
Abstract
GASMAN software, a simulation tool for inhalational anesthetics’ pharmacokinetics and pharmacodynamics, has become essential in both anesthesia education and clinical practice. This review explores its applications, highlighting its effectiveness in enhancing medical education and its impact on clinical anesthesia management. In educational settings, GASMAN software facilitates a deeper understanding of anesthetic pharmacology through interactive and visual simulations, thereby improving students’ learning outcomes and engagement. Clinically, it aids anesthesiologists in optimizing anesthetic dosing, enhancing patient safety, and supporting real-time decision-making during surgeries. Despite its advantages, GASMAN software faces limitations such as the absence of physiological feedback and the need for continuous data model updates. Future directions include technical enhancements, integration with advanced patient simulators, and broader dissemination through educational partnerships. This review emphasizes the significant contributions of GASMAN software to anesthesia education and clinical practice and suggests pathways for future improvements and wider adoption.
Introduction
With the development of anesthesia education, the application of simulation software has become increasingly widespread. These tools not only enhance teaching efficiency but also provide a safe training environment for anesthesia students and professionals.1,2 GASMAN software is an efficient tool for simulating anesthetic pharmacokinetics and pharmacodynamics, offering learners a near-real clinical experience to understand the pharmacokinetic and pharmacodynamic properties of anesthetic drugs. Over the past 40 years, GASMAN software has made significant progress in its application in anesthesia education and clinical practice. To comprehensively review the functions of GASMAN software and its current applications in teaching and clinical practice, and to discuss future development directions, we conducted an extensive literature search. The databases searched included PubMed, Embase, Web of Science, and Cochrane Library for English publications, and WanFang and CNKI for Chinese publications. The search terms used were “GasMan software or GASMAN@ or GasMan simulator” and “anesthesia or anesthesia simulation or anesthesia teaching or pharmacokinetics simulation.” The literature search encompassed studies published from 1982 to 2024.
The inclusion criteria were defined as follows: Studies focusing on the application of GASMAN software in anesthesia education and clinical practice. Article types encompass original research, reviews, case studies, and practice reports. Peer-reviewed articles published in English or Chinese. Exclusion criteria were: Articles not related to the topic. Conference abstracts, book reviews, and commentaries without original data support.
We systematically analyzed the included literature, extracting information related to the functionalities, application outcomes, advantages, disadvantages, and future development directions of GASMAN software. Employing a narrative synthesis approach, we categorized and summarized the effects of GASMAN software in both educational and clinical settings, and explored potential future directions. This review aims to provide a comprehensive, systematic, and evidence-based assessment that underscores the significant role of GASMAN software in anesthesia education and clinical practice, while also suggesting avenues for its enhancement and broader adoption.
Overview of GASMAN software
GASMAN software was developed by Dr. James H. Philip and his team at Harvard Medical School in 1982. 3 By inputting patient weight, anesthetic type, and flow rate, the software can calculate and display the concentration changes of anesthetics in various tissues in real-time, as well as the resulting changes in anesthetic depth. This feature allows users to intuitively understand the distribution and metabolism of anesthetic drugs, thereby optimizing anesthesia management.
Specifically, GASMAN software can achieve the following functions (https://www.gasmanweb.com/software/):
Simulate the dynamic process of inhaled anesthetics: The software can simulate the transport of anesthetic drugs in the lungs, blood, and tissues in real time based on the input parameters.
Provide detailed pharmacokinetic and pharmacodynamic data: Users can view the concentration change curves of anesthetic drugs in the body and analyze their effects. Support the simulation of multiple anesthetics: Including isoflurane, sevoflurane, desflurane, and other commonly used inhaled anesthetics. Personalized settings: Allow users to conduct personalized simulation settings based on the specific conditions of different patients to ensure the accuracy and clinical relevance of the simulation results. Parameter input interface (Figure 1A): Users can input basic patient information and anesthetic parameters, such as weight, anesthetic type, and concentration. Real-time simulation display interface (Figure 1B): This interface displays the concentration change curves of anesthetic drugs in various tissues during the simulation, allowing users to observe changes under different conditions by adjusting parameters. Results analysis interface (Figure 2A): Provides detailed simulation results analysis, including drug concentration changes and anesthetic depth evaluation, allowing users to conduct in-depth learning and research based on these data. Help and support interface (Figure 2B): This interface provides user manuals, operation guides, and frequently asked questions to help users resolve issues encountered during use.
The user interface of GASMAN software is designed to be simple and intuitive, allowing users without a professional computer background to get started easily. The main interfaces include:

(A) Parameter input interface; (B) real-time simulation display interface.
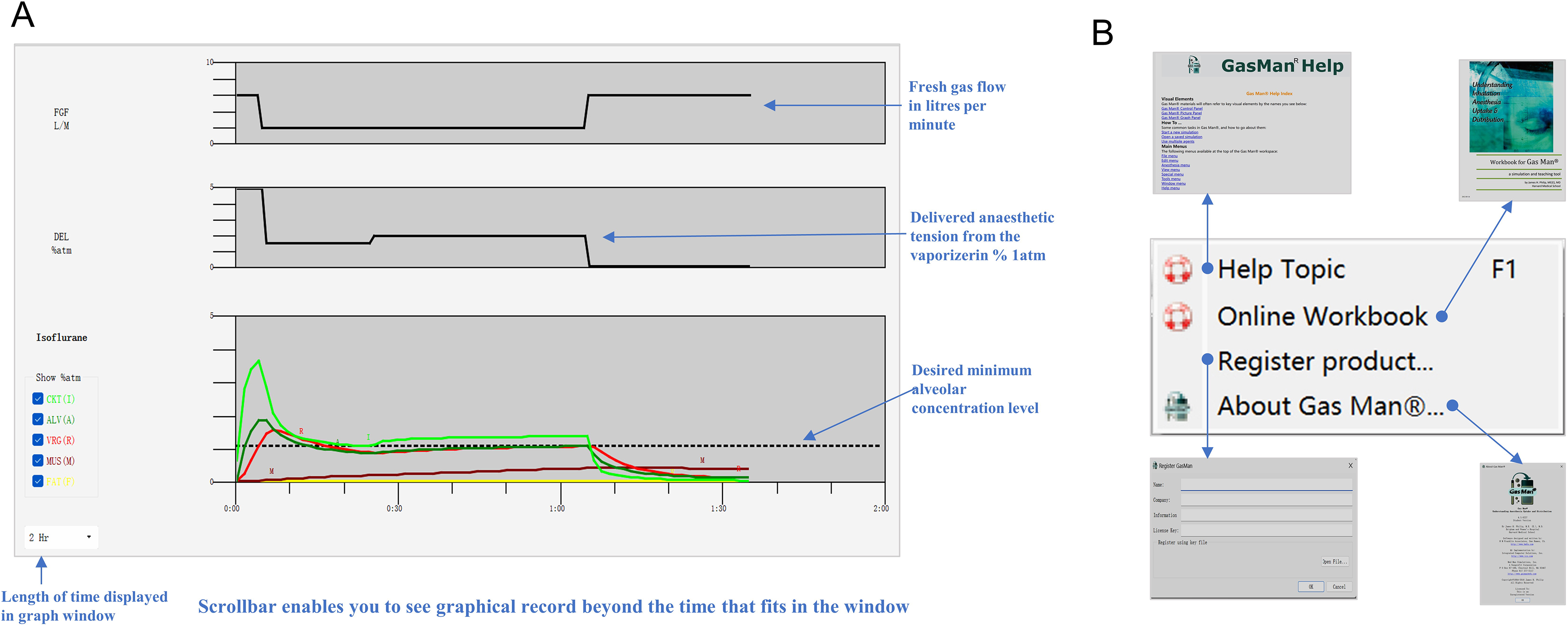
(A) Results analysis interface; (B) help and support interface.
Logistics of using GASMAN software
Software Installation and Licensing Management: The basic license for GASMAN software is free for individual users and supports both Windows and Mac OS X versions (https://www.gasmanweb.com/order). Users can download the software from the official GASMAN website and register as needed to access the professional version. The installation process is straightforward, requiring users to follow the provided instructions.
Training and Support: GASMAN software includes comprehensive tutorials and usage guides that cover basic and advanced concepts in pharmacokinetics and pharmacodynamics (https://gasmanweb.com/Workbook.pdf). These tutorials address single-compartment and 2-compartment models, alveolar tension curves, blood/gas solubility, optimal anesthesia plans, low-flow anesthesia, and closed-circuit anesthesia. Additionally, GASMAN software offers online support and technical assistance to ensure users can effectively utilize the software for teaching and research purposes (https://www.gasmanweb.com/educational-tools/).
Integration into Educational Curricula: Many medical schools and teaching hospitals have incorporated GASMAN software into their anesthesia education programs. For example, GASMAN software is used in anesthesiology residency programs to assess and enhance trainees’ core competencies through assignments and mentor evaluations (https://www.gasmanweb.com/). The software's computer-based exploration activities allow trainees to reinforce theoretical knowledge through practical application.
Evolution of GASMAN software
Since its inception, GASMAN software has undergone significant advancements in both functionality and application. Initially developed in the 1982s by Dr. James H. Philip, GASMAN started as a basic tool for simulating drug uptake and distribution in anesthesia . Over the years, the software has evolved to incorporate more complex physiological feedback mechanisms and real-time data updates, enhancing its accuracy and applicability in clinical settings. 4
Technological Advancements: The early versions of GASMAN were primarily focused on simple pharmacokinetic simulations. 3 The current versions now include advanced features such as the ability to simulate the pharmacodynamics of various anesthetic agents in real-time, providing a more comprehensive understanding of anesthesia management. 4 The software now supports cross-platform compatibility, allowing it to be used on both Windows and Mac OS systems, and has been optimized for a wide range of hardware configurations, making it accessible to a larger user base (https://www.gasmanweb.com/order). Educational Expansion: Initially used for basic education of anesthesia students, GASMAN is now widely integrated into residency programs and advanced training for anesthesiologists. The software's comprehensive tutorials and interactive modules help trainees understand complex concepts in pharmacokinetics and pharmacodynamics through practical application. 5 The software includes detailed tutorials and workbooks that guide users through various scenarios, enhancing their learning experience. It has been used in numerous medical and veterinary schools worldwide, demonstrating its versatility and effectiveness in different educational contexts (https://gasmanweb.com/Workbook.pdf). Deepening Clinical Applications: As GASMAN software has been applied across various anesthesia subspecialties, an increasing number of clinicians have started using the software to optimize anesthesia plans, improve patient safety, and support real-time decision-making.6,7
Application of GASMAN Software in Anesthesia Education
GASMAN software has extensive applications in medical education, particularly in anesthesia courses for medical students, training for novice anesthesiologists, and training for anesthesia nurses.5,8 The following sections provide a systematic review of the application of GASMAN software in these fields based on published literature.
Understanding pharmacology
Studies have shown that the use of GASMAN software significantly enhances medical students’ understanding of the pharmacology of inhaled anesthetics.6,7 By simulating the use of different doses and drugs, students can more intuitively grasp the concepts of pharmacokinetics and pharmacodynamics. The interactive and visual features of GASMAN software make complex pharmacological principles easier for students to understand, increasing their interest and engagement in learning. 9 By simulating real clinical cases with GASMAN software, students can practice different anesthetic strategies for patients with various disease states, thereby improving their practical skills. 10 Additionally, GASMAN software can provide personalized teaching content based on students’ learning progress and needs, maximizing learning outcomes. 9
Clinical decision training
Research indicates that GASMAN software plays a crucial role in clinical decision training for novice anesthesiologists. By simulating the use and adjustment of different anesthetic drugs during surgery, novice anesthesiologists can practice making reasonable decisions in various clinical situations. Virtual simulation allows novice anesthesiologists to practice in complex clinical scenarios, consolidating their skills and boosting their confidence. 11 The real-time feedback provided by GASMAN software helps novice anesthesiologists better understand the consequences of their actions, improving their ability to handle emergencies. 12 Furthermore, GASMAN software provides a risk-free virtual environment where novice anesthesiologists can repeatedly practice different anesthetic techniques and strategies without the risk of harming real patients. 13
Integrated teaching applications
Studies have explored the potential of integrating GASMAN software with other simulation tools. For example, combining GASMAN with high-fidelity patient simulators (HPS) provides a more comprehensive teaching experience, significantly enhancing beginners’ overall clinical abilities.1,4 GASMAN software is not only suitable for teaching students in school but also for continuing education and training of practicing doctors and nurses. Through continuous simulation training, healthcare professionals can continuously update and enhance their professional skills. 14 Qian et al 11 found that compared to traditional teaching methods, the application of GasMan software's computer simulation teaching method in the standardized training of anesthesia nurses significantly improved theoretical test scores, practical operation skills, and satisfaction levels. Qian et al 11 used GASMAN software to assist in teaching inhalation anesthesia to junior anesthesiologists, which improved theoretical test scores, learning interest, and efficiency, gaining recognition from both resident physicians and training instructors.
Other simulation software in anesthesia training
In addition to GASMAN software, several other simulation tools are widely used in anesthesia training, providing comprehensive educational resources and enhancing clinical skills development. For instance, SimMan® (Laerdal Medical) is a high-fidelity patient simulator that offers realistic training scenarios for anesthesiologists, including emergency situations and routine procedures.15,16 The Virtual Anesthesia Machine (VAM) is another valuable tool that simulates the behavior of anesthesia machines and patient responses, making it useful for both education and research. Developed at the University of Florida, VAM allows users to interact with a simulated anesthesia machine, providing visual and auditory cues to enhance learning. 17 Anesthesia SimSTAT, developed by the American Society of Anesthesiologists, focuses on online, interactive simulations that cover critical incidents and perioperative management. 1 METI HPS (Medical Education Technologies, Inc.) is renowned for its advanced physiological models and the ability to simulate a wide range of patient responses to anesthesia and other interventions. 18 These tools, along with GASMAN, form a comprehensive suite of resources that significantly contribute to the education and training of anesthesia professionals.
Application of GASMAN Software in Clinical Anesthesia Practice
In recent years, the application of GASMAN simulation software in pharmacokinetic studies of anesthetics has been widely validated. Van Zundert et al 19 used GASMAN software to study the effects of solubility, cardiac output, and ventilation on the FA/FI curve and FVRG, obtaining results similar to clinical studies. Athiraman et al 20 compared the end-tidal isoflurane concentrations predicted by GASMAN with actual patient measurements, finding that the software's predictions were very close to the actual values, with a median absolute performance error of 9.39% and a median performance error of −5.30%, demonstrating the software's accuracy and utility in pharmacokinetic education. Casan et al 4 developed a software-based anesthesia workstation compatible with LLEAP simulators, creating a pharmacokinetic model of inhaled anesthetics based on GASMAN. Their results showed that the model's deviation from the GASMAN reference was <.01 volume percent, indicating high accuracy in simulating mechanical ventilation and halogenated agent delivery. 4 Weber et al 21 compared a GASMAN model with standard models for predicting end-tidal desflurane and sevoflurane concentrations in healthy lung patients. The results showed that the parameter-matched model had significantly higher prediction accuracy during induction and elimination, while both models had no significant difference during maintenance. Enhancing the standard model with improved ventilation and hemodynamic input variables can improve its predictive performance. 21 These studies validate the high accuracy and practical application of GASMAN software in simulating and predicting the pharmacokinetics of inhaled anesthetics, laying a solid foundation for its application in clinical anesthesia simulation.
Anesthesia emergence simulation
Facilitating patient emergence from anesthesia is important for improving operating team efficiency and reducing anesthesia costs. Desflurane has lower solubility compared to isoflurane, leading some clinicians to consider switching to desflurane at the end of anesthesia to aid recovery. Simulations using GASMAN software have shown that this method has limited effect on promoting anesthesia recovery, 22 a finding subsequently confirmed by clinical studies. 23 This highlights the importance of using simulations to validate clinical strategies.
Hyperventilation at the end of anesthesia can aid the elimination of anesthetics, potentially benefiting patient recovery. GASMAN software simulations have shown that the benefits of this method are more pronounced for highly soluble inhaled anesthetics. 24 These results have been validated in clinical studies, 25 providing valuable insights into ventilation strategies in anesthesia management.
Prolonged anesthesia recovery has always been a concern. GASMAN software can simulate the concentration changes of inhaled anesthetics in various tissues (VRG, muscle, and fat) during prolonged anesthesia, helping to improve the accuracy of predicting patient recovery and reducing the incidence of delayed recovery. 26
Anesthesia induction simulation
In pediatric anesthesia, inhalation induction is commonly used when establishing intravenous access is difficult. Using GASMAN software to pre-optimize the anesthesia plan can significantly shorten induction time and increase safety. 27
Another study used GASMAN software to compare the effects of intravenous propofol induction and vital capacity inhalation (8% sevoflurane) induction in general anesthesia, explaining the similarity in induction and recovery times between the 2 methods. This simulation revealed the actual effects of 2 common anesthesia methods, providing evidence for clinical choices. 28
Anesthesia depth control simulation
End-tidal anesthetic concentration is often used as an indicator of anesthesia depth. Clinical studies validating GASMAN software simulations of end-tidal anesthetic concentrations have yielded consistent results, suggesting that the software can be a useful alternative when direct end-tidal concentration monitoring is unavailable. 29
Anesthetic waste management
The environmental impact of inhaled anesthetics has garnered significant attention. Dexter and Epstein 30 and Candries et al 31 studied the application of GASMAN software in anesthetic waste management, demonstrating its value in improving waste capture efficiency and predicting anesthetic consumption. Dexter and Epstein 30 used GASMAN software to simulate the capture of desflurane and sevoflurane under various fresh gas flow rates and anesthesia durations, showing that efficient gas capture systems can significantly recover anesthetics even under low-flow conditions. Candries et al 31 validated GASMAN software's accuracy in predicting sevoflurane consumption across different fresh gas flow rates, finding that the software's median performance error and median absolute performance error were both <10%. These studies indicate that GASMAN software has a significant application value in anesthetic waste management and consumption prediction.
Other clinical anesthesia scenarios simulation
Kuo et al 7 simulated spontaneous recoveries after airway obstruction during inhalation induction using GASMAN software, exploring the time needed for the VRG anesthetic level to drop below the obstruction threshold under different conditions. This study highlighted the importance of considering anesthetic levels at the effect site during induction. 7
Leeson et al 6 investigated the potential for re-anesthesia due to hypoventilation after initial recovery from volatile anesthesia, using GASMAN software to simulate desflurane, sevoflurane, and isoflurane uptake and elimination. The results showed that re-anesthesia is likely with prolonged anesthesia and severe hypoventilation, with muscle tissue being the main source of anesthetic redistribution and fat tissue contributing to sustained recovery. 6
Weber et al 32 used GASMAN software to simulate the impact of obesity on volatile anesthetic elimination, constructing models with different body weights by increasing fat tissue. The results indicated that while wake-up times were similar, recovery and washout times were prolonged with increasing obesity, suggesting that excess fat tissue in obese patients may serve as a reservoir for volatile anesthetics, affecting the recovery process. 32
Advantages and Disadvantages
Advantages
GASMAN software demonstrates numerous advantages in anesthesia education and clinical practice. In education, the interactive and real-time feedback features of GASMAN software significantly increase students’ interest and engagement. Students can intuitively understand the pharmacokinetics and pharmacodynamics of different anesthetics by simulating various doses and combinations, improving their grasp of complex concepts. Additionally, the risk-free virtual environment allows students to repeatedly practice different anesthetic techniques and strategies, enhancing their practical skills and confidence. In clinical practice, GASMAN software helps anesthesiologists accurately adjust anesthetic doses by simulating the effects of different drug doses, optimizing anesthetic use, and reducing side effects. Moreover, the software provides real-time data on drug metabolism and physiological parameter changes during surgery, aiding in quick and accurate clinical decision-making.
Disadvantages
Despite its significant advantages, GASMAN software also has notable limitations. Firstly, GASMAN software can only simulate the pharmacokinetics of drugs and lacks feedback on physiological functions such as vital signs and bispectral index (BIS), meaning users still need a solid foundation in inhalational anesthetic pharmacology to use it effectively. Additionally, although GASMAN software is trained on extensive clinical sample data, it cannot cover all clinical situations and individual variations, necessitating continuous updates to its data models to improve simulation accuracy. Finally, the usage costs may limit its adoption in medical schools in economically underdeveloped regions. According to the GASMAN software website, the basic license for individual users is free, including downloads for Windows and Mac OS X versions. However, for educational institutions and medical facilities, while the software itself is free, there are costs associated with user training, hardware equipment, technical support, and maintenance that need to be considered.
Future Directions
In terms of technical improvements, further development, and optimization of software algorithms are needed to enhance simulation accuracy for complex clinical situations and individual variations. Integrating GASMAN software with advanced patient simulators could provide feedback on vital signs and BIS, achieving immersive anesthesia simulations and enhancing teaching effectiveness. 4 Regarding research and evaluation, long-term follow-up studies should be conducted to assess the actual impact of using GASMAN software on students’ career development and clinical practice, providing more evidence to support its educational benefits. Comparative studies should also be performed to clarify its unique advantages and applicable scope. In terms of promotion and dissemination, partnerships with educational and medical institutions should be strengthened to expand the application of GASMAN software through training sessions and seminars. Additionally, advocating for supportive policies from relevant authorities to provide funding and resources would encourage the adoption of GASMAN software and similar innovative technologies in educational and medical institutions.
Conclusion
GASMAN software offers significant advantages in anesthesia education and clinical practice, including enhanced understanding, improved practical skills, optimized anesthetic use, and real-time decision support. However, its limitations, such as the lack of physiological feedback, insufficient simulation accuracy, and high costs, cannot be overlooked. Future research should focus on technical improvements, outcome evaluations, and wider adoption to further enhance the value and impact of GASMAN software.
Footnotes
Author Contributions
Chao Chen and Shengfeng Yang contributed equally to this work. Literature search: Chao Chen, Shengfeng Yang, Yewei Shi, and Xingfeng Zhong. Manuscript writing: Chao Chen and Shengfeng Yang. Manuscript revision: Xinglong Xiong and Jing Shi. Funding acquisition: Chao Chen. All authors contributed to, approved, and take accountability for the final manuscript.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Teaching Content and Curriculum System Reform Project of Guizhou Higher Education Institutions, The 2021 Undergraduate Teaching Content and Curriculum System Reform Project of Guizhou Medical University (grant numbers 2021145 and JG2021026).