
Abstract
Introduction
Sickle cell disease (SCD) is a genetic blood condition that affects approximately 100,000 people in the United States, predominately those of African descent (Hassell, 2010). There are several subtypes of SCD, with the most common and severe form being hemoglobin SS, known as sickle cell anemia. Sickled red blood cells are abnormally shaped, break down faster than normal red blood cells, and cause vaso-occlusion (blockages in blood vessels) that can lead to oxygen desaturation, pain, and stroke (Morton & Key, 2002; Rees et al., 2010). SCD contributes to health complications that can emerge in the child’s first year of life and persist throughout the lifespan (Hogan et al., 2006; Prussien et al., 2019; Thompson et al., 2002). Sequelae of the disease can have a detrimental impact on typical child development; thus, it is critical to identify developmental delays as early as possible so that federally funded early intervention (EI) through Part C services, as written in the Individuals with Disabilities Education Act (2013; 20 U.S.C. § 1400; 34 C.F.R. Part 303), can be provided (Rees et al., 2010). However, no standard of care exists for screening young children with SCD for developmental delays, and it is unclear among providers as to who should be conducting screening and when. Most individuals with SCD receive the majority of their health care through specialty providers, typically a hematologist (Aljuburi et al., 2012). It is likely that development delays go undetected among children with SCD because of low rates of screening among primary care providers and hematologists (Aguwa et al., 2021; Drazen et al., 2016; Lance et al., 2021).
Developmental delays can present as early as 9 months of age in children with SCD (Hogan et al., 2006). By age 4, about half of the children with SCD may be classified as having a clinically significant developmental delay (Drazen et al., 2016; Thompson et al., 2002). Delays in cognition are most common and may progress with age (Hoyt et al., 2022). Children with SCD have poorer academic achievement and attainment than peers, impacting socioemotional and cognitive milestones (Berkelhammer et al., 2007; Epping et al., 2013; Schatz et al., 2008; Thompson et al., 2002). Consequently, children with SCD often fall behind their peers in the foundational skills critical for the successful execution of daily activities and academic tasks (Drazen et al., 2016). Early intervention is crucial to ameliorate the impact of long-term disability.
Given the high risk of developmental delay among young children with SCD, early detection through screening presents an opportunity for intervention services, such as EI, a federally funded program, to be provided to children during this period of rapid neuronal development. EI may include parental education, speech therapy, physical therapy, and other services based on need and can be provided to children of age 0 to 3 years in the child’s natural environment for free or at a reduced cost. Although specific research on the effects of EI on the SCD population is scarce, EI has demonstrated beneficial effects on cognitive development of preterm infants and caregiver mental health (Hoyt et al., 2023; Puthussery et al., 2018; Spittle et al., 2015). Specifically, significant improvements in cognitive and expressive language were observed among young children with SCD who participated in a home visitation program with an occupational therapist (Fields et al., 2016).
Despite the availability and affordability of EI services and the potential for EI to positively benefit children with SCD, EI remains underutilized among historically marginalized communities, especially Black or African American communities (“Individuals With Disabilities Education Act,” 2004; Rosenberg et al., 2013). In one study, over 50% of children with SCD younger than 3 years had a developmental delay, but none had been referred to EI services (Fields et al., 2016). Individual, environmental, and systemic factors may contribute to EI underutilization among children with SCD. One of the major barriers is that SCD is not a qualifying diagnosis for EI (Thompson et al., 2002). EI service utilization may be additionally delayed because indicators of developmental delay in children with SCD are often overlooked, and symptoms like pain and silent stroke (cerebrovascular infarct with no noticeable symptoms) are not obvious (Shenoi et al., 2011; Zempsky, 2009). These barriers are exacerbated by systemic forms of racism and oppression, which results in inequitable access to health care services, including EI (Hood et al., 2022; Rosenberg et al., 2013; Wakefield et al., 2017). Previous research shows that Black children are five times less likely to receive services when not automatically eligible (Feinberg et al., 2011). Because of the complex comorbidities and elevated risk of developmental delays associated with SCD (Hoyt et al., 2022), EI that provides home-based caregiver education and support for meeting developmental milestones could have a meaningful long-term impact on the lives of children with SCD and their caregivers (Bann et al., 2016; Casey et al., 2017; de Azevedo & Malmegrim, 2020; Drazen et al., 2014; Fields et al., 2016).
Our long-term goal is to develop a comprehensive developmental screening and referral program for children with SCD that can be incorporated into the standard of care so that all children in need would receive EI. To understand how we can improve screening and access to EI, we need to first identify the concerns and values of the communities we intend to serve. Reasons for low utilization of EI interventions among children with SCD are likely multi-faceted, including low caregiver engagement due to lack of knowledge of developmental needs, providers’ low awareness of service needs of this population, or structural challenges at the EI organizational level related to service eligibility. Engaging with those in the SCD and EI community is needed to better understand the reasons for the low utilization of EI services among this population and to identify areas for improvement to establish better service linkages. For this reason, in the present study, we sought to gather input from both SCD caregivers and EI service providers. The purpose of this study was to (a) assess caregivers’ knowledge of developmental milestones and risk of delays among children with SCD, (b) assess EI professionals’ practice contexts to adopt evidence-based service changes, and (c) understand caregivers’ and EI professionals’ attitudes regarding the need for and perceived barriers and facilitators toward providing EI services to children with SCD through a screening and referral program.
Methods
To fulfill the purpose of this study, we followed a mixed-methods approach grounded in implementation science. The research team included experts in SCD, EI, qualitative research, and implementation science research. To assess caregiver knowledge about child development and EI professionals’ practice contexts to adapt service change, we used existing validated surveys for assessment. We also conducted semi-structured interviews to understand caregivers’ and EI professionals’ attitudes regarding the need for and perceived barriers and facilitators toward providing EI services to children with SCD through a screening and referral program. Qualitative data collection followed the consolidated criteria for reporting qualitative studies guidelines (Tong et al., 2007). Survey data and interviews were collected by the first author. Results from surveys and interviews were compared to one another for each participant and analyzed concurrently. All study activities were approved by the institutional review board at Washington University School of Medicine. Participants provided informed consent before the study procedures were initiated.
Participants
Over a period of 3 months from September to November 2020, caregivers were recruited from the St. Louis Children’s Hospital Hematology Clinic. Caregivers were approached to participate if their child had a confirmed SCD diagnosis per the medical record (all SCD genotypes were included) and if the child was between the ages of 3 and 5 years. This age range was selected so that caregivers would have already experienced the current standard of care for developmental screening and EI referral among children up to 3 years of age and could describe strengths and areas for improvement. The caregivers must be English-speaking is one of the inclusion criteria; however, no one was excluded for this reason.
To ensure the representation of EI professionals, regional leaders, and decision-makers, we used a purposive sampling approach to recruit EI professionals from different domains including service coordination, direct service providers (e.g., physical therapy, occupational therapy, special instructors), and regional directors who had over 12 months of experience in EI.
Data Collection
Demographic Information
Caregivers provided demographic information including caregiver age, gender, race, ethnicity, income level, number of children and adults living in the home, address, and education level. Medical records of each child were reviewed to identify their SCD genotype. EI professionals listed their role in EI, years of experience in EI, and gender. All data were collected and managed in REDCap, an online data-capture tool that allows for data collection using a secure link sent via email (Harris et al., 2009).
Caregiver Knowledge of Infant Development
Caregivers completed the Knowledge of Infant Development Inventory (KIDI), a two-section, 58-item parent report survey, to determine their understanding of developmental milestones and awareness of when they should be achieved (e.g., can a 6-month-old follow directions?) (MacPhee, 2002). We were interested in assessing caregivers’ knowledge about typical child development to better understand if caregivers would know how and when to identify if their child had a delay and to determine if additional education or support in this area is warranted. The first section of the assessment lists statements about behavior and development, and caregivers were asked whether they agree or disagree with the statement. The second section requires the caregiver to state whether a developmental milestone is matched with the correct age and, if not, to indicate whether the milestone should occur at a younger or older age than stated. The KIDI is a validated measure and has been previously used with caregivers of children with SCD (MacPhee, 2002; Thompson et al., 2002). Caregivers were given the option to complete the KIDI verbally over the phone or online using a Health Insurance Portability and Accountability Act (HIPAA) secure link sent via email.
EI Professionals’ Practice Contexts
Children with SCD can benefit from EI, which is supported by clinical practice guidelines and evidence for developmental delay (DeBaun et al., 2020; Hoyt et al., 2022). However, state-level policy is needed to ensure that children with SCD are considered eligible for EI. To determine if this change is possible, the Implementation Climate Scale (ICS) was administered (Ehrhart et al., 2014) to assess the organizational context to adopt evidence-based practice changes. The ICS is a validated 18-item survey to assess the readiness of an organization to embrace evidence-based practices and new programs (Ehrhart et al., 2014). It includes six dimensions of fundamental context to indicate how the organization prioritizes and values the implementation of evidence-based practice (Ehrhart et al., 2014). Subsections include the focus, educational support, recognition, rewards, openness, and selection for evidence-based practice. Professionals were asked to answer on a 0- to 4-point scale (0 = not at all; 4 = very great extent) to indicate their level of agreement with each statement, such that higher scores indicated greater acceptance. EI professionals were given the option to complete the ICS verbally or with a HIPAA secure web link.
In addition to the ICS, the research team developed a follow-up survey to understand strategies to increase provider engagement in evidence-based practice change within their current settings. The follow-up survey asked the same EI professionals to rank order six incentives extracted from the literature (Jacobs et al., 2010). Incentive options included social media recognition, the chance to decide something (e.g., learning topic of the month with their EI team), a team award (e.g., coffee), thank you letters from team members (e.g., card or virtual bulletin), therapist of the month award, opportunity to present something and receive continuing education credit, and an open-ended field for suggestions to increase evidence-based practice change.
Caregiver and EI Professionals’ Attitudes Toward the Need for and Perceived Barriers and Facilitators of EI Programming
Interviews were conducted with SCD caregivers and EI professionals to understand current attitudes toward the need for and perceived barriers and facilitators of EI screening and service delivery for children with SCD. Semi-structured interview guides were developed by the first author (CH), a trained White, female occupational therapist with over a decade of experience working in EI and with patients with SCD (Creswell & Poth, 2016a). The caregiver interview guide was piloted with a mother of two children with SCD, and the EI interview guide was piloted with a direct service provider with over 10 years of clinical EI experience. The EI professional interview guide contained nine questions (Table 1), and the caregiver interview guide contained eight questions (Table 2). All interview participants were provided a brief standard explanation of EI, SCD, and the potential impact on development. Interviews were designed to last about 30 minutes to minimize participant burden and ensure adequately rich data. All interviews were conducted by the first author (CH) and were conducted over the phone (n = 12) or via video conference (n = 7) to abide by safety procedures during the COVID-19 pandemic. This method is not expected to impact outcomes (Johnson et al., 2021). Field notes were taken during each interview to document important points related to the discussion. Participants were compensated with a $20 electronic gift card.
Caregiver Interview Questions.
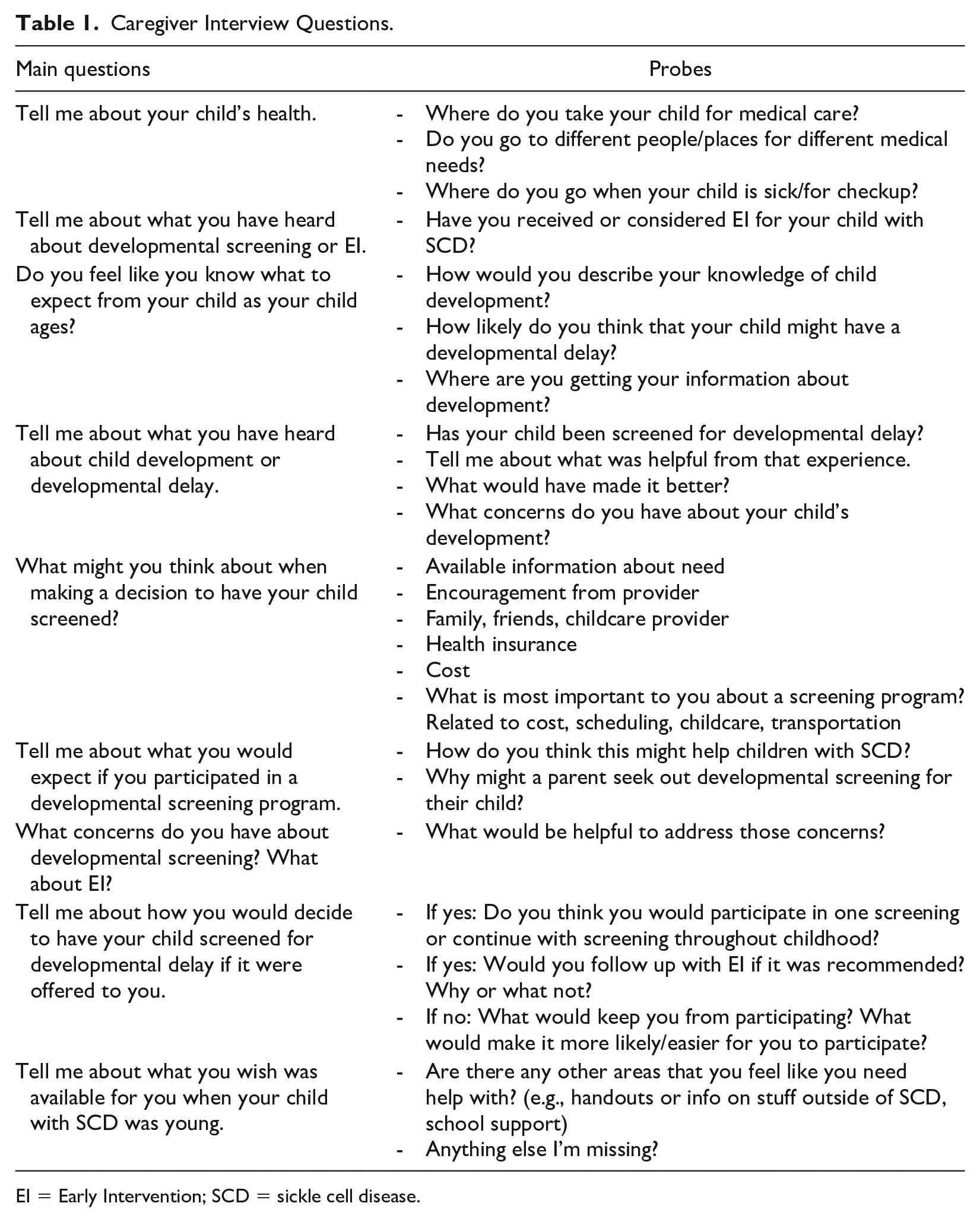
EI = Early Intervention; SCD = sickle cell disease.
Early Intervention Provider Interview Questions.
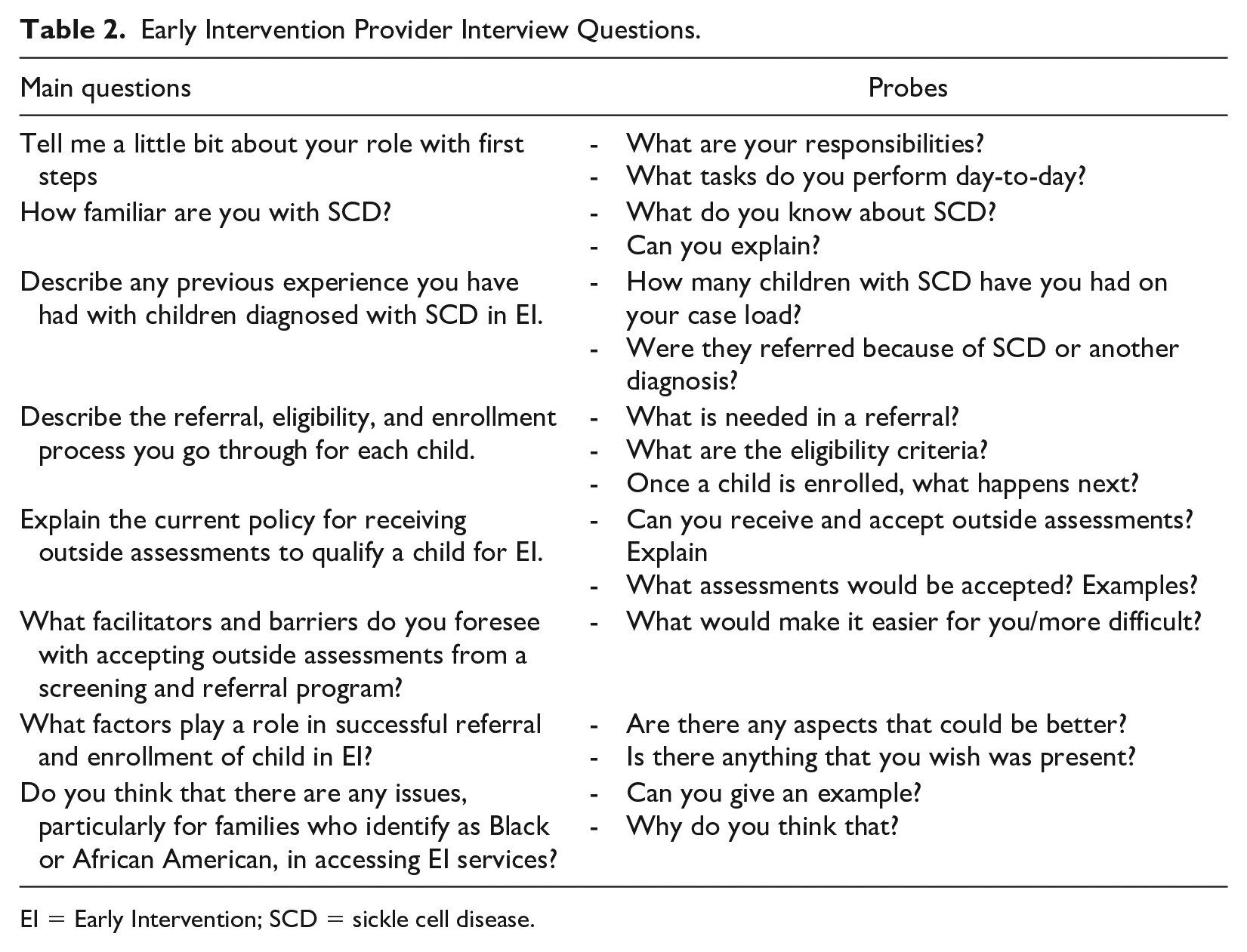
EI = Early Intervention; SCD = sickle cell disease.
Analysis
Quantitative Data
Quantitative survey results were scored and analyzed following procedures outlined in their respective manuals and publications (Ehrhart et al., 2014; MacPhee, 2002). Descriptive statistics summarized demographic and survey data. Scores on the KIDI and ICS were summarized alongside qualitative interviews to determine the need for and feasibility and acceptability of an EI referral program and uptake among EI professionals and caregivers.
The responses to the follow-up incentive rank order survey for EI professionals were summarized by the mean score for each incentive. Each incentive was ranked from 1 to 7, so items with a lower mean score indicated higher preference. Responses to the open-ended question were reviewed and summarized by two authors (CH, JE).
Qualitative Data
Interviews were audio-recorded, transcribed verbatim, and independently reviewed for accuracy by two investigators (CH, JE). All data files were loaded into QSR International’s NVivo 12 software v.12 for analysis (International, 2018). Authors (CH, JE) completed a pre-self-reflection of potential biases and assumptions to alert and prevent potential biases before beginning the coding process. All transcripts were independently reviewed by two team members to identify themes emanating from the data. Preliminary themes were discussed using a consensus approach, and a codebook was developed. Once the codebook was finalized, the same two team members coded all transcriptions independently; codes from each transcript were discussed until a consensus was reached. Following the coding process, transcripts and field notes were reviewed to ensure no themes were overlooked. Intercoder agreement checks were used in place of an interrater analysis due to the increased reliability of having two research team members develop and share an initial codebook, apply the codebook to transcripts and compare all codes between both researchers, assess intercoder agreement among researchers, revise and finalize the codebook, and compare all codes until consensus was reached (Creswell & Poth, 2016b, pp. 264–265). Although our sample size was relatively small, our interview data yielded a saturation of topics and themes. Following our interviews, we thoroughly reviewed the recordings and field notes and determined that we reached saturation with no new themes emanating from the interviews.
Results
Participants
A total of 19 participants were interviewed and completed either the ICS or KIDI. Among 39 caregivers identified as eligible, 11 consented and completed both the interview and survey. Reasons for not participating included not being able to reach the family (e.g., disconnected phone line) and time constraints. Eight of the 11 participating caregivers (73%) were the children’s mothers, and the remaining were fathers. Of the children represented in the interviews, 56% were diagnosed with hemoglobin SS genotype, and 36% with hemoglobin SC genotype (Table 3), which aligns with the general SCD population (Saraf et al., 2014). Similar to previous reports, many children with SCD in our cohort were living in low-income households (King et al., 2014; Yarboi et al., 2017).
Demographics of Caregivers of Children With SCD and Demographics of Early Intervention Partners.
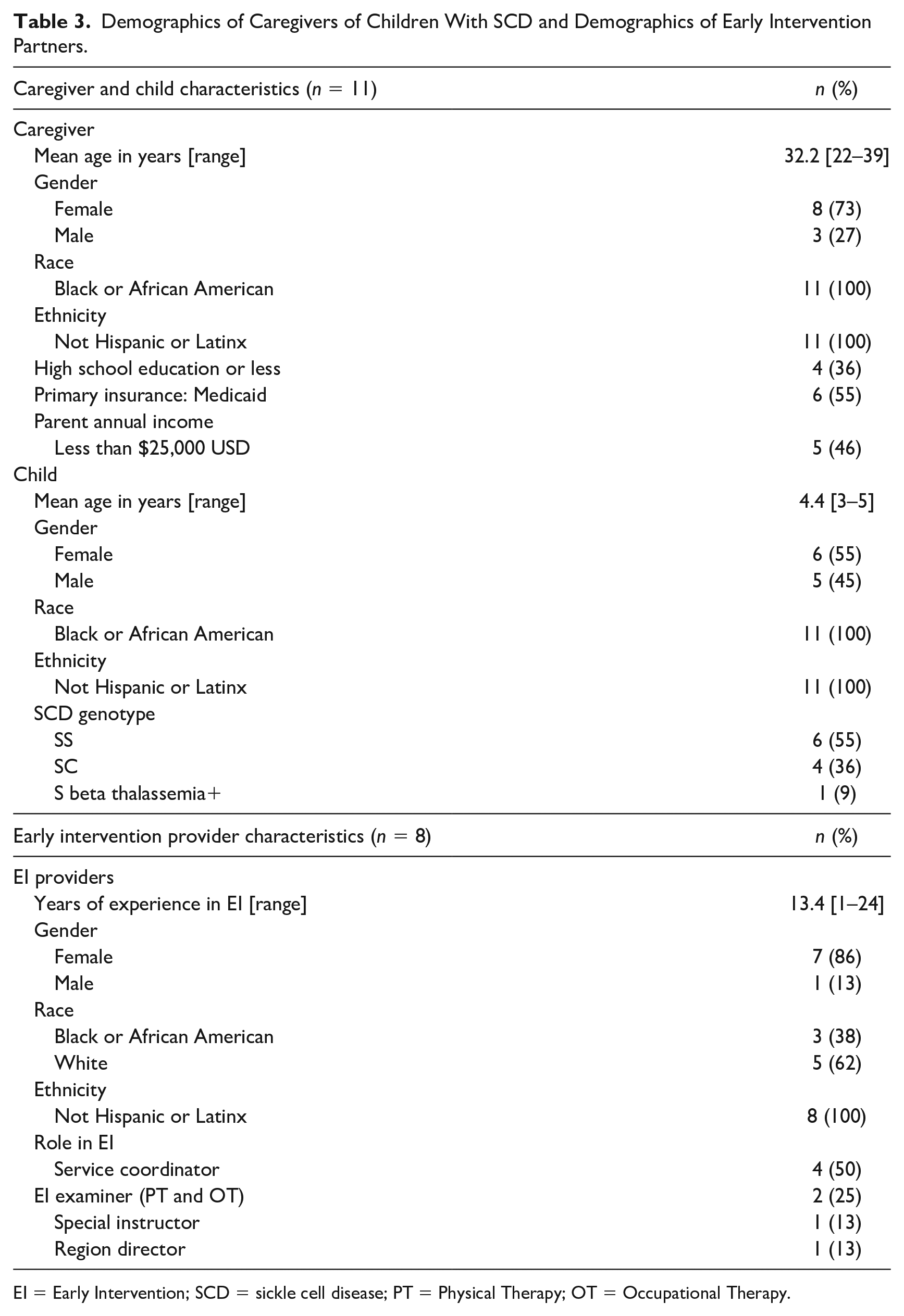
EI = Early Intervention; SCD = sickle cell disease; PT = Physical Therapy; OT = Occupational Therapy.
Among 10 EI partners approached to participate, eight consented and completed an interview and the ICS. Our cohort included four service coordinators, three direct service providers, and one regional director. Participants have experienced EI professionals, with an average of 13.4 years of service (range 1–24 years) (Table 3).
Caregiver Knowledge
Ten caregivers (91%) completed the KIDI verbally over the phone, while one (9%) completed it independently the following day using an emailed survey link. On average, caregivers selected “unsure” for 6.6 questions (range 1–23), stating that they were unsure or did not want to respond to an item. The average accuracy score across all caregivers was 79% (range 66%–92%, SD = 9%). The number of skipped questions and range in accuracy indicate a high level of variability in the confidence and knowledge that caregivers have about early childhood development and when to expect to observe developmental skills (e.g., awareness of danger at the stairs, starting solid foods). The most frequently missed items focused on child attachment (e.g., crying, being clingy, providing comfort). The variable knowledge of child development, particularly as it relates to caregiver relationships, aligns with caregivers’ qualitative reports of psychosocial challenges and the need for more education related to child development (further described below).
EI Professionals’ Practice Contexts
Seven professionals (88%) completed the ICS verbally, and one (12%) completed it independently following the interview. Survey results from the ICS are summarized in Table 4. EI professionals reported a high level of focus on evidence-based practices in EI (M = 2.75, SD = 0.97), but little to no reward to individuals who use evidence-based practice (M = 0.08, SD = 0.22). Despite the absence of rewards, professionals indicated a fair amount of interest in receiving more educational support (M = 1.54, SD = 1.26) and recognition from peers (M = 1.79, SD = 0.83) for using evidence-based practice. In terms of EI leaders supporting evidence-based practice, professionals endorsed a moderate level of openness (M = 2.21, SD = 1.13) and selection of providers for their application of evidence-based practice (M = 1.92, SD = 1.02). The high level of interest but low incentive suggests that EI partners are willing to modify their practice when provided with appropriate education, resources, and training.
Results From Implementations Climate Scale.
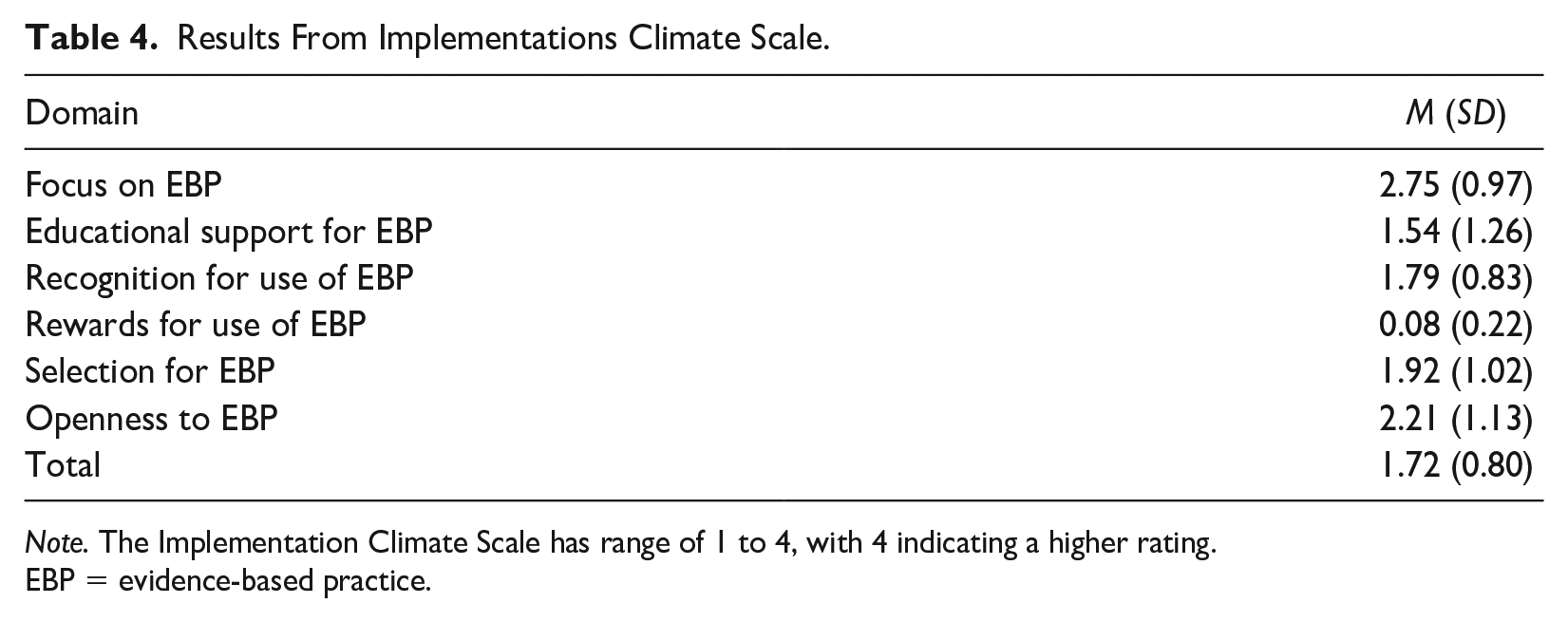
Note. The Implementation Climate Scale has range of 1 to 4, with 4 indicating a higher rating.
EBP = evidence-based practice.
All eight EI professionals completed the follow-up survey to rank order incentives. The most favored incentive was the chance to decide something, such as choosing the learning topic of a monthly EI team meeting (M = 2.63), followed by a team reward, like coffee (M = 3.13). Thank you notes (M = 3.38), therapist of the month award (M = 3.75), and the opportunity to present something (M = 3.75) were also moderately favored. Social media recognition was the least preferred (M = 4.38). Four respondents (50%) provided additional suggestions, which all described a desire for access to additional training and educational materials, particularly for service coordinators.
The Need for and Perceived Barriers and Facilitators of EI Interventions for Children With SCD
The 11 caregiver interviews lasted between 15 and 41 minutes (M = 24 minutes). The eight EI professional interviews lasted between 14 and 49 minutes (M = 33 minutes). Three major themes emerged from the interviews that described the need for and acceptability and feasibility of developmental screening, referral, and uptake of EI for young children with SCD: (a) disparities and racism in health care delivery and caregiver experiences, (b) high acceptability of screening and referral to EI program for children with SCD, and (c) importance of education to increase partner buy-in as a program facilitator.
Theme 1. Caregiver Experiences and Mental Health Related to Disparities and Racism in Health care Delivery
Cultural and communal disparities were defined as statements related to background, race, socioeconomic status, or diagnosis of people with SCD that negatively impact opportunities for resources, education, and services to be provided or utilized.
Caregivers
Caregivers discussed how the SCD community has historically been excluded from access to resources, culturally tailored education, and dialog regarding the impact of SCD. When discussing the intentions for this study and the long-term goal of creating a screening and referral program, one caregiver said, “thank you, because most people wouldn’t think about the sickle cell kids.” (p. 7). Over 50% of caregivers mentioned a previous experience with stigma or limited resources for their child. When discussing SCD and the complications related to the diagnosis, one caregiver stated, “The African American community aren’t aware of it [SCD] themselves, so we need more knowledge.” (p. 9). Comments like “You have [the] preconceived notion that the doctors and the team are kind of against you. Sickle cell isn’t something that you can necessarily see. I think people have this notion that, oh, it’s not as big of a deal” (p. 16) and “with something like SCD and the population that it affects, there is widespread and really well-known discrimination when it comes to treating and believing the patient” (p. 16) allude to the perception among caregivers of systems that limit access to high-quality health care for this population.
Three caregivers described the psychosocial impact of being a caregiver for a child with SCD and shared statements of emotional distress. One parent commented “I am thinking of relocating [to somewhere warmer]” to reduce the impact of the cold weather on her child’s SCD symptoms and followed up by sharing “I don’t want to leave my job . . . but I don’t want to be here no more. I was thinking about killing myself when she was in the hospital. I didn’t know if she was going to make it or not . . . When she is in pain, I’m in pain.” (p. 13). Another parent described how SCD has influenced their day-to-day life saying, “You hear all the negative and bad things that could happen. Sounds like she [child with SCD] has to live in a bubble . . . We didn’t have a lot of knowledge on it, so you trust your health care provider, they say she can’t go to daycare, then she’s not going.” (p. 19). One parent stated, “I just had a friend that died from sickle cell anemia . . . It freaked me out.” (p. 9). The same parent described when she learned that a sibling could be a bone marrow match to cure SCD, “I tried for a second child, and it was born healthy, so he is her donor.” The psychosocial impact of caring for a child with SCD has specific challenges and limits caregivers and their families from participating in the community and affects family planning decisions. There is a great need for health care providers to discuss the potential psychosocial impact of an SCD diagnosis, including caregiver mental health, early and often with families of children with SCD.
EI Professionals
EI professionals reported limited exposure to children with SCD. Most were unaware of the increased risk of developmental delay or the potential benefits of home-based parent education services for this population. Professionals made reports such as, “I have not worked with a child with sickle cell disease in Early Intervention” (p. 2) and “I’ve never had a referral [of SCD]. So, I think not having a referral is a huge thing and it opens my eyes to the fact that, wow, we really need to make sure doctors and providers in the hospital are referring them.” (p. 4). Only three of the eight professionals reported ever having worked with a child with SCD, and all these children were referred based on a secondary diagnosis, such as stroke. Delivering evidence-based education to health care providers about SCD and associated complications, such as developmental delay, is a necessary step toward increasing rates of developmental screening and referral to EI.
In addition, EI professionals recognized that financial resources for many families with SCD are limited and that changes in the health care system need to occur to address the problem. One professional stated, “we want to be reaching these families [in the SCD community], especially now more than ever, when there are so many limited resources for them, and private therapy can be more difficult to access.” (p. 2). Professionals described the social and economic disparities present in this population and how disparities make it more difficult for families to access the services they need. Remarks like “the social inequalities and income disparities, unfortunately, systemically can make it harder for us to access families, and that’s something we really want to know how we can address better” (p. 2) suggest that professionals want to reach this community and provide services but need support to bridge the gap.
Theme 2. Acceptability of a Screening and Referral Program for Children With SCD
Program acceptability refers to comments related to a participant’s level of willingness to participate in a screening program, support its implementation, or comments associated with agreement with the program (Lewis et al., 2015).
Caregivers
Overall, caregivers of children with SCD were very interested in developmental intervention for their child, and there was high acceptability for a screening and referral program to EI. When asked about willingness to participate in a screening and referral program, one caregiver stated, “If you tell me that there’s something I could do because my child should be somewhere at six months and they’re not, and I could be doing something that will help them through that, then yeah, I would do it.” (p. 17). Another caregiver thought that screenings should take place “three times a year when they’re even smaller because the sooner you can identify something the sooner you can correct it.” (p. 16). All caregivers expressed interest in learning more about their child’s development and willingness to learn more about a screening and referral program.
Caregivers also expressed a high level of acceptability toward participating in new programs or research that could support their child. They stated they wanted more research that focuses on the sickle cell community so that there is more awareness about the diagnosis to encourage health care providers to invest more resources to the community. Caregivers desired research to address gaps that might benefit children with SCD and improve developmental outcomes. One caregiver stated, “this [program] is something that could help set up this community in general even if it is not to help my child. If it was something that would help in general, I would be open to it” (p. 17) and “I believe that it can help others in the future by doing the research now” (p. 7), which reflect the positive responses from caregivers regarding SCD research. Overall, caregivers communicated that compensation was not a motivating factor to participate in a study with novel programming, and they were highly interested in anything that could support their ability to care for their child, as described by one caregiver, “if it is helping my child, then I don’t need to be paid for it” (p. 11).
EI Professionals
Similar to caregivers, EI professionals reported high acceptability toward a program that would screen and refer children with SCD to EI. Professionals stated that a “[screening program] would help bridge the gap of skills with special needs or developmental delays because the earlier you start working on the delay, the less the child will have the delay longer in life.” (p. 3). Responses across EI interviews were consistent in their openness to a screening and referral program and how “it would be beneficial for everyone, especially the families.” (p. 1).
Following a brief description of SCD and the associated complications, 100% of EI professionals communicated that EI would be beneficial and indicated they would support systemic changes that would enable children with SCD to be considered automatically eligible for EI, indicating acceptability to modify recruitment methods based on increased knowledge of the impact of a diagnosis on child development. One person stated, “although it’s [SCD] not an automatic eligibility diagnosis [for EI], is definitely one of those diagnoses that really does put a child at risk for developmental delays.” (p. 2). Another individual stated, “I don’t know why SCD is not listed as one of the important conditions that we should be looking at . . . just looking at our eligibility criteria and expanding that, or at least updating it to make sure that we’re capturing what’s really happening.” (p. 8).
Theme 3. Importance of Education to Increase Partner Buy-In as a Program Facilitator
The third central theme was related to program buy-in, which described comments that refer to a caregiver’s or professional’s willingness to actively participate in developmental screening and engage children with SCD in EI. This theme included factors (barriers and facilitators) that would influence a caregiver’s decision to participate in a screening and referral program or an EI professional’s willingness to include children with SCD in EI programming.
Caregivers Want Education about SCD and Development to Guide Decision-making
All caregivers reported a desire to better understand the implications of an SCD diagnosis and the availability and benefits of different resources and services. When caregivers were asked questions regarding practical ways to educate caregivers, one stated, “I think incorporating the education into a conversation because I think that helps patients feel heard and then it helps them buy into it more and be more willing to have buy-in.” (p. 16). Another caregiver stated, “I would like to just know what are more options on things you can do more of and try to prevent things without basically sheltering your child” (p. 19). This caregiver desired more education and resources about SCD to keep their child healthy while allowing them to have as normal of a life as possible. Overall, caregivers communicated a need for more personal guidance about their child’s diagnosis and development. Caregivers expressed that receiving more tailored information would increase their likelihood to participate in programming related to development. Thus, an essential component to increasing caregiver buy-in for developmental screening and EI programming is guidance on intervention options for SCD and education related to child development.
Caregiver-Reported Barriers to Participate in Developmental Screening and EI
Other factors that contributed to a caregiver’s willingness to participate in screening and EI included knowledge that the program existed, work schedules, availability of child care, and length of clinic visits. When discussing factors that would facilitate or inhibit participation in a screening program, a caregiver stated, “The time constraint is like . . . most people are trying to get back to work or something along those lines” and “I definitely would be interested in having it [screening] at home just because that takes a burden off of trying to find time, like I’ve got multiple kids.” (p. 16). Caregivers were clear that though life circumstances were barriers to participation, they were highly interested in services that could help their child. Costs associated with services (i.e., transportation costs) were not identified as a barrier.
Professional Education Can Increase Recruitment to EI
Due to the limited experience EI professionals had with SCD, most did not know about the elevated risk of developmental delay in the first years of life. We found similar uncertainty and misunderstanding related to policies that guide qualification criteria for EI services, particularly related to outside assessments and referrals. Professionals reported discrepancies regarding their understanding of EI qualification criteria or had an inaccurate understanding of how children could qualify for EI services. One direct provider stated, “I don’t know if we would have to re-do [standardized evaluation] or not. I’m not sure about that process.” (p. 3). While a regional leader in EI stated, “if the evaluation tool already establishes the half-age delay, yes we can use it.” (p. 8). Education to increase professionals’ understanding of EI policy may encourage greater inclusion of children with SCD in EI.
Following a standardized description of the health and developmental impact of SCD with EI professionals, subsequent complications, and policies, interest toward a screening and referral program for children with SCD increased drastically. When asked about how best to provide this information to other professionals in EI, EI professionals identified that service coordinators would benefit most from increased education on SCD and surrounding policies due to their position in the enrollment process. One professional stated, “provider education needs to be done across [EI programming] more than it already is” (p. 5), but specifically “service coordinator education because a [direct service] provider can start the [qualification] process, but it can either be supported or killed by the service coordinator.” (p. 5). One of the service coordinators stated, “if we all are educated on sickle cell and things like that as a service coordinator and how some of these diseases impact families and impact children’s lives, I think it helps us to better understand why it’s so important that they get EI.” (p. 4).
Discussion
The purpose of this study was to explore the acceptability and feasibility of a developmental screening and referral program so that more children with SCD could benefit from EI services. This study has assessed caregiver knowledge, EI professionals’ practice contexts and preferred incentives for adopting practice changes, and caregiver and EI professionals’ attitudes regarding the need for and perceived barriers and facilitators of providing EI services to children with SCD through screening and referral services.
Caregiver responses on the KIDI demonstrated that caregiver knowledge about child development is moderate and may reflect the ongoing education families receive in the first years of life. However, it is also possible that cultural beliefs and expectations may have influenced responses. The KIDI was selected for its intended purpose and because it has been used previously with this population, but an updated assessment of child development would be beneficial (MacPhee, 1981; Thompson et al., 2002). Caregivers expressed the importance and need for more education on how to support development and the risk of developmental delay among children with SCD. Many caregivers lacked confidence in their responses and skipped several items, verbalizing that they were unsure of the answer, which reinforces the potential benefit of caregiver education to increase caregivers’ awareness and interest in a screening and referral program.
During the interviews, caregiver participants expressed interest and motivation to participate in research and programming but also described logistical barriers, like child care and work schedules, which aligns with previous research about the challenges of care access among low- and moderate-income families and racial/ethnic minorities (Jacob et al., 2016; Phillips et al., 2000). While acceptability was high, understanding information, like why screening children under the age of three for developmental delays is essential, was lacking and could present as a barrier for participation. The limited awareness of the risk of developmental delay in the SCD population and availability of services like EI further demonstrates the need for additional education to be provided during future research and within the screening and referral program to increase caregiver buy-in. Listening to caregivers and incorporating their input into the development of screening and referral programs will increase caregiver buy-in because it increases the amount of appropriate and helpful education provided. Most caregivers stated that there is no such thing as too much information when it concerns the well-being of their child.
A striking observation was the willingness of caregivers to discuss the negative mental health impact of having a child with SCD and their impression that their child’s diagnosis, and accompanying psychosocial impact, was often ignored. Caregivers perceived this lack of concern from health care providers and inequity in service provision and availability to be due to the family’s race and that most children with SCD are African American. These perceptions embody the presence of structural and systemic racism that has limited research to develop and implement interventions for this community (Farooq et al., 2020). Given that SCD is a genetic disorder, caregivers of children with SCD often experience emotional distress and guilt, especially at the early stages when their children are newly diagnosed. EI can be a critical service because it supports family-centered interventions that address child development and family support, which could help families cope with the psychosocial impact of living with SCD (Bioku et al., 2021; Jacob et al., 2022).
Although EI professionals communicated a high level of interest in supporting a developmental screening and referral program to EI for the SCD population, results from both the interview and ICS survey show a clear need for programming that supports the delivery of evidence-based care through valued incentives. It is promising that results from the ICS survey demonstrated focus and openness for evidence-based practice among EI professionals; however, the minimal educational support, recognition, and reward for doing so is a concern. EI professionals reported close to zero rewards for implementing evidence-based interventions in their daily practice. Given that SCD is often not considered an automatically eligible diagnosis for EI, it is imperative that EI professionals are motivated to modify their clinical practice as they learn new information about diagnoses, such as SCD. The follow-up survey identified preferred incentive approaches for EI professionals to implement or modify their clinical practice to align with the evidence. Most professionals reported that contributing to the team by deciding a meeting topic (e.g., a topic for the EI team to learn about) and peer recognition-related incentives were the most rewarding. EI professionals seek engagement with colleagues, and provider-led education may be a crucial component in building and implementing a successful screening and referral program to ensure that EI programs are provided to children with SCD in a sustainable manner. Future programming could also customize incentives to meet individual preferences.
Key partner buy-in and engagement is an important facilitator for the implementation and sustainment of EI services (Hickey et al., 2018). Based on our interview results, most EI professionals were not familiar with SCD, and as such, partner buy-in efforts should also include strategies to build interest in SCD among EI professionals. As an SCD diagnosis does not automatically qualify children for EI services in many states, communicating about the risk of developmental delays in this population to caregivers and professionals will strengthen buy-in.
As with every study, there are limitations. Primarily, all interviews were conducted by a single person at a single site, and these results may not be generalizable. In addition, all interviews were conducted virtually because of the COVID-19 pandemic. It is possible that the format of the interview influenced participation to those who had access and comfort in completing a virtual interview. The individual facilitating the interviews knew several of the participants in a professional capacity, and the established rapport helped increase the comfort level during the interview but may have also contributed to biases in how interviewees responded to questions. However, caregivers were open about their experiences of having a child with SCD and shared feelings of grief, depression, and anxiety, so we do not think that participants limited or refrained from sharing their opinions openly. Thus, despite this limitation, we believe that interview findings accurately represent the participants. The interviews produced novel information and insight that specific education for both caregivers and EI professionals is needed to implement a successful screening and referral program.
Conclusion
Given the elevated risk of developmental delay among young children with SCD and underutilization of EI, a developmental screening and referral program for EI services that incorporates multi-level partner feedback could improve outcomes for children with SCD and their families. Semi-structured interviews and surveys with caregivers of young children with SCD and EI professionals identified a need for and high acceptability of such programming once education on the risk of developmental delay among this population was provided. An important finding was that caregivers reported experiences or awareness of stigma related to their child’s diagnosis or racial identity, which may contribute to their willingness to participate in research that helps the SCD community. EI professionals described interest in helping children with SCD access EI services but were unsure about policies regarding how a child can qualify for services. Findings from this study demonstrate that the following components are necessary for the successful development and implementation of a screening and referral program to EI for young children with SCD: (a) caregiver education about child development, (b) caregiver mental health support as a component of EI programming, (c) EI professional education about the impact of SCD and risks of developmental delays among this population, (d) partner buy-in from both caregivers and professionals for implementing and sustaining the screening and referral programs, and (d) organizational incentives to provide evidence-based care and adapted services to better meet the needs of this population.
Footnotes
Acknowledgements
We would like to thank all the parents and EI stakeholders that participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health awards 5K12HL137942 (C.R.H., A.A.K.) and 1K24 HL148305-01 (A.A.K.).