
Abstract
OBJECTIVES
Medical schools considering longitudinal integrated clerkships (LICs) have access to literature that provides recommendations for planning, implementation, and sustainability. However, LIC development and implementation remain notoriously challenging. University of Utah’s LIC development process was informed by the documented experiences of long-established LIC programs. A literature gap was identified pertaining to more recently implemented LICs. The aim of this study was to explore the experiences of faculty in the early stages of LIC development.
METHODS
Thirteen representatives from eight LICs implemented after 2015 participated in 2 Zoom focus groups (5 participated in the first and the other 8 participated in the second). Participants were asked questions to assess key supports, barriers, and recommendations. Following the focus groups, participants were asked to rank the responses based on their level of importance.
RESULTS
Highest ranked supports included stakeholder and partner involvement; a dedicated coordinator or team; and strong, committed leadership. Highest ranked barriers included difficulty recruiting preceptors and clinical sites; underestimation of the amount of work required to coordinate the LIC; and challenges in providing the needed faculty development. Top recommendations for new LICs included investing in the needs of clinical partners; staffing or assigning a dedicated coordinator early in the development and implementation process; and frequent communication with all stakeholders.
CONCLUSION
Despite variation among the types of new LICs represented, there was consensus among participants on the importance of key supports, barriers, and recommendations. Knowledge of these factors can help new schools plan and allocate resources during their LIC development process. Participants found the focus group process and follow-up discussions useful and have formed an ongoing workgroup which meets quarterly.
Introduction
While undergraduate medical education varies across schools, third-year medical students typically move out of the classroom and begin an intensive clinical education. These students are often assigned to traditional block rotations (TBRs) in which they engage in a series of brief (eg, 4-8 weeks) clinical placements within different disciplines (eg, pediatrics, family medicine, obstetrics/gynecology, surgery, internal medicine, psychiatry). Students are immersed sequentially in each discipline and work with clinical faculty within each specialty before moving on to the next rotation. An alternative to the TBR model is the longitudinal integrated clerkship (LIC) model. In an LIC, students engage with multiple specialties simultaneously, for less time per specialty in any given week, but over a longer period of time (the full length of the LIC). LICs allow for an educational experience that is grounded in longitudinal relationships with preceptors, patients, peers, places, and pedagogy.
In the half-century since LICs began emerging as alternatives to TBRs in clinical medical education, a great deal of literature has been published on this model. The model's types and program logistics have been described,1–10 along with considerable benefits. Benefits for students include closer relationships with preceptors11–17 and higher quality of feedback3,11,14,15,18–20; professional identity development11,12,21–23; and academic outcomes, clinical experiences, skill, and confidence.2,13,15–17,19,24–33 LIC students are more likely to enter primary care24,34–37 or rural practice15,23,37–39; and demonstrate greater patient-centeredness.15,19–21,40,41 Benefits have also been shown for patient satisfaction and perceived patient health benefits42–46; as well as preceptor satisfaction.8,14,27,47,48 Additionally, recent review articles have compiled recommendations for planning, implementing, and sustaining LICs.7,10,49–52
LICs represent a significant departure from the TBR model in which most faculty and clinicians completed their education. Additionally, the training and logistics within most existing clerkships have been designed around the TBR model. Accordingly, the initiation of a new LIC remains a complex and difficult process that bears continuing investigation. Moreover, much of the literature focuses on important factors for ongoing program and student success rather than those factors critical in early-stage LIC implementation. In their 2021 literature review, Hense et al noted that although they originally wanted to focus on barriers and facilitators of LIC development in the early implementation phase, most studies they reviewed did not indicate where they were in the development process. 50 Bartlett et al's 2020 review intentionally gave more weight to longer-running programs, as these have demonstrated sustainability. 7 Additionally, many of the studies in recent reviews were published more than 10 years ago.1,7,10,49,50 Brown et al (2019) note a “relative dearth of recent literature” on factors enabling LIC success. 49 Given the rapidly evolving landscape of undergraduate medical education, including the accessibility of guidance from literature and faculty from well-established LIC programs, we undertook a qualitative study of the factors affecting the early phases of LIC development and implementation.
Previous Findings
The literature on LIC implementation includes factors relevant to the initial development of LICs as well as ongoing LIC success. During the early development stages, the literature indicates that medical schools need to determine their goals and objectives in choosing the LIC model, and based on these, make informed decisions regarding the type of LIC to be adopted (eg, amalgamative, blended, or comprehensive 1 ), setting and duration of the LIC, and percentage of students who will participate in the LIC.7,10,49 Other factors that should be considered at the outset include how the LIC will integrate with the broader curriculum, including online resources7,10,51,53; how the LIC will recruit and support students, mentors, and clinical sites4,7,10,50,54; and how assessment, evaluation, and quality assurance will be managed.7,10,49–51 Significant time and resources must be allocated to the development process.7,49,50,53,54
The same considerations that are important for the ongoing success and sustainability of LICs seem likely to be important for successful development and initiation. These include recruiting and preparing engaged students7,26,49,55 and enthusiastic preceptors7,49,52,54,55; eliciting and responding to evaluation data and stakeholder feedback7,49,51,53; securing strong support from school of medicine and clinic leadership2,3,7,10,49,53,55; encouraging student sense of belonging at clinical sites7,26,49,55; facilitating use of the Electronic Health Record system and notifications to enhance continuity with patients19,49,51; engaging in cross-disciplinary collaboration3,49; providing professional development and other support to preceptors2,4,7,10,17,49,51,53,54; and ensuring the program provides mutually beneficial outcomes to both academic and clinical partners.2,7,50 Barriers to ongoing success and sustainability include failure of faculty to adapt to a different style of teaching7,49,50,54; student isolation in remote placements7,17,49,50; and conflict or poor match between student and preceptor.10,49 Recruitment of new faculty and clinics not accustomed to teaching can present challenges3,4,8 and recruitment of faculty and clinics that already work with traditional block students can present a different set of challenges.4,10,49 Costs associated with LICs may be daunting, both in terms of added expenses for students placed in remote locations and costs of faculty time for developing and running the LIC. Research suggests that these expenses may be recovered through eventual benefits to the teaching clinics and their larger communities.10,49–51,56–59
While the aforementioned works shed light on previously reported factors related to LIC development, faculty at the Spencer Fox Eccles School of Medicine at the University of Utah were interested in exploring the experiences of programs that had initiated LICs in the last 5 years in hopes of identifying the most important facilitators, most challenging barriers, and top recommendations from a group of early-stage LICs. An ongoing understanding of these factors is needed to inform evidence-based LIC development, particularly as this model continues to be an increasingly popular approach to undergraduate medical education worldwide.
Methods
Participant recruitment
Faculty and staff of LICs were eligible to participate if they were implementing an LIC in the United States that was initiated less than 5 years ago or was still in the development stage. There were no other inclusion or exclusion criteria. To identify LICs established within the last 5 years, we first downloaded the listing of all LIC programs provided on the website of the Consortium of LICs (CLICs). 60 We identified 45 LIC programs located in the United States. If the LIC initiation year was not included in the program listing, we reviewed program websites to determine their start date or anticipated start date. (If the program website did not provide the initiation year, the program was removed from consideration.)
Ten LICs established in 2016 or later were identified, and leadership from nine of those programs were able to be reached via email or phone and invited to participate in a 1.5-h focus group. Five of these nine LICs participated. Additionally, the University of Utah participated in an ad hoc group of 10 medical schools awarded Value-Based Medical Student Education Training Program grants from the Health Resources and Services Administration (HRSA) in 2020. Seven of these grantees (including the University of Utah) were developing LICs and were also invited to participate. Three of these seven LICs participated. Thus, staff from 16 LICs were invited and 8 LICs participated (13 individual participants). Reasons for nonparticipation included lack of time and being too early in the development process to have information to contribute. Figure 1 illustrates our recruitment process. Table 1 shows that participating schools varied in terms of their LIC length, focus, and percentage of students participating.
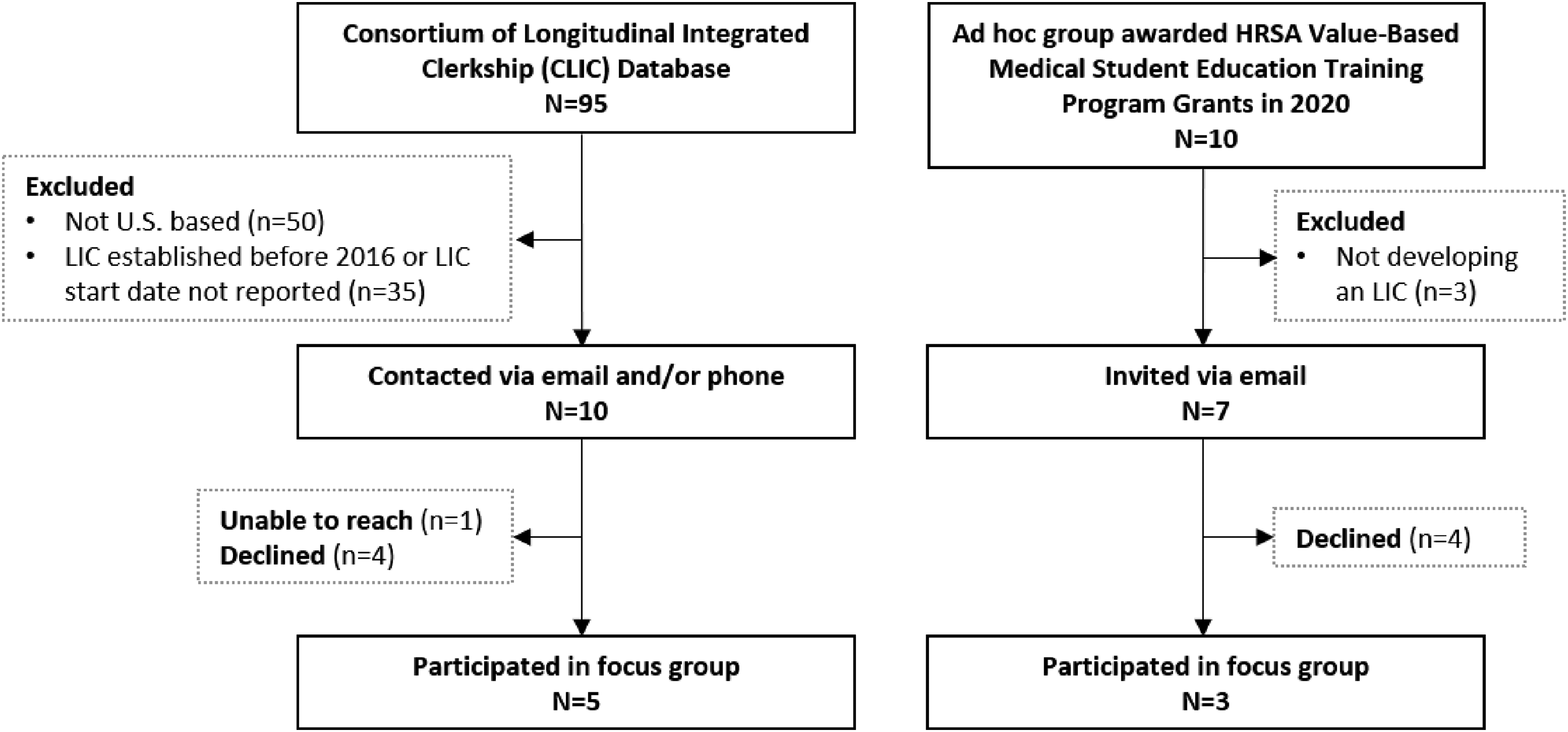
Consolidated criteria for reporting qualitative research (COREQ) diagram.
Participating new LICs.

LIC, longitudinal integrated clerkships.
Data Collection
Two 1.5-h focus groups were held over Zoom in June 2021. Five participants attended the first session, and the remaining eight participants attended the second. Both sessions were recorded. The three questions posed to the members of each focus group were:
What have been key supports or key actions which have supported or led to your successful LIC launch? What significant barriers have been encountered in your LIC implementation process? What recommendations do you have for those seeking to start an LIC (which would be helpful in successful implementation)?
We used a modified nominal group process (see Figure 2).61,62 Participants were emailed the questions beforehand, and asked to consider their responses prior to the focus group. During the focus group, answers to each question were solicited from participants in a round-robin fashion. A moderator summarized each answer on a shared screen and asked for clarification as needed. During the focus groups, SG led the discussion and SKE summarized participant answers. LLB was a participant in the first focus group as the LIC Director of the University of Utah Spencer Fox Eccles School of Medicine. Once participants had no more answers to share for a given question, they were given time to review the written summaries and select the 2 answers that they felt were most important. Once everyone made their selections, they shared their choices with the rest of the group. (In the first focus group, participants shared their selections privately with the moderator using the chat feature, and the moderator summarized the results back to the group. During the second focus group, the chat feature was inadvertently disabled, so participants shared their selections out loud to the full group.)
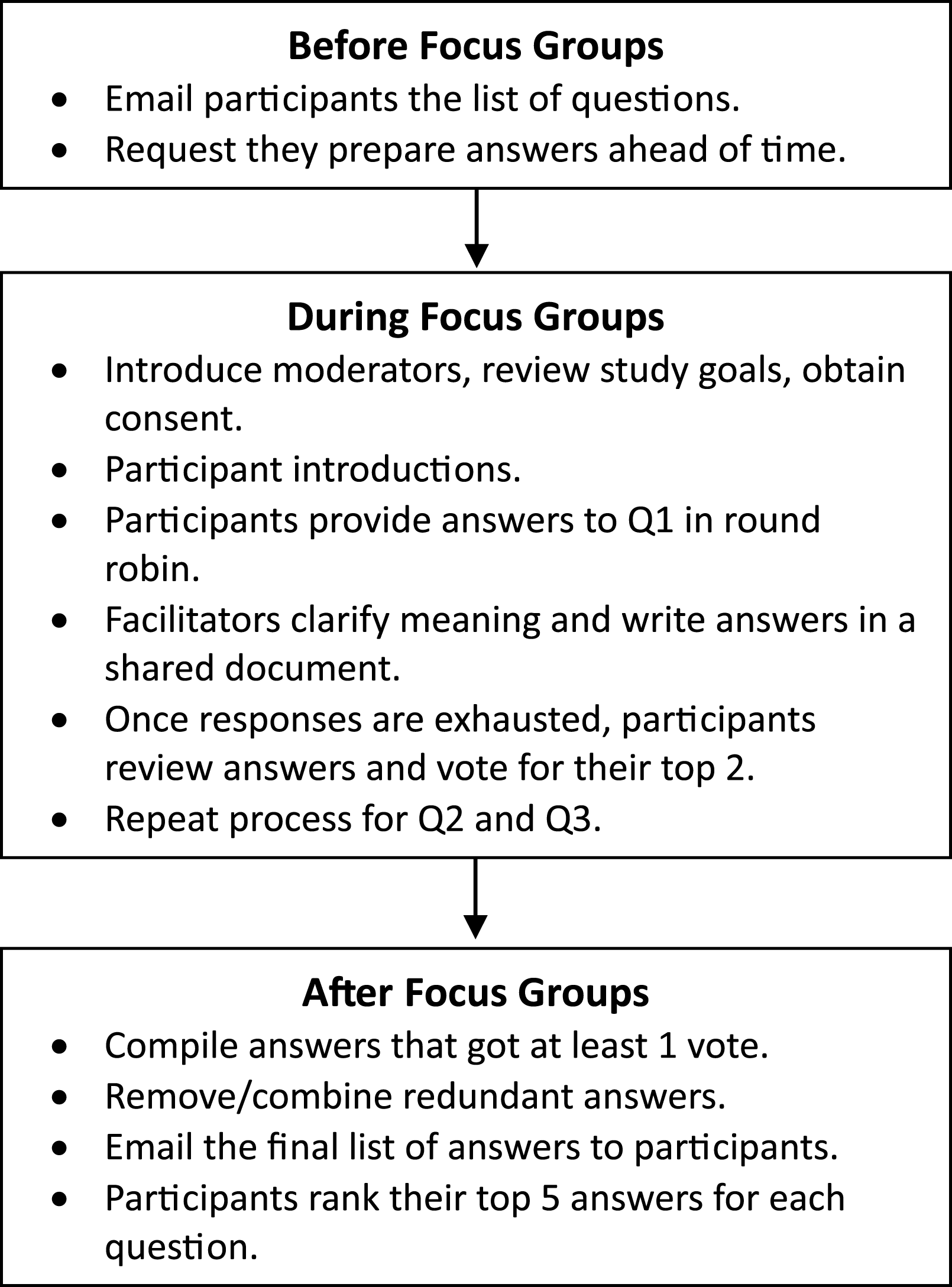
Modified nominal group process.
Due to time constraints, after each initial vote, we did not have the customary discussion and final vote. Instead, following the second focus group, the authors compiled all of the responses that received at least one vote across the 2 groups. Participants were asked via email to rank order what they felt were the top 5 most important answers to each question. All 13 focus group participants provided their final rankings.
Data Analysis
Because the researchers summarized the focus group responses during the focus group and the participants provided clarification as needed, we were confident that the written summaries accurately captured the participants’ sentiments. However, because participants had prepared their answers in advance, in many cases there were similar answers provided by multiple respondents, both within and across the 2 focus groups. Therefore, prior to sending the responses back to the participants for their final ranking, SKE and SG combined similar answers from both focus groups into concise statements to prevent redundancies from diluting the ranking process. Table 2 provides an example of multiple statements combined into a single item for ranking. Once all 13 respondents had submitted their rankings, the percentages of participants who ranked each answer in their top 5 were calculated and graphed.
Example of combined statements.

LIC, longitudinal integrated clerkships.
Despite a small sample size, our methodology, and the content of the participants’ answers gave us confidence that we were able to reach saturation of the most important supports, barriers, and recommendations for new LIC implementation as experienced by these participants. The nominal group method encourages participants to spend time prior to the focus group thinking about their answers. Additionally, the round-robin format ensures that all participants have an opportunity to provide their answers. We did not end the discussion of any question until all participants indicated they had provided all their answers. Most importantly, there were redundancies among the answers both within and between the groups that indicated we had reached data saturation. 63
Ethical Considerations
This study was determined to be exempt by the Institutional Review Board of the University of Utah (IRB_ 00141272) in 2021. Participants were informed of the study purpose, questions, and procedure prior to the focus groups. Verbal consent was obtained at the beginning of both focus groups with the approval of our IRB because the study presented no more than minimal risk of harm to subjects and involved no procedures for which written consent is normally required outside of the research context.
Results
Key Supports for Successful Launch of an LIC
The first question discussed in the focus group addressed key supports or actions that supported the successful launch of the LIC. The first group (5 participants) provided 15 key supports, and the second group (8 participants) provided 23 key supports. The vote tallies taken during the Zoom group for this question in both groups revealed diversity in opinions about the most important key supports, with the majority of key supports receiving only one vote. The final key supports are provided in Figure 3, along with the frequency with which respondents ranked each factor in their top 5. Table 3 provides additional information about each factor as well as additional supports that were not ranked as top factors.

Percentage of respondents who ranked each key support in their top 5.
Details about key support.

LIC, longitudinal integrated clerkships.
Significant Barriers Encountered During LIC Implementation
The second question discussed in the focus group addressed significant barriers to the successful launch of the LIC. The first group provided 17 barriers, and the second group provided 22 barriers. The vote tallies taken during the first group showed diversity in opinions on the most important barriers. The vote tallies in the second group showed more convergence in opinions, with all respondents voting for preceptor and clinical site recruitment and 5 of the 7 participants voting for underestimating coordination work. This convergence was also seen in the online rankings of the responses. Figure 4 provides the responses that received at least one vote, and the percentage of respondents who ranked each factor in their top 5 after the focus groups. Table 4 provides additional information about each factor as well as additional barriers that were not top factors.

Percentage of respondents who ranked each barrier in their top 5.
Details about barriers.

LIC, longitudinal integrated clerkships.
Recommendations for Starting an LIC
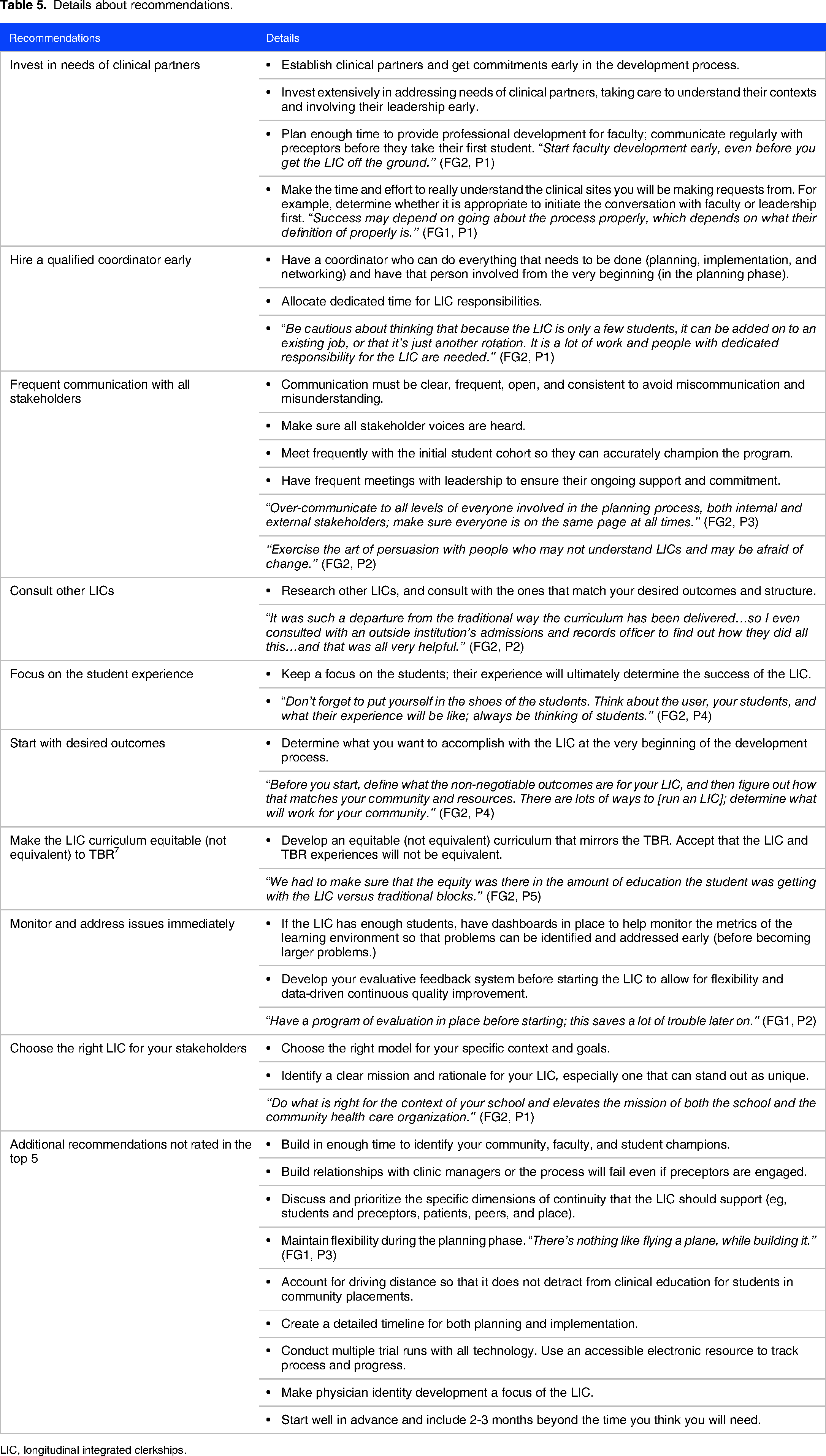
The final focus group question addressed recommendations for the successful launch of the LIC. The first group provided 14 recommendations, and the second group provided 21 recommendations. As with the first question, the vote tallies taken by both groups showed diversity in opinions about the most important recommendations. Figure 5 provides the combined recommendations that received at least one vote, and the percentage of respondents who ranked each factor in their top five after the focus groups. Table 5 provides additional information about each factor as well as recommendations that were not top factors.

Percentage of respondents who ranked each recommendation in their top 5.
Details about recommendations.
LIC, longitudinal integrated clerkships.
Discussion
Overall, our qualitative research indicates that the challenges described in earlier studies continue to apply, and lead to a conclusion that was woven throughout the study regarding facilitators, barriers, and recommendations: The early stage of LIC development takes a significant amount of time, generally more than anticipated, and needs to be resourced accordingly. Moreover, having those resources and staff in place early in the process was strongly recommended.
While there was general consensus around the key supports, barriers, and recommendations, there was divergence in participants’ votes regarding the most important factors. The greatest convergence was found among barriers. All of the participants selected preceptor and clinical site recruitment and all but one selected underestimating the amount of time and effort needed to develop and launch an LIC as a top barrier. These two barriers are not unrelated, considering the time and effort participants described as necessary for the preceptor recruitment process. The minor divergences in importance ratings represent the unique context of each school of medicine. Despite dissimilarities in the top two rankings of supports and recommendations collected during the focus group, participants agreed that the factors discussed were relevant to their programs. During the focus group, it was clear that participants could relate to all of the key supports, barriers, and recommendations.
Across the three categories, the majority of the factors listed as most important were related to human capital. As the LIC is fundamentally a model of learning through relationships,26,53 it makes sense that relationships with stakeholders form the backbone of the early development process. Within this overarching topic of relationships were contributing factors of good relationships: frequent communication, investment of time, and reciprocity in terms of needs and priorities. Participants also noted the importance of repetition of a consistent message and updates as changes occur to avoid misunderstandings. Despite the increasing popularity of the LIC model, a lack of understanding of the model persists, even among medical school faculty, but especially among clinical partners.
Limitations
This study limited participation to new LICs located in the United States, in order to increase the likelihood of finding consensus. While there are likely common issues for new LICs regardless of location, medical schools considering LICs in other geographical areas may have different barriers, facilitators, and recommendations based on their specific local and cultural contexts. Additionally, while the current study included LICs with a range of characteristics in terms of length, size, focus, and percentage of students in the LIC, we did not have enough participants to be able to draw conclusions about different subtypes of LICs.
Next Steps
Preliminary results were presented virtually and discussed at the CLICs 2021 Conference in Stellenbosch, South Africa. 64 Subsequent efforts led to a collaboration of several participating medical schools on a Personally Arranged Learning Session (PeArL) on recruiting, retaining, and supporting preceptors in the early stages of LICs at the CLIC 2022 Conference in Limerick, Ireland, 65 as well as a roundtable discussion on community preceptor recruitment for LICs at the Society of Teachers of Family Medicine (STFM) 2023 Conference on Medical Student Education in New Orleans. 66
After the initial focus groups were held, we realized there was an opportunity for a continuing workgroup to problem solve and support one another in their early stage LIC implementation. We invited participants to continue to meet over Zoom on a quarterly basis. LIC staff from all eight schools have continued to participate, as well as a faculty member from another school who joined after hearing about our project at the 2021 CLIC conference. Discussion topics have included barriers and strategies for preceptor recruitment; how the LIC model compares to the TBR model in terms of the numbers of preceptors needed and the amount of time precepting requires of preceptors; administrative staff-to-student ratios needed for LICs; and how to engage preceptors in professional development and how much professional development to provide. Additional research is needed on the critical factors in early stage implementation of LICs, including expanding the geographical scope and comparing different subtypes of LICs.
Conclusions
The early stages of LICs continue to be challenging. While there was divergence in the participants’ preliminary votes regarding the most important supports, barriers, and recommendations, there was consensus regarding the final importance rankings of each of these factors. These findings demonstrate both the commonality of the issues in the LIC development process and the uniqueness of the specific needs and challenges in early-stage implementation within each LIC. Knowledge of these factors can help new schools allocate resources during their LIC development process. Participants found the focus group process and follow-up discussions useful and have formed an ongoing workgroup to meet quarterly.
Authors’ information
SG (MS, PhD, MPH) is an Adjunct Professor in Family and Preventive Medicine at the University of Utah Spencer Eccles Fox School of Medicine. He is also a Professor Emeritus at East Stroudsburg University of Pennsylvania. At the time of this study, he served as the lead program evaluator for the Health Resources and Services Administration (HRSA) grant-funded Value-Based Medical Student Education and Training Program. He has extensive experience with mixed methods program evaluation, including teaching research methods and statistics to Public Health graduate students.
SKE (PhD) is a Research Associate at the University of Utah Spencer Eccles Fox School of Medicine and the Evaluation Manager for the HRSA grant. She has extensive experience with mixed methods program evaluation.
LLB (MD) is a practicing pediatrician. At the time of the study, she was the LIC Director and clinical faculty at the University of Utah Spencer Eccles Fox School of Medicine.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231217894 - Supplemental material for Qualitative Findings of a Nominal Group Process to Identify Critical Factors in New LIC Implementation
Supplemental material, sj-pdf-1-mde-10.1177_23821205231217894 for Qualitative Findings of a Nominal Group Process to Identify Critical Factors in New LIC Implementation by Stacy K. Eddings, Laura L. Brown and Steven Godin in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231217894 - Supplemental material for Qualitative Findings of a Nominal Group Process to Identify Critical Factors in New LIC Implementation
Supplemental material, sj-docx-2-mde-10.1177_23821205231217894 for Qualitative Findings of a Nominal Group Process to Identify Critical Factors in New LIC Implementation by Stacy K. Eddings, Laura L. Brown and Steven Godin in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The researchers wish to thank all of the focus group participants for their time and their insightful answers to our questions. We would also like to thank the three anonymous reviewers who provided valuable feedback on our initial draft.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimers
The views and content are those of the authors and not an official position of their institutions or funder.
FUNDING
This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of the Value-Based Medical Student Education and Training Program (#T99HP39203) award totaling $17,644 661 with 10% financed with nongovernmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS or the U.S. Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.