
Abstract
OBJECTIVE
The use of transesophageal echocardiography (TEE) by certified registered nurse anesthetists (CRNAs) during noncardiac surgery is relatively uncommon despite its unique potential to diagnose causes of hemodynamic instability. To address this problem, educational endeavors designed to provide practical TEE skills to CRNAs are needed. The aim of the current study was to evaluate the feasibility, acceptability, efficacy, and utility of a 2-day focused TEE workshop in nurse anesthesia education that employed a protocol involving a limited number of views and used goal-directed, qualitative assessments of critical physiologic parameters.
METHODS
This was a prospective, observational study involving 14 second-year nurse anesthesia students. The cohort was evaluated following completion of this workshop by simulator-based testing involving hypothetical clinical scenarios, and this test data was analyzed according to the percent successful acquisition and interpretation of TEE views to determine immediate objective teaching efficacy. The acceptability, perceived efficacy, and perceived utility of the workshop were assessed by online survey, and survey responses were qualitative and quantitative in nature.
RESULTS
Participants acquired appropriate TEE views associated with clinical scenarios 99% of the time and correctly interpreted the pathology in those views 93% of the time. Participants uniformly perceived significant educational value in this workshop and intend to incorporate TEE in their future clinical practice.
CONCLUSIONS
A 2-day workshop to teach focused TEE to nurse anesthesia trainees directed by a streamlined protocol is feasible, acceptable, and perceived as useful by participants, and provides practical experience and entry-level competency in this point-of-care ultrasound modality.
Keywords
Introduction
Increasingly, transesophageal echocardiography (TEE) has become a standard monitor to assist with management of severe adverse hemodynamic events during noncardiac surgery.1,2 Recommendations for perioperative TEE supported by expert opinion and formulated into guidelines by professional organizations include the evaluation of acute, unexplained circulatory perturbations resulting in refractory hypotension or hypoxia.2,3 Such assessments define “rescue” TEE indications and involve identifying hypovolemia, global and regional ventricular function including right ventricular dysfunction arising from myocardial ischemia, pulmonary embolism, and cardiac tamponade.2,4,5 A broader application of perioperative TEE during noncardiac surgery includes its use for monitoring purposes in patients at increased risk of hemodynamic disturbances. 3
Although there is a lack of high-quality studies examining the risk-versus-benefit of intraoperative TEE in noncardiac surgery, 6 there are a limited number of absolute and relative contraindications to its use.7,8 It is also clear that the frequency of serious adverse events associated with TEE is low. 9 While TEE is an invasive monitor, the incidence of major complications associated with its use is likely 1 to 2 orders of magnitude smaller than a comparable complication rate associated with pulmonary artery catheters,9,10 with a mortality of less than 1 per 10 000 patients and morbidity (including odynophagia) of approximately 1 per 500 patients for perioperative TEE. 7 Unlike other forms of point-of-care ultrasound, TEE requires anesthesia, but such anesthesia is usually provided as part of surgery and TEE can be utilized consistently to assess hemodynamics without interference with surgical or resuscitative processes. Furthermore, there is a significant quantity of observational data indicating that intraoperative TEE commonly can discern the underlying pathology of hemodynamic compromise during noncardiac surgery, guide therapy to prevent its occurrence or mitigate its effects, and direct appropriate resuscitation when it occurs.6,11–14 Whether the use of intraoperative TEE in this setting changes surgical outcomes remains unclear. 6
Despite the value of focused TEE, most certified registered nurse anesthetists (CRNAs) do not employ TEE in their practice especially if their practice is exclusive to noncardiac surgery. 15 One perceived reason for the relative underutilization of perioperative TEE in this population relates to the lack of adequate education in the curriculum of most nurse anesthesia teaching programs. For this reason, recently both the Council on Accreditation of Nurse Anesthesia Educational Programs and the American Association of Nurse Anesthetists (AANA) have identified point of care ultrasound—a term that includes focused TEE (involving a goal-directed, qualitative technique with a limited number of views chosen to assess for a select number of pathologies; consistent with existing modified TEE protocols4,16)—as a desired skill in nurse anesthesia training.17,18 Note that the term “focused TEE” in this manuscript includes not only focused “rescue TEE,” defined as focused TEE performed acutely after the occurrence of hemodynamic collapse,4,8 but also use of a limited number of perioperative TEE views (focused) for more common monitoring purposes to provide potentially preventive, early warning of impending collapse in higher risk patients. 3
This level of TEE proficiency is less than that required for performing a complete basic perioperative cardiac examination as set forth by the National Board of Echocardiography (NBE), which involves 11 views. 2 Similar to basic NBE certification, training of nurse anesthesia personnel in focused TEE should be associated with an expectation that they would seek appropriate consultation with a more advanced echocardiographer if complex pathology was encountered. 2 Since hospital privileging in perioperative TEE is frequently based on NBE certification, this expectation readily could be incorporated into CRNA performance of this task.
It has been shown that most conditions leading to hemodynamic instability during noncardiac surgery are recognizable by TEE and that such recognition often alters management following the use of protocols with a few views (approximately 70% of these views demonstrating either hypovolemia or the absence of any major new pathology consistent with vasodilation as a cause of hypotension). Thus, an increased number of anesthesia professionals using a limited number of focused TEE views likely would add significant value to their professional capabilities.4,11 As such, a practical argument can be made that the use of TEE should not be restricted to those practitioners who choose the more arduous route of NBE certification involving experience with a larger spectrum of views but should include those individuals who safely employ a subset of these views to prevent, diagnose, and manage relatively common hemodynamic disorders. A key question then becomes how? ie, how does one realistically certify that CRNAs can safely begin to perform limited TEE exams in patients to monitor for, potentially prevent, and treat adverse circulatory events during noncardiac surgery?
In order to achieve competency in this limited point-of-care ultrasound (US) modality, it is important to have an educational curriculum with specific learning objectives. The curriculum could include a workshop for nurse anesthetists with no previous TEE experience with the following goals:
Teach a limited number of views consistent with TEE protocols that have been demonstrated to allow diagnosis of the common causes of intraoperative hypotension Teach TEE views that can be consistently acquired and interpreted with relative ease by the novice provider (ie, be feasible in a relatively short time span) Transform a potentially puzzling diagnostic modality into a positive educational experience Provide useful skills that allow nurse anesthesia providers to glean valuable insight into perioperative adverse events (ie, demonstrate competency-based potential efficacy).
The aim of the present study was to determine if a workshop employing a single instructor and a 2-day time span could achieve these goals with nurse anesthesia trainees with no previous TEE exposure. The workshop involved both didactic and simulation-based instruction. The latter teaching was particularly important to allow students to acquire the haptic experience of image acquisition (not just image interpretation) and thereby promoted the equivalent of the “shows how” level of Miller's pyramid of clinical competence (Figure 1).19,20 Furthermore, simulation-based TEE training has been demonstrated to be particularly effective in teaching this skill set to novice users.
21

Miller's pyramid for clinical assessment. Higher levels of the pyramid model are associated with increasing professional competence which can be assessed by different means. For example, “knows” can be evaluated by multiple choice questions, “knows how” by oral examination, “shows” by simulation, and “does” by clinical interactions.
Methods
This small scale, prospective observational investigation was not considered human research by the university Institutional Review Board, and the workshop was a mandatory part of a course in advanced anesthesia techniques for second-year nurse anesthesia trainees preceding their period of clinical immersion. Enrollment in this course was the only inclusion criterion. All 14 student nurse anesthetists in the course provided written informed consent and participated in the workshop, constituting the study cohort. Previous individual experience with TEE was the sole exclusion criterion, and none of the students had such experience. The workshop instructor was a board-certified anesthesiologist with approximately 25 years’ clinical experience with TEE in cardiac and noncardiac surgery and certified in basic perioperative TEE. Demographic details of the study cohort are provided in Table 1.
Demographics of study cohort.
Numbers in parentheses represent standard deviations.
Structure and learning objectives of the workshop
The workshop had didactic and simulation components followed by a simulation-based competency assessment and took place over 2 days. The didactic portion occupied an entire teaching day and occurred in 2 sessions, each 3.5 h in length and separated by a 1.5-h break. The simulation portion (on a separate day) involved 1 hour per student.
There were 4 broad learning objectives for the workshop:
Understand TEE fundamentals including the significance of a select number of TEE views Interpret 4 views commonly associated with focused rescue TEE in noncardiac surgery—the transgastric midpapillary short axis (TG MP SAX) view, the midesophageal 4 chamber (ME 4C) view, the midesophageal 2 chamber (ME 2C) view, and the midesophageal long axis (ME LAX) view (see Figure 2; a modification of a protocol proposed by Staudt and Shelton)
4
Reproducibly acquire these 4 TEE views during simulation Acquire and correctly interpret these same TEE views efficiently in the context of common adverse event clinical scenarios in noncardiac surgery (ie, in-context synthesis during simulation of objectives 2 and 3).

Simulator screenshots of the 4 views used in the focused transesophageal echocardiographic protocol: (A) transgastric midpapillary short axis; (B) midesophageal 4 chamber; (C) midesophageal 2 chamber; and (D) midesophageal long axis views. Abbreviations: Ao, aorta; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
The didactic sessions focused on objectives 1 and 2. Objectives 3 and 4 were undertaken with the TEE simulator. The final 15 min of these simulation sessions consisted of an evaluation of learning objective 4 in which students performed focused TEE to diagnose causes of refractory hypotension and/or questionable myocardial ischemia in 5 hypothetical clinical scenarios (Table 2).
Simulation evaluation.

Abbreviations: LV, left ventricle; LVEDV, left ventricular end diastolic volume; LVESV, left ventricular end systolic volume; MAP, mean arterial pressure; RV, right ventricle; SD, standard deviation; TG MP SAX, transgastric midpapillary short axis.
Didactic curriculum
The curriculum content for the didactic sessions was delivered in 2 sessions. Figure 3 illustrates the content of these sessions. In session I, practical TEE concepts were introduced including TEE contraindications (relative and absolute) and potential complications, image orientation, and the significance of omniplane angle manipulation. A step-by-step “how to perform” a basic 2-dimensional (2D) TEE exam was outlined that involved the following steps: Powering on and connecting the probe to the machine, entering patient information, selecting the image mode, choosing TEE presets, inserting the probe, acquiring, and centering the desired image, adjusting the image processing settings, and choosing the appropriate sector depth. Since a Doppler exam has limited utility in focused perioperative TEE, only basic qualitative continuous wave Doppler was discussed. 12 TEE views (ten midesophageal and 2 transgastric views) were detailed in this first session in order to provide an overview of TEE imaging potential. For each view, the specifics of how to obtain the view (including a logical flow from view-to-view), the anatomic orientations of those views, and the important structures visible in each view (and therefore the view's potential clinical utility) were identified. Didactic session II focused on TEE interpretation of relatively common, significant intraoperative issues and was taught via a case-based method (Figure 3).

Curriculum for the didactic sessions I and II of the workshop. Abbreviations: LVOT, left ventricular outflow tract; SAX, short axis; SWMAs, segmental wall motion abnormalities; TEE, transesophageal echocardiography.
The simulator
The simulator employed in this study was the CAE Healthcare Vimedix 3.3 TEE trainer with cardiac module (Figure 4). This device consisted of a mannequin torso with a laptop computer-based 2D TEE system that demonstrated simultaneous, continuous ultrasound (US) and augmented reality (AR) images of intrathoracic structures using a motion tracker. 22 The simulator TEE probe was nearly identical in configuration to an adult TEE probe, and TEE views were generated in a realistic fashion that varied with probe motion including depth of insertion, anteflexion-retroflexion, lateral flexion, and axial rotation. These views appeared on the laptop screen with a split view layout divided between US and AR displays. All the image processing options available for routine 2D TEE were available on the trainer, including an image pause option that maintained the probe position (and had considerable instructional utility). In addition to normal anatomy, the simulator software allowed display of the anatomy and imagery associated with approximately 60 pathologies that were employed for evaluation purposes in a “hidden” mode, where activity titles were not visible to students (see below).

Transesophageal echocardiography simulator. Trainer includes mannequin torso, probe, and laptop with a split screen demonstrating simultaneous ultrasound and augmented reality displays. External motion tracker is not shown. See text for details. Photo by CAE Healthcare with permission.
Simulation curriculum
Simulation sessions were performed on separate days following the didactic instruction and students each had 1 hour of individual 1:1 training with the instructor during 14 separate periods. In these sessions, the trainees were taught how to obtain 4 focused TEE views (TG MP SAX, ME 4C, ME 2C, and ME LAX views; see Figure 2), and performed these exercises repeatedly until mastery with a normal simulated patient; thereafter repeating this process in simulated patients with specific pathologies. A teaching manner was used consistent with best practices for simulation instruction employing rapid-cycle deliberate practice that specifically has been effective in teaching TEE.23,24 After practicing obtaining these views, they learned a simplified algorithm (Figure 5) that relied on initial acquisition of a TG MP SAX view to diagnose causes of hemodynamic instability in common scenarios amenable to the use of focused TEE.
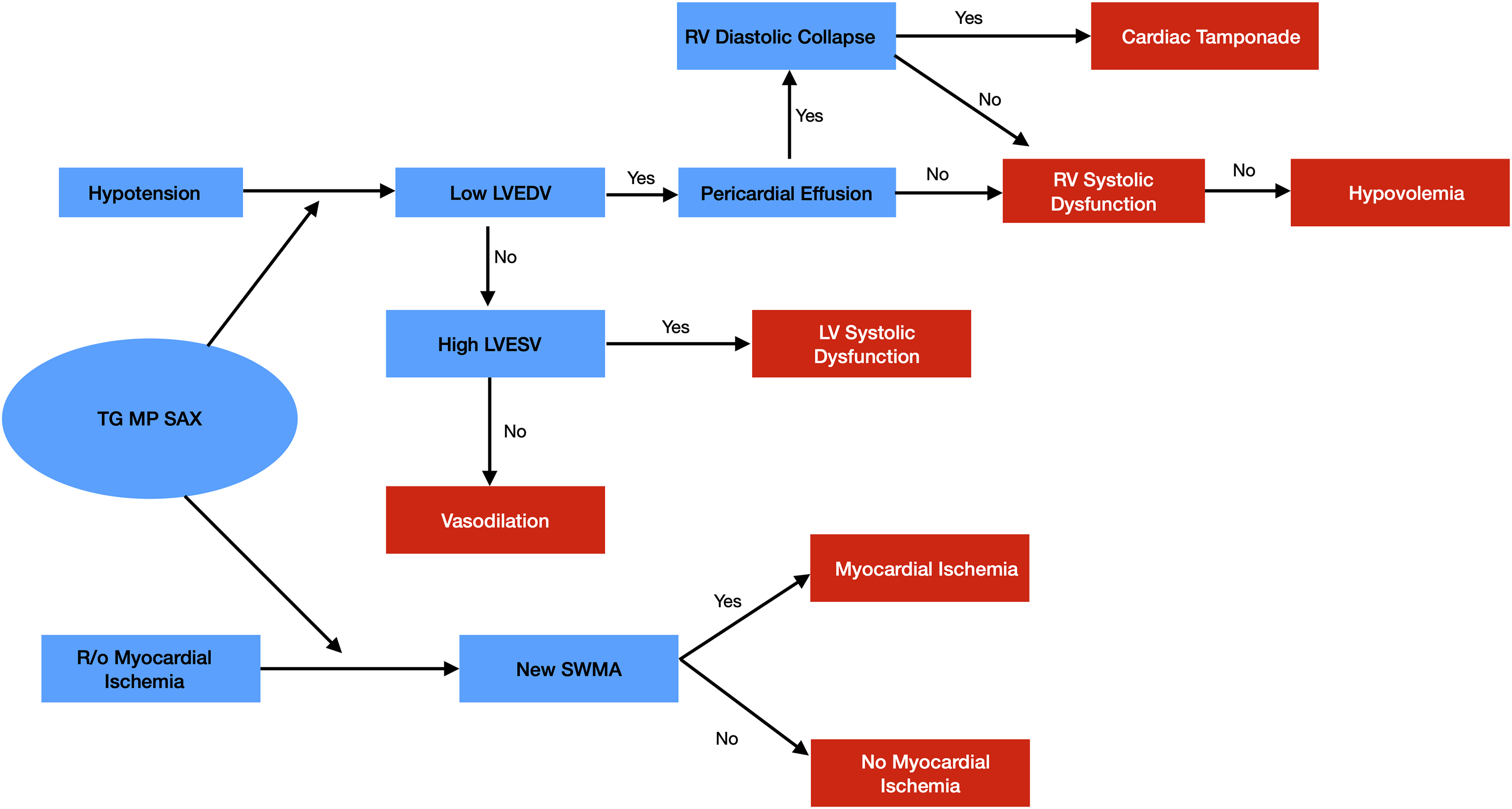
Focused transesophageal echocardiography algorithm. Abbreviations: LV, left ventricle; LVEDV, left ventricular end diastolic volume; LVESV, left ventricular end systolic volume; RV, right ventricle; SWMA, segmental wall motion abnormality; TEE, transesophageal echocardiography; TG MP SAX, transgastric midpapillary short axis view.
This algorithm was predicated on the qualitative assessment of critical physiologic parameters. For example, visual estimates of changes in ventricular wall thickness (regional wall motion abnormalities) were judged to indicate normal wall motion, mild hypokinesis, severe hypokinesis, akinesis, or dyskinesis. While this non-quantitative method introduced some “greyness” into the diagnostic process, it represented a realistic approach to perioperative TEE assessment and was relatively easy to replicate with simulation where clarity and consistency can be readily achieved. Student findings on an initial view were then confirmed by acquisition of an additional view or views from the above focused list (ME 4C, ME 2C or ME LAX views). For example, if they diagnosed anteroseptal myocardial ischemia initially by seeing an appropriate segmental wall motion abnormality on a TG MP SAX view, they then corroborated this finding by obtaining a ME LAX view that visualized the same (anteroseptal) portion of the left ventricle. Likewise, if they saw evidence of early diastolic collapse of the right ventricle (RV) free wall in the presence of a significant pericardial effusion on TG MP SAX view consistent with cardiac tamponade, they then visualized the RV on the ME 4C view to verify consistent findings.
Data collection
After approximately 45 min of simulation-based instruction, each student was evaluated using 5 clinical scenarios associated with appropriate TEE simulator presentations. These scenarios involved (1) refractory hypotension with aortic cross-clamp release following abdominal aortic aneurysm resection (hypovolemia); (2) refractory vasodilatory hypotension as the sole, initial manifestation of anaphylaxis (low afterload); (3) severe oliguria despite fluid resuscitation during a small bowel resection (acute RV infarction); (4) refractory hypotension with a damped arterial waveform after a motor vehicle accident (cardiac tamponade); and (5) questionable ST-segment elevation during a carotid endarterectomy (acute inferior wall myocardial ischemia) (Table 2). Scoring of the clinical scenario evaluations was divided into scoring of image acquisition and scoring of image interpretation. Although acquisition and interpretation are a priori related to each other, the evaluations of the 2 skills were separated in the following manner:
For each scenario (with activity titles in a “hidden” mode not visible to the trainee), students were asked to first acquire a TG MP SAX view as the initial step of the desired focused TEE algorithm. They then were instructed to interpret the scenario pathology (ie, make a diagnosis) and obtain an appropriate second image (either ME 4C, ME 2 C, or ME LAX) that corroborated that diagnosis. “Acquisition credit” (1 point per scenario) was given if students first acquired a clear TG MP SAX image, made the correct diagnosis, and then obtained an appropriate clear second image to view the same pathology, OR if they first obtained a clear TG MP SAX image, made an incorrect diagnosis, and then obtained a second image that was appropriate to view the same (misidentified) pathology. In this manner, “acquisition credit” was possible despite loss of “interpretation credit.” For example, if students correctly or incorrectly interpreted their initial TG MP SAX image as showing inferior wall hypokinesis, they would receive 1 point for “acquisition credit” if they also acquired a clear view of the inferior wall in a ME 2C view (not ME 4C or ME LAX views that did not show the inferior wall well). “Interpretation credit” (1 point per scenario) was given if students correctly interpreted the initial TG MP SAX image. Such credit was dependent upon acquisition of this initial view, and as such, hypothetically these skills were not separable if students failed to acquire that view.
In this manner, a total of 2 points was possible for each of the 5 scenarios, with a total possible score of ten points for the exercise. As such, the specific benchmarks in this part of the study were the ability to acquire and interpret views correctly in the context of hypothetical adverse event clinical scenarios. TEE setup and probe insertion could not be realistically evaluated with this simulation. Students were allowed a maximum time of 3 minutes per scenario for both the acquisition and interpretation of images.
Following the completion of the didactic and simulation curricula, students were emailed surveys (QualtricsXM) that focused on issues related to the TEE workshop's acceptability and its utility for promoting professional growth. The questionnaires specifically addressed whether the trainees perceived that the workshop learning objectives were achieved ie, they provided information concerning students’ perceptions rather than objective evaluations of this issue. These surveys also queried whether students were likely to seek additional TEE training, apply for TEE privileges, and/or employ TEE in their future clinical care as a result of this TEE workshop. Survey data consisted of responses to Likert scale questions as well as descriptive free-style answers.
Data analysis
For simulation evaluations, performance scores were reported for the entire cohort and then separated into the percentage of correct view acquisition and correct view interpretation for each scenario. Likewise, errors were grouped as either acquisition errors or interpretation errors. Ranges of scores were compared descriptively.
For the post-TEE survey, mean Likert scale scores were computed for each statement. Qualitative responses to open-ended inquiries were merged and analyzed to generate themes. These themes related to the perceived educational value of the didactic and simulation components of the workshop, to the likelihood of future TEE training and clinical utilization, and to potential improvements in workshop design.
Results
Feasibility
All students completed the study, indicating that a workshop with the parameters (1 instructor, 10-20 trainees, and 2 days) and curriculum of the present endeavor is feasible with nurse anesthesia providers with no previous TEE exposure. The workshop design was associated with a significant instructor time burden (21 h with 14 trainees). More than half of this time was devoted to 1:1 simulation instruction.
Acceptability and efficacy
All post-TEE surveys were completed and returned (14/14). The responses to questions 1 to 10 in this survey demonstrated that the workshop was acceptable to all attendees and that they perceived significant benefits from their experiences (Table 3). This was true for both the didactic and simulation portions: “The TEE didactic exercise was extremely useful as it will allow us as future clinicians to utilize TEE in assessing patients for a number of … abnormalities;” “Having the hands-on experience helped solidify what we learned in the didactic session.” The Likert-scale responses to these same survey questions (in particular, question 10) also made it clear that the workshop served to ease some of the intimidating aura surrounding TEE: “Putting our hands on the TEE simulator was one of the most engaging, educational, yet low-stress simulations we've had.”
Mean Likert scale student scores for the post-TEE survey (Scale 1-5).

Abbreviations: SD, standard deviation; TEE, transesophageal echocardiography.
The efficacy of this workshop also was assessed objectively (and quantitatively) by students’ performances on the simulation evaluations (Table 2). These exercises judged whether students could correctly acquire and interpret TEE data applicable to 5 hypothetical adverse event clinical scenarios in real time (3 minutes per scenario). Students correctly performed both tasks in mock clinical situations in real time during 64/70 (91%) endeavors. They acquired images correctly 69/70 (99%) of the time and interpreted images correctly 65/70 (93%) of the time. The lowest score (10/14 [71%]) occurred with scenario 3 and related to incorrect interpretation of TEE images showing acute RV dysfunction with RV hypokinesis and dilation.
The lowest student cumulative score was 8 points (out of 10 possible points); 4 students scored 9 points, and the remainder (9 students) had a score of 10 points. Six responses were judged inadequate and received no credit. Five of the 6 inadequate responses (83%) related to incorrect image interpretations; one related to an incorrectly performed image acquisition. The latter event occurred because a student did not recall that the left ventricle (LV) inferior wall is better visualized in an ME 2C rather than in an ME LAX view. All students successfully acquired an initial clear TG MP SAX view, and in the 5 instances of misinterpretation of this initial view, students acquired an appropriate second image of the same anatomical area of “misdiagnosis.” In the case of these 5 students, appropriate image interpretation was carefully explained in a post-test period to prevent anchoring of these incorrect diagnoses.
Likelihood of future TEE training and clinical utilization
All students agreed or strongly agreed that they were “likely to seek opportunities to improve” their TEE skills and “request further instruction in TEE” in the future. Furthermore, nearly all students strongly agreed that they were “likely to seek TEE privileges and employ TEE” in their clinical practice. These findings clearly suggest that students appreciated the value of TEE as a perioperative monitor for patients with unstable hemodynamics.
Areas for improvement
Students recommended that the simulator be incorporated into the didactic portion of the workshop as an adjunct method to demonstrate acquisition and interpretation of images. Most students were not averse to the entire TEE didactic experience occurring in one day and therefore being “content dense.” The mean Likert scale response to “The TEE didactic experience would be better if it occurred over more than one day” was 3.6 (0.7).
Discussion
Despite the lack of randomized controlled studies comparing the benefit (both for intraoperative clinical outcomes and for 30-day postoperative recovery) to the risk of TEE in noncardiac surgery, 6 there is a large volume of observational evidence to suggest a vital role of TEE in this setting.11–14,25 For these reasons, and possibly because of diminishing use of pulmonary artery catheters, anesthesia providers have increasingly employed perioperative TEE as a real-time monitor to guide resuscitation and optimize perioperative hemodynamic interventions in noncardiac surgery patients.5,11 A relatively recent AANA survey, however, showed that only 20% to 25% of CRNAs incorporate TEE in their clinical practice, 15 although the survey did not provide data to define the context (possibly largely for cardiac surgery cases) nor the training, certification, or privileging associated therewith (presumably they would not have met the NBE eligibility criteria). 26
A probable reason for these findings is the lack of readily available TEE units, especially in centers that do not provide cardiac or major vascular surgery. Another important reason for this low prevalence likely relates to the lack of adequate TEE training in nurse anesthesia education. These conclusions represent assumptions regarding causation and should be assessed by additional surveys to better understand barriers to the use of TEE by CRNAs.
Several studies relate to whether workshops can adequately provide entry-level TEE training. Although a 1-day combined didactic and hands-on instruction in focused transthoracic echocardiography for anesthesia and critical care physicians (not CRNAs) has been shown to correlate with improvement on a multiple-choice test, 27 this testing modality fails to assess higher order critical thinking and correlates poorly with competency. 28 There is similarly unconvincing data in the nurse anesthesia population that workshop training positively impacts clinical performance with TEE. Shields and Gentry studied 2 cohorts of nurse anesthesia students and showed that the group that trained in basic TEE with a high-fidelity simulator in-person performed better than a comparable group that underwent web-based training. 15 Unfortunately, there are a number of important limitations in their investigation: (1) the study cohort consisted of first-year students with incomplete didactic foundations; (2) both student groups in the study performed poorly (the higher scoring group averaged 69% in their post-course evaluation); (3) the training occurred over 4 weeks; (4) the study did not utilize a focused TEE curriculum involving a handful of select views; and (5) outcome parameters relied on multiple-choice testing of knowledge of cardiac anatomy, identification of TEE windows, and interpretation of TEE images of cardiac valvular pathologies 15 rather than on more practical issues arising during noncardiac surgery. As such, although a workshop for CRNAs that can provide novice expertise in TEE image acquisition and interpretation is needed, it is important initially to establish the feasibility, acceptability, efficacy, and utility of any such planned endeavor.
For this purpose, we chose to study a workshop designed to teach focused TEE because of its relative simplicity and significant value in monitoring hemodynamics and guiding patient resuscitation during noncardiac surgery.4,11 This design followed the initial steps of the Kern model which has been shown to facilitate the development and implementation of successful educational systems in medicine.
29
These steps included problem identification and a general needs assessment, a targeted needs assessment related to the development of a focused perioperative TEE skill set, choice of goals and objectives, enumeration of educational strategies, and production of a curriculum, core content, and timeline as part of implementation. Our workshop involved nurse anesthesia students (rather than CRNAs) because of their relative homogeneity with respect to their novice status and accessibility. Hypothetically, desired aspects of such a workshop for trainees (or practitioners) included:
Concentrating on the practical aspects of perioperative TEE. For example, since focused TEE is often a qualitative process, the details of quantitative TEE data collection largely were avoided. Furthermore, most issues related to significant hemodynamic instability (eg, hypovolemia, impaired contractility, vasodilation, tamponade, etc) do not require a detailed understanding of cardiac anatomy. The didactic component of the workshop therefore assumed a basic knowledge of this subject and only involved such information when it was relevant to the goal of image acquisition and interpretation of intraoperative cardiovascular perturbations. Teaching a limited number of TEE views as part of a focused protocol. Most perioperative adverse events benefiting from TEE in noncardiac surgery can be addressed with 4 TEE views requiring only 2 imaging positions (TG MP SAX, ME 4C, ME 2C, and ME LAX views)—a fact that simplifies learning of focused TEE. Teaching a larger subset of the 28 comprehensive views
7
can be confusing and intimidating. This is consistent with a focused rescue TEE protocol recently advocated by Staudt and Shelton for noncardiac surgery patients.
4
The latter protocol involved 5 views (rather than 4 views), including ME Bicaval and Ascending Aorta views rather than an ME 2C view. Using an uncomplicated algorithm to guide diagnosis of major hemodynamic problems. Since a normal examination (or possibly a hyperdynamic presentation consistent with vasodilation) or hypovolemia were the findings in approximately 60% of rescue TEE studies performed for noncardiac surgery patients,
4
and working recall of the protocol details is important for real-time responses to intraoperative crises often under stressful circumstances that may impair memory retrieval,
30
this algorithm should be as streamlined as possible. More involved echocardiographic protocols for preoperative assessment of high-risk patients represent expert approaches, but they likely are too complex for routine use by novices.31,32 Also, it should be emphasized that unlike nonoperative TEE, perioperative TEE is not usually performed just at 1 point in time (a hemodynamic “snapshot”), but rather consists of viewing sequential images after interventions are performed. As such, repeated application of this algorithm to the same patient at successive times is important and should be encouraged.
The present study utilized the aforementioned elements in its design. A basic familiarity with cardiac anatomy, physiology, and pathophysiology was assumed, and didactic sessions focused largely on the “how to” of TEE performance, providing a practical guide to TEE image acquisition and analysis. Although 12 TEE views were discussed in the didactic curriculum, only 4 views were emphasized and described in detail to address adverse perioperative events. The algorithm employed with these views (Figure 5) started with a single view (TG MP SAX) and used one or more of the remaining 3 views for confirmation of the diagnosis. This protocol for initial focused perioperative TEE is comparable to a simplified version of other recommended approaches,
33
employing views that usually are relatively easy to acquire.
Given the limited number of views mastered for focused TEE in this process, workshop-trained professionals should understand the importance of requesting assistance when additional views and/or expertise may be useful. This is a key consideration and the potential need to seek assistance from more experienced NBE-certified echocardiographers is foundational to this workshop process. As set forth in the current guidelines spelled out in a consensus statement of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists, professionals certified in basic perioperative TEE “encompassing the 11 most relevant views” need to seek “appropriate consultation with an advanced echocardiographer” “if complex pathology is anticipated or suspected (eg, valvular abnormality or aortic dissection).” 2 Likewise, practitioners introduced to focused TEE via a workshop that provides novice level competency in this skill set based on didactic and simulation teaching should have staged privileges with its use during patient care.
Patient experience remains a valuable part of the complete perioperative TEE certification process to ensure safety and serve as a quality control for instruction of this clinical procedure. 2 For example, patient-based introductions of the probe are essential to developing a routine for doing so, estimating normal versus abnormal tissue resistance, and avoiding potentially serious complications related to malposition (eg, nonmidline insertion into a pyriform sinus). Also, qualitative judgments related to heart chamber volumes or wall motion require experience to diagnose properly especially when not presented in extremes; and patient care issues arising during TEE performance complicate an operating room TEE experience in a manner that is not easily replicated in this study's instruction. Despite these considerations, however, high-fidelity simulator-based training can serve an important role in teaching basic perioperative TEE and can be used to discriminate between expert and novice echocardiographers. 34
One potential modification in curriculum design that should be considered for future endeavors involves delivery of the didactic content asynchronously online prior to simulation. Such modification would significantly decrease workshop time and instructor teaching burden and may be an equally effective method of delivering educational content. These workshops, with or without such modification, introduce anesthesia providers in a nonthreatening way to the practical aspects of this technology, and thereby serve as valuable stepping stones for their ultimate acquisition of full operating room privileges. Otherwise, it is likely that current significant underutilization of this technology will continue, particularly by nurse anesthesia personnel who are unlikely to have the opportunity to acquire basic or advanced NBE certification. Informed, staged competency to permit privileging with varying degrees of supervision may be a superior alternative that encourages safe utilization of perioperative TEE for prevention and rescue of abnormal hemodynamics.
This situation is similar to suggested credentialing and privileging of other medical professionals that utilize TEE for specific and limited goals. For example, the American College of Emergency Physicians (ACEP) has advocated a streamlined and focused protocol involving 3 TEE views to certify emergency physicians to employ TEE to manage cardiac arrests and periarrest hemodynamics.35,36 For analogous reasons, these ACEP recommendations occurred because use of TEE (that has been shown to alter cardiac arrest management in a large percentage of cases 37 ) was rarely performed in emergency departments due to lack of appropriate training and certification, 36 and the ACEP desired to steer “a delicate balance between establishing benchmarks to ensure safe TEE evaluation and yet not developing insurmountable roadblocks to learning potentially lifesaving diagnostic techniques.” 36 Furthermore, given its relatively low complication rate, 9 focused TEE represents a novice competency that is safely attainable by CRNAs providing anesthesia for noncardiac surgery.
Possibly related to this workshop's design considerations, participants in this small-scale study performed very well. Like the cohort in Shields and Gentry's study, 15 these nurse anesthesia students had no previous exposure to TEE, and in this regard, they were reasonable surrogates for many CRNAs in practice. Unlike that previous study cohort, however, the mean score (for all scenarios) for all students tested in the present investigation on a simulation-based exam of image acquisition and interpretation associated with hypothetical adverse event clinical scenarios was well-above passing: 95%. There were only 6/70 (9%) occurrences when students either failed to acquire an appropriate image or misinterpreted an image (mostly the latter) ie, 91% of the time, students acquired and interpreted images correctly within 3 minutes.
While a 9% failure rate seems low, if 9% of interventions based on focused TEE were incorrect, this value clearly would be unacceptable. For this reason, prior to patient interventions based on TEE analysis alone, trainees need to seek confirmation from more extensively prepared echocardiographers. As such, it is important to recognize that these figures do not represent mastery, but they suggest a level of expertise that can provide an entry to patient care. As stated previously, and reiterated here, the concept that such trainees “need to seek assistance from more experienced NBE certified echocardiographers is foundational to this workshop process.” In this context, it should be noted that our specific evaluation process has not been verified. However, simulation-based exams test the third level of Miller's pyramid model of competence (shows how) (Figure 1), and in so doing, they provide an improved assessment compared with standard multiple-choice exams.20,28
Uniformly, nurse anesthesia trainees in this study believed that both the didactic and simulation components of the workshop were valuable educational experiences (ie, acceptable) that prepared them to use TEE in order to diagnose common significant perioperative adverse events (hypovolemia, vasodilation, and myocardial ischemia). Their perception that they learned to acquire and interpret specific, focused TEE views accurately is consistent with their simulation-based evaluation scores. As such, there was both perceived and measured efficacy of the workshop. Importantly, all the students (14/14) also believed that the workshop had “de-mystified” TEE and all students strongly agreed (12/14) or somewhat agreed (2/14) that they will seek TEE privileges in their future clinical practice.
Limitations
The cohort sample was a small convenience sample limited to its size; a power analysis was not performed as it would not be feasible to alter the sample size in this study. Future investigations should be repeated on a larger scale. Furthermore, although the immediate results of the workshop suggest that it was effective, the study did not assess retention of content (crucial for long-term competency), and future investigations should be designed to address this element most easily by repeating the same or an equivalent simulation-based assessment after a significant time interval (weeks to months). In the absence of such “maintenance” data, this study cannot make conclusions regarding future performance of the attendees, either simulator-based or clinically assessed. We also did not include an assessment of patients undergoing surgery with practicing, workshop-trained CRNAs, which represents the ultimate goal of this type of workshop (the top level of Miller's pyramid of competence).
Other aspects of the study design also impose limitations on its precise conclusions. Pre- and post-didactic testing (for either didactic session) was not performed, so an objective assessment of the effectiveness of this process cannot be judged. Similarly, while familiarity with cardiac anatomy, physiology, and pathophysiology was presumed prior to initiation of the workshop based on previous education and training, this assumption was not corroborated by pre-testing. Finally, a validated survey has not been developed for the purposes of assessing student's perceptions of a TEE workshop, and therefore the survey used in this study (Table 3) was not validated prior to its use. It also was not pilot tested.
Conclusion
The present study suggests that a well-accepted and effective 2-day workshop to teach acquisition and interpretation of appropriate images during focused TEE in noncardiac surgery for nurse anesthesia providers is achievable predicated on survey results and short-term competency-based evaluative findings. The critical design elements for this workshop include concentrating on practical aspects related to noncardiac surgery rather than on more esoteric aspects of TEE performance (commonly related to cardiac surgery), teaching a limited number of TEE views as part of a focused protocol, and using an uncomplicated algorithm to guide diagnosis of major hemodynamic problems. Although the workshop was feasible, one of the weaknesses of the current construct is that there is a significant teaching burden on the sole instructor (21 h for 14 students). This burden could be reduced significantly with the introduction of additional instructors, especially for 1:1 simulation sessions. In addition to making use of multiple instructors, future studies should examine the feasibility and efficacy of similar endeavors for larger cohorts, including practicing CRNAs, and testing maintenance of novice competence by assessments performed weeks to months after workshop completion.
Footnotes
Author contributions
BS, LOS, and JS contributed to the conception and design, drafting, data analysis, critical revision, and final approval of the article. A preliminary version of this manuscript has been published elsewhere as a preprint.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study (#00024517) was not considered human research by the Oregon Health & Science Institutional Review Board (IRB), and hence IRB approval was not required (IRB Memo 6/3/2022).
Informed Consent
All participants gave written consent for their data to be used for publication.
Data availability
The data supporting the conclusions of this study are available on request from the corresponding author.