
Abstract
OBJECTIVES
Transesophageal echocardiography (TEE) is being increasingly utilized during orthotopic liver transplantation to guide perioperative management. Obstacles of improving TEE utilization include the challenge of becoming familiar with the TEE machine, optimizing TEE images, and translating skills acquired in didactic or simulator center-based training into clinical use.
METHODS
In an effort to expand TEE utilization and improve workflow among the liver transplantation (LT) anesthesiologists at our institution, a LT-specific TEE guide was created to serve as a reference and educational tool during LT. A 26-question survey was distributed to all LT anesthesiologists before and 6 months after implementation of the LT-specific TEE guide.
RESULTS
All seven LT anesthesiologists completed the survey questions during the study period. No statistically significant difference was detected in participant-reported confidence in optimizing targeted TEE views, performing technical aspects of the exam, navigating the knobs on the TEE machine, or in ability to identify abnormal cardiac pathology during the study period. One participant became basic-TEE certified during the study period.
CONCLUSIONS
Implementing a liver transplant-specific TEE guide is a strategy to expand TEE utilization, encourage longitudinal TEE education and reinforce concepts learned from hands-on education sessions; however, we did not detect a difference in participant-reported confidence of performing a TEE exam, ability to identify abnormal cardiac pathology or altering workflow. Further studies with larger sample sizes will be needed to evaluate the effectiveness of a LT-specific TEE guide.
Background
Transesophageal echocardiography (TEE) during orthotopic liver transplantation (OLT) is increasingly utilized to guide perioperative management.1,2 The Society of Cardiac Anesthesiologists (SCA) and the American Society of Anesthesiologists recommend the use of TEE in non-cardiac surgery when the nature of the planned procedure or the patient's pathology is expected to result in severe hemodynamic instability. 3 Additionally, the Society for the Advancement of Transplant Anesthesia (SATA) has emphasized the safety and benefit of TEE during OLT in their 2020 position paper. 4
While SATA and SCA recommend that anesthesiologists using TEE obtain formal certification by the National Board of Echocardiography (NBE), TEE is commonly used regardless of certification status due to the challenges of formal certification. Board certification by the NBE involves passing an examination to obtain testamur status and further application to become a diplomate. Diplomates must provide documentation of 300 TEE exams with 150 exams personally performed by the applicant to become board-certified in Advanced perioperative transesophageal echocardiography (PTE). For certification in Basic PTE, applicants must have documentation of 150 TEE exams, of which a minimum of 50 must be personally performed by the applicant. Despite the challenges of obtaining formal certification, efforts to enhance TEE utilization by liver transplantation (LT) anesthesiologists and critical care anesthesiologists have been successfully implemented through didactic presentations and hands-on TEE simulator training. 5
While information learned during a TEE simulator session can improve echocardiographer knowledge and skill, a number of challenges may hinder the more widespread adoption of these educational sessions and subsequent application intraoperatively by LT anesthesiologists.
Obstacles to improving TEE utilization among LT anesthesiologists include the challenge of becoming familiar with the TEE machine, understanding ultrasound knobology and learning to optimize the target TEE image. Translating skills acquired on a TEE simulator to a live patient TEE exam may be hindered by the challenges of maintaining esophageal-probe contact and navigation in the setting of a nasogastric tube in place. In a qualitative study evaluating the most common challenges encountered by students learning echocardiography, the concept of bridging the theory-practice gap was described as a major challenge with students finding it difficult to integrate knowledge from class in practicing with the ultrasound machine. 6
In an effort to expand TEE utilization among the LT anesthesiologists at our institution, a liver transplant-specific TEE guide was created to serve as a reference and educational tool to be used by LT anesthesiologists during OLT. This project was determined to fall within the category of a quality improvement project and thus deemed to not require IRB review or require written informed consent. It was believed that by repeated exposure-learning and reinforcement by having a LT-specific TEE guide, there would be a continued expansion of TEE use by the LT anesthesiologist. It was believed that this guide would serve as a tool to ensure the appropriate baseline images are obtained as well as to be a guide in optimizing the target images when difficulty is encountered. In an effort to encourage continued growth and expanded use of TEE by the LT anesthesiologist, the TEE guide included a tiered approach to gradually incorporate additional TEE exam techniques into their exam beyond the recommended basic views.
Methods
This is an exploratory survey study conducted as part of a quality improvement project within the department of anesthesiology and perioperative medicine at Mayo Clinic Arizona. The liver transplant-specific TEE guide was developed in an effort to expand TEE utilization among LT anesthesiologists at our institution, improve TEE-related workflow, increase acquisition of clips during OLT, and assist those seeking formal TEE basic certification. The LT-specific TEE guide was created by a fellowship-trained cardiac anesthesiologist and member of the institution's LT team with certification in Advanced PTE (ADS). Survey participants were included if an active member of the LT anesthesiology team with board certification in anesthesiology during the study period and excluded if they were not an active member of the LT anesthesiology team during the entire study period. A survey consisting of 26 multiple-choice questions was distributed to all active LT anesthesiologists at our institution to gauge comfort level with various aspects of a TEE exam and overall utilization of TEE during OLT (survey questions shown in Tables 1 and 2). The LT-specific TEE guide was distributed electronically to all active LT anesthesiologists and a laminated copy of the guide was placed with the TEE machine of the operating room where OLT procedures take place. All LT anesthesiologists were encouraged to complete a basic-TEE exam during OLT procedures unless contraindicated and received personalized instruction by a member of the LT with advanced TEE certification (ADS or PPF) while performing a TEE exam. The LT-specific TEE guide consisted of three sections (shown in Tables 3, 4, and 5) which were “recommended basic LT-specific TEE exam,” “Tier 2, advanced liver transplant TEE exam,” and “knobology reference guide.” The guide contained a series of TEE images for the recommended basic views, each one labeled with anatomical structures and a description next to it providing recommendations on how to optimize the view. The knobology section of the guide described how to navigate the buttons of the TEE machine (Philips Epiq CVx®) with images highlighting the location of buttons and how to use them to optimize the desired TEE exam component. The survey was re-distributed after a 6-month period to assess for increased TEE utilization among the group.
TEE confidence survey questions.

TEE, transesophageal echocardiography.
TEE workflow survey questions.

TEE, transesophageal echocardiography.
Components of TEE knobology reference guide.

TEE, transesophageal echocardiography.
Components of basic LT-specific TEE exam guide.

TEE, transesophageal echocardiography; LT, liver transplantation.
Components of tier 2 advanced liver transplant TEE exam guide.
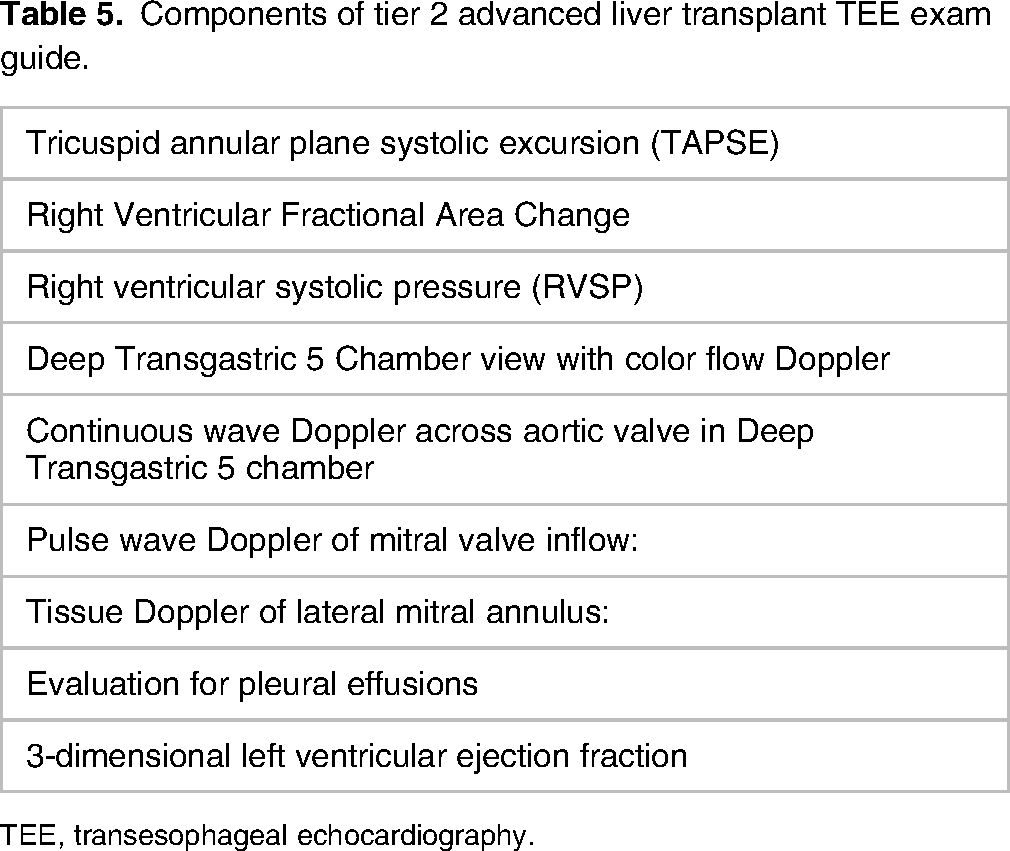
TEE, transesophageal echocardiography.
Statistical analysis
Descriptive statistics were used to summarize survey responses, median and range. Differences between pre- and post-survey responses were compared using Chi-square test for categorical data and Wilcoxon Rank Sum test for continuous data. All statistical tests were two-sided. P-values < 0.05 were considered statistically significant. Statistical analyses were performed in R version 4.2.2.
Results
Overall, seven LT anesthesiologists completed the survey questions both before implementation of the LT-specific TEE guide and after a 6-month period. A 123 liver transplants were completed during the study period (July 2022–January 2023) and as per institutional practice, all patients had TEE performed during the procedure unless an absolute contraindication existed. One LT anesthesiologist became basic-TEE certified during the study period.
Results of the survey before implementation of a liver transplant-specific TEE guide and 6-month post-implementation are shown in Tables 6 and 7. The median response for confidence in optimizing targeted TEE view, performing technical aspects of the exam and navigating the knobs on the TEE machine increased during the study period; however, none of these questions reached statistical significance. Median survey response score also increased during the study period on confidence in identifying abnormal cardiac pathology, specifically for assessing RV function, diagnosing systolic anterior motion of the mitral valve, identifying valvular pathology, identifying a patent foramen ovale, and evaluating flow from the liver allograft into the inferior vena cava; however, none of these questions reached statistical significance.
Survey results of TEE confidence questions before and 6 months after implementation of LT-specific TEE guide.

TEE, transesophageal echocardiography; LT, liver transplantation.
Survey results of workflow-related questions before and 6 months after implementation of LT-specific TEE guide.

TEE, transesophageal echocardiography; LT, liver transplantation.
In terms of workflow-related survey questions, median response scores for time spent on obtaining a baseline TEE exam decreased and post-procedure TEE exam did not change, while the number of reported clips acquired during a liver transplant increased; however, none of these questions reached statistical significance. The median score for how often participants follow a designated pre- and post-transplant exam sequence changed from rarely to frequently; however, this was not statistically significant. There was a statistically significant increase in the median response for how often a TEE reference guide is immediately available while performing a TEE exam during a liver transplant.
Discussion
This exploratory survey study was conducted as part of a quality improvement project to implement a liver transplant-specific TEE guide and improve workflow and TEE confidence among liver transplant anesthesiologists at our high-volume institution. A survey was conducted before the LT-specific TEE guide was distributed and again after 6 months. We felt this time frame allowed for sufficient exposure to the liver transplant guide given the number of anesthesiologists on the LT team and the volume of liver transplants at our center.
Despite an increase in median response score for various aspects of performing a TEE exam including confidence in adjusting technique, optimizing a targeted TEE view, navigating the buttons and knobs of the TEE machine and assessing various cardiac pathology, no statistically significant difference was found between the pre- and post-scores. The reason for this is unclear, although it is possible that the small number of individuals taking the survey (seven anesthesiologists) led to the study being underpowered to detect these differences. It is also possible that the LT-specific TEE guide may take longer than 6 months to lead to a significant difference in TEE workflow and utilization among participants. It is also possible that a LT-specific TEE guide is not an effective tool in improving TEE utilization and workflow.
While TEE guides are not meant to replace formal TEE education or dedicated simulation, an immediately available liver-specific TEE guide may theoretically enhance TEE utilization, help reinforce knowledge obtained in simulation-center training or other hands-on teaching, and encourage longitudinal TEE learning. Additionally, a TEE guide may be an efficient and useful tool to provide tips on troubleshooting TEE image optimization, improve TEE knowledge, and confidence of TEE knobology.
Furthermore, by helping to enhance TEE workflow and allow for increased number of TEE image acquisition, there may be benefit in documentation of baseline cardiac function and more precise evaluation of changes in cardiac function during a dynamic case. Increased number of stored TEE images may be helpful when reviewing challenging cases and when complications arise. Having a TEE guide immediately available while in the OR may help facilitate anesthesiologists to develop a structured TEE exam sequence. By following a structured TEE exam sequence, there is likely to be a more thorough TEE exam with reduced chance of missing a relevant TEE finding.
An important aspect of making a TEE guide is to provide the right amount of detail to be helpful without being overwhelming. We felt that by limiting the exam to a number of views and study techniques most relevant to LT, it will allow the anesthesiologist to have a structured TEE exam that is likely to be helpful in perioperative care and to diagnose the most serious complications that can arise. We felt that by having a tiered approach to a liver transplant TEE guide, the interested echocardiographer can first focus on the basic-TEE exam views relevant to LT and then incorporate more advanced TEE techniques such evaluating for an intracardiac shunts or assessing tricuspid annular plane systolic excursion to quantify RV function.
Evidence suggests that TEE use along with pulmonary artery catheter monitoring may lead to improved outcomes after LT. 7 Additionally, a number of pathologies with different treatment strategies can be diagnosed with TEE. 8 While there is no substitute for rigorous clinical and didactic training to achieve TEE certification, there are many anesthesiologists without testamur status or board certification using TEE during LT 8 who are likely making important diagnoses and guiding perioperative care in challenging clinical scenarios and may benefit from various supplemental educational material. While TEE has the potential to enhance patient care during LT, it is also important to note that performing a TEE exam caries risk to the patient, including risk of esophageal mucosal injuries, which may be more common than previously recognized. 9 We wish to emphasize that there must be a certain level of skill and competence by the echocardiographer for there to be a benefit in clinical care and to ensure proper technique is followed so that potential complications are minimized.
We acknowledge the limitations of our manuscript which include the lack of a control group and potential bias of survey participants. We focused on participant perception of personal TEE skills and confidence level and thus did not administer a specific knowledge assessment at the end of the study period. Additionally, this survey was not previously validated as this was is an exploratory study and was not pilot-tested due to the small number of survey participants available in our study group. Because of the limited number of individuals on the liver transplant team and exploratory nature of the project, a sample size calculation or power analysis was not performed. We acknowledge that our study may be underpowered which may limit the ability to detect a difference in pre- and post-survey responses or make conclusions regarding effectiveness of the LT-specific TEE guide.
Futures studies may expand upon the approach of this study by including multiple centers to increase the number of study participants or increase the duration from pre- and post-survey to ensure sufficient exposure to a LT-specific TEE guide.
Conclusion
Implementing a liver transplant-specific TEE guide is a strategy to expand TEE utilization, encourage continued TEE education and reinforce concepts learned from hands-on education such as simulation-center training among liver transplant anesthesiologists. No difference was detected over a 6-month period in survey participant-reported confidence of operating the TEE machine, assessing relevant cardiac pathology, or altering workflow. Further studies with larger sample sizes will be needed to evaluate the effectiveness of a LT-specific TEE guide.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.