
Abstract
OBJECTIVE
This study assessed 2 modalities for teaching responsible conduct of research and human subjects protection (RCR/HSP) to surgical residents in Guatemala—an “off the shelf” online curriculum and a new in-person curriculum specific to the local context.
METHODS
In 2018, 160 surgical residents in 3 large urban hospitals in Guatemala City completed 2 online programs in RCR/HSP. Residents in the intervention arm also completed 7 weeks of in-person training. Pre- and post-assessments tested awareness of key concepts with particular attention to international and Guatemalan research regulations. Group differences in matched (pre- and post-) mean scores were analyzed using t-tests.
RESULTS
One hundred forty residents completed pre- and post-training assessments and were included in the analytic sample. Overall mean scores improved modestly from 52.7 to 58.7 points out of 100. Intervention-arm trainees reported greater confidence in recognizing ethical issues, understanding legal and ethical requirements for research, and identifying, reporting and avoiding scientific misconduct than control-arm trainees.
CONCLUSION
Given the limited availability of RCR/HSP faculty, financial resources, and time in the surgical training schedule, the investigators recommend that academic authorities in Guatemala consider online training programs in RCR/HSP in all surgical residency programs as an affordable and scalable strategy to build ethical research skills in its surgical workforce. Investment in human resources to support in-person ethics education as a way to build self-efficacy in ethical decision-making should be considered.
Keywords
Introduction
While responsible conduct of research and human subjects protection (RCR/HSP) training programs can vary significantly in content, they share the common goal of building competency in human subject protections, understanding of scientific misconduct and conflict of interest, and appreciation of the attributes and conditions necessary for ethical collaboration, data handling and sharing, authorship, and mentorship. Some programs focus on formal guidelines, general ethical principles, and historically noteworthy cases of research abuse. These programs provide researchers with information needed to comply with regulatory and institutional guidelines but may not necessarily prepare them to apply ethical reasoning skills to the design and conduct of research. 1 Studies have suggested that researchers are more likely to formulate their concepts of scientific integrity and responsibilities toward others from climate, institutional contexts, and ethical norms than from formal guidelines.2,3
Training programs in RCR/HSP generally take the form of face-to-face short courses, workshops, online standardized certificate programs, and hybrid versions that combine one or more of these techniques. Although online programs require fewer in-house resources and offer maximum flexibility, particularly when publicly available programs exist such as those available through the Collaborative Institutional Training Program (https://about.citiprogram.org/en/homepage/), other important factors need to be considered. A 2009 quantitative meta analysis of ethics program evaluation efforts, for example, found that ethics courses that emphasize student engagement through highly interactive learning and practice activities promoted instructional effectiveness more than those that relied on self-directed learning. 4 A 2011 randomized-controlled study in Botswana suggested that there was little difference in rule-based knowledge acquisition by trainees completing interactive learning activities compared to online, self-paced programs; trainees who participated in context-relevant case discussions with feedback, however, appeared to be more likely to identify ethical issues correctly. 5
Although training in responsible conduct of research and human subjects protection (RCR/HSP) has become a standard part of graduate education in academic medical centers in high-income countries, training in RCR/HSP is still seldom required as part of postgraduate medical education in many low-and middle-income countries (LMICs). Resource-constrained countries with wide socioeconomic disparity pose added ethical difficulties to medical practice. Standards of care vary depending on the level of access, and bioethics training for medical practitioners is seldom sufficiently context-specific to help them resolve practical medical challenges they may encounter in everyday practice. With an increasing number of researchers and health professionals from LMIC countries participating in international multicenter research projects, there is a growing need for training programs in these settings to include RCR/HSP in their curricula. This is particularly true in countries like Guatemala where the number of internationally sponsored clinical trials taking place is growing without comparable expansion or evaluation of education and training programs to ensure that research by local research collaborators is conducted ethically.
The current study has 3 aims:
To implement a training program in human subjects protections and responsible conduct of research for surgical residents in Guatemala To develop a new face-to-face curricula in Spanish that is context-relevant and engaged trainees in active learning of the materials To examine an in-person active-learning curriculum in research ethics as a viable addition to surgical residency training in Guatemala.
Methods
Study Setting
Undergraduate medical education in Guatemala consists of 3 years of preclinical and 3 years of clinical training. Graduates receive a medical license from the Colegio de Médicos y Cirujanos (College of Physicians); those who wish to pursue careers in surgery must complete a 5-year residency, 1 year of which is a field placement in a hospital providing care for underserved segments of the population. Residency graduates receive a diploma from the national university, Universidad de San Carlos de Guatemala (USAC), which allows them to perform general surgical procedures. Surgeons who complete a fellowship in a surgical subspecialty can register as surgeons with subspecialty training.
Although there are currently efforts to create a “national” medical education curriculum, including a board examination, medical school and residency curricula may currently vary in content and mode of instruction provided that they meet the curricular requirements of the Office of Registration and Academic Control of the Faculty of Medical Sciences, an administrative unit within USAC. Under these requirements, all undergraduate medical students must complete at least 2 courses in bioethics and a research project in order to receive a medical degree. In theory, all residency programs in Guatemala are required to include a course in research methods (of which research ethics is a component) and complete an independent research project. While all residents do complete research projects, research methods courses tend to emphasize the timely completion of projects rather than the research process itself. It is rare in practice that a residency offers a true methods course, relying instead on mentorship by faculty and trial-and-error research experience to fulfill this curricular requirement. Often residents receive little to no training in research methods, human subjects protections, or responsible conduct of research; few faculty responsible for overseeing resident research activities have experience as researchers themselves and often have limited knowledge of the ethical principles that guide clinical research. This study aims to explore the feasibility of implementing a training program in RCR/HSP as part of surgical residency training in Guatemala, where no such training is currently required. The study also aims to evaluate the effectiveness of 2 different modalities of content delivery by comparing the use of online, publicly available, training materials as a stand-alone requirement with online training that is augmented by in-person, case-based training delivered by an instructor with knowledge and experience in the field.
Study Sample
This 2018 study took place in the surgical residency programs of 3 large urban hospitals in Guatemala City with well-established residency training programs- Hospital General San Juan de Dios (HOSPIGEN), Instituto Guatemalteco de Seguridad Social (IGSS) and Hospital Roosevelt. As part of the residency curricula, all surgical residents at the 3 hospitals (N = 160) were required to complete training activities in RCR/HSP and to complete pre-and posttraining assessments. Trainees were advised that the pre- and posttraining assessments would, with their permission, also be used as data for a study investigating different methods of teaching research ethics in Guatemala. All residents were given the opportunity to verbally “opt out” of having their assessment data used for research purposes. Residents at IGSS (n = 63) and Hospital Roosevelt (n = 55) served as the control arm for the purposes of the research activities; residents at HOSPIGEN (n = 42) were assigned to the research intervention arm.
Measures
All training programs and assessments were administered in Spanish. Surgical residents at each of the 3 hospitals were required to complete a pretraining assessment followed by 2 online training programs: a self-paced certificate program in responsible conduct of research, Conducta Responsable en Investigación (http://cri.andeanquipu.org/), which has been developed for Latin American researchers by faculty at Universidad Peruana Cayetano Heredia in Peru as part of a National Institutes of Health (NIH) Fogarty program; and the NIH Office of Extramural Research—Protecting Human Research Participants online training program (https://phrp.nihtraining.com/#!/) and to complete post-training assessments. In addition, the residents in the intervention arm (HOSPIGEN) were required to complete 7 weeks of face-to-face training in responsible conduct of RCR/HSP that was embedded in a research methods course taught by a member of the study team.
The intervention RCR/HSP curriculum, developed by members of the study team and taught by one of its Guatemalan team members included 14 hours of content delivered using a combination of didactic lectures and interactive case-based discussions. The curriculum was modeled after one developed by one of the authors and her colleagues as part of a 5-year research ethics training and curriculum development program funded by the NIH Fogarty International Center and the Human Genome Research Institute (Grant No. R25-TW009738). The current study reported here was supported by a seed grant from the Rutgers Global offices at Rutgers, The State University of New Jersey.
Topics included ethical issues associated with study design; collection and use of data; human research subjects; authorship, and publication. To address the reality that trainees’ schedules at HOSPIGEN would inevitably result in schedule conflicts and to accommodate those trainees who missed a module, module intensives—with module repetition—were designed and taught during weekends. Every module was also live-recorded, and the video was available to HOSPIGEN trainees to be watched at their own pace as desired. Upon completion of the assigned training requirements for the 3 hospital residencies, all trainees completed a post-training assessment to assess gains in RCR/HSP knowledge and ethical reasoning skills.
Questions used in the pre- and post-training assessments were designed to test awareness of key concepts covered in the online courses with particular attention to international and Guatemalan regulations regarding research. Of particular interest to the study team was the extent to which either mode of delivery contributed to trainees’ ability to identify areas of ethical concern when presented with various scenarios and to utilize ethical reasoning to decide upon an ethically appropriate solution from among several choices of action. All questions were classified according to the cognitive skills hierarchy defined in Bloom's taxonomy (Figure 1). 6 For the purposes of analysis, each question was labeled as requiring either higher- or lower-order thinking, with lower-order questions being those that only measured “knowledge” and/or “comprehension” and higher-order questions including those that measured “application,” “analysis,” “synthesis,” and/or “evaluation” (Figures 2 and 3). Both the pre- and post-assessments were administered using REDCap, a widely used online web application for building and managing online surveys and databases (https://www.project-redcap.org/).

Bloom's taxonomy of cognitive learning objectives.

Sample test question requiring lower-order thinking according to Bloom's taxonomy.

Sample test question requiring higher order thinking according to Bloom's taxonomy.
Consent to Participate
Although surgical residents at all 3 hospitals were required as part of their residencies to complete the assigned training in research ethics provided under this educational program, they were given the opportunity to “opt out” of their assessments being used for the research portion of the project by communicating with their instructors verbally. No trainees in the training programs opted out of having their assessment data included in the analytical sample for this study.
Ethics Review
Prior to the start of the program, the study, included the passive consent process used with the trainees. was reviewed by the Institutional Review Board at Rutgers University (Pro2018001095) and a nonhuman determination was issued for the protocol as program evaluation and quality improvement in an educational setting. Similarly, the hospital ethics committees at HOSPIGEN and IGSS reviewed the protocol and verbal passive consent process and conveyed informally through email to the instructors that the training program could proceed as proposed.
Analysis Plan
Pre- and post-training assessment data were analyzed in deidentified form and stored separately from academic records. Only those records for which both pre-and post-training assessment data were available and, in the case of the intervention arm, only data from residents who had completed the requisite face-to-face training were included in the analytic sample. Results were analyzed using STATA12. 7 Descriptive statistics were run for all demographic data, and Pearson's chi-square tests of significance (Fisher exact tests in instances where the cell size was too small) were computed to identify where the variability in responses by the 2 arms was statistically significant. Gains in knowledge irrespective of group assignment were analyzed using matched (pre- and post-) mean scores. Group differences in mean scores were analyzed using difference-in-differences analysis to determine gains by study arm assignment and account for baseline differences. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement 8 (see Supplemental File S1). 9
Results
All of the 160 surgical residents enrolled in the 2018 RCR/HSP training programs at the 3 hospitals agreed to have their assessment data included in the study. Of these, only 140 surgical residents met the criteria for inclusion in the analytic sample: 42 (100%) from the intervention arm (HOSPIGEN) and 98 (83%) from the control arm, including 48 (76%) trainees from IGSS and 50 (91%) trainees from Hospital Roosevelt (Figure 4).
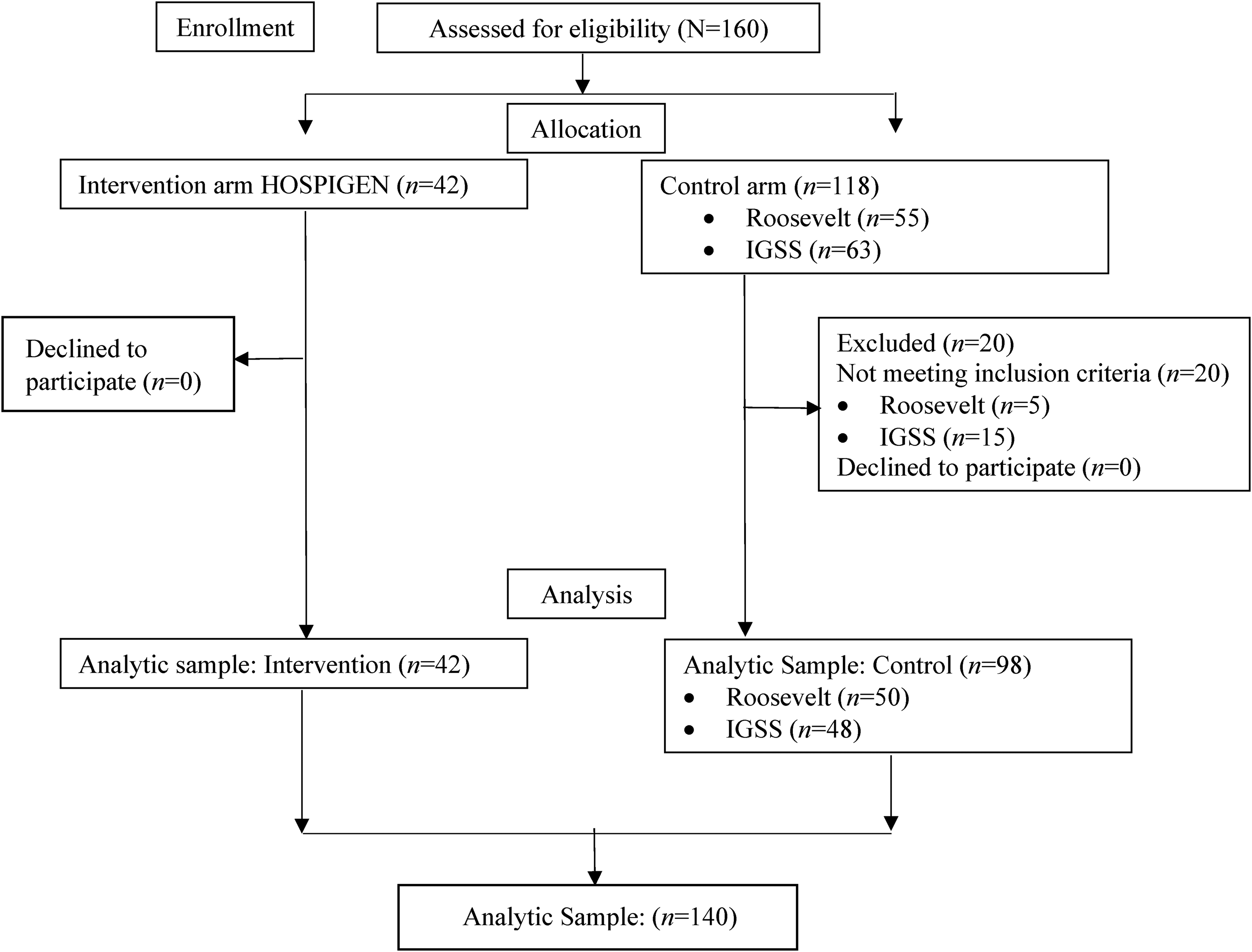
Flowchart of study population.
Descriptive statistics appear in Table 1. Most residents were male, with the largest number of trainees in the sample being in their first year of residency training. More than half of the residents reported that they had previously received training in research ethics. Overall only 16% of residents reported no prior experience in conducting research in a study involving patients or information about patients; residency site, ie HOSPIGEN (the study intervention arm) or IGSS and Hospital Roosevelt (the study control arm) was significantly associated with whether or not a trainee had had previous research experience involving human subjects or human subjects data (χ2 = 5.4340, P = .02) or had been involved in a study requiring ethics committee approval (χ2 = 17.67, P = .00). Before the study, more students in the control arm, compared to students in the intervention arm, reported they had never participated in a research study involving human subjects, used secondary data sets as the source of data for their undergraduate research study, or been involved in a study requiring ethics review.
Descriptive statistics.
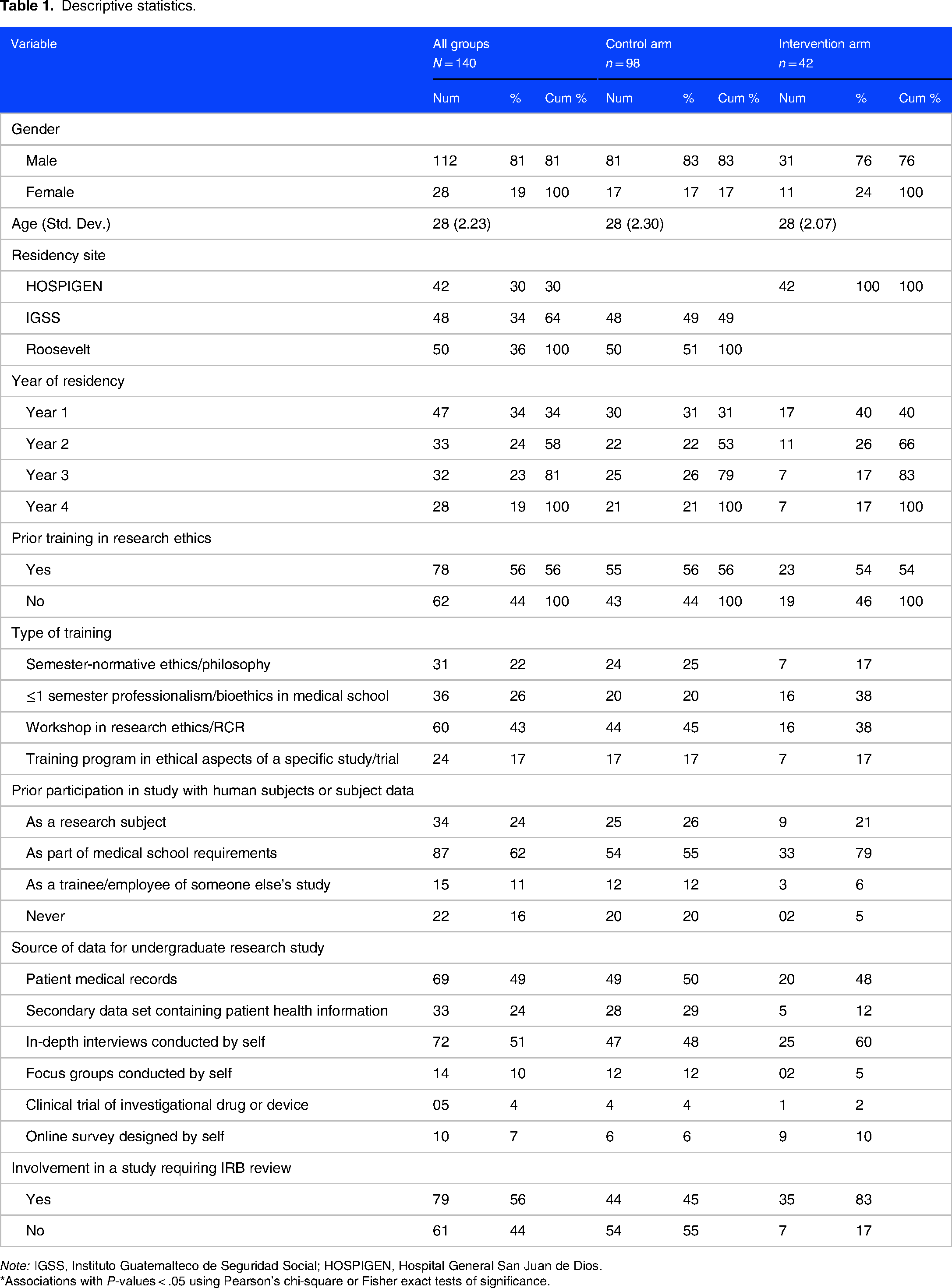
Note: IGSS, Instituto Guatemalteco de Seguridad Social; HOSPIGEN, Hospital General San Juan de Dios.
*Associations with P-values < .05 using Pearson's chi-square or Fisher exact tests of significance.
Pre- and post-training assessment scores are reported in Table 2. Overall, mean scores improved in all groups (from 52.7 to 58.7 points out of 100), with a slightly larger, but not statistically significant, gain in the intervention arm. Mean scores in lower-order questions improved by approximately 10 points, with a larger gain (11 points) in the control arm than in the intervention arm (8.5 points). The mean scores on higher-order questions were 4 points higher among trainees in the intervention arm than those in the control arm (66.7 points compared to 62.7 points, P = .009).
Pre- and post-assessment scores.

Note: 1P-value by t-test.
P-value by difference in differences.
Pre- and postscores P-value: .00 by matched t-test.
Table 3 reports study findings on measures of trainee familiarity and self-efficacy with respect to RCR/HSP. At the start of the program only 12% of trainees reported being familiar or very familiar with RCR/HSP, and only 19% reported that they knew enough about RCR/HSP to handle ethical issues that they might encounter in the course of conducting research studies in the future. Following the training, both groups reported having high levels of confidence that they could recognize most of the ethical issues that they encountered in research design and implementation; they knew the ethical principles and legal requirements for research in Guatemala; and they would be able to design and implement a research study that conformed to them. Over 95% of all trainees reported that they were very confident/confident that they understood and could avoid scientific misconduct through fabrication, falsification, and plagiarism in research and could recognize any such transgressions by their colleagues. Over 95% of the trainees reported that the training had given them confidence/high confidence to speak up if they observed scientific misconduct by a colleague. Trainees in the face-to-face training reported having higher levels of confidence that they could recognize ethical issues, knew legal requirements, could design ethical research, and could identify, report and avoid scientific misconduct than the trainees in the control arm; the observed differences were statistically significant at the P < .01 level.
Familiarity and self-efficacy in responsible conduct of research and human subject protections.

Note: *P-value computed using Fisher exact test.
Discussion
This study is a first-ever attempt in Guatemala to understand empirically the extent to which surgical residents are familiar with and can apply ethical principles and regulations in determining right actions in clinical research. It provided an opportunity to consider the relative benefits of online training only compared to online training augmented by face-to-face training in RCR/HSP in a resource-constrained environment where human and physical resources to teach these topics are limited.
Despite the very high numbers of residents in both arms who reported prior research ethics training and experience with research involving human subjects and/or human subjects data, overall pre-assessment scores were poor. Although it was beyond the scope of this study to examine in any systematic way the reasons for low pre-test scores, a number of underlying factors may be involved. Although most undergraduate medical curricula in Guatemala include courses in ethics, many such courses focus on normative ethics that reinforce predominant social norms in Guatemala rather than introduce students to the country's regulatory environment or internationally accepted ethical principles in research. Most course instruction in Guatemala takes the form of didactic lectures; opportunities for students to engage actively in their own learning are limited. This is a particular shortcoming in research ethics education given the substantial body of literature that supports the use of active learning pedagogy to encourage students to engage with the material through small group work, case discussions, and role play. 10
In pre-assessments there was no statistical significance between study arms in total scores and scores for lower-order questions; however, residents in the intervention arm had higher scores for questions involving higher-order thinking in comparison to residents in the control arm. HOSPIGEN introduced a year-long, in-person research methods course in 2017 as part of an effort by the hospital and university authorities to improve training for postgraduate surgical trainees. Although HOSPIGEN residents were not explicitly trained in RCR/HSP, they were encouraged to apply concepts, analyze scenarios, apply rules, and evaluate approaches in their research methods coursework—all of which involve higher-order thinking. Residents who had taken or were taking the HOSPIGEN methods course may have drawn more easily on such skills when confronted with a higher-order question in ethics than residents at the other hospitals where similar skills had not been reinforced through coursework.
Intervention-arm residents also had significantly higher scores on questions involving higher-order thinking in the post-assessment than control-arm residents. This finding would suggest that in-person training sessions may help build critical reasoning skills, a finding that echoes previous work evaluating teaching modalities in Botswana. 5
This study's findings of a statistically significant association between gains in self-confidence in a number of domains make a promising case for active learning approaches in working with these topics. Prior research suggests that greater gains are achieved in learning environments that involve social interaction and active engagement with the subject material.4,10–16 Trainees in the intervention arm had 14hours of peer-to-peer interactions in analyzing and reacting to ethical issues in research and research conduct; such “practice” is likely to have built trainee confidence in ways that are less easily achieved in more static learning environments. While such improvements in self-efficacy must be viewed with some skepticism in light of the very modest gains overall in knowledge and ethical reasoning skills, residency programs may nonetheless want to invest in human and physical resources to support in-person ethics training programs to promote self-efficacy in ethical decision-making among their trainees. Future efforts to evaluate the efficacy of in-person research ethics training modalities in this setting would benefit from the use of qualitative methodologies.
This study reveals several uncomfortable truths: first, despite, an extensive curricular load in ethics in undergraduate medical school, surgical residents in Guatemala lack basic knowledge in this domain as measured in pre-assessments, and second, residents received failing scores in post-assessments irrespective of how ethics content was delivered. This latter finding suggests that the challenges in teaching RCR/HSP in busy surgical residencies in this setting may be as much practical as pedagogical ones. Surgical residents work long hours as part of their surgical training, often beginning in the early hours of the morning and not finishing their last surgeries until mid-afternoon.17–19 In-person class activities begin immediately afterward and frequently take place in cramped and ill-equipped facilities with inadequate ventilation, poor lighting, and few technology aids—hardly ideal conditions for “active” engagement with the course content. Online content is likely to be glossed over in the evenings when residents finally leave the hospital. Certificates of completion from the online courses serve merely as evidence that trainees completed the modules and cannot be considered accurate measures of the extent to which information will be retained or trainees will be able to apply that information appropriately when faced with an ethical issue in research.
Another practical challenge is one of resources. Despite efforts in the past decade to build capacity in research ethics in Guatemala, there remains only a handful of medical professionals with the content and teaching skills necessary to teach in-person courses in RCR/HSP. While this challenge might be overcome by using a train-the-trainer model to build capacity within each surgical residency program in the country, it is unlikely, given the low remuneration for teaching faculty and limited interest on the part of the surgical staff, that a sufficient number of faculty trainers with expertise in RCR/HSP, active-learning pedagogy, and surgery could be marshalled in the near future for this purpose. Given the very modest difference in gains between the 2 arms of this study, the adoption of online modules for teaching RCR/HSP in this setting seems the more scalable option.
A more intractable challenge may be one of attitude on the part of medical professionals toward the teaching of ethics in general, particularly in surgery residency programs focused on honing surgical skills in their trainees. Despite recent well-publicized instances of corruption and mistreatment in Guatemala's public hospitals,20,21 doctors are held in high esteem and their decisional authority in matters of medicine tends to go unchallenged. Course content that may prioritize the rights and concerns of patients over the prerogatives of doctors may not be well received. Doctors are presumed to be ethical professionals and teach by example rather than coursework. Changing these attitudes will take time, although efforts by the Office of Registration and Academic Control of the Faculty of Medical Sciences to improve resident education and the move toward board certification are positive steps in that direction.
This study has several limitations that should be noted. The lack of statistical power to determine significance limits the extent to which one can draw definitive conclusions about the value of face-to-face as compared to online training. We have included in this study the 3 largest surgical residency programs in Guatemala, representing the majority of surgical trainees in the country; were the Guatemalan authorities to mandate further research on RCR/HSP training programs in ALL residencies in the country, more definitive findings might have been possible, but such a study exceeded the scope of this current effort. In addition, the assessment tools were those developed by the instructors as coursework for the residents and, as is the case in most academic settings, were neither pilot-tested nor validated as a study instrument in advance of its use. It must also be noted that one of the online training programs utilized in this study, the NIH Office of Extramural Research Protecting Human Research Participants program, has been archived since this study was undertaken prior to revisions in the United States Common Rule and is no longer maintained or updated. While this will make replication of this study difficult, the authors’ intention, which was to identify best practices in teaching RCR/HSP, can still be served through high-quality replacement programs such as the Research Ethics Online Training program developed by the World Health Organization in partnership with the Bill and Melinda Gates Foundation and the University of Oxford (https://globalhealthtrainingcentre.tghn.org/elearning/research-ethics/).
Conclusion
Differences in gains in RCR/HSP knowledge and self-efficacy between trainees completing online training only and those completing in-person as well as online training are too modest to prefer one mode of instruction over another in this setting. Given the limited availability of RCR/HSP faculty, financial resources, and time in the surgical training schedule, academic authorities in Guatemala should consider online training programs in RCR/HSP in the future in all surgical residency programs as an affordable and scalable strategy to build ethical research skills in its surgical workforce. Adopting online education as the mode of delivery should not preclude the addition of in-person training when possible nor capacity-building efforts in ethics education within medical school and residency faculties. In addition, greater attention should be given to the content and quality of research ethics instruction in undergraduate medical schools in Guatemala to ensure that research projects are conducted in an ethical manner and to improve students’ familiarity and knowledge of RCR/HSP as they matriculate into the country's residency programs and healthcare system.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241257079 - Supplemental material for Developing an Evidence-Based Ethics Education Program for Surgical Residents in Guatemala
Supplemental material, sj-docx-1-mde-10.1177_23821205241257079 for Developing an Evidence-Based Ethics Education Program for Surgical Residents in Guatemala by Maria Lorena Aguilera Arévalo, Sergio Nicolás Martínez Seikavizza, Ery Mario Rodriguez, Miguel Angel Siguantay, Jorge Fernando Solares Ovalle, Luis Fernando Talé Rosales and Francis Barchi in Journal of Medical Education and Curricular Development
Footnotes
Author Contributions
MLA, SNM, and FB were responsible for study design, selection of online course materials, and development of the in-person curricula. MLA, EMR, MAS, FS, and FT were responsible for the implementation of the training programs at HOSPIGEN, IGSS, and Hospital Roosevelt, respectively. All authors read and contributed to multiple versions of the manuscript in draft and read and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded under an International Collaborative Research Grant award from Rutgers Global, Rutgers University. Individual faculty development in ethics education for Drs. Aguilera and Martinez and partial salary support for Dr Barchi were provided by the National Institutes of Health, Fogarty International Center and Human Genome Research Institute, Grant No. 1R25-TW009738-01.
Ethics Statement
The study was approved by the Institutional Review Board at Rutgers University (Pro2018001095) and the hospital ethics committees at HOSPIGEN and IGSS. Surgical residents at the 3 hospitals were given the opportunity to “opt out” of their assessments being used for the research portion of this project. All trainees gave their consent to have their assessment data included in the analytical sample for this study.
Availability of Data and Materials
An earlier version of this manuscript was published in 2019 as a preprint on Research Square under a Creative Commons Attribution 4.0 International License, doi: ![]() . The datasets used and/or analyzed during the current study are available in deidentified form from the corresponding author upon reasonable request.
. The datasets used and/or analyzed during the current study are available in deidentified form from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.