
Abstract
Point-of-care ultrasound (PoCUS) is increasingly being adopted by clinicians to augment their clinical examination and aid procedures. Evidence-based clinical practice guidelines now support many aspects of PoCUS practice. As a result, more and more medical schools are integrating PoCUS into their curricula, creating a significant demand for training resources. All training must ensure that trainees have the appropriate knowledge, skills and behaviour to enable the clinical integration of PoCUS. The transition from supervised to unsupervised practice is an important step in PoCUS, but should not be confused with expertise. At the start of clinical practice, confirming that something is not normal is probably enough, and trainees can subsequently improve their PoCUS diagnostic accuracy at the bedside during clinical rotations. Our hypothesis is that competency can be achieved without the need to scan patients suspected or suffering from the target pathology. This would enable most of the training to be carried out outside the clinical environment, using volunteers in planned sessions. These planned sessions will be able to accommodate a larger number of trainees and may facilitate collaboration between specialties. When patients are scanned in the clinical environment, trainees should have acquired a good level of competence beforehand. In summary, normology principles could help PoCUS trainees, at the start of their training, to acquire the knowledge, skills and behaviour necessary to achieve a level of competency allowing them to proceed to unsupervised practice. Initially confirming whether something is normal or not is enough. Nevertheless, further research should be conducted to support this concept, and its impact on PoCUS teaching in clinical practice.
Keywords
Introduction
Developments in ultrasound technology have led to improved image quality, machine features, reduction in machine size and thus portability, as well as reduced costs.1,2 In addition, the popularity of ultrasound has moved beyond the remit of traditional specialties and has been increasingly adopted by clinicians using it to augment their clinical examination and reduce the risks associated with some procedures.3–5 The term point-of-care ultrasound (PoCUS) has been used to describe this use. The availability of low-cost ultrasound machines, specifically aimed at PoCUS users, has increased with time, and has included many portable hand-held personal devices. 6 As a result, access to PoCUS has become increasingly easier, with low levels of associated litigation, making it a safer tool for incorporation into clinical practice. 7
Clinicians from specialties such as trauma surgery and emergency medicine were among the first to adopt PoCUS. 2 Initially, the focused assessment with sonography in trauma (FAST) scan was popular in order to rapidly identify potential bleeding into body compartments in major trauma patients. 2 Subsequently, further uses have evolved and there are now a plethora of focused scans described, which cover a range of body systems and presenting complaints. 8 Protocols, which incorporate more than one focused scan type, have also been described and are aimed at aiding evaluation of patients presenting with a number of clinical scenarios, such as those with shock, dyspnoea and chest pain.9–11 Evidence-based clinical practice guidelines now support many aspects of practice, with many specialties now incorporating PoCUS into their curricula. This has also included allied health care professions such as paramedics, nurses and physiotherapists.12,13–15 There has been increasing move to teach PoCUS skills at an earlier stage of training, and as a result many medical schools now include PoCUS in their basic curriculum.16,17 However, with an increasing number of potential PoCUS users this is likely to create a significant demand for training resources, and introducing this to already busy medical school and post-graduate training curricula will be challenging. To mitigate some of these challenges, we propose the concept of normology, which embraces four key principles (Figure 1).
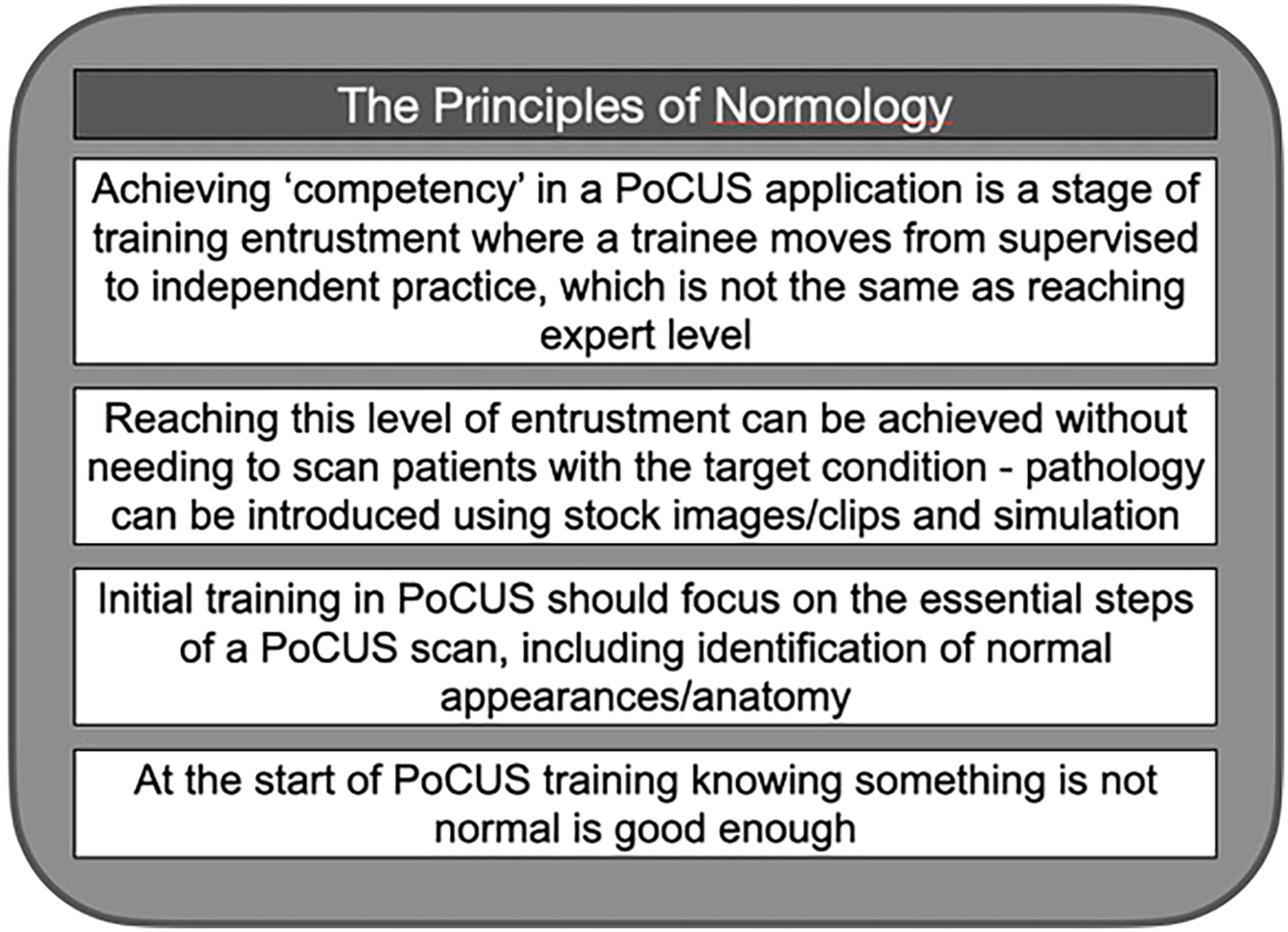
The principles of normology.
Normology, a New Concept
The training journey for practitioners of PoCUS will start with novice and may finish at expert level. However, not all will complete this journey in its entirety and the speed of progress will be variable depending on the individual and their circumstances. This mirrors many aspects of clinical training and practice where levels of entrustment can be applied at varying stages of this journey (Figure 2).18,19 When considering what competency in PoCUS looks like, this most likely describes a transition from one level of entrustment to another, eg, level 2 to 3, and not a point at which the trainee evolves into an expert, requiring no further mentorship and supervision. Thus, providing support for trainees who have been deemed as competent should still be considered necessary, with an implicit emphasis on a culture of continued learning and education.

Levels of entrustment for PoCUS.
Key inclusions for any training in PoCUS should include the following: learning the basics of ultrasound physics, knobology and transducer probe manipulation, setting up the ultrasound system for a particular scan type, appropriate patient placement and positioning, attainment of a suitable image/video loop, interpretation of the image/video loop and how this may influence clinical care. Practicing each of these components to a suitable standard, on a regular basis, will support the development of core skills and improved pattern recognition. Trainees have to experience and develop techniques to be able to scan a range of different body shapes and sizes, regardless of whether the patient has pathology or not. We propose that trainees in PoCUS can progress beyond the need for direct supervision without having scanned any patients with an abnormality/pathology – ie, progress to the next stage of entrustment.
Normology encompasses the principle that the PoCUS training journey should start with the emphasis on confirming normal as opposed to identifying abnormal. In addition, it is possible to become “competent”, ie, able to scan independently, having only scanned normal subjects and patients. Abnormal findings can initially be introduced via stock images and video loops rather than needing to be experienced in practice. There may also be benefits in reducing the cognitive load of PoCUS trainees needing to be exposed to a plethora of abnormalities and pathology, especially in the early stages of training. Initially, only expecting trainees to confirm the presence of normal findings allows them to focus on their technique as well as reinforcing familiarity with a range of normal appearances. In cases where appearances are not deemed normal, they should be encouraged to seek the help of a more experienced practitioner. Therefore, trainees should initially aim to scan a range of patients/volunteers of differing baseline characteristics, including age and body mass, rather than focusing on undertaking training scans on patients with the potential target pathology.
An analogy can be made between the normology approach for PoCUS training and how pilots learn to fly. After a theoretical program, a pilot learns how to fly a plane in normal flight situations. Pilots are not expected to have experienced a range of adverse conditions to be able to fly independently, such as bird strikes, engine failures etc The pilot initially learns how to manage adverse events theoretically and during simulation sessions. We acknowledge that some PoCUS educators may see normology as a challenge to established PoCUS education and training programmes.
Current Training in PoCUS
Any PoCUS training programme should aim to ensure that trainees have the required knowledge, skills and behaviour required to enable clinical practice integration. This should encompass five core skills and behaviours: being able to generate and optimise ultrasound images, being able to interpret the generated images, incorporating the information into clinical decision making, maintaining their skills and supporting the training of other clinicians in PoCUS. 20 Many PoCUS curricula describe three phases of training: induction, experiential, and attainment of competency, prior to practicing independently. 20
Induction
This phase is aimed at teaching the relevant knowledge as well as introducing the required skills for the specified applications. There should also be inclusion of illustrative clinical cases and the promotion of good governance to underpin how the taught components can be incorporated into clinical practice. There are many ways this phase can be delivered; from comprehensive courses, which cover the whole curriculum, to a modular approach for each application. The learning may be delivered face-to-face or remotely, or a mixture of both. With the COVID19 pandemic, there was a need to move much of the learning online, often adopting a range of blended learning methods, to reduce physical contact. Any practical teaching should start with basic principles, such as being familiar with the ultrasound machine and features and introducing the scanning technique for the chosen applications. For many established programmes, this is already the case, especially the use of normal volunteers.
Experiential
The experiential phase allows for the development of skills taught during the induction stage. The trainee will usually be assigned a mentor or supervisor, who should oversee this stage of learning, and can also provide supervision of their scanning. Some unsupervised practice may be undertaken, with the intention of not contributing to or influencing patient management. Despite such intentions, there is a risk of false interpretation with regards to any findings, which may result in patient harm or unnecessary additional investigations. This phase of learning is generally undertaken in the trainee's clinical environment, with emphasis on scanning patients with the likely target pathology, ie, when practicing to scan the abdominal aorta they target patients with a suspected aneurysm. This creates barriers to scanning opportunities as trainees may just focus on patients with potential pathology, which may be infrequent for some conditions. Such behaviour is reinforced when trainees are expected to include a specified proportion of abnormal findings in their training log. Many curricula recommend creating a logbook to record the scanning activity, as well as collecting supporting ultrasound video loops or images, which are usually scrutinised on a regular basis by the supervisor or mentor.
Competency
Achieving competency for an application may be defined as reaching a level of ability to perform a specified scan independently. 20 How this is determined is variable, for example, the Canadian Emergency Ultrasound Society recommends 200 scans under direct supervision, the American College of Emergency Physicians proffers that competency could be achieved after 25 to 50 reviewed scans for each emergency ultrasound application while the Accreditation Council for Graduate Medical Education uses a threshold number of 150 scans to determine PoCUS proficiency.8,21,22 The Australasian College for Emergency Medicine and the Society for Acute Medicine (UK) recommends a certain number of recorded pathological scans depending on the subject covered.23,24 This explains why, for many curricula, the experiential phase often needs to occur in a clinical setting. The American College of Surgeons, recommends a combination of images or video loops of normal, and of abnormal, ultrasound findings to be recorded and proffered for competency assessment. 25 In some curricula, a logbook alone is not sufficient to achieve competency and another form of assessment is undertaken. The Royal College of Emergency Medicine (RCEM), for example, suggests a minimum specified number of reported scans and a triggered objective assessment. 26 With regards to such assessments, they evaluate key aspects related to pre-scanning, scanning and post-scanning elements, with only a small component focused on identification of pathological findings. With the adoption of normology, the latter may be provided as an image or clip and the rest of the assessment conducted using a normal volunteer in a controlled environment, without compromise.
Independent Clinical Practice
After obtaining accreditation, clinicians should evolve and mature in their PoCUS practice as they continue to undertake regular activity and encounter more pathologies, however, some may develop bad habits and without appropriate support fail to improve. Thus, achieving competency at a point in time does not necessarily ensure that this is maintained thereafter, and some clinicians may cease to perform particular PoCUS applications due to lack of confidence. The RCEM advises a minimum scanning activity that should be undertaken to ensure competency is maintained. Adopting a preceptorship model may aid maintenance of competency. 26
Being Competent to Practice Independently Is Not the Same as Expertise
Moving from supervised to non-supervised practice, and being able to practice independently, is an important milestone in PoCUS training. 27 However, this should not be confused with expertise. In many aspects of medicine, knowledge, skills and behaviour will continue to evolve with practice and time, resulting in an ability to manage more complex cases and develop more enhanced clinical ‘toolkits’. PoCUS is no different, and the skillset of a trainee who has been assessed as suitable to progress to independent practice is likely to be basic compared to an operator who has regularly practiced for many years. Although PoCUS is different from traditional ultrasound, this does not mean that PoCUS is inferior to traditional ultrasound and there are levels of complexity and expertise in both. 28 Whatever stage of practice a user may be at, there will be occasions when advice and guidance are sought from another practitioner with more experience – which applies equally to trainees and those deemed competent. Normology promotes seeking help, when appropriate, especially when novice trainees encounter abnormal findings.
Challenges
Number of Trainees
With an increasing number of specialties incorporating PoCUS into their curricula, including moves to introduce training at an earlier stage, the number of trainees is set to rise. All trainees should expect supervision and mentorship, which might be difficult to implement. Currently, there is not enough supervisory capacity, especially problematic for specialties which have only recently embraced PoCUS into their practice. 29 In many cases, this is due to a paucity of trained practitioners with the time and motivation to be involved, as often there are existing commitments due to academic or clinical activity. 29 For example, acute internal medicine trainees in the UK must now achieve PoCUS competency for a number of applications in order to complete their higher specialty training. This will require a rapid expansion of supervisors, which will be challenging to deliver in practice, or a change in focus of the training pathway. Adopting normology principles may help with the latter.
Difficulties with Accommodating and Supervising Trainees in a Clinical Environment
The clinical environment should always be focused on the patients’ needs rather than the trainees, therefore any training undertaken should not be detrimental to patient care. This is especially relevant during high acuity and time-critical clinical situations in acute specialties, when any PoCUS scans undertaken should be performed by a competent practitioner.
As previously alluded to, bedside PoCUS supervision may be difficult due to the poor availability of supervisors, a limitation in available training time for trainees and residents due to working time limits, and high clinical pressures/workload. 29
Any programme that expects trainees to log a minimum proportion of pathological findings, is reliant on such patients presenting with specific conditions. Exposure to target pathology can be very unpredictable and affected by many factors, such as the local population burden of disease and type of clinical unit, eg, whether the trainee works in a large major trauma centre or a small community clinic.
Benefits from Adoption of Normology Principles
Benefits for the Trainee
Adopting a normology approach can facilitate the organization and delivery of supervised sessions for trainees, conducted away from busy clinical environments. With prior planning, an appropriate number of faculty can be arranged to ensure trainees are appropriately supervised, and enough volunteers/models recruited. Faculty attending such sessions are less likely to be distracted by clinical issues and more prepared. Healthy volunteers, as opposed to patients, are less dependent on changes to their clinical condition, and therefore more reliable with regards to being fit to attend. Trainees can also practice on each other. Planned sessions can ensure the availability of ultrasound equipment within dedicated teaching facilities, rather than relying on the equipment and space being available within clinical environments.
The learning environment in a dedicated teaching facility is preferable to that experienced in a stressful clinical environment, especially at the start of training. Being able to learn practical skills in a scheduled session, means that the trainees are likely to achieve a greater number of supervised scans in a shorter amount of time. Initially, not scanning patients with likely pathology allows the focus of training to be aimed at technique and familiarity with normal findings/anatomy. Abnormalities can still be introduced to trainees via case images, video loops and simulation. Although many studies report an ideal number of examinations to reach PoCUS competency, there is a paucity of evidence to specify the ideal ratio of normal to pathological cases for trainees.
Trainees who have completed their competency assessment, and are ready to move on to the next stage of entrustment in their training journey, are more likely to be ready to scan real patients with potential pathology in more frenetic, time-critical clinical environments. Their exposure to pathology and clinical scenarios will increase with continued practice, and conversely, their reliance on support from more experienced practitioners will decrease.
Benefits for the Trainers
Adopting normology principles can be beneficial to trainers. Supervising trainees is less likely to be disrupted at a planned event, compared to the unpredictability of clinical environments. This is especially pertinent in urgent and emergency specialties, as such sessions can be planned far ahead and are less influenced by clinical pressures. The availability of ultrasound machines, dedicated to teaching, can allow for a larger session to be conducted, hosting more trainers and trainees than possible in a clinical environment. Due to many specialties adopting the same PoCUS applications, a multidisciplinary faculty can be recruited, which supports collaboration between different medical specialties using PoCUS. This is especially helpful for specialties with a paucity of trained supervisors and mentors.
Benefits for Patients
Normology benefits the patients by ensuring that trainees should have a reasonable level of skill and knowledge before practicing in the clinical environment. This may reduce delays in patient management and flow as trainees should not be using patients to practice basic scanning skills, especially in high acuity areas.
Experience of Abnormalities
Trainees should have a sound appreciation of normal anatomy and sono-appearances, and experience scanning a range of body shapes and ages. Confirming normal is a good starting point, and having clear protocols in place about dealing with cases where appearances are not normal is essential. Initially, a range of relevant abnormal pathology appearances can be introduced during theoretical sessions, via stock media and the use of high-fidelity simulators. Trainees can also access various online teaching resources, which can provide further exposure to pathology. Ultrasound high-fidelity simulators have become increasingly available and can aid clinical skill acquisition. However, there is a lack of evidence to actively support the use of simulators over practice on healthy volunteers, for the development of ultrasound manipulation skills. 30 Despite this, simulators can be used to augment PoCUS teaching and provide opportunities to introduce pathology and allow discussion of their clinical relevance. 31
Collaboration with Experts
PoCUS should be considered an augmentation to clinical evaluation, rather than being used in isolation. Using the findings of a PoCUS examination to augment clinical assessment may provide additional clarity, and guide any further management or investigations. Clinicians adopting PoCUS do not need the experience or skills of an ultrasound specialist, such as a radiologist, as their roles are different. However, it is essential to develop collaborative links between users so that discussions of clinical cases where findings are abnormal can happen without animosity and be patient focused. This does not necessarily mean that novice trainees practicing normology should routinely seek the advice of a specialist, as often there will be more experienced PoCUS practitioners within their own specialty to liaise with. Being aware of their limitations is important for all users to consider. Normology promotes a culture to seek help when appropriate. Adopting preceptorship models may be beneficial to ensuring support is not removed when a trainee has passed a competency assessment.
Evidence
PoCUS is well established and likely to become more prevalent with time, hence, an increase in education and training is inevitable, regardless of whether its use is accepted. Initiatives to deliver this should be based on the best available scientific evidence. For this reason, it is necessary to evaluate the impact of training PoCUS for clinical practice, including the feasibility of how this can be delivered at various stages of training, especially in medical schools. Normology is no exception and should be further evaluated.
Conclusion
Achieving PoCUS competency does not mean that the trainee has reached expert level, rather it is a transition from one stage of entrustment to another – ie, supervised to non-supervised practice. The trainee will still need to access more experienced, and at times, expert guidance, which should be encouraged. We proffer that this level of entrustment can be reached without needing to scan patients suspected of having the target pathology. This would allow most of the training to be done outwith the clinical environment, using ‘normal’ volunteers, in planned sessions. However, it is important that trainees still scan a range of ages, body sizes and shapes. Such planned training sessions can facilitate a larger number of trainees than would be possible in a clinical environment. This is a pertinent consideration as we expect an increase in trainees requiring PoCUS skills in the future. It can also facilitate inter-specialty collaboration and invited faculty are less likely to be distracted by clinical activity. When patients are scanned in the clinical environment, trainees should already have a good level of ability. Resources can be provided to the trainees, such as images and video loops of pathology, but the novice trainee should not be expected to have experienced these in clinical practice. The focus should initially be on familiarity with normal appearances, as exposure to abnormal pathology will come later in the entrustment journey. In summary, normology principles will help PoCUS trainees at the start of training to achieve the knowledge, skills and behaviour to reach a level of entrustment that does not require direct supervision. Initially, confirming something is not normal is good enough.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and Consent
Not applicable.