
Abstract
OBJECTIVE
To improve patient outcomes and promote health equity, medical students must be taught not only biomedicine, but also the social sciences to understand the larger contexts in which patients live and health care operates. Yet, most undergraduate medical education does not explicitly cover these topics in a required, longitudinal curriculum.
METHODS
In January 2015 at Harvard Medical School, we created a two-part sequence (pre- and post-clerkship) of required, 4-week multidisciplinary courses—“Essentials of the Profession I and II”—to fill this gap. “Essentials of the Profession II (EOP2)” is an advanced social sciences course anchored in patient narratives and the lived experiences of students and includes clinical epidemiology and population health, healthcare delivery and leadership, health policy, medical ethics and professionalism, and social medicine that engages students to conduct structural analyses to be effective healers, advocates, and leaders.
RESULTS
Per student course evaluations, the overall course rating was 1.7 (SD 0.9, 1 = excellent and 5 = poor); its overall rating has improved over time; and it has scored well even when run virtually. It was rated highly in application of critical thinking, integration of the disciplines, and relevance for clinical work. Qualitative analyses of student responses revealed the following key course strengths: breadth of topics, teaching faculty and guest speakers, and small group discussions. The weaknesses included workload, lack of diversity of opinions, repetition, and time spent in lectures.
CONCLUSIONS
We argue that EOP2 is “essential” for post-clerkship medical education. It offers an opportunity to re-ignite and enhance humanism and activism; remind students why they chose the medical profession; equip them with frameworks and toolkits to help them to overcome challenges; and devise solutions to improve health care and patient outcomes that are applicable to their future training and ongoing practice of medicine.
Introduction
What does this student need to know to provide optimal care for this patient? Traditional medical training focused on basic and clinical sciences would have equipped this student to understand the microbiology of SARS-CoV-2, perform a physical exam that assesses pertinent findings, and judge the indications for intubation. However, to effectively care for this patient, medical students must be taught to go beyond the biomedical. They need an understanding of the healthcare system, a patient's social and economic contexts, and overarching societal issues that impact health outcomes. In this vignette, the student should consider effective, evidence-based interventions to treat COVID-19 as the literature rapidly evolves; the structure and (dys)function of the healthcare system to meet this patient's needs, both acutely and chronically; the medical profession's obligations towards underserved patients; how to name and address their own moral distress; the historical factors that led to disproportionate rate of COVID-19 cases in communities of color; and the best ways to care for patients who speak other languages and/or have low health literacy. Yet, most undergraduate medical education does not explicitly cover these topics in a required, longitudinal curriculum. Hence, students lack important knowledge and skills and how to apply them to optimize patient outcomes. At HMS, we created a two-part sequence (pre- and post-clerkship) of required, 4-week multidisciplinary courses to fill this gap. This design ensures that students have foundational knowledge that prepares them for what they will encounter during clerkships, followed by another rigorous course after being immersed in the realities of clinical practice that allows them to reflect on those encounters. We have described the pre-clerkship course previously. 1
In this article, we present findings from our post-clerkship multidisciplinary course, “Essentials of the Profession II” (EOP2). 2 We launched our course in March 2018 as part of the HMS “Pathways” curriculum reform. 3 The course integrates content across five disciplines (clinical epidemiology and population health (CEPH), healthcare delivery and leadership (HCDL), health policy (HP), medical ethics and professionalism (MEP), and social medicine (SM)); highlights clinical relevance and application; and discusses and debates solutions from multiple perspectives to promote optimal care and health equity. Students share patient narratives and health system issues encountered during their core clerkships to anchor discussions. As a multidisciplinary course, we are greater than the sum of our individual disciplines. The two-course sequence provides spacing (time between topics), interleaving (a mixing of more than two topics), and variability (different pedagogical strategies), which are key to retrieving information and making learning and knowledge stick. 4 To our knowledge, this is the first description of a post-clerkship, mandatory, multidisciplinary social sciences course at a U.S. medical school. We emphasize the significance of this course in the post-clerkship curriculum; describe our integrated pedagogy; provide results from student evaluations; and describe steps and explore potential barriers medical educators may face in implementation.
Background
In 2004, emphasizing the importance of the social determinants of health to health outcomes in the U.S. population, the National Academy of Medicine called for an increased focus on the social sciences in medical school curricula. 5 Despite these recommendations, medical student surveys reveal they consider social sciences to be underemphasized in medical school education, 6 resulting in calls for new curricula.7–9
During medical school, students are exposed to three types of curricula: a “stated curriculum” (courses, lessons, and learning activities students participate in and knowledge and skills educators intentionally teach students), an “informal curriculum” (the ad hoc, unscripted, interpersonal teaching and learning between faculty and students that takes places outside of the classroom), and a “hidden curriculum”(the unspoken and unofficial values, perspectives, and lessons to which students are exposed).10–18 Medical students describe the hidden curriculum as a powerful influence in shaping their experience, 19 yet medical schools rarely address how the hidden and informal curriculum shapes students and their values and principles in a longitudinal way that spans the 4-year continuum. 20
Currently, most U.S. medical schools do not teach social science disciplines. When they are taught, they are often not mandatory, nor multidisciplinary, and do not extend beyond the pre-clerkship period.1,21–23 Our two-course sequence, in contrast, provides students additional rigorous, developmentally advanced education to frame and address the health inequities and care inefficiencies they observed during their clerkships.24–30
Methods
Overall course description of essentials of the profession II
Our course operates under four key assumptions: students want to provide optimal care to their patients; students want their patients to achieve optimal health outcomes regardless of their social and economic contexts; students want to be effective agents of social change; and students experience cognitive dissonance when they face obstacles to accomplishing these goals. In EOP2, students confront concepts previously introduced and debated during their required first-year course in light of their new clinical experiences and discuss the informal and hidden curricula they have experienced. Advanced topics (eg, medical malpractice, value-based health care, moral distress, and innovative approaches to fighting racism in medicine), and contemporary topics (eg, opioid crisis, climate change, and the COVID-19 pandemic) are included.
Post-clerkship medical students are well-positioned to understand how the health care system operates, while also maintaining a relative “outsider” view that promotes creative thinking about large-scale change. 31 Our course is a valuable touchstone in the overall HMS curriculum. It instills a critical thinking and solution-oriented growth mindset for students to incorporate throughout their careers. It helps students acquire skills and tools to interpret and apply medical evidence, understand their professional role, perform structural analyses, advocate for health system and societal changes to improve population health, and ultimately become leaders and innovators in medicine.
Clinical epidemiology and population health
The CEPH component teaches students introductory skills in statistics, epidemiology, and study design. Students then use those skills to evaluate and interpret journal articles and discuss how to incorporate published literature into clinical practice. Residents and attendings who complete evidence-based medicine training are more likely to provide proven treatments, yet medical students are rarely explicitly trained in this skill.32–35 Feedback from practicing physicians suggests that statistical education in medical school is particularly valuable after students have clinical experience. 36 During CEPH, students read an assigned journal article in advance and propose questions related to methodology, study design, analysis, interpretation, generalizability, or clinical relevance; lead journal clubs in small groups; and attend lectures where the authors of the assigned journal articles discuss the study design, conclusions, and limitations. Students learn how to critically assess a paper’s conclusions based on the evidence presented and discuss how to use high-quality evidence to inform clinical care.
Healthcare delivery and leadership
The HCDL component's objectives are to understand the key tenets of value-based healthcare and their application to healthcare organization, delivery, assessment, leadership, and equity. Harvard Business School (HBS) faculty teach the business school's health care cases to illuminate topics like integrated practice units, bundled payments, and addressing the social determinants of health. It gives students who are not pursuing a business degree the chance to explore value, outcomes measurement, and cost-containment. 37 Students assume the role of the protagonist while also critiquing how different healthcare systems operate, an opportunity typically only afforded to physicians in leadership positions. Students are encouraged to challenge the status quo and innovate. By giving students the tools to think about how healthcare is run and discuss how the system could be changed, HCDL prepares students to be future healthcare leaders.38,39
Health policy
In the HP component, students assess the policy context in which the U.S. healthcare system operates and how it impacts clinical practice, as well as discovering opportunities for innovation and reform. During clerkships, students saw firsthand how concerns about achieving specific quality metrics and medical malpractice influence clinical practice.7,40–42 HP builds upon healthcare fundamentals (eg, role of health insurance, Medicare and Medicaid, payment models for physicians and hospitals, and factors underlying health disparities) taught in Essentials of the Profession I (EOP1). It also addresses student clerkship experiences and advanced topics like quality improvement in healthcare, the role of government in financing and providing healthcare, implicit bias, and structuring policies to promote medical innovation.
Medical ethics and professionalism
MEP encourages students to reflect on clinical experiences that triggered ethical concerns. This process helps them identify their own moral distress, articulate underlying ethical tensions, integrate formal ethical concepts with their lived experiences, and develop nuanced thinking about past experiences.10–12,43 Small group discussions are facilitated by physicians with ethics training to help students explore controversial topics including medical aid in dying, rationing, and reproductive autonomy. MEP draws on existing clinical vignettes, students’ stories, current dilemmas in clinical care and HP, and relevant Supreme Court decisions. Students engage in role-playing, placing themselves in the role of patient or practitioner to allow for more immersion into ethical dilemma scenarios.44–46 Students contemplate and refine their response to common ethical dilemmas that they will continually face throughout their careers, becoming conversant with contemporary and evolving moral standards and expectations of the profession.
Social medicine
In the SM sessions, students identify and confront social and structural forces that affect patients to develop strategies that can improve clinical care and advance health equity. Students learn the science of SM and explore how key social and structural determinants of health—such as housing, food insecurity, the climate crisis, mass incarceration, and racism—act as drivers of health inequities. Students engage in serious dialogue with their peers, study programs, and tools that can transform culture and policies, and gain skills to become advocates. SM provides examples of partnerships with community-based organizations (eg, food banks, violence-prevention agencies) and other professionals (eg, lawyers, community health workers, community organizers) to address patients’ social needs, advance health equity research, and dismantle structural barriers. These organizations and individuals are guest lecturers who teach the students in the classroom space and via site visits. They model how students can address these topics in residency and future practice. For example, an emergency room physician who also works in government relations leads a session on legislative advocacy, and students practice giving oral testimony on a current bill in small groups. Another session is led by resident physicians who present their process of conducting a race-based disparities research study, presenting the findings to hospital leadership, and implementing lasting policy changes to promote health equity. 47 SM frames the achievement of health equity as the professional responsibility of physicians, not as an extracurricular activity. 48
Course logistics
Faculty from across the disciplines collaborate to create sessions that emphasize integration and diverse perspectives and avoid duplication. A flipped classroom pedagogy is used: pre-assigned readings, videos, and assessments ensure knowledge acquisition, encourage reflection, elicit opinions, and prepare students to engage in lively, advanced in-class discussions.49–51 We estimate 1 hour of prep work per hour of class time. Trained faculty from each discipline prepare to facilitate discussions by reading the same materials and a detailed faculty guide. We deliberately assign students to small groups to optimize diversity and an environment that promotes maximal participation from the greatest number of students.
The course culminates in a final project that includes an oral presentation and written product. Projects must integrate cross-disciplinary perspectives from at least two EOP2 disciplines. Recent examples include studies of COVID-19 and efficacy of social distancing, how to pay for surprise medical bills for the un- and under-insured, and the ethics of mandated COVID-19 vaccination for healthcare workers. The final projects can take many forms, including op-ed, policy memo, scholarly analysis of a patient they cared for during their clerkship, research proposal, or proposal for new course content. Final projects have been published in peer-reviewed journals, blogs, and major newspapers; incorporated into the course curriculum; and expanded into year-long research projects.52–54
During the course, we work closely with student medical education representatives to revise and refine pedagogical strategies and content based on real-time student feedback. After the course, faculty debrief with medical education representatives, review course evaluations, and reassess topics based on clinical and contemporary relevance and opportunities for cross-disciplinary exploration. The course requires continuous revision to stay relevant and keep students fully engaged.
Study design and analysis
The third-, fourth-, and fifth-year medical students at Harvard who completed the course were asked to complete an anonymous course evaluation after the course ended, as they do for every course they take at HMS. All students who completed the survey between 2018 and 2020 were included, with no further exclusion criteria.
Demographic information on students enrolled in the course between 2018 and 2020 was collected from the school's registrar office. The survey consisted of rating scale questions and open-ended questions. Open-ended questions asked students to comment upon “the strengths of the course,” “areas in which this course could be improved,” “how issues related to culture, ethnicity and socioeconomic status, as they affect the topics in this course, were addressed,” “the educational environment created by this course,” and feedback on each section of the course (SM, ethics, etc). Rating scale questions included, “Please rate the course overall” (1 = excellent, 5 = poor), “This course consistently engaged me to apply critical thinking to solve problems” (1 = strongly agree, 5 = strongly disagree), “Please rate how well the five disciplines (MEP, HP, SM, clinical epidemiology and population health, HCDL) were coordinated with one another to facilitate your learning” (1 = excellent, 5 = poor), and “How relevant is this course to your clinical work?” (1 = a great deal, 4 = not at all). Rating scale responses were analyzed with means and standard deviations. Two authors with backgrounds in qualitative analysis independently coded the open-ended responses for themes (JK and JLG).
This project was undertaken as a Quality Improvement Initiative and as such does not constitute human subjects research. Consent was not obtained from individual subjects because data was initially collected for educational quality improvement rather than for research purposes. The data gathered was anonymous and presented no more than minimal risk to subjects. The Harvard Medical School Program in Medical Education's Educational Scholarship Review Committee waived the need for ethics approval and waived the need for informed consent for this study.
Results
Quantitative results
HMS students complete anonymous course evaluations for all courses. Of the 378 students who took our course between 2018 and 2020 (see Table 1), 332 completed the evaluation (87.8%). The overall course rating was 1.7 (SD 0.9, 1 = excellent and 5 = poor), its overall rating has improved over time, and it has scored well even when run virtually (see Figure 1). This is comparable to post-clerkship, elective Advanced Integrated Science Courses’ ratings (see Table 2). Most students rated the course as “a great deal” or “somewhat” relevant to their clinical work; said they “strongly agree” or “somewhat agree” that the course consistently engaged them to apply critical thinking to solve problems; and reported the coordination of the five disciplines to facilitate learning was “excellent” or “good” (see Figure 1).

Essentials of the Profession II ratings on key course indicators (scale 1-5, 1 is highest ranking).
Student demographic data (total enrollment from March 2018 to October 2020).

Comparison of overall course rating between essentials of the profession II and advanced integrated science courses.
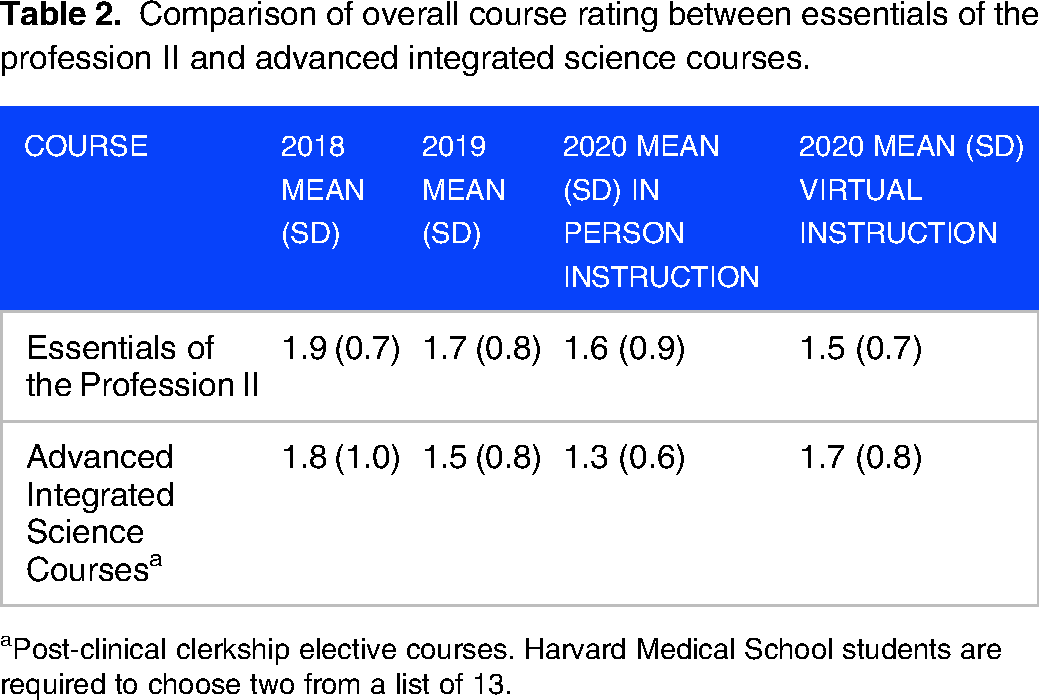
Post-clinical clerkship elective courses. Harvard Medical School students are required to choose two from a list of 13.
Qualitative results
Course strengths
Course evaluations also contain optional open-ended questions. Of the 376 who completed the course evaluation, 216 (57.4%) wrote about course strengths. As pertains to course strengths, the most prominent themes were the following:
Breadth of important topics. One student said EOP2 provided, “A well-coordinated overview with some deep dives into key areas. I appreciated that issues discussed were contemporary and important for emerging physicians.” EOP2 faculty and expert guest speakers. One student stated, “The faculty were amazing and inspiring. They went above and beyond in every way, probing us to think more deeply and listen more carefully.” Small group discussions. A student commented, “I consistently learned more from my classmates than anyone during this course. I loved hearing their interpretations of the readings, their reflections from their clinical experience, and to hear how they think their careers will be impacted by the knowledge that we learned from the course.” Another student spoke about faculty facilitation: “I was so impressed by the grace and nuance with which the faculty facilitated small and large group discussions.” Clinical relevance. One student reported, “It was really cool how this course's location at the end of the curriculum allowed us to return to our previous clinical experience with a new lens.”
Course weaknesses
A smaller number of students (193, 51.3%) also commented on shortcomings of the class; the most salient themes were the following:
Workload and amount of reading. A student said, “I felt there was too much reading, and I wasn't able to do as much reflecting on the issues of discussion that day as I would have liked.” This is a perennial issue. Similar to their clerkships, there is a body of scientific literature that we want to expose students to master the application of social science in medicine. We strive to find the most salient articles and audio-visual materials both to animate discussion and create a reference library that students can refer to throughout their careers. Lack of diversity of opinions. One student shared, “One of my biggest issues with the course was that it felt at times as though different perspectives were not included.” Politicization of EOP2's complex topics is an inevitable issue. We strive to elicit a diversity of opinions in three ways: (a) we explicitly state that we cover complex topics that require us to value a variety of perspectives, and stress that diversity of backgrounds and ideas produces more robust solutions; (b) use a variety of pedagogical strategies (eg, polling, debate, role-playing); and (c) we anchor discussions in health equity. Content repetition. Including similar topics from the perspective of different disciplines is a challenge. The discipline directors meet routinely throughout the year to collaboratively create course content that is synergistic but not repetitive. We meet annually with EOP1 faculty to build on topics and provide opportunities for students to review concepts from EOP1 since information retrieval is a key element of learning.
4
Time spent in lecture. One student commented, “Large group sessions were generally much less engaging than small group.” This was a theme raised by several students, while many others rated the lectures highly. We believe it is important for students to hear from a lecturer who is an expert in their field. Also, engagement in large group sessions has improved as teaching faculty institute innovative tools (eg, polling, break-out spaces) to increase participation.
Discussion
We identify several potential challenges at the student and faculty level that were not present in student evaluations. A few students balk at a required course like EOP2 because of lack of interest in the content, scheduling obstacles, and competing requirements (eg, sub-internships, away rotations, residency applications and interviews, and national exams). EOP2 cannot be tailored for the unique post-clerkship needs and interests of each individual student. Potentially salient topics for the practice of medicine not covered by EOP2 include law, information systems, and practice management. These are inevitable compromises and a perennial challenge among medical educators to maintain openness and flexibility in choosing course content. In our experience, EOP2 faculty have been successful in engaging both students who have specific interests in our course content and those not naturally inclined.
Our study has limitations. Our sample size was small and included students from a single medical school. The questionnaire used was not validated or pilot tested and instead was designed for students to give feedback to allow for iterative improvements to the course (Supplemental material S1). Many of the questions are standardized across feedback surveys for all courses at HMS and therefore may not be optimized for reliability and accuracy. Not all students who took the course completed the survey. Many students chose not to answer the open-ended survey questions, so the themes determined from qualitative analysis represent the opinions of a subset of students. The course may be difficult to replicate in other medical schools without the same faculty diversity and resources.
Our course maintains rigor and diversity because each discipline is taught by experienced educators who also practice clinical medicine, conduct research, and/or perform activities outside HMS (eg, serve on hospital ethics committees, teach at HBS, work at the Boston Department of Public Health); these faculty speak and teach from their lived experience. On average, faculty devote approximately 50 hours in course preparation and debrief, creation and delivery of didactic materials, feedback on final project ideas and presentations, and student office hours. We have a relatively low student to faculty ratio (ie, 10:1). The teaching faculty have found our course a rewarding endeavor.
Essentials of the Profession II is a high-caliber course that students have found rewarding. As part of a two-course sequence, it provides optimal exposure at the optimal time in medical students’ development, equipping future physicians with the skills they need to conduct structural analyses of patient illnesses and healthcare systems, create solutions, and be advocates for change to promote equitable patient care and health outcomes. EOP1 provided scaffolding that EOP2 expands and enhances. The combination of space, interleaving, and different pedagogical strategies increases the stickiness and retrievability for future clinical practice. 4 EOP2 explicitly includes the informal and hidden curriculum in small group sessions, allowing students to react, reconcile, and discern how to deal with these issues in residency and throughout their careers. 55
Medical students’ attitudes change most drastically during the student's clinical years, with a significant decrease in idealism27,29 and empathy during and after clerkships.25–29,56 Medical educators and bioethicists theorize that these changes are by-products of the moral dilemmas and contradictions that students experience during their clinical years, especially as the students feel inexperienced and powerless.57–62 One antidote is to provide an introduction to concepts of CEPH, HP, MEP, and SM prior to students’ core clinical experiences (ie, to prime the students), followed by consolidation and advancement of these concepts, along with the addition of HCDL, after core clinical experiences. If students’ humanism waned during clerkships, EOP2 offers an opportunity to re-ignite and enhance humanism and activism, remind students why they chose the medical profession, prepare them to overcome challenges, and devise solutions applicable to their future training and ongoing practice of medicine. 63
Conclusion
As one student wrote, the value of the Essential of the Profession II course is that it teaches students “about the water in which we will swim.” Despite the challenges, EOP2 successfully provides students deeper exposure to disciplines that are highly relevant to clinical practice yet often overlooked in traditional medical curricula, a space to reflect upon their own clinical experiences to better understand patients’ lives and optimize care, and tools to innovate in healthcare and advocate for health equity. Our patients and society require nothing less.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241232184 - Supplemental material for “The Water in Which We Swim:” A Unique, Post-Clerkship Multidisciplinary Course
Supplemental material, sj-docx-1-mde-10.1177_23821205241232184 for “The Water in Which We Swim:” A Unique, Post-Clerkship Multidisciplinary Course by Jessica N. Laird-Gion, Laura F. Garabedian, Rachel Conrad, Adam C. Shaffer, Mary L. Witkowski, Camila M. Mateo, David S. Jones, Edward Hundert and Jennifer Kasper in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
None.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contributions
All authors contributed to study conception and design and completed editing and review of the manuscript. Jessica Laird-Gion and Jennifer Kasper completed data collection, analysis and interpretation of results, and initial manuscript preparation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.