
Abstract
OBJECTIVES
There is little data evaluating procedural skills in current rural pediatric practices. In order to prepare a cadre of pediatricians to work in rural settings, we require an understanding of the unique procedural skills needed by rural pediatric providers. Our objective was to determine how often pediatricians performed various procedural skills, determine the importance of these skills to current practice, and how they differ between rural and urban pediatric providers.
METHODS
A survey evaluating pediatrician utilization of the 13 required Accreditation Council Graduate Medical Education procedural skills in current practice was developed and distributed to pediatric providers in New Mexico. Descriptive statistics were used to profile participants and describe survey responses. Chi-square tests were used to evaluate differences by urban setting or IHS. Fisher’s exact test was employed to assess differences if cell sizes were less than five. All p-values were two sided with alpha=.05. Benjamini-Hochberg method was used to control for type 1 errors.
RESULTS
Fifty-two of 216 pediatric providers responded. The majority surveyed performed each of the 13 procedures less than monthly but competency in many of these procedures is important. Thirty-two respondents submitted free-text responses recommending competence with tracheostomy changes, gastrostomy-tube changes/cares, and circumcision.
CONCLUSION
Majority of surveyed pediatricians performed the required procedures less than monthly but deemed several procedures to be important. Rural pediatricians recommended specific procedural skills needed in rural practice. All trainees receive procedural skills training. However, trainees interested in rural practice may need additional training in specific skills different than their non-rural counterparts.
Introduction
New Mexico (NM) is a rural/frontier state with a population of 2.1 million people and a child population of 488 476 children. 1 There are 58.5 general pediatricians per 100 000 children and almost half of the 33 counties are without any pediatricians. 1 Rural counties contain few, if any, pediatric specialists and sub-specialists. This distribution is also true of many rural states across the country. Across the US, there is an average of 74 pediatricians per 100 000 children. However, in more populous regions, that number is as high as 105.0, 101.7 and even 237.2 (Connecticut, New York, and Washington D.C., respectively); mountain region states such as Wyoming (40.3), Utah (52.4), and Nevada (40.8) have much lower number of pediatricians per 100 000 children. 1 There is an increased concentration of pediatric providers in more densely populated areas, and physician recruitment and retention in rural America continues to be a challenge.2,3
To address the rural healthcare needs, federally qualified health centers, rural health clinics, and critical access hospitals have been established throughout rural America.4‐6 This begins to address the overall healthcare demands in rural areas, but it does not differentiate between adult and pediatric care needs. Rural hospitals have less access to pediatric physicians, and the low volume of children presenting to their EDs makes it difficult for staff to maintain pediatric care skills. 7 This fact likely contributes to the higher child mortality seen in rural areas as compared to urban areas. 8
The low concentration of pediatric-trained providers in rural areas is an additional challenge for the children who live in these areas, especially those with multiple medical complexities requiring pediatric specialty care. Children from rural areas who are hospitalized tend to have more medical complexities. 9 Therefore, general pediatric providers in that environment need to be comfortable with many aspects of sub-specialty care and be prepared to manage certain procedures. 10 Compared to their urban counterparts, rural providers do not have the conveniences of local tertiary care support.
Literature suggests that recruiting students from rural areas and increasing exposure to rural medicine during training helps to increase recruitment and retention of rural physicians.11,12 However, we have little data and anecdotal evidence about the specific skill sets needed to work in these rural areas, especially in pediatric care. Our goal is to prepare a cadre of pediatricians prepared to work in these rural settings. Therefore, we required an understanding of the medical skills needed by the rural community providers and their patients.
The Accreditation Council for Graduate Medical Education (ACGME) establishes and monitors educational standards for all medical residency and fellowship training programs. 13 ACGME determined that by the end of graduate medical education, pediatric residents must be competent in 13 procedural skills. 14 These procedural skills are identified as essential for practice in the general pediatric setting. 15 However, there is limited data as to what procedural skills are practiced by general pediatricians today, and how it may vary based on practice location or type. Ben-Isaac et al evaluated residents who graduated from their urban program and noted that they were more likely to perform urgent procedures (fracture care, laceration repair, incision and drainage of abscess, foreign body removal) than emergent procedures in their pediatric practices. 16 Iyer compared ACGME procedures training guidelines with current clinical practice in Ohio and determined that pediatricians rarely performed most of the ACGME-required procedures. 17
There is a paucity of data directly addressing the current procedural skills needed in pediatric practice, and even fewer in rural/frontier areas. With the intention of developing a procedural skills list for pediatric trainees interested in rural practice, the objective of this study was to first understand the current frequency and importance of the 13 ACGME procedural skills practiced by pediatricians in NM, with secondary objective to evaluate the differences in procedural skills practiced by rural/urban and Indian Health Service (IHS) and non-IHS practices.
Methods
We conducted a prospective, cross-sectional survey of pediatric providers in the state of NM. NM is a state in the US Southwest, consisting of 33 counties (26 of which are considered rural). 18 Using Research Electronic Data Capture (REDCap), a structured survey was developed focusing on the 13 ACGME procedural skills. 14 The survey was divided into eight sections, in which procedural skills were divided into three groups—emergent, urgent, and office-based procedures, similar to Iyer et al. 17 Eleven questions regarding demographics, 13 questions regarding the frequency that each procedural skill was performed (almost daily, almost weekly, monthly, occasionally, almost never), 13 questions regarding the importance of maintaining competency in each skill (not at all, minimally, moderately, considerably, very important), and a free-response section. The survey was pilot-tested among eight separate pediatricians. They represented a mix of current or former members of the Association of Pediatric Program Directors, medical educators, and rural and urban providers with varying practice settings that were currently practicing within NM in order to achieve a diverse and heterogeneous pilot testing sample. Participants were then asked to rate the frequency in which they performed these procedures and the importance of competency in these skills. Of note, as survey respondents were the providers employing these procedures/skills in these rural areas on a regular basis, we allowed them to define “importance” and “competency” as they responded to the question, in order to avoid any bias which may arise should the investigative team attempt to do so (given a lack of objective, evidence-based standards in these settings). Participants were also given the opportunity to free-text additional recommended skills for current pediatric residency trainees.
In order to have representation from around NM, an e-mail list-serve was obtained from the New Mexico Pediatric Society and IHS, which included a convenience sample of 295 members. Only pediatricians or pediatric providers practicing in NM were included in the study. Providers who were not practicing in NM, other specialty services (ie, pediatric surgical specialties), and medical students were excluded. The survey was then distributed to pediatricians in NM twice, in August and December of 2019.
Data analysis
Descriptive statistics were used to profile participants (Table 1) and describe survey responses. Given the small number of respondents, participant responses regarding utilization of pediatric skills were then grouped as “at least monthly (≥12x/year)” versus “less than monthly (<11x/year),” and the rated importance of such skills was grouped as “moderately/very important” versus “minimally/not at all.” Both utilization and importance were compared by urban (<25 mi from a tertiary care center) versus rural (≥ 25 mi from a tertiary care center) practice setting (Table 2) and IHS versus other practice type (Table 3). Chi-square tests were used to evaluate differences by urban setting or IHS practice type. Fisher's exact test was employed to further assess differences if cell sizes were less than five. All P-values were two sided with alpha = .05. All analyses were conducted by Statistical Analysis Systems (SAS), v.9.4 (Cary, N.C.). Given the number of comparisons under-taken, the Benjamini-Hochberg method was used to control for type 1 errors, with a false discovery rate of 10% set a priori. 19
Demographics.

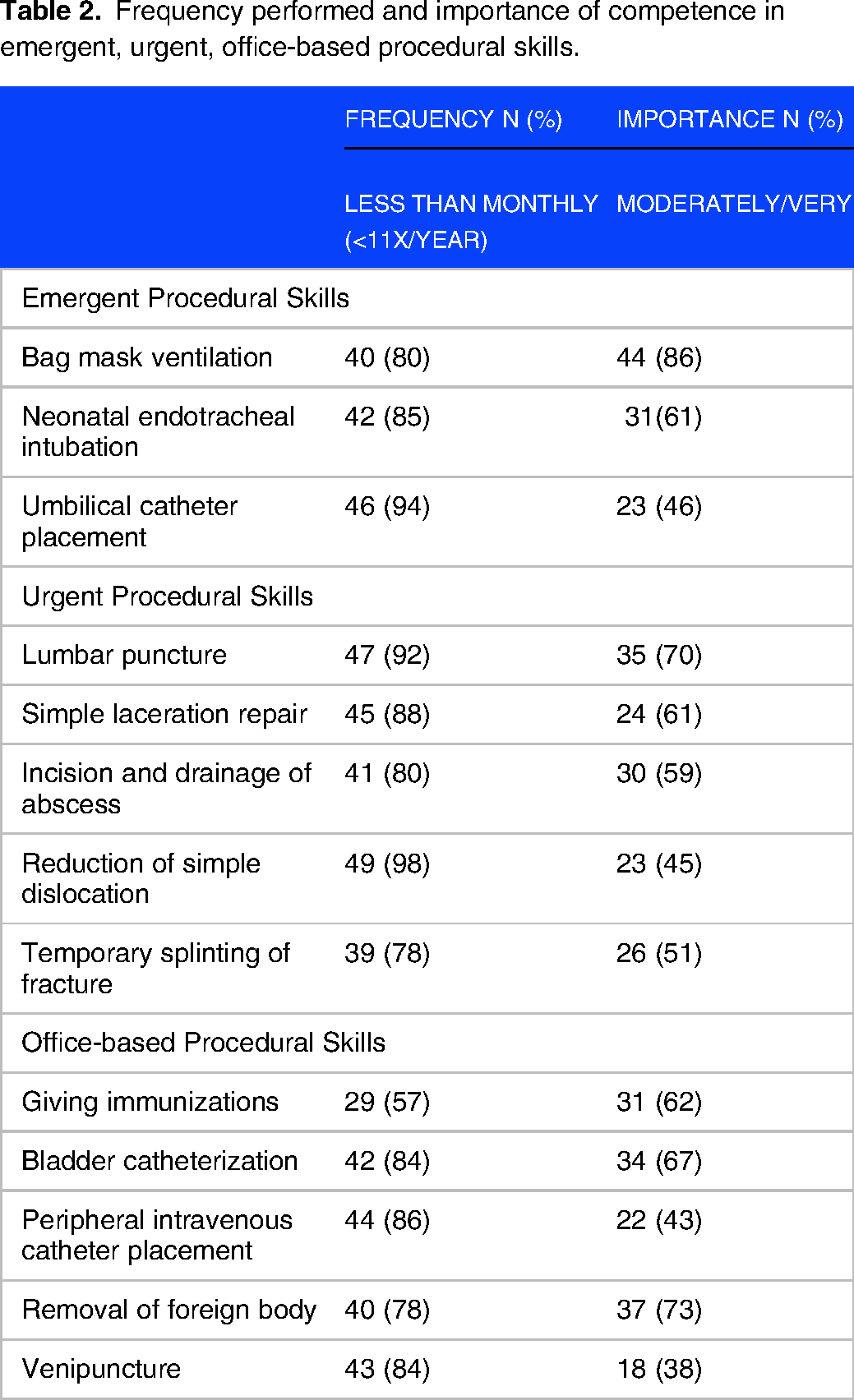
Frequency performed and importance of competence in emergent, urgent, office-based procedural skills.
Comparisons between urban and rural providers in their frequency of emergent, urgent, and office-based pediatric skills performed.

*Statistically significant; Chi-square tests used with significance determined with the Benjamini-Hochberg correction (false discovery rate 10%).
Free-text responses were qualitatively analyzed. Procedural skills that were not part of the 13 ACGME procedural skills, written in the free-text responses, and mentioned by more than one provider were flagged. Medical knowledge topics that were written in the free-text response and noted by more than one provider were also flagged.
This study was approved by the Institutional Review Board at the University of New Mexico (study ID 19-379, approved on 31 July 2019). Participants provided written informed consent before participation in the study.
Results
A total of 295 individuals were sent the survey; 216 were pediatric providers in NM and eligible to respond; 50 pediatrician and two advanced practice provider responses were received. A total of 52 responses were thus included, with a response rate of 24%. Participant demographics are listed in Table 1, in which all participants completed pediatric-specific training and share similar demographic distribution to NM pediatricians.20,21 Not all 52 respondents answered every question, ranging from 49 to 52 responses for each question. All respondents completed pediatric-specific training (Table 1). Thirty-seven respondents (71%) had more than 10 years in practice. Respondents worked in a variety of practice settings including inpatient, clinic, urgent care/emergency department, newborn nursery, and newborn deliveries. Fourteen respondents (27%) worked for IHS. Twenty-five (48%) respondents worked in a rural area. There were respondents from various counties throughout NM. Thirty-one (60%) respondents worked in a community with >50 000 persons.
Table 2 represents the frequency of 13 ACGME procedures that are performed less than once a month; it also shows the rated importance of competency in these skills, ranging from 38 to 86%. A majority of practitioners perform emergent, urgent, and office-based procedures less than once a month. However, respondents viewed a majority of these same skills as moderately/very important to maintain competence: bag mask ventilation (86%), removal of foreign body (73%), lumbar puncture (70%), bladder catheterization (67%), immunizations (62%), neonatal endotracheal intubation (61%), simple laceration repair (61%), incision and drainage of abscess (59%), and temporary splinting of fracture (51%).
Rural versus urban responses
When comparing responses from rural and urban providers for each of the 13 ACGME procedures, there was a statistical significance in that urban providers were more likely to perform endotracheal intubations (P = 0.006) and umbilical catheter placements at least monthly (P = 0.05) (Table 3). However, rural providers were more likely to view competence in umbilical catheter placements as moderately/very important (P = 0.02) (Table 4). However, after correction for multiple comparisons, placing umbilical catheters and the importance of competence in placing umbilical catheters did not retain statistical significance. There were no other statistically significant differences between rural and urban pediatric providers either in frequency of performing (Table 3) nor perceived importance of competence (Table 4) in the 13 ACGME procedural skills.
Comparisons of urban and rural providers in their assessment of the importance of competence in emergent, urgent, and office-based pediatric skills.

IHS versus non-IHS pediatrician responses
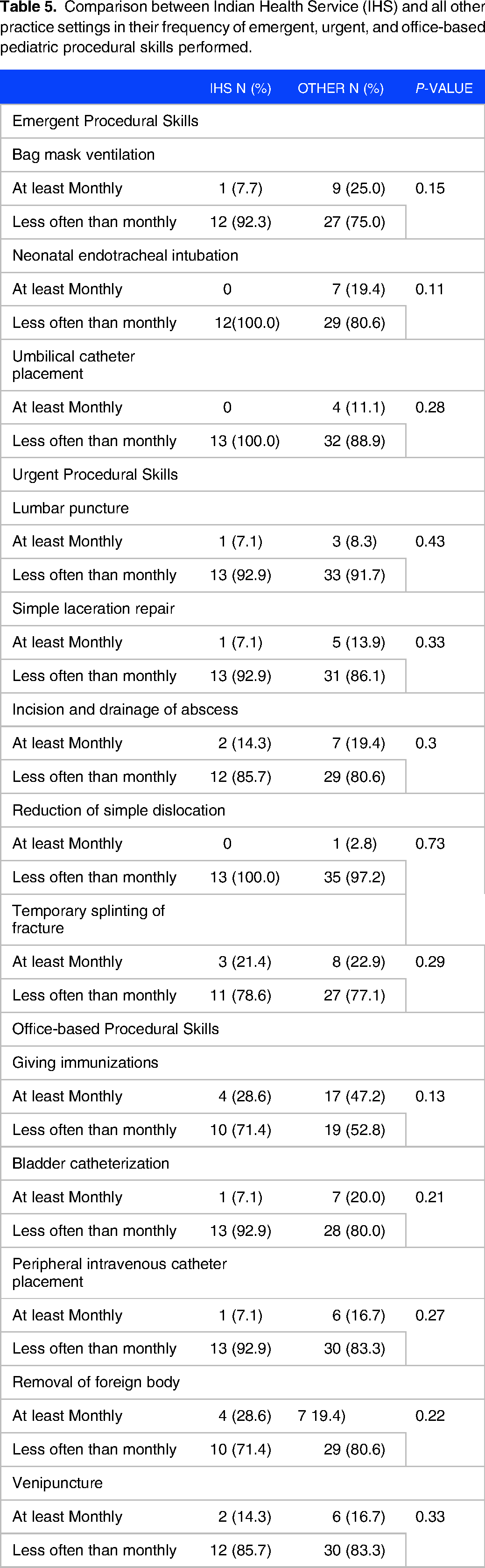
A subset of the rural pediatric providers surveyed included pediatric providers at IHS. Compared to other participants, IHS pediatricians also perform the 13 ACGME-recommended procedures less often than monthly. There were no statistically significant differences between the frequency of procedures used between IHS and non-IHS providers (Table 5). IHS providers, compared to non-IHS providers, rated that competence in umbilical catheter placement is moderately/very important (P = 0.02), and competence in bladder catheterization is minimally/not at all important (P = 0.02) (Table 6). However, both did not retain statistical significance after correction for multiple comparisons.
Comparison between Indian Health Service (IHS) and all other practice settings in their frequency of emergent, urgent, and office-based pediatric procedural skills performed.
Comparisons of Indian Health Service (IHS) and all other practice settings in the importance of competence in emergent, urgent, and office-based pediatric procedural skills.

Non-ACGME-recommended procedures
Thirty-two of 52 respondents submitted free-text responses recommending competence in additional procedural skills not currently required by ACGME, as well as suggestions on additional medical knowledge topics. The procedural skills recommended by more than one provider regardless of practice type or location included gastrostomy feeding tube cares (14), tracheostomy changes (4), and circumcision (3). Sixteen of the 32 respondents were rural pediatric providers, including IHS-specific pediatricians. More than one rural pediatric provider emphasized the importance of competence in gastrostomy feeding tube cares (7), all procedural skills (4), neonatal cares (3), and blood draws (2).
Additional medical knowledge topics that were recommended by multiple providers included nutrition (specifically in former preterm infants, complex patients, obesity, neurologically devastated patients, tube feedings) (9), and psychiatric evaluation and care (specifically eating disorders and depression/anxiety) (5).
Discussion
NM is a rural/frontier state in which pediatric services are difficult to access, mostly due to a lack of specialists. 22 Surveying the pediatric providers in NM allowed us to assess not only the procedural skills needed by general pediatricians, but also of those pediatricians working in remote rural settings. This distinction is important when advising pediatric residents with interests in working with rural populations, including those at IHS.
More than 75% of NM pediatrician respondents infrequently performed the 13 required ACGME procedural skills. Our results were similar to those reported by Iyer et al for pediatricians in Ohio. 17 However, competency in many of these skills is still important to the surveyed pediatricians.
Comparing rural and urban pediatric providers, we saw a statistically significant difference only in the frequency of endotracheal intubations, with no differences in the importance of ongoing competency. However, how often pediatric providers utilize certain procedural skills does not equate to the importance of competency in these skills. There was a general non-significant trend that urban providers perform emergency procedures more frequently than rural counterparts. However, rural providers still express that emergent procedural skills are important. Compared to children living in urban areas, children who live in rural areas have less access, different barriers to care, and tend to have greater unmet medical care needs.23,24 Additionally, the lack of immediate specialty and sub-specialty support in rural areas may also affect the type and frequency of procedures performed by general pediatricians in daily practice. 25 Therefore, rural pediatricians need to be prepared.
When given the opportunity, rural pediatric providers reaffirm the importance of competency in all 13 procedural skills. Additionally, they acknowledge the need for competence in additional procedural and medical skills needed to care for children with medical complexities—troubleshooting malfunctioning gastrostomy feeding tubes, tracheostomy cares, newborn cares and circumcision, blood draws, and managing nutrition of children who are medically complex and with complex neurologic diagnosis. These recommendations likely correspond with the increasing number of children with medical complexities cared for primarily by general pediatricians.26‐28 These skills, therefore, need to be highlighted during important graduate medical training for trainees interested in rural healthcare.
We see a similar trend among IHS pediatricians. They work with a unique patient population with specific health needs.29‐30 While they do not perform the emergent, urgent, or office-based procedures any more than their non-IHS counterparts, surveyed IHS pediatricians suggested competence in procedures specific to caring for neonates.
It is important to recognize the limitations to this study: we used a listserv that included 216 pediatricians, which includes the majority of active pediatricians in NM. We had a response rate of 24%, as such, our conclusions are somewhat limited. This also hindered our ability to assess outcomes on a more granular level, such as by sub-dividing the frequency with which procedures were performed in greater detail, and by stratifying perceived importance of a skill beyond the two choices we provided (eg, with a Likert scale). However, there was at least 1 respondent from 10 of the 19 counties of NM with a pediatrician in 2020 1 ; respondents practiced in a variety of settings including inpatient, clinic, urgent care/emergency department, newborn nursery, and newborn deliveries; almost half of respondents worked in a rural area, and respondents worked in a variety of community sizes with varying years in practice. The survey was sent to pediatric practitioners with specific pediatric training and did not include other specialties that care for children. Given the exploratory nature of the study and the recruitment limited to the statewide listserv, we did not perform power calculations. The data may not be generalizable to all pediatricians, but it provides valuable insight and an opportunity to compare procedural skills utilized by different practice locations.
Ensuring that rural providers possess the necessary procedural skills is complex. Multiple studies have evaluated pediatric residency procedural skills training, curriculums, and simulations.31‐35 A prior study by Gaies indicates that specific procedural skills training successfully increases competency in procedural skills. 31 Recurrent simulation training has been sufficient to maintain intubation skills.32,33 However, very few studies identify training gaps between residency training and rural pediatric practice.34‐38 Identifying these training gaps is important for pediatric residents planning a career in rural pediatric practice. This could guide their valuable learning time to focus on the specific skills that will be needed in independent rural practice. Currently, no distinction is drawn between competencies required (and maintenance of competency) of rural and urban practitioners in the US after graduation (though the ACGME in the US has permitted the creation of rural training tracks at requesting institutions). 39 Study of potential benefits of rural training tracks and differing competencies for rural versus urban providers should be pursued, as well as which certification procedures are best to document proper maintenance of those skills. Various factors affect the type of procedural skills needed in practice; tailoring procedural training to the individual resident and their career goals could improve competency in important procedural skills. 40
This study looks specifically at procedural skills practiced by rural pediatric providers and identified several skills not highlighted in the 13 ACGME-required clinical procedures which may be of relevance to rural pediatric providers. However, additional studies are needed to help guide pediatric residents interested in rural practice and their program directors in designing individual curricula. This will likely require qualitative research investigating training needs from the perspective of both rural pediatricians and those in training. In addition, future studies should assess the role that family practice physicians play in the care of children in rural areas. Such providers may not have the level of comfort caring for children that pediatricians have. However, a greater number of family practitioners work in rural areas than pediatricians and thus they may find themselves providing pediatric care nonetheless.41,42 Family practitioners may potentially have greater comfort than pediatricians with some procedures which are practiced relatively commonly in adults (eg, laceration repair and abscess drainage), while exhibiting less comfort with others (eg, neonatal tracheal intubation).
Conclusion
Of the pediatricians in NM who were surveyed, the majority performed the 13 ACGME-required clinical procedures less than monthly. However, competence in many of these skills was still felt to be important. They also recommended additional procedural skills needed in current practice that are not required by ACGME. Understanding the current pediatric procedural skills needed in specific practice types, rural and IHS, can help pediatric residents interested in these practice types to focus their procedural skills training and advise individualized procedural skills curriculum.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241229772 - Supplemental material for Understanding the Procedural Skills Needed in Rural Pediatric Practices: A Survey of Rural Pediatric Providers in the State of New Mexico
Supplemental material, sj-docx-1-mde-10.1177_23821205241229772 for Understanding the Procedural Skills Needed in Rural Pediatric Practices: A Survey of Rural Pediatric Providers in the State of New Mexico by Christal P. Chow, Deirdre A. Hill, Walter Dehority and E. Anne Greene in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241229772 - Supplemental material for Understanding the Procedural Skills Needed in Rural Pediatric Practices: A Survey of Rural Pediatric Providers in the State of New Mexico
Supplemental material, sj-docx-2-mde-10.1177_23821205241229772 for Understanding the Procedural Skills Needed in Rural Pediatric Practices: A Survey of Rural Pediatric Providers in the State of New Mexico by Christal P. Chow, Deirdre A. Hill, Walter Dehority and E. Anne Greene in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
New Mexico Pediatric Society, Dr Brian Etheridge, Dr Gilberto Alvarez, Dr Neal Golkar, Dr Hengameh Raissy, members of University of New Mexico Pediatric Educators Academy including Dr Chandler Todd, Dr Amy Staples, Dr Lanier Lopez, and Dr Rebecca Craig; CTSC grant support (DHHS/NIH/NCRR #UL1TR001449) for statistical support.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by Susan B. Tully Endowed Professorship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.