
Abstract
OBJECTIVE
In the United States, physicians and residents report inadequate training in managing adolescents and young adults (AYAs) during the transition from pediatric to adult care, particularly AYAs with chronic illnesses such as sickle cell disease (SCD). We developed an intervention where medical students serve as similar-aged “peer” mentors to offer informational and developmentally appropriate support to AYA patients during the period of transition. Our initial work showed the feasibility and acceptability of this intervention for young adults with SCD. In this report, we evaluate the feasibility, acceptability, and preliminary effects of this non-randomized trial on medical student mentors.
METHODS
Following training, medical student mentors were paired 1:1 with an AYA with SCD who was transitioning from pediatric to adult care. They conducted monthly video calls with mentees to address specific transition and disease self-management topics. Students completed baseline and follow-up surveys regarding knowledge of SCD and empathy. Satisfaction was measured at follow-up via survey and an exit interview.
RESULTS
Nine medical students were paired with a total of 24 patients. Student retention was 100%, but only eight completed the follow-up survey. Students reported increased knowledge about managing a chronic illness and transition and improved understanding about the patient's experience navigating the healthcare system. Students expressed high satisfaction.
CONCLUSIONS
A medical student mentor intervention was feasible and acceptable to medical students and may provide an opportunity for value-added role in medical education. Further research is needed to evaluate the efficacy of this type of intervention on both student and patient outcomes.
Introduction
In the United States, nearly 750 000 adolescents and young adults (AYA) with special healthcare needs and chronic illnesses (eg sickle cell disease, cystic fibrosis, juvenile arthritis) make the transition from pediatric to adult healthcare each year. 1 Transition is a multi-component process that includes the medical, psychosocial, and educational/vocational needs of AYAs. To address these complexities, relevant medical organizations, including the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians, have created consensus statements and clinical practice guidelines illustrating best practices in transition care. They have highlighted the need to educate physicians about transition care, disease processes of pediatric-onset chronic illnesses, and behavioral stages of development. 2 Physicians report inadequate training in dealing with chronic illness, 3 and pediatric and internal medicine residents specifically report a lack of training on managing young adults with chronic illness during the transition from pediatric to adult care. 4 Thus, strategies for educating medical students about medical and psychosocial complexities of chronic illness throughout the lifespan are needed.
In 2016, the American Medical Association (AMA) consortium investigated value-added roles for medical students, or roles that were “experiential and authentic, and have the potential for a positive impact on outcomes related to patients… and enhance student knowledge, attitudes, and skills.” 5 One of the recommendations for student opportunities included medical students acting as patient navigators, health coaches, or health care transition facilitators. 5 Longitudinal patient partnerships have been recommended as they allow students to cultivate a greater understanding of the broader context in which patients experience illness and improve their patient communication skills. 6 Serving as a patient mentor may offer a medical student the opportunity to develop a longitudinal patient relationship, improve communication skills, and become more culturally aware of patient experiences. 7
Peer mentoring and coaching can have many benefits, including harnessing social support to improve the quality of life of AYA with chronic illnesses. 8 Medical students have been utilized as peer mentors for AYA patients with chronic conditions and healthy adolescents to promote positive health behavior changes.7,9–12 Due to medical students being familiar with the healthcare system, they may be able to offer a unique perspective on the process of transition from the pediatric to the adult healthcare system.
Sickle Cell Disease (SCD) is a common genetic disease that may cause painful vaso-occlusion crises, organ damage and failure, and chronic pain. 13 Children with SCD are able to receive comprehensive, coordinated care from their pediatric hematologist, including prescriptions for pain medication, hydroxyurea, iron chelation, and preventive screenings. Adolescents and young adults with SCD have reported challenges during the transition to adult healthcare, where their medical care is typically more fragmented, requiring separate visits to multiple specialties to receive their care.14,15 Some of the barriers to successful transition include disease self-management, lack of knowledge about their disease, negative attitudes from adult care providers and other medical staff, and proper introduction to an adult care provider. 15 Within the existing literature, there is a clear need for evidence-based programs for transition care among adolescents and young adults with SCD. To develop a transition intervention that would address barriers to care and patient needs, our team conducted a qualitative needs assessment of AYA patients with SCD who were preparing to transition or who had recently transitioned to adult care. 16 Results indicated an interest in a longitudinal mentoring relationship with a medical student to help the patient navigate the transition as well as offer an opportunity to share the experience of a chronic health condition with a future physician. Medical students may serve as a similar-aged “peer” to offer informational and developmentally appropriate social support to these patients. An intervention pairing medical students with young adults who have a chronic illness may create a value-based role for medical students and may provide dual benefit for both medical student learning and patient outcomes.
We developed a medical student mentoring intervention that consisted of six-monthly video calls between a medical student mentor and patient mentee to discuss transition topics. We found the intervention to be feasible and acceptable to patients, providing promising results that such an intervention could address a gap in healthcare transition services for AYA patients with SCD. 10 Yet it is important to also understand any impact on the medical student mentors. The goal of this study is to examine the preliminary outcomes of the intervention on the medical student mentors to identify if this type of mentoring role might be considered a “value-added role” that could improve medical student understanding of the patient experience and patient communication skills. We hypothesized that medical student mentors would find the training educational and be satisfied with their experience of mentoring a patient. We explored whether participation would improve their knowledge of SCD and increase their empathy towards patients with chronic illness.
Methods
Study design
This study was a non-randomized single-arm feasibility trial using mixed quantitative and qualitative outcomes pre- and post-intervention. This research was approved by Rutgers Biomedical and Health Sciences Institutional Review Board (IRB # Pro2018001531).
Overview of program
The mentor program consisted of monthly medical student mentor video calls using a HIPAA-compliant videoconference system, supplemented by weekly text messages using an encrypted text messaging service. Each month, the mentors addressed specific content related to transition (Table 1).
Content for monthly video calls medical student mentors discussed with their assigned mentees.

Patients were recruited during routine visits at a pediatric or adult hematology clinic. Patients were eligible if they had sickle cell disease, were at least 18 years of age, and were either preparing for transition to adult care within the next two years (per pediatric clinical team) or had transferred to adult care within the past year. Patients were ineligible if they had documented or self-reported cognitive deficits or were unable to speak English. Patients were matched 1:1 with a medical student mentor, who could have from one to three mentees at a given time. Medical student mentors made initial contact via secure text message to set up a time to video chat. The objective of the first video call was to establish rapport and discuss the mentee's biggest challenges with regards to transition. During subsequent calls, they discussed one of the planned content topics (Table 1). Video calls ranged from 20 min to one hour. Mentors also sent text messages to their mentees at least once a week to answer questions and offer brief encouragement and support.
Medical student recruitment
Medical student recruitment took place at the Robert Wood Johnson Medical School in New Brunswick, New Jersey in 2018–2019. The recruitment procedures followed guidelines from the National Mentoring Research Center. 17 An email was sent to the entire student body describing the program and the application process. The mentor program was offered as a non-credit elective, defined as specific training in a topic spanning one to two years of participation. Successful completion of non-credit electives is included on students’ transcripts. To be eligible to participate as a mentor, candidates needed to be a current medical student in good standing (who had passed the required University background check for enrollment) and be between the ages of 21 and 29 years old. Interested students had to complete an application, including two letters of recommendation, and be interviewed to evaluate their interpersonal skills, level of commitment to the program, and counseling or related experience. There were no additional exclusion criteria. Recruitment occurred from November 2018 through May 2019 to meet the needs of mentee recruitment. In January 2019, seven medical students were interviewed and accepted into the program. Due to an increase in patient recruitment, two additional medical students were recruited in May 2019.
Procedures
Mentors provided written informed consent prior to engaging in any study activities. Mentors attended a four-hour training workshop, which included education on the content for the monthly telephone calls, expectations for the program, ethics, and role-playing with constructive feedback (Supplemental File 1 shows a sample agenda for a training). Clinical providers (pediatric hematologist, pediatric nurse practitioner, and adult hematologist) provided education about sickle cell disease and answered questions. A patient advisory board, comprised of four patients who had already transitioned to adult care, participated in a panel discussion with the medical students. Ethical issues, including confidentiality and setting appropriate boundaries with mentees, were discussed. Mentors were told that they were not allowed to provide medical advice to their mentees and that they should not set up in-person meetings with their mentees outside of the clinical setting. Mentors were also provided with a handbook that contained the information presented in the training (ie, program goals/expectations, strategies for effective mentoring, structure of monthly calls) and resources to use with mentees during their monthly calls. Medical student knowledge of SCD was assessed immediately prior to and following the training.
Mentors attended monthly group supervision meetings to discuss with one another and a clinical expert any challenges that arose related to their role as a mentor. If a mentor was unable to attend the group session, then an individual supervision was scheduled. Mentors reported the number of times and the method of communication they used with their mentee over the previous month. Additionally, mentors were encouraged to contact the research staff and clinical team throughout the month with any questions.
Mentors audio-recorded their video calls with their mentees (with patient consent) for use for fidelity checks, supervision, and content analysis. Each monthly education session had a corresponding checklist of items enumerating topics to be covered. For the first mentee-pairing for each mentor, the first of the six education calls were reviewed, as well as 20% of the remaining calls for the pairing (approximately 1 additional call). Mentor feedback was provided on (at least) a monthly basis.
Measures
Demographics
Mentors reported their demographic characteristics (eg, age, potential medical specialty, ethnicity) in the baseline survey.
Knowledge of sickle cell disease
Knowledge of SCD was measured using the validated 24-item Transition Knowledge Questionnaire adapted from prior research. 18 Items assessed knowledge of the pathophysiology, genetics, physical manifestations, treatment, self-care, psychosocial and developmental issues, and healthcare system relevant to SCD. The percentage of total correct items was calculated, with higher scores indicating higher knowledge. Mentors completed this questionnaire at baseline and at the end of the training workshop. In this sample, the measure demonstrated adequate internal consistency (α = 0.81).
Attitudes towards chronic illness
The 21-item Attitudes Towards Chronic Illness measure19,20 assessed students’ perceived comfort in managing chronic illness (eg, how comfortable or uncomfortable do you think you feel with dealing with inability to cure patients?), perception of patients’ attitudes (eg Please indicate the degree to which you agree or disagree with the following statements: it's important for patients to understand the specific mechanisms of their illness); and personal interest in patients (eg, How comfortable or uncomfortable do you think you feel with long-term professional relationships with patients?). In the prior validation study, 19 there was no consistent factor structure, and therefore, following the guide of the initial study, the items were reviewed individually to evaluate change. Mentors completed at baseline and post-intervention.
Satisfaction and perceived impact
Mentor satisfaction items were adapted from Ritterband and colleagues internet intervention utility and impact questionnaires. 21 Fourteen items were rated using a scale of 1 (not at all) to 5 (very much) to assess the perceived utility, impact, and adherence to the intervention at post-intervention. 21 Three open-ended items were added to asses mentors’ favorite part of the program, the extent to which they changed because of their participation in the program, and what they would change about the program. Brief semi-structured exit interviews were also conducted to obtain qualitative feedback on the intervention.
Mentor–Mentee relationship
For each mentor–mentee pair, both members of the pair completed a modified version of the validated Working Alliance Inventory-Short Form Revised, 22 to evaluate the quality and strength of their relationship at post-intervention. The inventory is comprised of ten items in three domains: agreement about tasks (3 items, eg, We agree about the steps to be taken to improve his/her transition), agreement about goals (3 items, eg, We are working towards mutually agreed upon goals), and development of a bond (4 items, eg, I appreciate my mentee as a person). In this sample, all subscales demonstrated high internal consistency (ie, task, α = 0.90; goals, α = 0.83; and bond, α = 0.90). Supplemental File 2 contains a copy of the survey items administered and the exit interview guide.
Sample size justification
The sample size for this feasibility study was based on the primary aim of determining feasibility and acceptability among patients with SCD and medical student mentors. A sample size of 20–25 patients was deemed appropriate for evaluating feasibility aims in a single arm study among patients.16,23 Given that we expected medical student mentors to work with between 2 and 3 mentees each, we anticipated needing 8–10 students in total to work with 20–25 patients in this single arm feasibility study.
Analyses
Quantitative data analyses consisted of descriptive and inferential statistical analyses using SPSS version 26. Descriptive analyses (means, standard deviations, frequencies) summarized the characteristics of the study sample. Mentor satisfaction was assessed using descriptive statistics (mean ratings, standard deviations, frequencies) of overall satisfaction with the program, satisfaction with the mentor training content and materials, and satisfaction with the program duration and format. Descriptive statistics were also used to describe the mentors’ perceived impact of the program and their relationships with mentees. The mean and standard deviation for each subscale of working alliance (goal, task, and bond) was calculated for the mentor and patient sample. Dependent samples or paired t-tests were used to evaluate changes in mentors’ SCD knowledge and attitudes towards chronic illness from pre- to post-intervention. The data generally met assumptions for dependent t-tests, with the exception of a single outlier in the comfort in managing chronic illness items. That individual was excluded from that analysis only (See Supplemental File S3, Table 1). Given the small planned sample size, Cohen's d measure of effect size was used to describe the magnitude of the differences in the means between the two time points. An effect size of 0.2 was considered small, 0.5 was considered medium, and 0.8 was considered large. 24
Thematic analysis of the qualitative open-ended responses and exit interview response data was conducted following the content analysis approach described by Pope and colleagues. 25 This approach generally involves five steps: familiarization of the raw transcript data, identifying a thematic framework (ie, identifying all key issues), indexing (ie, applying themes to the data), charting (ie rearranging data according to themes), and mapping and interpretation (ie, mapping associations and explaining findings). 25 In this study, at least two members of the research team read the material and identified themes in the data within the questions posed, such as what was their favorite aspect of the program, what could be improved, whether participation in the program impacted them personally, and their feedback on the mentor training, intervention content topics, and format. For each theme identified, we report the number of mentors who described it. No formal inter-rater analyses were conducted; any disagreements were resolved through discussion.
Results
Medical student participants
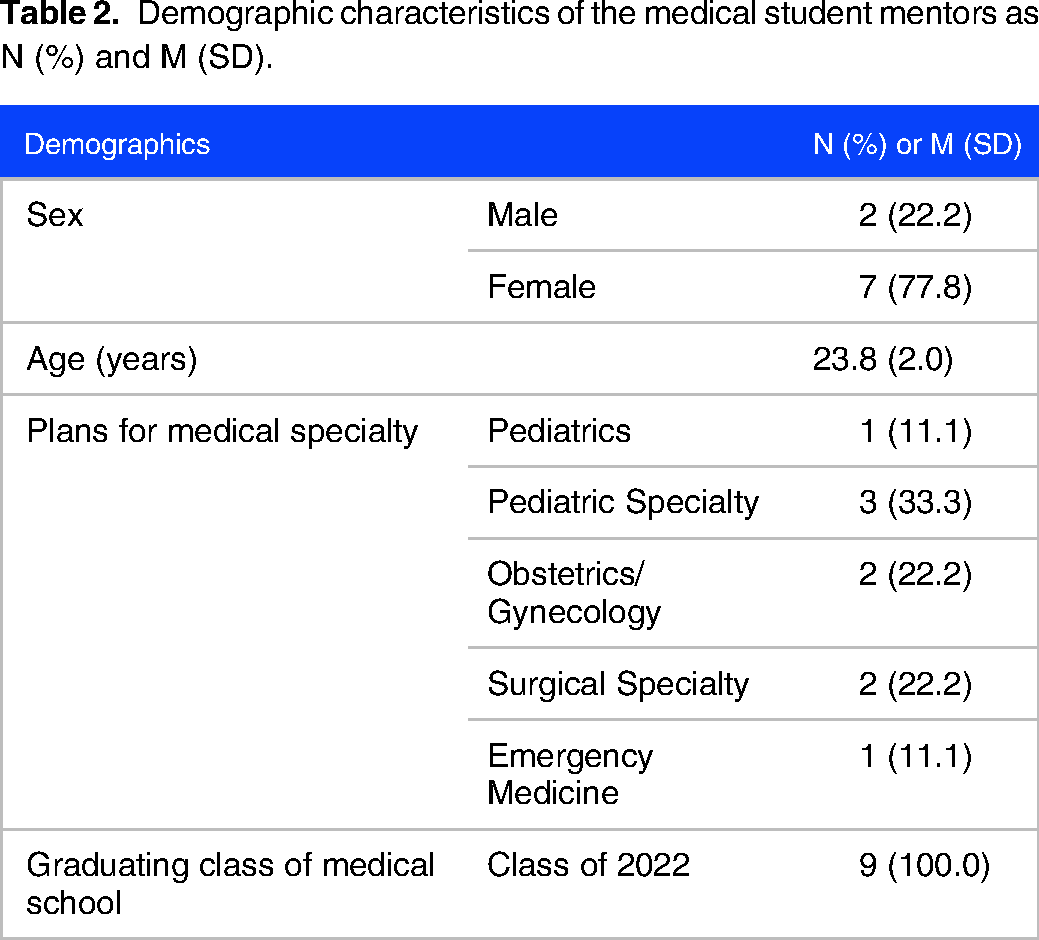
Nine medical students participated as mentors. The mentors were predominantly female (n = 7, 77.8%) and had a mean age of 23.8 years (SD = 2.0) (see Table 2). Each student was paired with between one and three mentees over the duration of the study, with the majority having two mentee relationships. All nine of the medical student mentors completed the non-credit elective requirements. Eight of nine completed the follow-up survey.
Demographic characteristics of the medical student mentors as N (%) and M (SD).
Knowledge of sickle cell disease
Medical students answered an average of 19 out of 24 items (79%) correctly on the baseline measure of knowledge of SCD. Immediately following the training, students’ mean score was 21.6 (90%). This showed a significant increase in knowledge from baseline to post-training (p = 0.014, Cohen's d = 1.04).
Attitudes towards chronic illness
In checking assumptions for the dependent t-tests, one outlier was found for the items related to comfort in managing chronic illness and was therefore excluded from those analyses. Given the small sample size, the focus was on characterizing the magnitude of any changes from baseline to post-intervention, rather than statistical significance. In general, the changes on items were small and need to be interpreted cautiously given the small sample (see Supplemental File S3).
Satisfaction and perceived impact
Medical students reported greatest satisfaction with the content of the mentor manual (M = 4.50, SD = 0.76), the content of the mentor training (M = 4.38, SD = 0.74), and the program overall (M = 4.38, SD = 0.52). Mentors perceived that their participation in the program improved their knowledge of transition (M = 4.50, SD = 0.76) and knowledge about managing a chronic illness (M = 4.25, SD = 0.71; Table 3). Mentors reported on their favorite part of the program, ways they felt changed by participating as a mentor, and suggestions/improvements for the intervention (Table 4). Many mentors felt their relationships were like friendships and developed strong bonds. Many mentors also reported that their favorite parts of the intervention were learning from their patients and getting a patient's perspective on living with sickle cell disease (Table 4).
Medical student mentor satisfaction.

Themes of mentor responses from open-ended questions.

Note. The numbers in parentheses indicate the number of mentors reporting on each topic area (out of a total of 9). Themes were driven by the questions asked to solicit feedback. Example quotes demonstrate how topics were extracted from the individual text response data.
Mentors were also questioned about the training experience during an exit interview. Mentors reported on the high value of both the mentor training as well as the monthly group discussions. Six of the mentors felt that the patient advisory board contributed an important perspective that shaped the way they approached their interactions with their mentee and allowed them to have a broader understanding of the more far-reaching effects of living with sickle cell disease. Many of the mentors (n = 5) also appreciated the opportunity to learn from the interdisciplinary care team during the training, and from each other's experiences (n = 4) during the monthly mentor meetings.
Mentor–mentee relationship
Mentors reported high ratings on the bond domain of the working alliance inventory, M = 19.63, SD = 0.62 (range 18 to 20), indicating high levels of relationship quality. They reported moderate levels of agreement on goals (M = 11.71, SD = 3.12, range 3-15) and tasks (M = 11.88, SD = 3.26, range 4-15).
Discussion
A medical student mentoring program for AYAs with sickle cell disease transitioning from pediatric to adult care was feasible and may be beneficial to medical students. In this small feasibility study, students reported several benefits that align with the AMA's call for value-added roles, including perceived increased knowledge about managing a chronic illness and transition, improved understanding of the patient's experience navigating the healthcare system, enhanced patient communication skills, and increased recognition of barriers to accessing high-quality healthcare. Medical students reported high satisfaction with the program, including the mentor training, program materials, and the relationship developed with their mentees.
Consistent with prior research that utilized medical student mentors,26,27 medical students felt that this experience deepened their understanding of barriers to accessing health care and complemented their didactic medical education about topics like managing a chronic illness and transitions of care. Students rated higher improvement in their knowledge of transition and managing a chronic illness, and less improvement in patient communication skills or clinical skills. This may be because this program was conducted virtually outside a clinical visit and thus focused on patient self-management topics rather than any clinical evaluation or questions. Prior work in peer-mentoring programs found that these programs offer educational benefits for both teachers and learners, including understanding basic concepts, improved interpersonal skills, and reduced anxieties learning new material.28–30 These outcomes may be prudent to explore in the future as other potential benefits of participation in the intervention. Additionally, future iterations may vary the frequency and/or duration of the mentoring relationships to determine optimal ‘doses’ for both medical student mentors and patient mentees.
It would also be valuable to follow these students over the course of their medical education to assess how this experience affected their medical education and if any benefit is maintained during their medical education and career. Comparing students who participated in the program to students who did not would help determine if participants experienced lasting changes in attitudes towards chronic illness. Practice-based experiences such as acting as a patient mentor serve as a way for medical students to contribute to health systems and improve patient outcomes. Initial results from this study found that both medical students and patients found the experience enjoyable and worthwhile, with evidence of preliminary efficacy for patient outcomes. 16 Utilizing medical students as mentors is a practice that could be implemented in many chronic disease populations, creating an opportunity to expand value-added clinical learning in the medical curriculum. Our program benefited from a strong working relationship between the pediatric and adult medical teams and our students. Creating a non-credit elective or service-learning opportunity may provide structure for initiating such programs. Initiatives such as this may facilitate integration of medical students into interprofessional care teams as well as contribute to high quality care for young adults with chronic illnesses. 31
Despite promising results, conclusions from this study must be interpreted cautiously as this pilot program only included a small number of medical students from one medical school. This small sample size may reflect highly motivated students and limits the ability to generalize results from this study. Second, the data used to assess impact and learning outcomes are self-reported and subject to desirability bias. Although students were not graded on their performance as mentors, they may have felt compelled to report in a positive manner. In the future, additional objective measures such as objective structured clinical examinations should be used to measure students’ progress. Third, based on prior work, the items from the Attitudes Towards Chronic Illness measure19,20 were examined separately, increasing the potential for error; future work would benefit from additional measure validation examining the construct of medical student and physician's attitudes towards patients with chronic illnesses. Lastly, there was no control group to compare how student's skills may have improved without participating in the program. Although the students attributed some positive changes to their participation in the program, such as increased knowledge of sickle cell disease, we are unable to draw causative conclusions given the uncontrolled design. Increased knowledge could be due to the medical school curriculum.
Conclusions
A medical student mentor intervention is both feasible and may be beneficial to medical students by providing a value-based role to educate students about the care of patients with chronic illness and the transition from pediatric to adult health care.3,4,32 Rigorous training of students prior to engaging in a mentoring role and ongoing supervision contributed to a high quality educational experience for them. Further research is needed to evaluate the efficacy of this type of student mentoring program on both patient and student outcomes.
Statements and declarations
Ethics
This research was approved by Rutgers Biomedical and Health Sciences Institutional Review Board (IRB # Pro2018001531). The study was conducted in accordance with the Declaration of Helsinki.
Consent
All participants provided written informed consent prior to enrolment in the study.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241274161 - Supplemental material for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors
Supplemental material, sj-docx-1-mde-10.1177_23821205241274161 for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors by Adrienne S. Viola, Mariah Jacqueline Scott, Hanin Rashid, Richard Drachtman, Amanda Kaveney, Ashwin Sridharan, Beth Savage, Cristine Delnevo, Jerlym S. Porter and Katie A. Devine in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241274161 - Supplemental material for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors
Supplemental material, sj-docx-2-mde-10.1177_23821205241274161 for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors by Adrienne S. Viola, Mariah Jacqueline Scott, Hanin Rashid, Richard Drachtman, Amanda Kaveney, Ashwin Sridharan, Beth Savage, Cristine Delnevo, Jerlym S. Porter and Katie A. Devine in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241274161 - Supplemental material for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors
Supplemental material, sj-docx-3-mde-10.1177_23821205241274161 for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors by Adrienne S. Viola, Mariah Jacqueline Scott, Hanin Rashid, Richard Drachtman, Amanda Kaveney, Ashwin Sridharan, Beth Savage, Cristine Delnevo, Jerlym S. Porter and Katie A. Devine in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-4-mde-10.1177_23821205241274161 - Supplemental material for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors
Supplemental material, sj-doc-4-mde-10.1177_23821205241274161 for Medical Student Mentors for Young Adults with Sickle Cell Disease: Impact on Mentors by Adrienne S. Viola, Mariah Jacqueline Scott, Hanin Rashid, Richard Drachtman, Amanda Kaveney, Ashwin Sridharan, Beth Savage, Cristine Delnevo, Jerlym S. Porter and Katie A. Devine in Journal of Medical Education and Curricular Development
Footnotes
Abbreviations
Acknowledgments
Elliot Coups, PhD contributed to the development of the intervention and an early draft of this work but passed in 2021 prior to the preparation of this manuscript.
Authors contributions
Adrienne S. Viola and Mariah Jacqueline Scott are co-first authors; Dr Adrienne Viola and Dr Katie Devine conceptualized and designed the study, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr Hanin Rashid, Dr Richard Drachtman, Dr Amanda Kaveney, Dr Ashwin Sridharan, Dr Beth Savage, Dr Cristine Delnevo, and Dr Jerlym Porter participated in the design of the mentor training materials, selection of measures, and recruitment and enrollment of participants. Ms. Mariah J. Scott participated in data analysis and critical revision of the results and the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Data availability
The data that support the findings of this study are available from the corresponding author, KD, upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Heart, Lung and Blood Institute of the National Institutes of Health under award number F30HL142311. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.