
Abstract
OBJECTIVE
Triage is the key to success in managing many injured people with limited resources. Therefore, triage training for crisis team medical staff is critical. This study aimed to evaluate the effectiveness of asynchronous learning on immediate care personnel based on the Simple Triage and Quick Treatment System (START) triage system.
METHODS
In this quasi-experimental study, asynchronous learning based on the START triage system was performed on the immediate care staff of Ahvaz Jundishapur University of Medical Sciences from February 2021 to December 2021. Sixty pre-hospital emergency medical staff were randomly assigned to intervention and control groups. Intervention group participants were provided an asynchronous digital training module, and control group participants received the usual training. Data were collected in both groups as pre-test and post-test with demographic information and knowledge assessment questionnaires.
RESULTS
Distance triage training based on the START triage system has a significant effect on the level of awareness of the need for triage and knowledge (awareness) and performance (individual efficiency) of immediate care in the intervention group compared to before training (P < 0.001).
CONCLUSION
Considering the positive results of the pre-organizing model on raising the level of awareness of immediate care personnel, the use of this training method in triage in emergency medicine and retraining workshops could be considered.
Introduction
Triage is a prioritization system for manageable hospital admissions in each hospital's department, which, by managing allocation, resources, and facilities needed, leads to patient care in the minimum waiting time.1,2 The concept of triage was initially created to allocate resources and medical care in cases of disasters and accidents with mass casualties. Because of the overcrowding in the emergency department due to limited resources available, including human resources, space, and equipment, decreased quality of care and patient safety. Increased costs of care today, in developed countries, hospital triage guidelines have been considered to reduce the rate of care and treatment errors and improve patient quality and safety. 3 There are two subsets of triage, including hospital triage and pre-hospital triage. 4 One of the most widely accepted and used triage systems for disaster management is the Simple Triage and Quick Treatment System (START), first introduced in the United States in the 1980s. 5 As a result of the simplicity of the START system, it is quick and easy to learn; however, like other fast triage protocols, it has some limitations, such as negligence in the mechanism of injury, limited evaluation, and lack of monitoring of patients with mild or moderate injury whose transmission is delayed. 6 As a developing country, Iran has constantly been exposed to disasters in recent years. 7 Solutions needed to solve problems related to these disasters include preparedness and planning, the use of advanced systems, accountability policy, a successful scientific and executive program, adequate emergency and trained resources, and skilled staff. 8 Like other triage systems, running the START system requires adequate training and support. 9 Without proper training in this field, nurses cannot use triage correctly and follow the standards provided. Unquestionably, nurses play a crucial role in the patient's stay in the emergency department with their professional measures, including patient triage, and can effectively reduce this time. 10 Therefore, in parallel with implementing any triage system, training has also been considered in hospitals. In this regard, taking at least eight hours of theoretical and 24 h of practical triage training under the supervision of an experienced nurse is emphasized. 11
This study aimed to evaluate the effectiveness of asynchronous learning based on the START triage system on immediate care personnel of Ahvaz Jundishapur University of Medical Sciences, southwestern Iran.
Methods
In this quasi-experimental intervention study, asynchronous learning based on the START triage system was performed on immediate care personnel of Ahvaz Jundishapur University of Medical Sciences from February 2021 to December 2021. EQUATOR reporting guideline was chosen based on the Equator network guideline (Supplemental 1).
Randomization and allocation methods
Based on a similar study and comparing two groups formula (Formula 1), the sample size for each group was 30. Sixty pre-hospital emergency staff were randomly assigned to intervention and control groups.

Participants were selected from the emergency staff who participated. We excluded those who left the workshop and those who did not answer the pre-test or post-test questionnaires.
The subjects were randomly divided into two groups through random allocation software: intervention and non-intervention. In order to balance the number of samples assigned to each studied group, the four permuted block randomization was used.
In the same previous study, the education was carried out in a class, 6 whereas, in the present study, training materials were prepared in the form of videos and sent to all the members of the intervention group so that the participants could see the training in the best situation according to them. In this file, the primary education principles were based on improving the awareness and performance of staff in triage. Following the education, it was expected that the participants would show higher skills in patient management in triage. To understand this hypothesis, a multiple-choice question was provided. Before the intervention, the level of awareness and knowledge of the two groups were compared. Two weeks after sending the triage training file to intervention groups, both groups completed the questionnaire again, and the data of both groups were compared.
The questionnaire includes three parts: the first contains demographic information, the second contains 19 multiple-choice questions to measure awareness, and the third contains 15 multiple-choice questions to measure staff's decision-making (Supplemental 2). The validity of the questionnaire was checked by presenting it to 10 experts, and the Pearson correlation coefficient was 0.8. Its reliability was also evaluated during a study on the sample population, and its Cronbach's alpha coefficient was 0.88. Based on this, the total score of the awareness questionnaire was from 0–15; (0–5) little awareness, (6–10) moderate awareness, and (11–15) good awareness also about performance; the total score was from 0 to 19; (0–6) weak performance, (7–12) moderate performance, and (13–19) good performance. 12
Informed consent
The written informed consent was obtained from each participant.
Statistical analysis
For the descriptive analysis, frequency (percentage) was used for qualitative variables, and mean (standard deviation) was used for continuous quantitative variables. In order to compare the mean of a continuous quantitative variable, if there is an assumption of normality, we used the independent t-test. Otherwise, we used the Mann–Whitney test. To compare the mean of the continuous quantitative variable in two dependent groups, a paired t-test was conducted. The chi-square test of independence was conducted to check the independence between the intervention and the qualitative variables. Otherwise, Fisher's exact test was conducted. We used the analysis of variance test to control confounding variables. All analyses were performed with the help of R statistical programming software and at a significance level of 0.05.
Results
Overall, 121 emergency staff with an average age of 29.4 ± 3.6 participated in this study (Figure 1). The duration of employment in the immediate care department was 2.9 ± 0.2 years in the intervention group and 3.5 ± 0.5 years in the control group. There was no significant difference between the groups regarding duration of employment (p = 0.6).
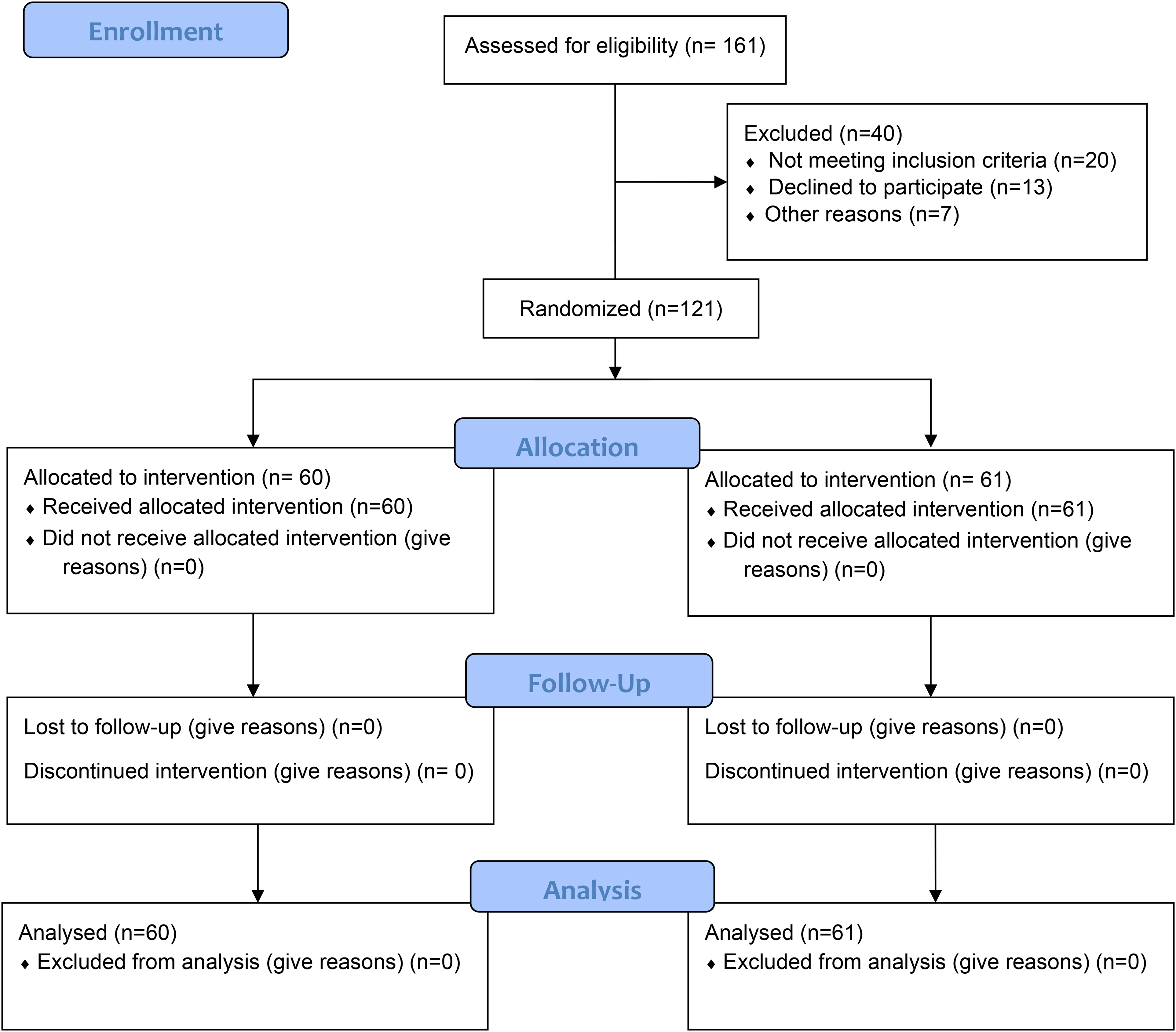
The overview of sampling and blocking participants.
The result showed that asynchronous learning triage training using the START triage system for immediate care personnel based on age does not have a significant effect on the evaluation of knowledge (awareness), performance (individual efficiency) (p = 0.08), and the level of awareness of the necessity of triage (p = 0.6) (Table 1). Also, asynchronous learning triage training using the START triage system on the immediate care personnel, based on the amount of work experience, does not have a significant effect on the evaluation of knowledge (awareness), performance (individual efficiency) (p = 0.1), and the awareness of triage necessity (p = 0.8) (Table 1).
The demographic information of included participants.

Pre-intervention analysis showed that there were no significant differences between the two groups for knowledge (p = 0.1) and awareness (p = 0.2) (Table 2).
Comparing the pre-intervention mean level of knowledge and awareness in participants.
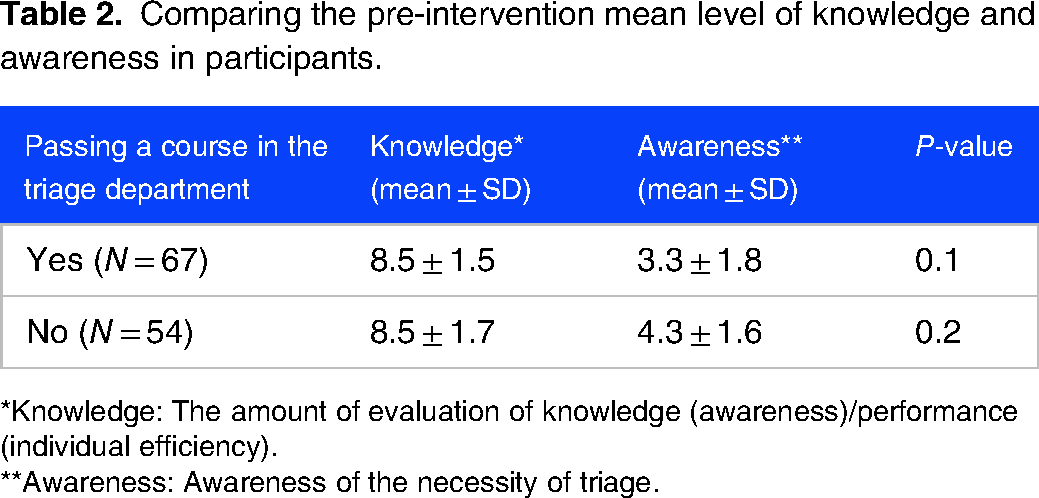
*Knowledge: The amount of evaluation of knowledge (awareness)/performance (individual efficiency).
**Awareness: Awareness of the necessity of triage.
Asynchronous learning triage training based on the START triage system for immediate care personnel has a significant effect on the level of awareness of the necessity of triage in the intervention group after the training compared to before the training (p < 0.001) (Table 3). The analysis showed that the asynchronous learning triage training based on the START triage system on the immediate care personnel has a significant effect on the knowledge (awareness) and performance (individual efficiency) of the immediate care personnel in the intervention group after the training compared to before the training (p < 0.001) (Table 3).
Evaluation the efficacy of education on knowledge and awareness between two groups.

*Knowledge: The amount of evaluation of knowledge (awareness) and performance (individual efficiency).
**Awareness: Awareness of the necessity of triage.
Discussion
The results showed that the asynchronous learning triage training based on the START triage system on the immediate care personnel on the level of awareness of the necessity of triage and the knowledge (awareness) and performance (individual efficiency) has a significant effect before training compared to the intervention group after the training. In 2017, Pouraghaei et al 6 conducted an interventional study to assess the effect of triage training using the START method on the knowledge and performance of emergency medical technicians. They found that holding pre-hospital triage training courses is effective in improving the knowledge and performance of employees such as Emergency Medical Services technicians. 6 Their finding was in line with the results of the present study, which showed that the asynchronous learning training of triage based on the START system for the immediate care personnel has a significant effect on the level of awareness of the necessity of triage and the knowledge (awareness) and performance (individual efficiency). In line with this finding, Mansour et al 13 conducted a study to determine the effect of implementing triage training competencies on newly graduated nurses working in the emergency department. They found a high statistical significance difference between the study group and control group in terms of knowledge and practice in the post and 2-month post-program implementation. 13 In 2016, Mahmoodian et al, 14 in a cross-sectional study on all the senior students of medicine, their results showed that 58 students (93.5%) had poor triage knowledge. In the scenario section, the correct triage percentage of students was 49.2%, and people over and under triage were 28.1% and 22.7%, respectively. There was a significant relationship between triage accuracy and triage level (Emergency Service Index 4). 14
In this study, considering the positive results of the pre-organizer model on raising the level of awareness of immediate care personnel, it is recommended to use this training method in presenting the subject of triage during the crisis in nursing schools and retraining workshops. In 2013, Rahmati et al 15 conducted a semi-interventional study on the effect of triage training on the knowledge, performance, and quality index of emergency department staff. Their results showed no significant relationship between individual characteristics and personal knowledge about the triage score 6 weeks after training. Nevertheless, a positive and significant correlation was found between nursing work experience in the emergency department, type of employment, and performance score 6 weeks after the training. The results of the study showed that triage training affects the performance and knowledge of nurses and improves the quality indicators of the emergency department, 15 which is in line with the results of the present study. In this study, both pieces of training were practical and based on personnel knowledge and performance. Aghababayan et al 12 conducted an interventional study on the effect of triage video training through the START style on the level of awareness of emergency medical workers and their performance. They showed that average awareness and performance also have a significant statistical relationship. Also, there was a statistically significant difference between the average knowledge and performance immediately after and 15 days after the training. 12 In 2012, Sedaghat et al 16 showed poor mean triage knowledge score and performance triage. In the present study, it was also shown that the asynchronous learning training of triage based on the START triage system on the level of awareness of the necessity of triage and the knowledge (awareness) and performance (individual efficiency) of the immediate care personnel on the intervention group has a significant effect after training compared to before training. Javadi et al 17 conducted a systematic review of educational intervention studies and found that almost all studies reported an educational intervention's effectiveness in improving nurses’ triage knowledge.
According to the studies compared with our findings, it was found that at the current level of triage education in our system, more educational intervention is highly required. As mentioned earlier, this short education period upgrades the knowledge and performance of medical staff. Our results indicated that our education influences the medical staff's performance (individual efficiency). It means that this type, of course, is accompanied by significant improvement in staff performance. Additionally, this course is not affected by age and amount of work experience. However, our data could not show that this training is suitable for the maximum amount of personnel experience.
Limitations
Lack of data regarding the minimum required length of education, the staff situation, such as mental and physical states, and level of job satisfaction are disrupting factors that can potentially influence the interpretation of findings.
Recommendations
To check the findings of the present study, other studies should be conducted in the immediate care rooms of other cities. Conducting other research to investigate the effectiveness of face-to-face training compared to non-face-to-face triage training based on the START triage system on immediate care personnel of Ahvaz Jundishapur University of Medical Sciences. Conducting other research to investigate the effect of training on the effectiveness of triage training based on the START triage system on immediate care personnel with a larger sample size.
Conclusion
Considering the positive results of the pre-organizer model, which was not previously educated on improving the level of awareness of immediate care personnel, it is recommended to use this training method in presenting the subject of triage in medical emergency and retraining workshops.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241278658 - Supplemental material for Effectiveness of Distance Training Based on Simple Triage and Quick Treatment System (START) Triage System in Pre-Hospital Emergency
Supplemental material, sj-docx-1-mde-10.1177_23821205241278658 for Effectiveness of Distance Training Based on Simple Triage and Quick Treatment System (START) Triage System in Pre-Hospital Emergency by Mofid Hosseinzadeh, Ali-Vafagh Nematollahi, Yasin Afra, Payam Amini and Alireza Rafati Navaei in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241278658 - Supplemental material for Effectiveness of Distance Training Based on Simple Triage and Quick Treatment System (START) Triage System in Pre-Hospital Emergency
Supplemental material, sj-docx-2-mde-10.1177_23821205241278658 for Effectiveness of Distance Training Based on Simple Triage and Quick Treatment System (START) Triage System in Pre-Hospital Emergency by Mofid Hosseinzadeh, Ali-Vafagh Nematollahi, Yasin Afra, Payam Amini and Alireza Rafati Navaei in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
This work has been provided by the credit of the approved MD for this thesis and research project no U-U-00039 at Ahvaz Jundishapur University of Medical Sciences. We wish to thank all our colleagues at Allied Health Sciences School, Ahvaz Jundishapur University of Medical Sciences.
Author contributions
ARN, MM, and MH designed the study, analyzed the original survey data, and created the first draft manuscript. AM and ARN reviewed the data interpretation from the original studies and contributed to manuscript revisions.
Availability of data and materials
All data are presented in the paper.
Ethics approval
This article is based on the MD thesis and research project no. U-00039 at Ahvaz Jundishapur University of Medical Sciences and approved by the Ethics Committee affiliated with the Ahvaz Jundishapur University of Medical Science.
Consent for publication
Informed consent have obtained from the subjects prior to study initiation.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.