
Abstract
Objective
The aim of this study was to identify the frequency, form, and underlying factors contributing to gender inequity experienced by medical undergraduates and assess its influence on their career choices.
Method
This was a cross-sectional, retrospective survey with a 100% response rate. This survey was distributed among medical students of clinical years in Karachi's private and government medical colleges from September 10th, 2021-March 30th, 2022. 430 participants were enrolled using a simple-random-sampling-technique. Chi-square/Fisher's Exact tests are employed to assess the relationships between gender and gender-based inequity in various specialties, including their characteristics, influence on career choices, adverse psychological effects, and potential mitigation strategies.
Results
Among 430 respondents, 28.6% were male, and 71.4% were female. 89.1% reported gender inequity, evenly distributed in government (80.4%) and private institutions (88.1%). The general surgery and gynecology disciplines stood out, each with a 56% prevalence. In gynecology and surgery clinical-clerkships, both genders experienced similar rates, with females at 54.5% and 42.3%, and males at 56.7% and 61.6%, respectively (P-value = .000*). Disrespect from staff/professors/patients (48.8%) was the most common manifestation, driven by factors like preferences (73.7%), gender superiority (62.6%), societal attitudes (54%), and cultural norms (50.9%). Furthermore, 82.6% of students reported that gender inequity had a negative impact on their career decision (Male = 82.9%;Female = 82.4%, P-value = .899). Additionally, gender inequity also caused demotivation (78.1%), poor self-esteem (67.2%), helplessness/hopelessness (48.6%), and frustration (45.8%).
Conclusions
Gender inequity is widely prevalent in the clinical-clerkships, affecting medical students’ career decisions and mental health, stressing the need to prioritize and implement solutions at the undergraduate clinical-clerkship level.
Keywords
Introduction
Emerging from its profound professional heritage, the field of medicine has been significantly influenced by a myriad of determinants. Notably, amidst these determinants, the escalating recognition revolves around gender inequity and discrimination pertaining to the harmful treatment and unfair distribution of opportunities, and privileges between individuals or groups based on their gender,
1
stands as a focal point, garnering emphasis on documenting it within various facets of medical and surgical training worldwide.2–5 Research consistently reveals the adverse impact of gender inequity on females throughout their medical careers compared to their male counterparts.6–9 Academic institutions globally grapple with various manifestations of gender inequity, encompassing physical, sexual, and psychological harassment.10–12 Strikingly, medical students appear to confront the highest prevalence of such disparities,
13
with nearly 95% of medical apprentices reporting encountering at least one form of inequity during their training.
14
While both genders may experience mistreatment, females bear a disproportionately higher burden of gender inequity, though instances affecting males are not uncommon.15,16 Gender-related inequities are conspicuous within medical specialties, with obstetrics and gynecology exhibiting marked gender discrimination that hinders mentorship, educational opportunities, and career pursuits, primarily impacting male medical students.
17
Conversely, the discipline of surgery is less conducive for female practitioners.18–20 These inequities are predominantly attributed to professors (43%) and clinical staff (48%).
21
Another publication highlighted the intertwined nature of diversity and wellness.
22
Despite contemporary society's strides in transcending gender-based inequity, medical graduates continue to grapple with gender-related disparities in the clinical settings,6,23 surpassing those encountered during pre-clinical education.
24
Our present study endeavors to examine clinical-year students’ experiences to provide a panoramic perspective on gender-related inequities and seeks to achieve the following objectives:
Ascertain the frequency of gender inequity encountered by medical undergraduates during each clinical clerkship within Karachi's medical colleges. Identify the forms and underlying causes of gender inequity within clinical clerkships and evaluate their impact on student's career choices. Examine which gender is predominantly susceptible to inequity during clinical clerkships and explore the negative psychological ramifications. Propose strategies to eradicate gender inequity within undergraduate clinical clerkships.
Materials and methods
Study setting, design, and period
This cross-sectional study involved clinical-year medical students (third, fourth, and fifth years) from both private and government medical colleges in Karachi-Pakistan. The study was conducted from September 10th to March 30th, 2022, following ethical approval from the Ethics Review Board of United Medical and Dental College. (UMDC/Ethics/2021/09/09/288-2022/07/03/306-2022/01/12/319/14/09/2023) All methods adhered to the most recent and relevant version of the Helsinki Declaration regarding human subjects in scientific research.
Sample size and sampling techniques
We determined a sample size of 357 using the Openepi finite sample size formula (n = deff Npq/[d^2/1.96]^2(N-1)+pq) at 95% confidence level and a 5% margin of error. This calculation was based on an estimated population size of approximately 5000 clinical-year students enrolled in government and private colleges in Karachi, awarding a Bachelor of Medicine and a Bachelor of Surgery (MBBS) degree approved by the Pakistan Medical Council (PMC). To ensure statistical significance, we expanded the final sample size to 430, anticipating a minimum of 26 participants from each college. We employed a simple-random-probability sampling technique, where each student was randomly selected from the student's list using the Giga calculator random name selector tool. 25 This approach reduced selection and participation bias. The student list was compiled with the assistance of students from each college. We chose the Giga random selector tool for its user-friendliness and to ensure the integrity of the selection process, eliminating any repetition that might occur when using Excel or another application.
Inclusion and exclusion criteria
This study included undergraduate medical students in their clinical-years of the MBBS program, aged between 18 and 30 years, enrolled in government and private Medical Colleges in Karachi. Exclusion criteria encompassed students in the first and second years of MBBS, students across all years of the Bachelor of Dental Surgery (BDS), Doctor of Physical Therapy (DPT), Pharmacy, and Nursing programs, as well as students with any documented psychological disorders or those who declined to provide written consent. Excluding students with psychological disorders from the investigation on gender inequity in clinical clerkships has multiple purposes. First, it helps maintain the integrity of the data and ensures adherence to ethical guidelines. Second, it safeguards the welfare of the participants, as including students with psychological disorders may potentially amplify their condition when they are asked about it.
Study tool, instrument validity and data collection procedure
We employed a self-administered, semi-structured questionnaire along with a consent form. The questionnaire was developed by the authors, drawing upon insights from prior studies15,18,21,23 (supplementary file 1) The questionnaire underwent validation by a panel of five members from the Ethics Board to ensure its validity, eliminate homogeneity, address double-barreled questions, and any writing or grammatical errors. Before initiating the study, a pilot study was conducted involving 30 students, with 10 participants from each academic year, to evaluate the questionnaire's timing, validity, and clarity. The questionnaire comprised two sections: Section-I consisted of five questions about students’ demographic characteristics, while Section-II included nine questions concerning gender inequity and discrimination during clinical clerkships and rotations. The survey commenced with written informed consent, followed by a verbal briefing about the authors, the study's objectives, the extent of their involvement, and the consequences of withdrawal or non-participation. Data collection was conducted face-to-face with students during their college hours to ensure a high response rate and enhance participant comprehension of the questionnaire.
Statistical analysis procedure
Responses were entered in an Excel spreadsheet and subsequently imported into IBM SPSS 23 for analysis. For categorical variables, we report frequencies and percentages. A Chi-square /Fischer Exact test is applied to assess the relationship or differences between variables. A p-value of <=.05 is considered statistically significant.
Gender and sex in the study: operational definitions and usage
‘Sex’ is defined as biological characteristics, encompassing traits such as reproductive organs, chromosomes, and secondary sexual characteristics, typically categorized as male or female. ‘Gender’ refers to the social and cultural roles, behaviors, and identities associated with being a man, woman, or another gender identity, extending beyond the binary concept of male and female. It is essential to clarify that in our study, ‘gender’ specifically denotes cisgender identities, where individuals’ gender identities align with the sex they were assigned at birth. Despite offering ‘other’ option in the questionnaire, participants in our study did not denote any other gender, indicating a predominantly cisgender sample.
Ethical consideration
Only the authors had access to the students’ lists compiled for the selection and administration phases. All personal information ie, name, email, and institution names about the total number of students and participants were securely discarded to ensure confidentiality and anonymity. Only the data regarding general demographic and gender inequity were utilized in this study.
Results
At the time of the study, 5000 students were enrolled in medical colleges in Karachi, encompassing the third, fourth, and fifth academic-years. Among these, females had a higher representation than males, with a ratio of approximately 3:1 (n = 3334; 66.68%:1666; 33.32%) (P-value = .000*). This gender distribution was consistent across institutional sectors, with the government accounting for one-third and the private encompassing two-thirds of the students.
Demographic data of students
Out of the 430 participants in the study, 123 (28.6%) were males, while 307 (71.4%) were females. The majority of participants, 302 (70.2%), were affiliated with the private sector, while the remaining 128 (29.4%) belonged to the government sector. Both male and female participants were 18-26 years old. Statistical analysis did not reveal any significant differences between male and female undergraduates regarding their current education status or the institutional sector. (Table 1)
Demographic characteristic of participants. (N = 430).

Frequency and experiences of gender inequity in each specialty and institutional sector
During clinical clerkships, a notable incidence of gender inequity was observed in 383 cases (89.1%), and 364 participants (84.7%) reported facing it. Both male and female students reported a similar prevalence of gender inequity, 56% each during gynecological and surgical clerkships. Likewise, male participants reported encountering gender inequity more frequently during gynecological clerkship, followed by surgical clerkship. Conversely, female participants reported the opposite. (Table 2)
Frequency and experiences of gender inequity in each specialty. (N = 430).
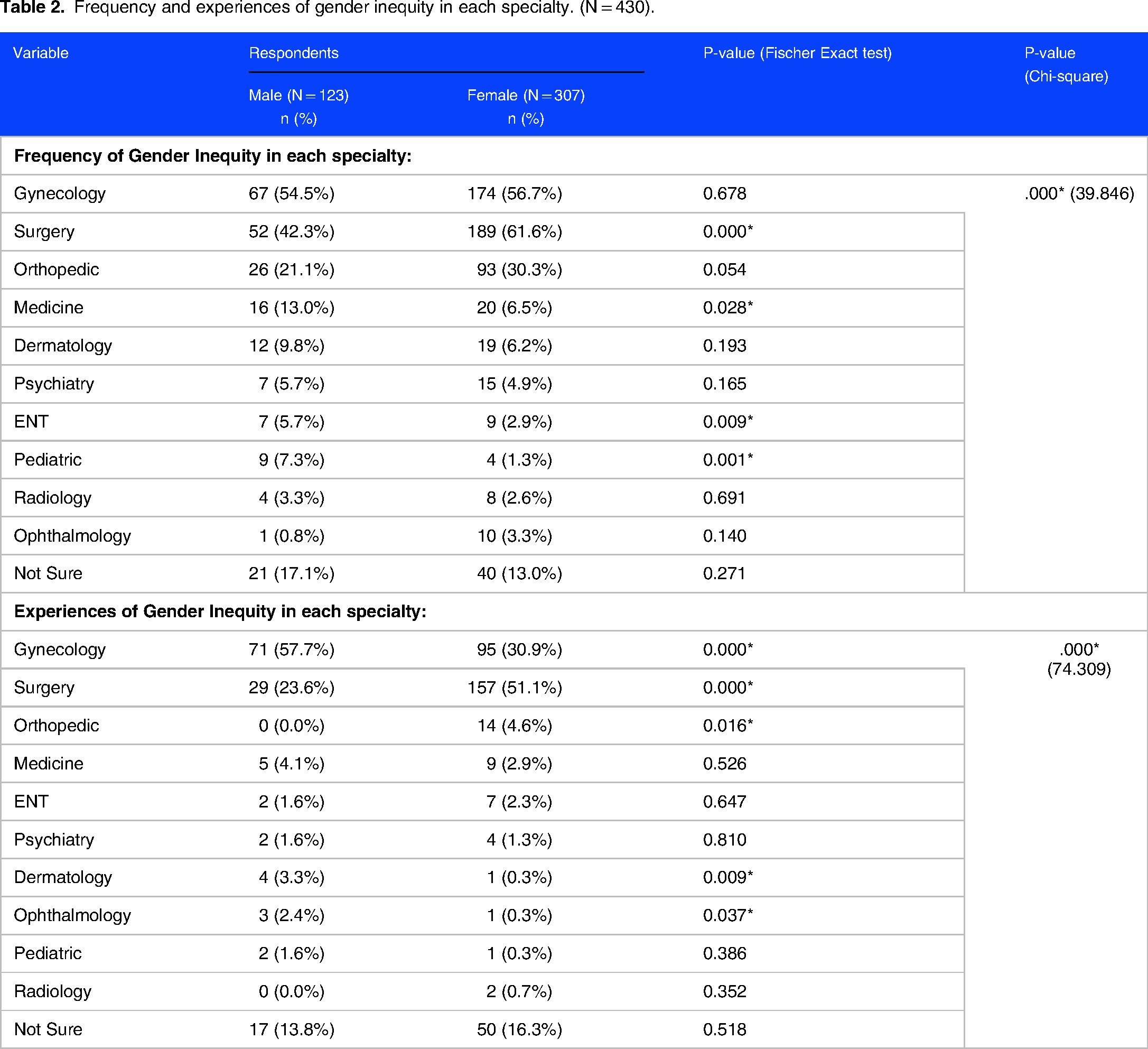
Equal percentages of gender inequity and discrimination were observed in both institutional sectors, with 80.4% (n = 103) in the government sector and 88.07% (n = 266) in the private sector. Notably, surgery (government n = 71; 55.5%; private n = 170; 56.3%) and gynecology (government n = 81; 63.3%; private n = 160; 53.0%) were identified as the primary specialties with pronounced gender inequity across institutional sectors (P-value = .004*).
Forms and reasons of gender inequity
Both male and female respondents commonly reported experiencing inequity in the form of a lack of respect from clerkship staff/professors and patients. This was followed by instances of mental harassment, inappropriate language, power harassment, indirect discrimination, sexual harassment, psychological harassment, direct discrimination, victimization, and physical harassment by staff/doctors and patients (Figure 1). The reasons behind this gender inequity were primarily attributed to patient preferences, societal mindsets, cultural norms, gender preferences by supervisors/instructors, and other factors (Figure 2). The Fisher's exact test showed, no statistically significant difference observed between male and female respondents in their reporting of forms of inequity. Nevertheless, noteworthy distinctions between genders were discerned in the reported reasons underlying such inequities.

Form of gender inequity practiced in clinical clerkships. (N = 430).

Reasons for gender inequity in clinical clerkships. (N = 430).
Impact of gender inequity on career selection
Those participants who reported experiencing or witnessing gender inequity during clinical clerkships indicated that it had influenced their career choices. This influence was statistically equivalent for both male and female students. (Figure 3)
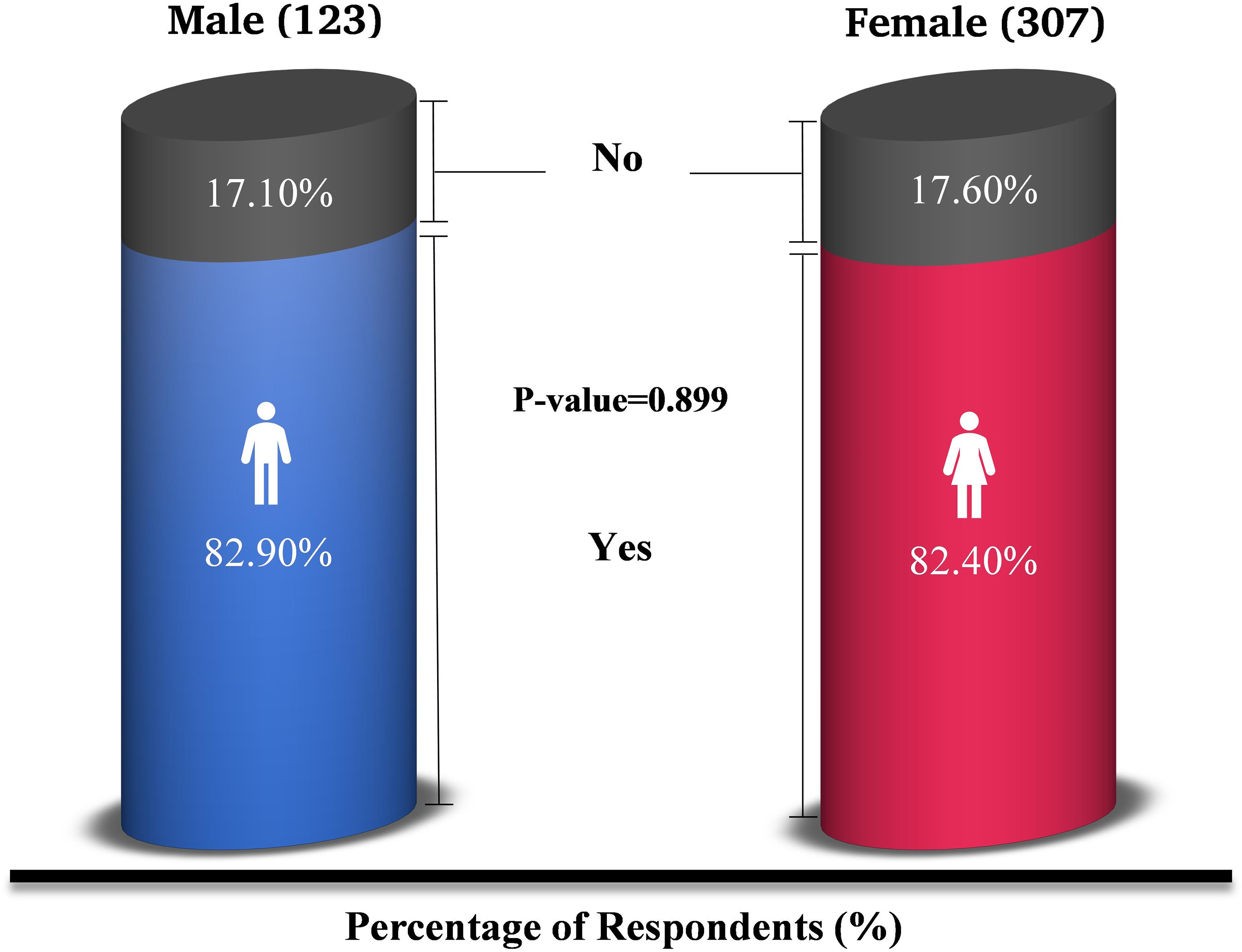
Impact of gender inequity on career selection. (N = 430).
Gender predominance, reporting and psychological effect
A significant proportion of students reported that both genders experienced gender inequity equally, followed by females and males predominantly. Similarly, most students (n = 283; 92.2%) did not report these incidents to relevant authorities due to fear and instead accepted the status quo. The results are statistically significant according to Chi-square test. A significantly higher number of individuals from both genders reported that gender inequity had a significant negative psychological impact on their mental state, leading to feelings of demotivation (78.1%), poor self-esteem (67.2%), helplessness/hopelessness (48.6%), and frustration (45.8%). (Table 3)
Gender pre-disposed to inequity, report to authorities, and negative psychological impact of gender inequity. (N = 430).

Strategies to overcome
Following are the strategies indicated by participants to overcome gender inequity in clinical clerkships. (Table 4) The predominant strategies include giving equal opportunities to both genders (73.3%), appreciating both genders (63.7%), and having the right attitude of professors and clinical staff towards students (52.8%).
Strategies to overcome gender inequity in clinical clerkships. (N = 430).

Discussion
Our survey revealed that gender inequity was observed by participants in clinical clerkships 89.1% of the time, with 84.7% reporting personal experiences. In contrast, prior studies by Hashmi AM et al 21 in a single private medical and dental college in Lahore, Pakistan, and by Bruce AN et al 2 in the United States among female students reported experience rates of 78% and 87%, respectively. These findings align with our results but are notable because they did not distinguish between pre-clinical and clinical-years; our study found it prevalent in clinical-years. Furthermore, our study had a multi-institutional focus and its use of a comprehensive gender perspective, aspects not addressed in the aforementioned studies.
Our study also highlighted two clinical clerkships, gynecology and surgery, as having the highest rates of gender inequity, at 56% each. An intriguing observation was that male and female students reported similar experiences in these clerkships, with 54.5% and 56.7% for gynecology and 42.3% and 61.6% for surgery. These findings contrast with a study conducted by Zahid AZ et al, 26 which reported 87% of male students experiencing inequity in gynecology clerkship, and Janjua MB et al, 18 who found 61.3% of females reporting gender-discrimination in surgical training. The discrepancies might stem from variations in the country's income level, the educational stage at which the studies were conducted, and evolving trends over time. Our analysis also revealed that gender inequity was equally prevalent in government and private institutions (80.4%; 88.07%). This finding is significant, as prior studies are predominantly concentrated on private institutions.2,18,21,26
Our study identified several prevalent forms of gender inequity. These included a lack of respect (48.8%), instances of verbal and inappropriate language (28.6%), and mental harassment (28.8%) from various individuals such as staff, professors, supervisors, and patients. These findings are consistent with a systematic review and meta-analysis by Fnais N et al, 10 which highlighted verbal harassment (63.0%) at the postgraduate level and unethical communication (43.6%) among undergraduates by Hashmi AM et al 21 are the most common forms. The similarities and minor variations in the presentation of gender inequity may be attributed to the unique blend of theoretical and clinical learning environments in undergraduate clinical clerkships, providing new insights. The reasons for gender inequity included patient/professor/instructor/staff preferences, Pakistani cultural norms, and societal mindsets, in line with the study conducted by Devine PG et al 27 This suggests that deeply ingrained habits result from socialization, particularly learned and experienced behaviors shaped by cultural and societal norms. Addressing these underlying factors is crucial for eradicating gender inequity.
One of the significant findings is that most students (59.3%) perceive that both genders are equally exposed to gender inequity in clinical clerkships. This observation contrasts with the prevailing notion in many other studies, which commonly assert that females are more susceptible to gender inequity, particularly within the medical field.28–30 This divergence in perception may partly arise from the vulnerability of students as easy targets for inequity and the heightened prevalence of gender inequity at the undergraduate-clerkship level compared to the postgraduate and pre-clerkship stages. Importantly, our findings suggest a shift in recent years, where gender inequity and discrimination have moved from being female-centric to affecting both genders equally. This shift has implications and merits further investigation. Prior studies have primarily focused on postgraduates and females.
Another alarming observation was that 92.2% of students did not report gender inequity to the college authorities, citing fear or acceptance of the status quo as reasons, comparable with Hashmi AM et al 21 study at 83.3%. This reluctance to report is concerning as it perpetuates the issue. Furthermore, a significant discovery arises from the adverse impact of these experiences on students’ career decisions. This impact manifested in 82.90% of male and 82.40% of female students. Consequently, affected students exhibited a negative psychological-toll, with 45% to 80% reporting demotivation, poor self-esteem, feelings of helplessness/hopelessness, and frustration. This psychological impact appears to be more pronounced compared to previous studies, 21 attributed to the heightened influence of the clinical setting on students’ mental well-being.
Numerous studies have proposed strategies to address gender inequity in postgraduate settings,31–33 but there is a notable gap at the undergraduate level. Our study proposes strategies to reduce and potentially eliminate gender inequity within clinical clerkships. Both students and institutions can play pivotal roles in achieving this goal. Promoting equal opportunities, supporting the advancement of students into senior roles regardless of gender, and establishing fair hiring practices are key approaches. This will foster appreciation for the contributions of all genders and eliminate the perception of preferential treatment. Cultivating a positive attitude among professors and clinical staff towards all genders through periodic interventions, empowering students to report such issues through a secure online reporting system or monthly scrutinizing questionnaires which not only enhances student protection, supported by numerous studies34–37 but also contributes to addressing the problem of underreporting such incidents, and implementing transparent anti-discrimination/anti-inequity policies are vital. Additionally, screening professors and staff for their commitment to equity during the hiring process and actively working with current faculty to promote gender-equity can contribute to addressing the root causes of the problem. Lastly, a national initiative to foster a culture of meritocracy and diversify the governing boards of medical institutions, led by relevant national authorities, represents a potent tool for eradicating gender inequity and discrimination.
While our findings may not initially appear groundbreaking, this study represents a pioneering examination of gender inequity during undergraduate clinical clerkships, emphasizing its origins and impact on students’ career choices. Addressing them during undergraduate education is crucial to eliminating gender inequity at the professional level. Our research is significant because it highlights that many students encounter these problems, demonstrating their potential to influence career decisions and perpetuate the issue across generations. Additionally, this challenge is exacerbated by doctors from low- and lower-middle-income countries, like Pakistan, who have experienced these inequities and seek education and employment in middle- or high-income countries, 38 potentially sustaining and exacerbating the problem in new settings, as human nature tends to reflect those traits that they experienced. Therefore, our research hopes to tackle this persistent issue at its root, ultimately ending its decades-long existence.
A limitation of our study is the exclusion of DPT, BDS, and Pharmacy students, who undergo similar clinical settings but may yield slightly different outcomes than MBBS students due to variations in their final years. However, a study in Pakistan found no significant differences in experiences among these student groups. 21 Additionally, our study was conducted in a lower-middle-income country. While our findings align with postgraduate studies showing similar outcomes across different income nations,2,4,16–18,21,39 results could vary in middle-to-high-income countries. Our study primarily featured students from private medical institutions (3:1 ratio) rather than government institutions. This composition's impact on results may vary in countries with different institutional sector proportions. Nevertheless, our findings remained consistent across both sectors, underscoring the issue's widespread nature. One noteworthy limitation of our study is the use of binary gender classification. This simplification was necessitated by the absence of alternative gender categories in the responses obtained, historical precedent in prior studies, and the current state of knowledge regarding gender diversity in Pakistan, which facilitated straightforward data analysis, allowing meaningful comparisons between male and female students. It is crucial to acknowledge that this binary categorization may not fully encapsulate the intricate spectrum of gender identities, as gender is a multifaceted spectrum, encompassing an individual's self-identified sense of being male, female, or another gender, distinct from physical and biological sex, which may not align with their assigned sex at birth. 40 Additionally, we did not consider factors like race, caste, religion, or ethnicity, which could influence gender inequity in clinical clerkships.
Conclusion
In conclusion, our study illuminates the frequency of gender inequity within clinical clerkships in Pakistan's medical colleges, affecting both male and female students equally. This revelation significantly impacts students’ career choices and professional advancement in medical specialties. Clinical years play a pivotal role in shaping students’ morals and professionalism, as individuals tend to assimilate the traits they have experienced over time. Our findings underscore the need for a paradigm shift in addressing the root cause at the undergraduate clinical clerkship level. Implementing our proposed solutions, in collaboration with relevant authorities, can help reduce and eventually eliminate gender inequity in undergraduate education, potentially creating lasting change within the next five to ten years. Furthermore, our research also provides a foundation for other countries to address gender inequity at the appropriate educational level, promoting equitable opportunities in the field of medicine.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241257401 - Supplemental material for Gender Inequity in Clinical Clerkships and its Influence on Career Selection: A Cross-Sectional Survey
Supplemental material, sj-docx-1-mde-10.1177_23821205241257401 for Gender Inequity in Clinical Clerkships and its Influence on Career Selection: A Cross-Sectional Survey by Muhammad Hamza Dawood, Mavra Roshan, Muhammad Daniyal, Sheza Sohail, Haseefa Perveen and Umair Ul Islam in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241257401 - Supplemental material for Gender Inequity in Clinical Clerkships and its Influence on Career Selection: A Cross-Sectional Survey
Supplemental material, sj-docx-2-mde-10.1177_23821205241257401 for Gender Inequity in Clinical Clerkships and its Influence on Career Selection: A Cross-Sectional Survey by Muhammad Hamza Dawood, Mavra Roshan, Muhammad Daniyal, Sheza Sohail, Haseefa Perveen and Umair Ul Islam in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank Dr Omer Bin Khalid Jameel, Khadijah Abid, Lailamah Rehman Sherani and Abdullah Akmal Minhas for study design, initial analysis, and data collection of the study, respectively, without compensation for their contribution. The author wishes to express profound gratitude to Dr Faisal Khosa (MD, MBA, FFRRCSI, FRCPC), affiliated with the Department of Radiology at Vancouver General Hospital, located at 899 W 12th Avenue, Vancouver, British Columbia, Canada. Dr Faisal Khosa, a distinguished recipient of the Michael Smith Health Research BC Award for the years 2023 to 2028, the Don Rix Physician Leadership Lifetime Achievement Award in 2022, and the Radiology Department, University of British Columbia Excellence in Equity, Diversity & Inclusion Award in 2023, played an invaluable role in providing guidance, corrections, and oversight during the preparation of this manuscript. The authors also acknowledge the Research Council of Pakistan for their support and assistance in the study.
Author's Contribution
MHD is the guarantor of this study. Concept and design: MHD. Acquisition, analysis, or interpretation of data: MHD, MR, MD, SS, HP. Drafting of the manuscript: MHD, MR, SS, HP. Critical revision of the manuscript for important intellectual content: MHD, MR, MD, SS, HP, UUI. Administrative, technical, or material support: MHD, UUI. Statistical analysis: MHD. Supervision: UUI.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study proposal was approved by the Institutional review board (IRB-Committee) of United Medical and Dental College at Karachi city (Ref. No: UMDC/Ethics/2021/09/09/288-2022/07/03/306-2022/01/12/319/14/09/2023). Participants gave written consent to participate in the study before taking part.
Data sharing
The study's datasets, which safeguard participant anonymity and uphold the confidentiality of responses, are not publicly available. Interested parties can request access from the corresponding author, with data sharing occurring only when essential and with identifiable information removed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.