
Abstract
BACKGROUND
Despite scholarly activity being an accreditation requirement for residency programs by the Accreditation Council for Graduate Medical Education (ACGME) since 2006, many family medicine programs have struggled to meet this requirement. A myriad of approaches and curricula have been proposed to enhance the scholarly output of residency programs.
OBJECTIVES
To determine the impact of a multimodal curricular intervention consisting of clear expectations, structured roadmap, availability of resources, and standardized accountability on the scholarly activity of residents.
METHODS
This is a quasi-experimental study with a retrospective data collection. The scholarly activities of residents completing training in the pre-intervention (2009-2012) and post-intervention period (2013-2017) were compared. Chi-square, Fisher's exact, Mann Whitney U, and Kruskal Wallis H tests were utilized to detect differences between the pre- and post-intervention groups. Multivariable Poisson regression models were used to detect independent predictors of per-resident scholarly activity. The institutional review board determined that the study was exempt from full review.
RESULTS
A total of 67 residents, 20 (30%) pre-intervention and 47 (70%) post-intervention, were included in the analysis. The number of total scholarly activities per resident increased significantly in the post-intervention period after adjusting for confounding factors (1.9 vs 6.4). The number of scholarly activities per resident also showed an increasing trend over time (P = .04). Moreover, traditional scholarship, including published manuscripts (0.35 vs 2.43) and national-level presentations (0.35 vs 1.27) also increased in the post-intervention period.
CONCLUSION
Implementing this comprehensive curriculum increased the scholarly output of residents and helped enrich the scholarship culture in the residency program.
Keywords
Introduction
The Accreditation Council for Graduate Medical Education (ACGME) is tasked with establishing and monitoring educational standards for physicians in training so that they are prepared to deliver the highest quality medical care to the American Public. It requires that faculty and residents in graduate medical education programs demonstrate scholarly activity to maintain institutional and program accreditation. 1 Scholarly activity during residency influences careers and how future physicians would practice.2,3 Although a culture of scholarship is essential to the existence of GME, it was not mandated by the ACGME for accreditation until 2006. 4 Since then, different approaches and curricula have been proposed, with varying degrees of success.4–7 However, it has been a common struggle for many family medicine residency programs to fulfill these requirements.6,8 In 2012, Crawford and colleagues noted scholarly activity as one of the most common citations by the Residency Review Committee (RRC). 8 In 2009, only 12.5% of the programs had > 25% of their residents published. Only 25.9% of the programs had 25% or more of their residents present at a regional, national, or international forum/medical conference. 8 “Scholarly activity” is not well-defined by the Residency Review Committees (RRCs) of the ACGME. Boyer 9 proposed 4 forms of scholarship: discovery, integration, application, and teaching. Seehusen et al 6 presented a “scholarly activity point” system to measure and serve as a catalyst to enhance resident scholarly activity.
Several studies report some success using interventions targeting different programmatic elements to enhance scholarship.10–12 However, a systematic review and metanalysis showed these to be inconsistent. 13 In 2009, our residency program introduced and implemented a 13-step structured roadmap as an intervention to completing at least one scholarly activity by every resident. 1 The development of a culture of scholarship transcends just fulfilling the accreditation requirements of resident scholarly activity. The cultural transformation where residents and core faculty work together on scholarly pursuits is challenging in the residency programs, given the open nature of the ecosystem. The constant flux of group members as they onboard and graduate, traditional models of cultural transformation developed for relatively closed groups aiming at creating critical mass, etc, are not as applicable to an open group. Waheed et al 1 showed that a process-driven approach with the process being a constant factor could work even with partial implementation of the curriculum. As different classes moved in and out of the residency over the years, this process remained a constant factor. It was shown to be associated with the successful establishment of a culture of scholarship. 1 Later, the process was further enriched with a bundled intervention with the addition of individual accountability by linking the progress to the Clinical Competency Committee summative and promotion, the addition of a standardized way of measuring the outcome of scholarship, and rewarding success in multiple ways. This study employs a retrospective cohort design to study the impact of full implementation of this bundled intervention.
We hypothesized that total scholarly activity and the number of activities in each type of scholarly activity per resident would increase in the post-intervention group, irrespective of the control variables.
Materials and Methods
Study design, study settings, interventions, and variables of interest
Study design: This study is part of a larger educational intervention thesis on creating and enhancing scholarly activities in Family Medicine residency training at the Pennsylvania University School of Medicine. 14 This study utilized a quasi-experimental design with a retrospective review of variables of interest in pre- and post-intervention periods. This study followed the SQUIRE 2.0 guidelines 15 or quality assessment and reporting the results (Supplementary Files). The Institutional Review Board (IRB) committee determined it to be “Not Human Subjects Research” via notification STUDY00004290.
Study setting: The principal investigator maintained a database of demographics, all types of scholarly activity, and other variables for all residency program graduates under study from the academic year 2009 through 2017. The intervention was fully implemented during the academic year 2012 to 2013. This divided the residents into 2 distinct periods of academic years: pre- (2009-2012) and post-intervention (2013-2017) groups.
The intervention: The intervention consisted of a comprehensive curriculum and supportive structure based on 3 basic elements (Supplemental Appendix A):
Clearly demarcated expectations:
Availability of resources:
Written guidelines and didactic curriculum supportive of scholarly activity. Quarterly resident and project update presentations, attended by the mentoring faculty, librarian, statistician, and IRB staff. Support (financial and administrative) for presentations at local, regional, national/international forums, and publications. Availability of protected time spanning 64 h of scholarly activity time requested by the resident from clinical and other work for important meetings and other pursuits involved in scholarly activity. Accountability on each step of a 13-step roadmap (Supplementary Appendix B):
Linkage of the 13-step roadmap to the Family Medicine Milestones. Quarterly reporting of project progress linked with milestones to regular performance evaluation by the Clinical Competency Committee, resident academic advisor, and the program director. For struggling residents, resident Individualized Education or Remediation Plan (IEP) created by the Directed Education Committee (DEC) targeting specific deficits. Rewarding the success of both faculty and residents with awards. Independent variable is the year of graduation as a marker of pre- or post-implementation of the intervention.
- Pre-intervention: graduates of the academic year 2009 to 2010 through 2010 to 2011. - Post-Intervention: graduates of the academic year 2012 to 2013 through 2016 to 2017. The dependent variable is the culture of scholarship as evidenced by per-resident scholarly activity from projects originating during the residency training period as calculated below:
Peer-reviewed web articles published Peer-reviewed articles (original research, case reports, letter to the editors, book chapters, other published work) in scientific journals indexed in PubMed and DOAJ. Local, Regional, National, or International presentations (podium/oral and poster). Other activities fulfilling Grassick criteria approved by the Program Director. The control variables include:
Medical School (LCME, International, and COCA accreditation) graduated from before joining the residency. Prior training or work experience before joining the residency. Type of clinical practice joined (academic or non-academic) after graduation. Fellowship pursued after residency training, if any.
Variables of interest:
Data collection and analysis
Data collection: The study investigators collected, de-identified, and stored the scholarly activity data of all residents in pre- and post-periods in an Excel workbook. The database was kept safe on a university-approved secured computer.
Data analysis: Chi-square and Fisher's Exact tests were used to determine differences in frequencies of independent and control variables at baseline in the pre- and post-intervention groups. The non-parametric Wilcoxon Rank Sum Test, also known as the Mann-Whitney U test, was used for bivariate analysis to determine statistical differences in dependent variables between the pre- and post-intervention period. The Wilcoxon Rank sum test was also used to detect any differences in dependent variables based on the independent variables. The Cochrane-Armitage trend test was used to determine the trend of scholarly works over the study period. 16 Multivariable Poisson regression models were used to detect independent predictors of per-resident scholarly activity. The parameter estimates for β were then exponentiated to calculate the rate of scholarly works per 10 residents and the relative likelihood of scholarly activity by each predictor variable. All statistical analysis was performed using SAS Software 9.4, and the level of significance was set at P < .05.
Results
A total of 67 residents completed 3-year family medicine residency training during the study period. Of these, 20 were in the pre-intervention group, and 47 were in the post-intervention group. Table 1 details the differences in pre- and post-group social and demographic characteristics. Of note, only race and prior training had significantly different distribution across the 2 groups. However, the skew of prior training was towards the pre-group (65% vs 12.8%), leading to more conservative estimates in the multivariable models.
Social and demographic characteristics in pre- and post-groups.
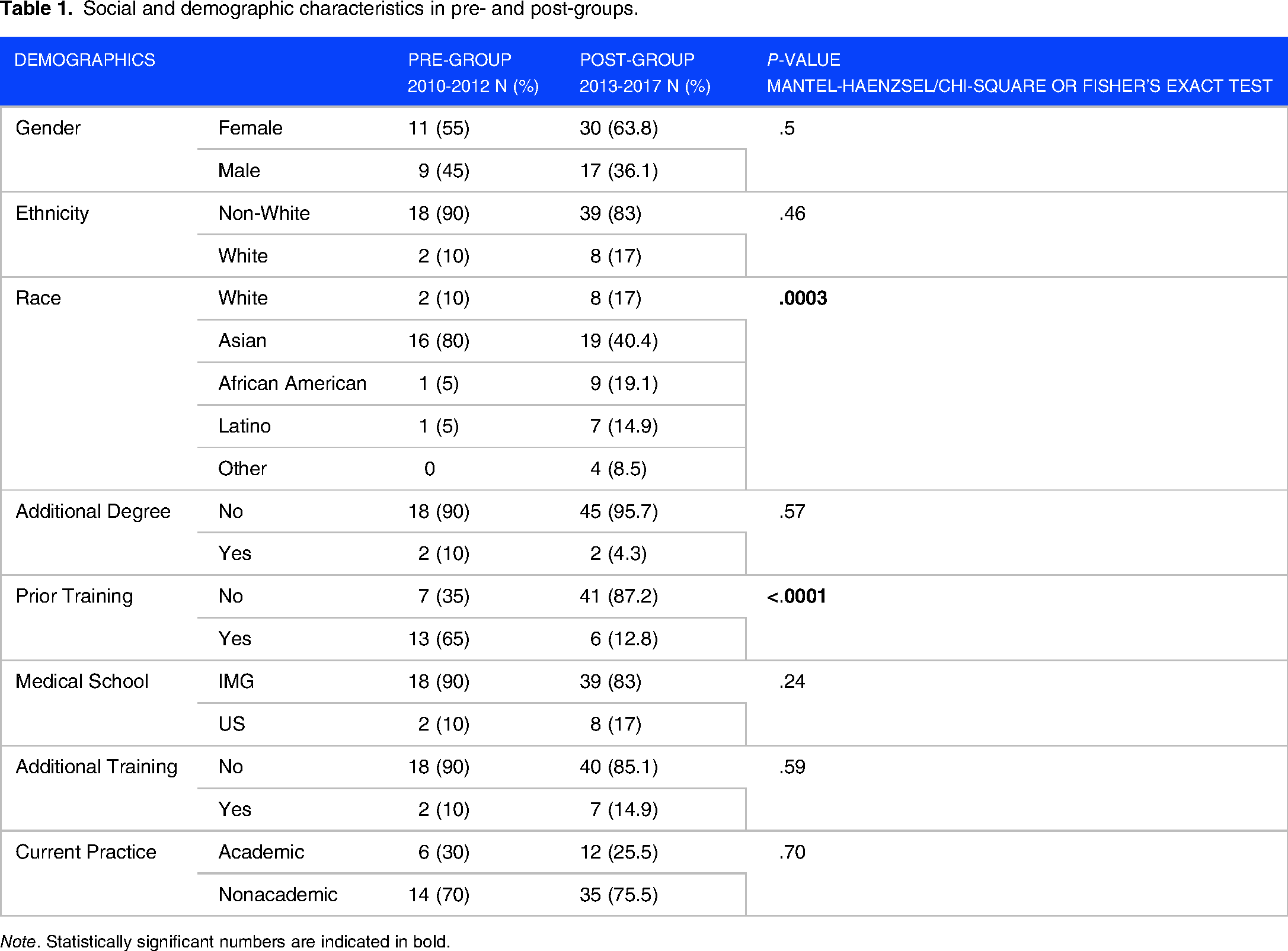
Note. Statistically significant numbers are indicated in bold.
Figure 1 shows bar charts indicating the cumulative numbers for all scholarly activities, presentations, and manuscripts produced by residents in each residency training class from 2010 through 2017. Figure 2 suggests an increasing trend in the number of works per resident by graduation year since the number of residents did not remain constant throughout the years (Cochrane-Armitage trend test analysis: P value = .04). Further breakdown of the number of presentations and manuscripts by residents in the pre-and post-intervention graduation years can be found in Supplemental Appendix C.
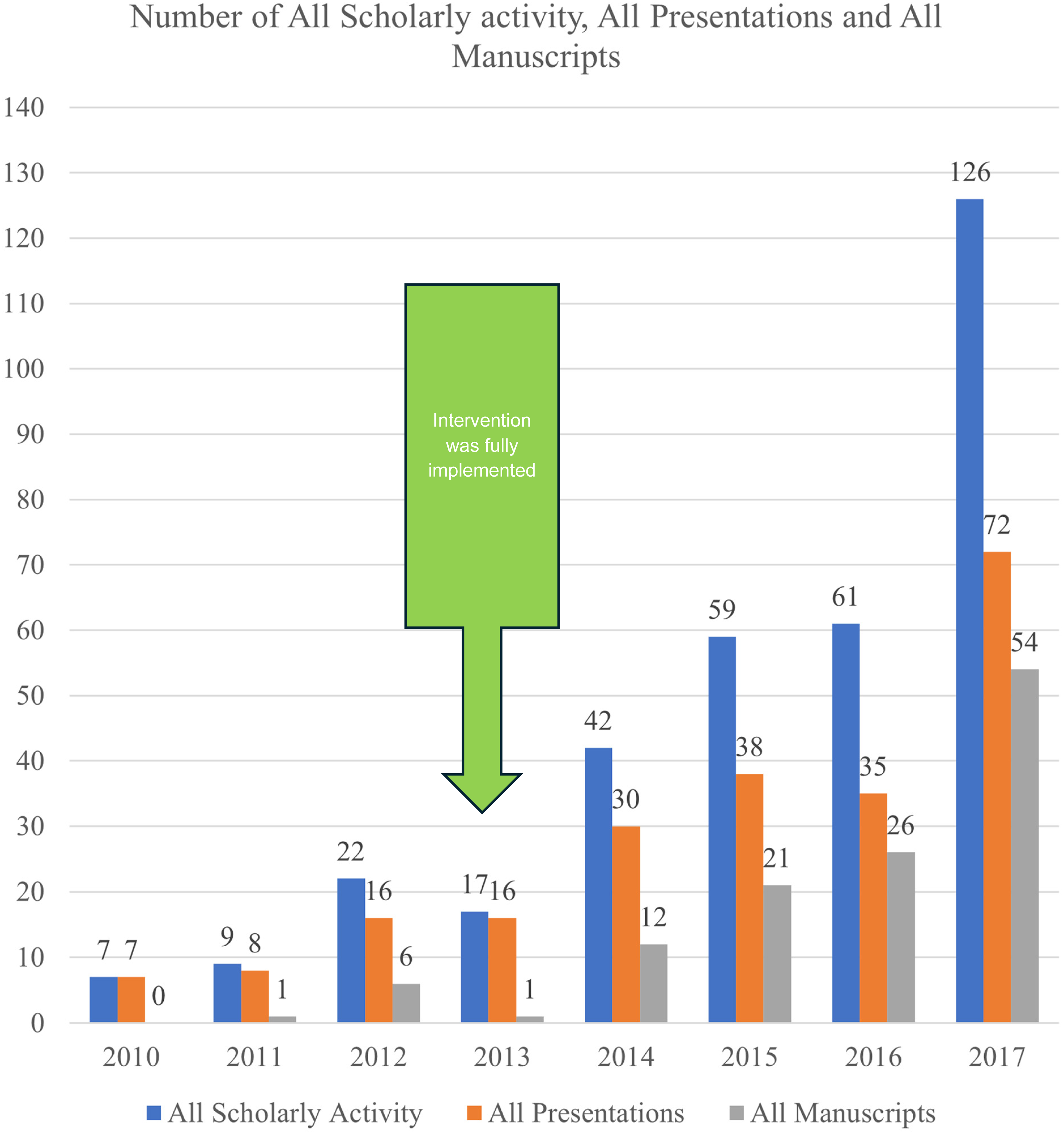
All scholarly activities by graduation year.

Number of all scholarly activities, all presentations, and all manuscripts per resident by graduation year.
Statistically significant differences in the overall and individual scholarly activity existed between pre- and post-group (Table 2). Specifically, statistically significant differences were noted in all scholarly activities, all presentations, regional and national level presentations, all manuscripts, original articles, reviews, and book chapters. The increase in post-group was not statistically significant in local-level presentations, case reports/series, community/letter to the editors, and non-peer-reviewed publications.
Number of all scholarly activities and all manuscripts by pre- and post-group.
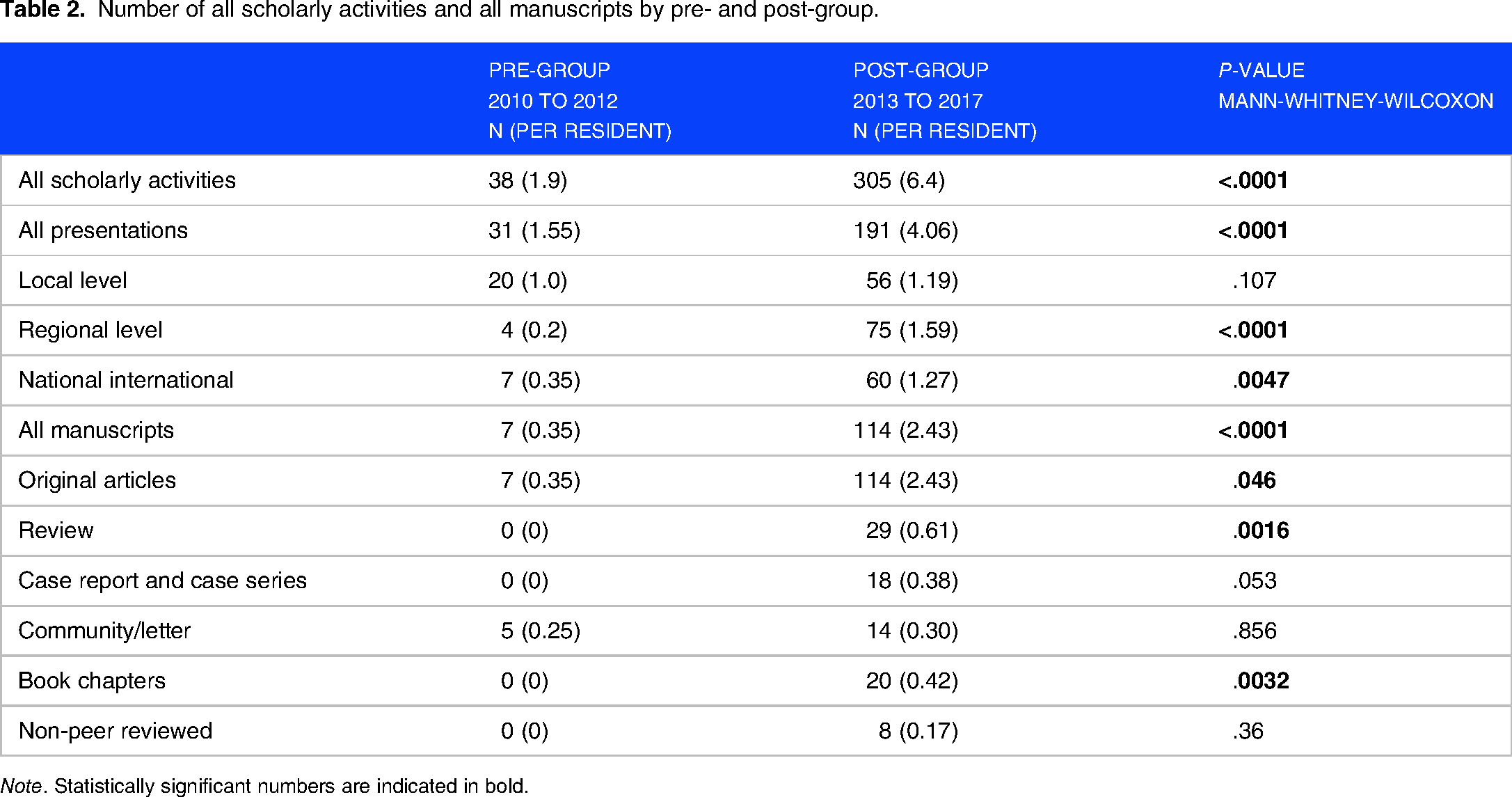
Note. Statistically significant numbers are indicated in bold.
The multivariable Poisson regression model demonstrated the point estimates of overall scholarly activities, incidence per 10 residents, and the relative risk associated with each independent variable (Table 3). There is a trend of increase in the number of scholarly activities produced by the resident as the time progressed from the graduation year 2010 through 2017, and the effect became statistically significant in the graduation year 2014, 2015, 2016, and 2017 (post-group). After adjusting for confounders, female residents’ overall scholarly activities were 60% higher than male residents (P value = .018). Similarly, after adjusting for all the control variables and graduation year, the international graduates (IMGs) produced 171% more scholarly activities than US MD and DO residents (P value = .0054). Those who joined academic practice produced 123% more total scholarly work than those who joined nonacademic practice (P value = .0004). Multivariable models for specific scholarly activities, including presentations and manuscripts, can be found in Supplemental Appendix D.
Poisson regression analysis of a number of all scholarly activities and the predictor variables.

Note. Statistically significant numbers are indicated in bold.
Discussion
This study shows the establishment and enrichment of the culture of scholarship in a residency program indicated by a statistically significant increase in resident scholarly activity as measured by the number of local, regional, and national presentations and publications.
Although the scholarship is integral to what academic clinicians do, it can be challenging to teach and accomplish in residency programs. This becomes even more challenging when the rigor of scholarly activities in 4 domains is judged with Glassick criteria. The most challenging domain for family medicine programs has been reported to be the Scholarship of Discovery and Teaching. 17 Demonstrating the fulfillment of multiple Glassick criteria, especially effective presentation, can also be challenging in many programs, especially in community hospitals.18,19 These challenges are evident at the individual program level, with citations from accreditation 8 and deficiencies in the workforce needed for the future of family medicine. 20 Waheed et al 1 previously reported the results of some efforts. They showed some positive trends in establishing a culture of scholarship 3 years after implementing a structured roadmap. This study demonstrated further enhancement and enrichment of the culture of scholarship by showing better outcomes comparing the last 3 years of the previous study (the year 2010 through 2012) with partial implementation of the intervention and 5 years after that (2013 through 2017) with full implementation. The demographics shown in Table 1 indicate that the population studied was diverse and comparable to what others have reported. 21
Overall, an increasing trend in producing scholarly works was found, as shown in the cumulative frequency graph in Figure 1. This was found to be statistically significant with a P value of < .0001 between pre- and post-intervention time, as shown in Table 3, and overall in 8 years over time as well. Although there is an increase in the post-intervention period (the year 2013), it only strengthens over time (in contrast with the year 2017). This is consistent with what others have reported with similar models.1,6 One could argue that the 3-year length of the residency program and resulting in overlap with other classes it might have confounded and artificially inflated the statistical difference between the pre- and post-intervention period. The contrary argument is that it takes time to nurture and strengthen a culture of scholarship. Waheed et al 1 from the same program published the scholarly activity preceding this period showing that implementation of some elements of this same curriculum showed improvement. The continued increasing trend with full implementation supports the hypothesis that the results are attributable to the comprehensive curriculum.
The overall number of presentations grew over time. There was a statistically significant increase in the number of per-resident presentations (Supplemental Appendix D) over the years. The difference is more prominent between the pre- and post-intervention periods (Supplemental Appendix C). Interestingly, although the number of local presentations increased in 2016 and 2017, the number of presentations at regional and national or international forums accounted for most of the growth observed in the overall number of presentations from 2010 through 2017. These trends are similar to what Seahusen et al 6 reported after introducing a point-scoring system.
The peer-reviewed publications are universally accepted as the prestigious form, outcome, and evidence of scholarly activity. 1 It is interesting to note that the publication of manuscripts is where there was maximum growth potential when it started in 2010. There were no manuscripts published by any of the graduates in 2010. The year 2011 showed only one publication. It increased to 6 presentations for all the residents who graduated in 2012 (Supplemental Appendix C). If drilled down closely, the rise in 2012 was because of 2 residents who wrote 4 and 2 manuscripts, respectively. These might have been outliers. To adjust for this, the graduation year was replaced in the Poisson regression model by a new variable that combined all the observations in the years 2010, 2011, and 2012 in pre-intervention years and 2013 through 2017. There was a 586% increase in the number of manuscripts published per every ten residents in the post-intervention group compared to the pre-intervention group (P value < .0001). This is remarkable growth overall.
Although historically, there has been a gender gap in scholarly activity, especially in the authorship of peer-reviewed publications, with males publishing more than females, 22 more recent studies show that the gap is decreasing. 23 This study shows a possible mechanism to educate female residents and bridge the gender gap over time. It shows that the female gender predicted a statistically significant increase in the number of scholarly activities regardless of the curriculum, medical school, prior training, additional training after residency, and practice setting type after graduation. This is an interesting finding since the number of females entering medicine in general and family medicine in specific has increased over time. 24 Although Malchuk et al, 25 in their recent article, argued that the increase in the first authorship of articles by females is related to the increase in the number of last authorships by females, indicating that the increase in mentorship from females has occurred, this study did not look at the gender of mentors. This area is where further investigation is needed to understand the causes and remedies to bridge the gender gap.
This study shows that the type of medical school where the residents graduated is an independent predictor of the number of scholarly activities overall and in all categories. The international medical graduates, for example, had 171% more overall scholarly activities (P value < .0054) and 141% more presentations (P value < .0010) as compared to the graduates of LCME graduates (P value < .0054). It is intuitive to believe that the culture of scholarly activity in a residency program indicates the strength and academic rigor of a program. In 2005, Senf et al 26 showed that interest in research and scholarship among medical students in LCME-accredited schools was inversely proportional to students’ interest in family medicine as the choice of specialty. More recently, data on this issue has been scarce. However, Waheed et al 27 reported the strength of research and scholarly activity to be a lower priority for medical students when ranking programs. Although some might argue that higher requirements for scholarly activities might serve as a detriment in recruiting graduates of LCME-accredited institutions, more work needs to be done to understand the relationship.
A recent survey of program directors shows that most program directors value applicants’ experience of scholarly activity for residency and fellowship programs. 28 Although it is intuitive to think that residents interested in pursuing academic careers and fellowships after residency would try to produce more scholarly works to be more competitive, there is not enough data documenting that. This study shows that those who pursued academic practice produced 123% more overall scholarly activities than those who went into non-academic practice after graduation (P value < .004). Similarly, those who went into academic practice presented 99% more than those who went into private practice (P value < .005). Although it is consistent with a similar previous study from our program, 1 personal characteristic and training parameters that shape the decision on practice setting after graduating from the residency program need further investigation.
Our study has both strengths and weaknesses. The data was collected retrospectively, and recall bias could play a role while data was stored or abstracted for this study. The tracking and storing mechanisms for at least the presentation category might have been more robust in the post-intervention period. The diversity of our residents does increase the generalizability to the diverse US population in the residency programs. However, the increase in scholarly activity seen after implementing a scholarly activity road map in our study is an association. It does not fulfill all conditions to establish a causal relationship conclusively. It is also possible that with the development of a program's reputation where scholarly activity is valued and encouraged, the program started to attract candidates with a genuine interest in publishing scientific work, leading to a selection bias in the latest cohorts. However, it is also prudent to point out that the pre-intervention group had a higher incidence of work experience or training before starting residency. This would lend out estimates of the impact of the intervention to be more conservative.
Conclusion
The implementation of a comprehensive curriculum based on clear expectations, availability of resources including teaching and mentorship, and accountability on a structured roadmap increases the likelihood of more scholarly activities by the residents. The increased scholarly activities by the residents are a way of demonstrating the establishment and enrichment of a culture of scholarship in a residency program.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241287449 - Supplemental material for Impact of a Structured Roadmap, Individual Accountability and Support, and Outcome Measurement on the Culture of Scholarship in a Residency Program
Supplemental material, sj-docx-1-mde-10.1177_23821205241287449 for Impact of a Structured Roadmap, Individual Accountability and Support, and Outcome Measurement on the Culture of Scholarship in a Residency Program by Abdul Waheed, Erum Azhar, Faisal Aziz, Munima Nasir, Muhammad Ali Chaudhary and Li Wang in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241287449 - Supplemental material for Impact of a Structured Roadmap, Individual Accountability and Support, and Outcome Measurement on the Culture of Scholarship in a Residency Program
Supplemental material, sj-docx-2-mde-10.1177_23821205241287449 for Impact of a Structured Roadmap, Individual Accountability and Support, and Outcome Measurement on the Culture of Scholarship in a Residency Program by Abdul Waheed, Erum Azhar, Faisal Aziz, Munima Nasir, Muhammad Ali Chaudhary and Li Wang in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors thank Dr Paul V. Atiken Jr, MD MPH, FAAFP, Program Director of Penn State Family & Community Medicine Residency (2005-2012) for his contributions to the development of “Scholarly Activity Guidelines” which became the basic framework for the curriculum and developing the intervention in this study.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author's Contributions
The authors confirm their contribution to the article as follows: AW and EA contributed equally to the study conception, designed the study protocol, submitted it to the Institutional Review Board, and participated in data collection and entry. Data analysis was performed by AW, EA, MAC, and LW. All authors were involved in the interpretation of the results. The manuscript was written by AW, MAC, and EA. All authors contributed intellectually and edited the manuscript. All authors read and approved the final manuscript. AW is the corresponding author and is responsible for the integrity of the work.
Ethical Approval
The Institutional Review Board (IRB) at Pennsylvania State University College of Medicine determined it to be “Not Human Subjects Research” via notification STUDY00004290.
Patient Consent
Patient consent was not applicable since it is not Human-Subjects-Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.