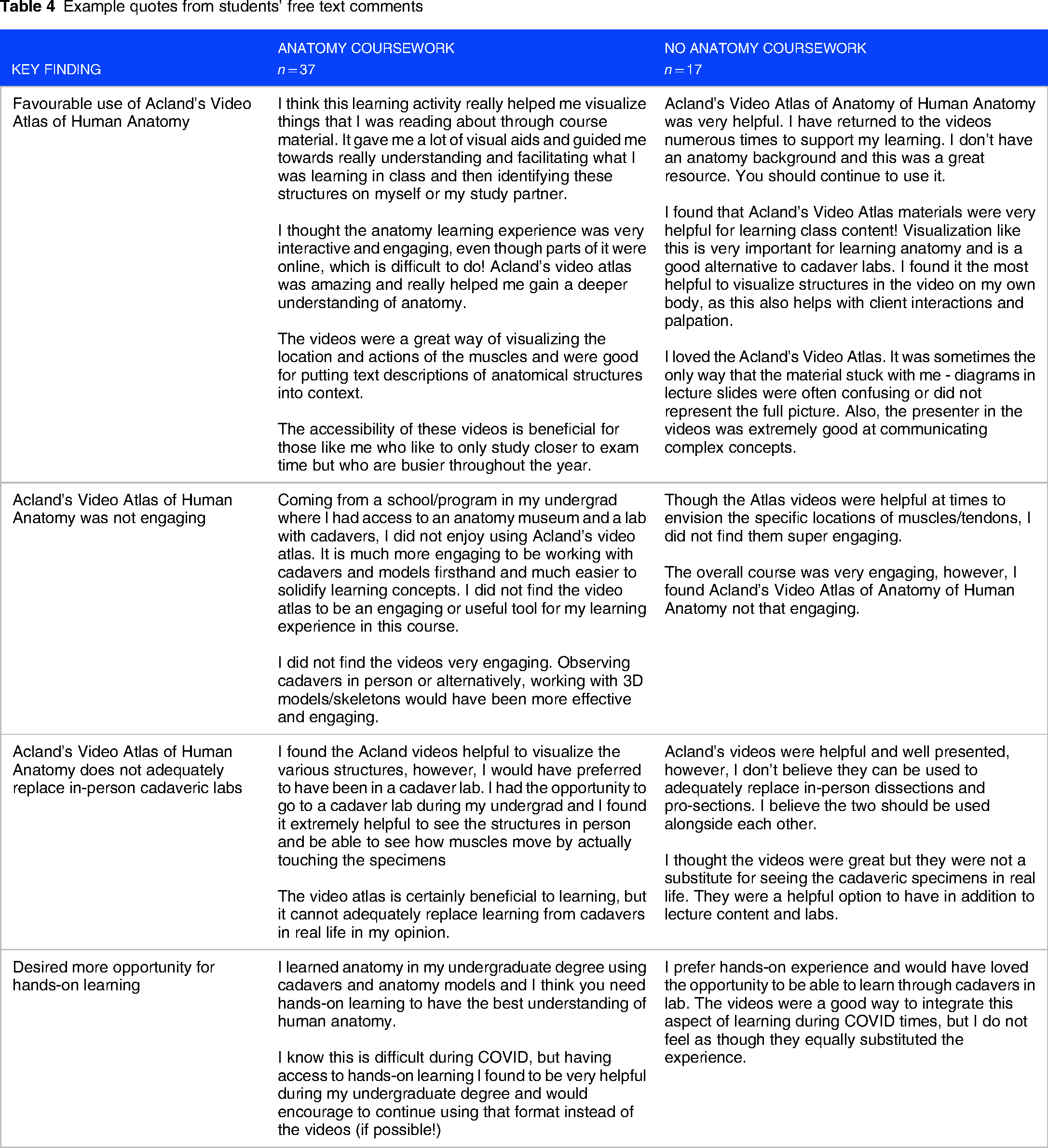
Lastly, 54 (56%) students provided free text comments with proportionate representation from those with previous anatomy coursework (n = 37, 55%) and those without (n = 17, 57%). The key findings from the descriptive analysis of the students’ comments are summarized in Table 4 using example quotes. While some students were in favour of using Acland's Video Atlas, many were critical of this CAI approach. Positive comments about Acland's Video Atlas included the opportunity to visualize the structures within the body, observing how the muscles activate, and the accessibility of the videos for studying purposes. In comparison, several students found that the videos were not engaging and should not be used in replace of in-person cadaveric labs. Students also desired greater opportunities for hands-on learning of anatomy. These views were expressed by students with and without previous anatomy coursework. Lastly, general appreciation for the diversity of resources offered to learn anatomy in this course was expressed and illustrated by this student: As an individual with a Kinesiology undergraduate degree, I believe that I have a thorough anatomy background. However, during all of my years in my undergraduate, I have always been taught anatomy in traditional ways (e.g., lecture and labs). What I genuinely enjoyed about this MSK term is that many of my different learning styles were brought to the forefront. Even though my recall was practiced, I was also encouraged to reflect and to practice my clinical judgement. I have never been taught anatomy in this manner, but I believe that I responded quite well (arguably better than all of my anatomy courses from my undergrad). I believe that providing many ways of learning allowed me to practice my anatomy in a comprehensive and thorough manner, and I feel that my learning was enriched significantly.
Example quotes from students’ free text comments
Discussion
This study aimed to describe students’ critical self-reflection while using CAI involving online self-guided anatomy modules with video-based pro-section instruction. Evidence from Kember's Critical Self-Reflection Questionnaire indicates that students did not engage in more reflective than nonreflective actions while using this type of CAI. Critical self-reflection was not related to previous anatomy coursework and academic outcomes. Lastly, some students expressed favourable use of Acland's Video Atlas of Human Anatomy, while many did not. Of those who did not, their comments indicated that this CAI is best used in a supplementary manner and additional hands-on opportunities to learn anatomy were needed. These findings provide important insights on how to best deliver anatomy education with cadaveric-based CAI.
The findings from this study indicate that students largely used cadaveric-based CAI to understand musculoskeletal anatomy. Students used Acland's Video Atlas to clarify and deepen their understanding of the spatial orientation of anatomical structures. The strength of this CAI approach was its usefulness in visualizing structures in the human body. However, students did not readily engage in critical self-reflection while viewing videos of pro-section instruction. These findings align with the recent survey conducted by Pettersson et al that found that medical students often use digital resources to identify and better visualize anatomical structures. Their study also reported that students would more likely use these online resources if there was an introduction provided on how the tool may be used and/or if there was an opportunity to interact with a tutor. 14 Therefore, students may require additional support to deepen their learning when using digital resources such as video-based cadaveric instruction.
Students’ lack of critical self-reflection while using video-based pro-section instruction may be related to the CAI but may also be associated with the overall course design and assessment approach. First, the Kember results indicate that CAI did not encourage students to reflect on why they were learning anatomy as student OTs. Although the online anatomy modules contained case-based scenarios, the clinical relevance of these cases was not readily appreciated. Intentional and effective strategies are needed to help students integrate what they are learning from cadaveric-based CAI with practice contexts. 24 Furthermore, occupational therapy anatomy instructors are called to and should place occupation at the centre of the curriculum. 25 Therefore, greater effort is necessary to design cadaveric-based CAI to support integrated learning of anatomy with the occupational and clinical sciences. 24
Next, the positive correlation between academic outcome and the Kember Understanding (U) subscale and the negative correlation between all other Kember subscales and academic outcome demands a closer look at course design and assessment. These findings appear to indicate that the course assessments (i.e., anatomy quizzes, reflection assignments, clinical skills assignments, practical skills exams) largely focused on lower-order thinking skills. Lower-ordered thinking skills are defined as Bloom's Taxonomy of cognitive learning levels of knowledge and understanding. 26 Our course is designed with a stronger focus on higher-order thinking assessments in the second term of the full-year course to evaluate students’ anatomy, biomechanics, and physiology knowledge using short-answer case-based exam questions. Therefore, despite the clinical orientation of the practical exam and clinical skills assignments, these performance-based assessments focused on students’ knowledge of surface anatomy, joint movements, goniometry, and muscle actions. Higher-order analysis of these concepts to clinical scenarios was not assessed. Therefore, the overall course assessment approach targeted knowledge and understanding of anatomy; this may have influenced students’ approach to learning with cadaveric-based CAI. Fostering critical self-reflection while learning anatomy with cadaveric-based CAI must include using course assessments that evaluate higher-order thinking. Contextualization of course assessments with simulations, case-based scenarios, and critical reflection may be helpful. 27
Lastly, the students in this study had differing perspectives on the use of cadaveric-based CAI. Overall, student free-text comments indicated that cadaveric-based CAI should be used in a supplementary manner and that opportunities for hands-on anatomy learning were needed. Experiential and hands-on anatomy pedagogies can be offered digitally through interactive applications such as virtual reality or using a nontech approach.28–30 For example, Gangata (2008) demonstrated that paper two-dimensional cutouts of muscles may be positively received by students as an effective method of learning spatial relationships between anatomical structures. 30 Chaudhuri trained students to draw during anatomical dissection. Students who engaged in drawing expanded their repertoire of learning styles to effectively learn anatomy. 29 As such, a variety of pedagogical approaches can offer hands-on learning experiences. Whether using digital technologies or not, anatomy educators should use innovative hands-on learning opportunities in conjunction with video-based pro-section CAI to optimize anatomy learning outcomes.
Limitations
This study provides new insights regarding the cadaveric-based CAI, but the findings should be considered within the context of its limitations. This study was conducted at a single institution with a response rate of 77% of the 2021–2022 MScOT student cohort. Despite anonymity at the time of completing the study, the students who participated may be more representative of students who have an interest in anatomy. Being conducted at a single institution from the University of Toronto may also have greater generalizability to learners from similar academic institutions. An a priori sample size calculation was also not conducted as this study sample was a convenience sample of MScOT students. Therefore, interpretation of the results must be considered within the limitations of potential type II error of nonsignificant results. Evaluating direct student usage of Acland's Video Atlas of Human Anatomy would have also enhanced this study as there is a known relationship between the frequency of accessing online resources and learning outcomes. 12 However, data regarding students’ usage of Acland's Video Atlas was not available. Lastly, the content analysis of the students’ free text comments was by no means meant to be a comprehensive approach to elucidating student perspectives of using cadaveric-based CAI. These descriptive findings were reported as an adjunct to the quantitative analysis of the Kember questionnaire.
Conclusion
This study found that entry-level student OTs used cadaveric-based CAI to understand musculoskeletal anatomy. The online self-guided anatomy modules and video-based pro-section instruction did not foster students’ critical self-reflection. Student's reception of video-based pro-section CAI was varied, but they welcomed its use in a supplementary manner. Overall, additional instructional and assessment design is needed to foster critical self-reflection and integrated learning of the anatomical and practice sciences. Anatomy educators using cadaveric-based CAI should invest in resources to design course and curriculum materials with integrated and hands-on learning strategies to optimize student anatomy learning experience and academic outcomes.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Department of Occupational Science and Occupational Therapy, Temerty Faculty of Medicine, University of Toronto.
Authors’ contribution
Emily S. Ho contributed to project administration, conceptualization, methodology, formal analysis, resources, supervision, writing–original draft, and review and editing. Erica Dove contributed to conceptualization, methodology, formal analysis, writing–original draft, and review and editing. Lorna Aitkens contributed to methodology, and writing–review and editing. Andrea Duncan contributed to methodology, resources, and writing–review and editing. Anne M. R. Agur contributed to conceptualization, methodology, and writing–review and editing.
Ethics
Approval for this study was obtained from the University of Toronto Research Ethics Board (Approval number: 41315).
Consent
Informed consent was received from the students who participated in this study.