
Abstract
OBJECTIVES
Virtual reality (VR) appears to be a promising educational tool for otorhinolaryngology (ORL) residency training, as it allows for safe and effective practice immediate feedback and potential improvements in patient outcomes. Despite these advantages, VR has not yet been incorporated into residency training in ORL, which may be due to limited availability or validation and skepticism toward incorporation of new training methods. This study investigates whether a VR model of the temporal bone improves learning success for ORL residents in comparison to standard plastic models and whether it depends on surgeon's experience. We also included a subjective evaluation of the learning experience with both models.
METHODS
ORL residents and specialists at 2 German university hospitals were tested on their knowledge of temporal bone anatomy after training with either VR or standard plastic models. In addition, we compared knowledge of the temporal bone anatomy before- and after-VR training. Lastly, a subjective survey on the benefits and limitations of VR was conducted to assess participants’ views on this new technology.
RESULTS
About 85% of the participants considered VR to be better than conventional models and agreed that VR was a useful tool for teaching complex anatomy. Objective evaluation showed significant improvement in knowledge after using VR (before/after comparison), especially in participants with a higher level of preexisting knowledge. Direct comparison to conventional plastic models showed no superiority of the VR model.
CONCLUSION
VR models in ORL are not only appealing and motivating for residents, but also objectively improve their anatomical knowledge, especially in advanced residency. In addition, VR—in contrast to the plastic model—offers opportunities for further development and optimization.
Keywords
Introduction
This study aims to investigate if virtual reality (VR) technology has the potential to revolutionize teaching in otorhinolaryngology (ORL) as has been anticipated. 1 VR can simulate real-world scenarios and surgical procedures in a safe and controlled environment, which allows for valuable hands-on experience without the risk of injuring a patient. 2 Especially in complex anatomy such as the temporal bone, VR improves visualization, offers repeatable practice, and reduces the need of cadaveric models.
A major advantage of VR is that data can be shared, and models can evolve. An excellent example is “The Visible Ear,” a digital image library of the temporal bone. 3 It was the basis for “The Visual Ear Surgery Simulator,” 4 which has been used as a template for many other VR models. Once a suitable model has been created and evaluated, other ORL departments may integrate it into their residency curricula to establish a training standard.
However, VR is not an integral part of German residency programs in ORL yet. 1 To incorporate VR into the residency curriculum a multi-step approach is needed. After assessing the needs, researching VR technology, and developing an appropriate VR program, it must be piloted with a small group of residents. In this study, we investigated a VR model of the temporal bone in terms of utility and usability. The goal was to determine whether otolaryngologists learn the temporal bone anatomy better with VR than with a standard plastic model. Furthermore, we focused on whether VR improves anatomic knowledge and whether the improvement increases with the surgeon's experience.
Methods
Study design and ethical considerations
We performed a prospective randomized controlled trial, including an objective comparison, a pre-post evaluation, and a subjective comparison using a VR temporal bone model and plastic replica of the temporal bone. Participants were ORL residents and specialists of the university hospitals Freiburg and Heidelberg in Germany. The data were obtained between 2022 and 2023. Inclusion criteria were being a resident or specialist at a German ENT hospital and consenting to participate in this study. Exclusion criteria were refusal of consent to participate in this study.
Simple randomization was performed using computer-generated random numbers. This study was conducted according to the Declaration of Helsinki (Washington, 2002) and current national regulations. This study was approved by the ethics committee of the University of Freiburg (Number of ethics committee approval: 21_1343_1). Written informed consent was obtained from all participants. They were also informed about their rights according to current data protection regulations and gave written informed consent for the collection, analysis, and storage of their personal data. The trial is part of a larger study and has been registered at the German Clinical Trials Register (DRKS00025540). Parts of this larger study have been published by von Schnakenburg et al 5 The reporting of this study conforms to the SQUIRE-EDU ((Standards for QUality Improvement Reporting Excellence in Education)) publication guidelines 6 (the SQUIRE-EDU checklist is provided as a Supplementary File).
The VR temporal bone model “Human Ear”
The VR model was created to gain a better understanding of the temporal bone structures. It was custom-built by realworld one GmbH & Co. KG (Freiburg, Germany) under the instruction of the departments of anatomy, radiology, and ORL of the University and University Hospital Freiburg.5,7 The VR model was created from high-resolution CT data sets of the temporal bone which were provided by the radiology and anatomy departments. To create the 3D experiences of the human ear, the development platform Unreal Engine 4 (Epic Games Inc., Cary, USA) was used. Developers implemented the project-related functionalities using visual scripts. Models were created using 3DsMax and Maya (Autodesk Inc., San Francisco, USA) and anatomical objects were textured with Substance (Adobe Inc., San José, USA). It displays the middle ear and its surrounding structures: outer ear canal, tympanic membrane, ossicles and their ligaments, round and oval window, cochlea, vestibulum, facial and vestibulocochlear nerve as well as tendons and muscles of the middle ear (Figure 1.1). The model is virtually set up in a defined area of about 3 × 4 meters and can be enlarged to man height. Wearing a VR headset, users can walk through and enlarge structures and look at them from different angles and perspectives (Figure 2). This allows inspection of areas which are usually difficult to display in standard models, eg, the articulating surface of the ossicles. Also, one can “physically” follow the nerves (eg, facial nerve) through the bone. The latest version of the model is animated so that the sound transmission from the outer auditory canal through the tympanic membrane, ossicular chain, and inner ear are visualized. The aim of this design was to comprehend the anatomical relationships between structures (eg, the course of the chorda tympani in relation to the tympanic membrane) and in subsequent versions surgical approaches (eg, posterior tympanotomy), and functional concepts (eg sound transmission).

Illustration of the VR model (1) and the standard plastic models (2) used in this study. This figure is a modification as published by von Schnakenburg et al. 5

Participating ORL resident using VR goggles to immerse into the temporal bone model.
Standard plastic models used as control
As control to the VR model, we used a commercially available plastic model of the temporal bone and a one-to-one replica of the temporal bone (Figure 1.2). The models could be partially disassembled to get a better view of the different structures. As with the VR model, the parts of the plastic models were not labeled.
Study procedure
Total study time per participant was approximately 90 min. First, all participants were given a 30-min lecture outlining the basic middle ear anatomy to achieve a common baseline knowledge. The participants were then randomized into 2 groups: Group A (study group) and Group B (control group). In a pretrial evaluation (Figure 3), participants were asked to rate their comprehension of the temporal bone anatomy on a scale from 1 (“very good”) to 5 (“very poor”). On the same scale, their previous experience with VR was estimated. Group A then had 10 min to answer the MCQ2 test, which was part of the before/after-VR evaluation. Subsequently, Group A had 10 min of training with the VR model. During the training, participants were “guided” by an instructor who pointed out the most important structures shown in the model. This guided instruction was standardized for all participants. Directly after the VR session, Group A had 10 min to answer the same MCQ2 again. Then they also answered MCQ1, which is part of the comparative study between VR and the standard plastic models (10 min). Afterwards, Group A also had a training session with the standard plastic models. For 10 min they could study the 2 models (Figure 1) and received a similar standardized explanation of the structures like the one during the VR session. Finally, Group A finished the study by answering the subjective evaluation. Group B took the same sessions and tests, but in a different order as outlined in Figure 3.
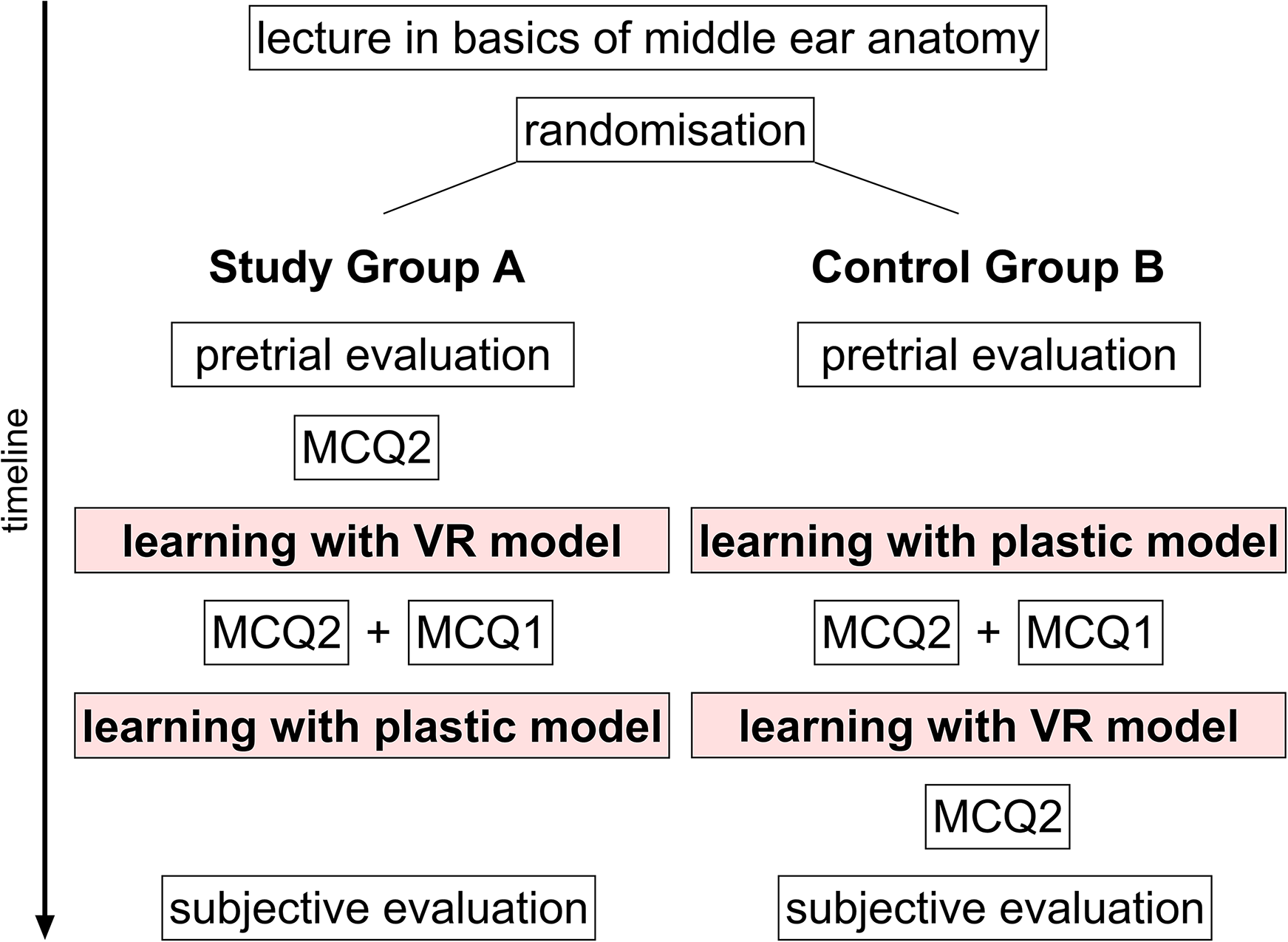
Layout of the study plan. MCQ, multiple-choice question test.
Objective evaluation
To assess objective learning outcomes, we used 2 multiple-choice questions (MCQ) tests on temporal bone anatomy. MCQ1, which was constructed by Schnakenburg et al 5 was completed by both groups to compare the learning effect after using the VR model or the plastic models (refer to Supplementary Appendix 1 for a sample of the MCQ1). To determine if the VR model improves the anatomical knowledge, all participants were given the MCQ2 before and after the VR session (refer to Supplementary Appendix 1 for a sample of the MCQ2). MCQ1 consisted of 10 questions, allowing a maximum test score of 10, whereas MCQ2 consisted of 7 questions, allowing a maximum test score of 7 points.
Subjective evaluation
For subjective evaluation of the VR models in comparison to the plastic models, participants were asked to evaluate 11 statements about learning experience, usefulness, advantages, and disadvantages of the different models (statements are shown in Table 1). Participants could rate each statement using Likert scales ranging from 1 (“strongly agree”) to 5 (“strongly disagree”).
Subjective evaluation of the VR model and standard plastic models. The Likert scale score ranges from 1 (“strongly agree”) to 5 (“strongly disagree”).

SEM, standard error of the mean.
Statistical analysis
Data were analyzed using statistical software (GraphPad Prism 9© 2022, GraphPad Software). First, normal distribution was tested using the Shapiro-Wilk test, because it is an appropriate normality test for small sample size as seen in this study. Normally distributed data were assessed with t-tests, and nonparametric data were assessed with a Wilcoxon test. Statistical significance was set to P < .05. When necessary, data were paired, such as in the before/after comparison. Descriptive analysis included calculation of the mean and its range as the standard error of the mean.
Results
21 ORL residents and 17 ORL specialists participated in this study. Group A included 10 residents and 10 specialists, whereas Group B had 11 residents and 7 specialists. ORL residents were in Years 1-5 of their training. The average level of training of participating residents were 2.0 years in Group A and 2.2 years in Group B. Specialists were not specifically trained in otology. In the pretrial evaluation all respondents rated their knowledge of the temporal bone anatomy on a “medium” level (Likert scale score for residents was 3.1 ± 0.2 and for specialists 2.95 ± 0.2) and stated that their experience with VR before this study was “low” (Likert scale score for residents and specialists was 4.18 ± 0.14 and 4.21 ± 0.2, respectively).
Objective evaluation: VR versus plastic model
There was no statistically significant difference of test performance after learning with the VR or plastic model between the VR model and the plastic model (6.8 vs 6.9 points, P = .75) (Figure 4). When considered separately, specialists scored slightly higher than residents, but overall, there was no difference between the 2 groups.
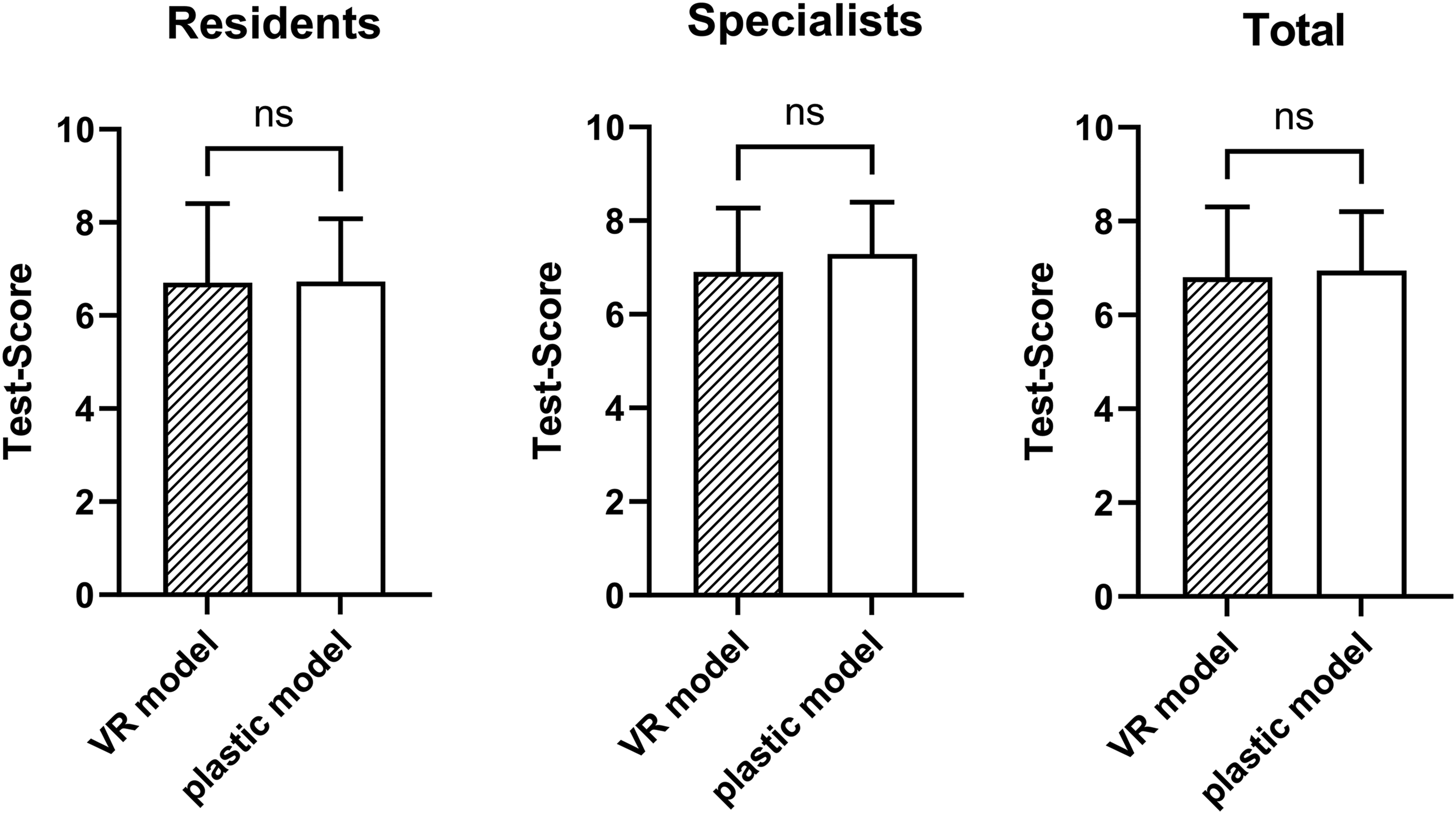
There was no significant difference in anatomy test performance of residents and specialists after learning with VR versus learning with the standard plastic model.
Objective evaluation: before and after using VR
In Group A, residents could not improve their MCQ2 results through the VR session (P > .99). On the other hand, specialists performed much better after using VR (P = .012). We saw different results in Group B, whose participants received teaching on the standard plastic model in advance of the VR session. In Group B both residents and specialists showed a statistically significant improvement using the VR (residents: P = .038; specialists P = .031), which was even more distinct when specialists and residents were analyzed together (P = .001) (Figure 5).

In the before/after learning with VR analysis, residents did not significantly improve their anatomical knowledge through learning with VR in Group A (only VR usage), but in Group B (first plastic model, then VR). Specialists significantly improved through VR in both groups. In total there was no improvement in Group A, but a highly significant improvement through VR if participants had used the plastic model beforehand (Group B). *P < .05; ***P < .001.
Subjective evaluation
According to the participants, VR is superior to the plastic models in visualizing temporal bone anatomy (Table 1). They agreed or strongly agreed that VR offers a whole new learning experience and gives a deeper understanding of anatomy, physiology, and pathology. Most participants thought VR was an effective tool to teach complex anatomy and would like to have more innovative teaching methods during residency training. When asked if VR was merely a “gadget” the majority disagreed (Table 1).
At the beginning of the study, participants indicated that they had not yet been exposed to VR during their residency, but their impression of VR changed over the course of the study. After the study, they agreed to a much greater extent that VR is a useful tool to otolaryngology residency training (Likert scale score before = 1.75 vs after = 1.25, P = .004).
Discussion
VR is a teaching method is at least equal to standard plastic models
Our results show no statistically significant difference between the knowledge gained with anatomical training with conventional plastic models of the temporal bone and the VR model. These results are consistent with studies conducted on medical students by Schnakenburg et al, 5 who also did not see a statistical difference in anatomy test performance after using a VR model or a standard plastic model. Nevertheless, the training with VR seems to be as effective as training with conventional plastic models. Also, participants rated learning with VR technology significantly better than plastic models. In contrast to VR, plastic models’ anatomical accuracy can be limited, they are unable to simulate physiological responses or complications of surgery, they lack interactivity, they potentially degrade over time, and they need to be physically stored. VR on the other hand, is just beginning to evolve as an educational tool and its potential for optimization is promising.5,8 With VR, complex organ structures can be magnified and visually disassembled to understand their functional units. 9 The user can rotate their viewpoint around the object and repeat the training indefinitely which augments the training effect. 10 Although not used in this model, VR can provide labels, additional information and allow interaction with the viewer.8,11 In 2023 Shin et al introduced a photorealistic VR model of the middle ear, which was tested by ORL residents and showed high content and face validity. 11 Overall, VR education provides ORL physicians with a highly effective learning experience that is at least equally effective as physical models and can be adapted and continuously improved, which cannot be achieved with plastic models.
VR is more effective when the prior anatomical knowledge is higher
When testing the temporal bone anatomy before and after VR, specialists improved more in comparison to residents. Also, participants who went through a teaching on the standard plastic model before VR, performed significantly better than those who did not get this prior tuition. This effect was also seen in Shin et al's study on the photorealistic VR middle ear, where senior residents had a higher comfort level with middle ear anatomy than younger residents. 11 Younger residents may have been overwhelmed with the VR experience. The anatomical structures in the VR model are not yet labeled and parts cannot be taken apart, making orientation difficult for inexperienced residents. However, repetitive VR sessions could help to focus better on the anatomical structures and overcome this effect of being overwhelmed. It seems comprehensible, that a certain level of knowledge is required to be able to fully utilize the full potential of the VR model to improve anatomical knowledge. Therefore, VR could be more beneficial at advanced stages of residency training but could also help inexperienced residents if VR training was offered to them repeatedly. Also, our results suggest that a combination of VR and standard teaching models are the most advantageous.
VR is not yet incorporated into ORL residency training but can be very beneficial
Although there are several well-evaluated VR simulators available,12–16 these devices are not yet incorporated into the ORL residency curriculum.17,18 This might be because of low validation, 18 inadequate equipment or resources, resident time constraints and lack of faculty participation. 19 As suggested by Offergeld et al resistance to change may also slow down the process of improving digital and virtual teaching. 20 Our participants confirmed that they had little to no experience with VR prior to this study. However, after completing the VR program, they indicated that it was a very effective tool for teaching complex anatomy such as the temporal bone. Precise knowledge of the anatomy and its function is particularly important in middle ear surgery, as a small error can have major consequences. Improved anatomical knowledge in combination with surgical simulation-based training during ORL residency could improve patient's outcome.
Limitations of the Study
One limitation of the study is that the full potential of the VR model could not be used yet as the model did not have functional components and could not be disassembled. This limitation may have impacted the depth of understanding of anatomical relationships and structures. Future studies with more advanced VR models may provide a clearer picture of the technology's benefits.
Because the sample size, respectively, the number of participants in the study, is limited, a power analysis was not performed. A larger sample would improve the reliability and generalizability of the results. The relatively small sample of participants may not represent the full range of experiences and preferences of ORL residents and specialists. In future studies, a multi-center (more than 2) analysis can overcome this issue.
Because this is a pilot study, the questionnaires MCQ1 and MCQ2 have not been scientifically validated although MCQ1 has been used in a different pilot study conducted by Schnakenburg et al 5 In future larger studies adapted standard questionnaire could be more precise.
The study focuses on ORL residency training in German university hospitals. The results may not be directly transferable to other medical specialties or residency programs with different training structures and requirements. Consideration of these factors is essential for transferring the results to a broader context.
The results provide information on the immediate learning outcomes following VR training. However, the long-term retention of knowledge and skills acquired through this VR model remains unclear. A follow-up study examining knowledge over a longer period of time would provide a more comprehensive understanding of the effectiveness of the technology.
Conclusion
In conclusion, the study demonstrates that VR models for temporal bone anatomy in ORL residency training are not only engaging and well received by residents but also effectively enhance anatomical knowledge, particularly among more experienced surgeons. Although VR training does not show superiority over traditional plastic models in terms of objective knowledge gains, it offers distinct advantages such as improved visualization, repeatable practice, promoting collaboration and interactivity, which can be continuously optimized. The study suggests that incorporating VR into ORL training, especially in combination with conventional methods, could significantly benefit surgical education by providing a deeper understanding of complex anatomical structures. However, broader validation, enhanced model functionalities, and larger sample sizes are needed to fully realize VR's potential in medical education. Further developments are already in progress and upcoming studies—like long-term follow-ups—look promising.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241281506 - Supplemental material for A Virtual Reality Anatomy Model of the Temporal Bone in ORL Residency Training—Gain or Gadget?
Supplemental material, sj-docx-1-mde-10.1177_23821205241281506 for A Virtual Reality Anatomy Model of the Temporal Bone in ORL Residency Training—Gain or Gadget? by Friederike Everad, Tobias Albrecht, Jan Kromeier, Stephan Heermann, Philip von Schnakenburg, Tanja Hildenbrand, Iva Speck, Andreas Knopf and Christian Offergeld in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241281506 - Supplemental material for A Virtual Reality Anatomy Model of the Temporal Bone in ORL Residency Training—Gain or Gadget?
Supplemental material, sj-docx-2-mde-10.1177_23821205241281506 for A Virtual Reality Anatomy Model of the Temporal Bone in ORL Residency Training—Gain or Gadget? by Friederike Everad, Tobias Albrecht, Jan Kromeier, Stephan Heermann, Philip von Schnakenburg, Tanja Hildenbrand, Iva Speck, Andreas Knopf and Christian Offergeld in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241281506 - Supplemental material for A Virtual Reality Anatomy Model of the Temporal Bone in ORL Residency Training—Gain or Gadget?
Supplemental material, sj-docx-3-mde-10.1177_23821205241281506 for A Virtual Reality Anatomy Model of the Temporal Bone in ORL Residency Training—Gain or Gadget? by Friederike Everad, Tobias Albrecht, Jan Kromeier, Stephan Heermann, Philip von Schnakenburg, Tanja Hildenbrand, Iva Speck, Andreas Knopf and Christian Offergeld in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to thank realworld one GmbH & Co. KG and in particular Dr Corvin Walter for their cooperation in creating the VR model that made this research project possible. We would also like to acknowledge the support by the Open Access Publication Fund of the University of Freiburg.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
FE helped conceptualize the study, designed the study schedule, collected, analyzed and interpreted the data, and drafted the manuscript. TA helped in data collection and revised the manuscript. JK and SH helped in creating the virtual reality temporal bone model. PvS helped in data collection. TH, IS, and AK revised the manuscript. CO conceptualized the study and the virtual reality temporal bone model, helped in designing the study schedule, helped in interpreting data, and substantially revised the manuscript.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted according to the Declaration of Helsinki (Washington, 2002) and current national regulations. This study was approved by the ethics committee of the University of Freiburg (Approval No.: 21_1343_1). Written informed consent for participation was obtained from all participants.
Consent for Publication
Participants were informed about their rights according to current data protection regulations in written form and gave written informed consent for the collection, analysis, storage, and publication of their personal data. Written informed consent for publication was given by 1 participant, whose image is shown in this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.