
Abstract
OBJECTIVES
Early introduction to research prepares medical students for the practice of evidence-based medicine. Few studies have examined the experiences of research among medical students in the Arab region. This study assesses medical students’ experiences in pursuing research at the national College of Medicine (CMED) in the state of Qatar.
METHODS
This cross-sectional study was conducted using an online questionnaire distributed through Google Forms. The inclusion criteria called for students over 18 years old enrolled in the college in Years 2 to 6 (pre-clinical and clinical phases) during the spring semester of 2022. The questionnaire included 5 sections with multiple-choice questions and 5-point Likert-scale questions. The questionnaire was validated using esperts review and by piloting it on 10% of the eligible students. STATA 17.0 was used to perform the statistical analysis, which involved a logistic regression and Mann–Whitney U test.
RESULTS
The study had 179 student participants (over half of the eligible group). Half were in the preclinical phase, and half were in the clinical phase. Approximately half had published at least 1 paper. For voluntary research, the main motivators were passion and positive past experiences, while the main demoralizer was inadequate time. For mandatory medical-student research, supervisor help was the main facilitator, and an academic load leaving insufficient time for research was the main barrier. The factors positively influencing voluntary research participation were being older, being male, studying in a more advanced program phase, and having a lower score for negative attitudes toward research. The main limitation of the study was the inclusion of only 1 medical school with 1 type of curriculum.
CONCLUSIONS
Our findings suggest that better research experience can be ensured by providing space, time, and proper academic and moral support to students. The authors believe that doing so will indirectly positively affect the future translation of skills in evidence-based medicine into clinical practice.
Introduction
The recent surge in medical research has made evidence-based medicine a significant component of clinical practice to ensure correct diagnoses, appropriate treatment, and disease management as well as improvement in healthcare services. 1 Consequently, it is crucial for medical students to become familiar with both the conduct and the critical appraisal of research during their undergraduate studies. The usefulness of undergraduate research (UR) as a rich learning experience is well supported by past studies. 2 Accordingly, it is essential to examine the opportunities for UR offered at medical colleges, the attitudes of medical students regarding these research opportunities, and the difficulties they encounter.
Different undergraduate medical programs use different approaches for student research. While some offer it as optional, others consider it mandatory for graduation. Although the scholership on medical students’ experiences in pursuing research in the Arab region are scarce, studies indicate the use of both approaches with prioritizing it as optional. For instance, the American University of Beirut has applied this approach through the Medical Research Voluntary Program, which provides medical students with an opportunity to gain a deeper understanding of the medical research process as well as hands-on experience. 3 Few medical colleges have mandatory research programs as part of their formal assessment. 4 Past reports indicate that despite having access to voluntary research (VR) opportunities, students have implied that there is a need for mandatory research programs.5,6
This study was conducted at the College of Medicine (CMED) at Qatar University (QU). CMED's Doctor of Medicine (MD) program is a 6-year program based on a problem-based learning approach with English as the medium of instruction. The MD program comprises 3 phases. Phase 1 is the foundational year; Phase 2 (pre-clerkship/pre-clinical phase) spans Years 2 to 3 and the first semester of Year 4; and Phase 3 (clerkship/clinical phase) encompasses the second semester of Year 4 together with Years 5 to 6. The college aims to meet the health needs of the multicultural and multiethnic population and improve the quality of Qatar's healthcare delivery. Qatar's population includes almost 94 nationalities, incorporating various religious and ethnic identities that are reflected in the student population at CMED.
The College offers its students VR opportunities under the supervision of faculty members, and a mandatory Medical Student Research (MSR) project is part of the assessment at the end of their preclinical phase. The purpose of the current study is to investigate how CMED students perceive various aspects of the 2 types of research, along with the challenges to and facilitators of the mandatory MSR project and the motivating and demoralizing factors associated with VR. An additional goal is to examine the impact of UR in terms of acquired skills and outputs.
Methods
Study design
A cross-sectional study was conducted using an online questionnaire distributed through the Google Forms platform. Eligible students included those aged above 18 and those studying in Years 2 to 6 (pre-clerkship and clerkship phases) during the spring semester of the 2021–2022 academic year at CMED. Year-1 students were excluded because they had insufficient knowledge and involvement in research.
Study tool
The questionnaire included 5 sections:
The first section collected data on the participants’ sociodemographic characteristics. The second section, titled “Research experience details,” included questions to elicit participants’ research details, such as the type of research they worked on, the number of research projects conducted, the number of resulting publications, and more (see Supplemental material 1: The Questionnaire). The third section, titled “MSR experience,” was divided into 2 subsections that assessed the following:
The student's perceptions of 4 different aspects of the mandatory MSR experience, using 3 to 4 5-point Likert-scale questions for each aspect. The 4 aspects evaluated were gain in statistical-analysis skills, gain in literature-writing skills, gain in general research skills, and satisfaction with the MSR experience. The facilitators and challenges attending the MSR project, using multiple-answer questions that allowed the students to choose from a set of options or type their own answers.
The section began by asking if the participant had taken part in an MSR project or in any voluntary project(s). Those who answered no (mostly from Year 2) were directed to the last section, Section 5.
4. The fourth section, titled “Voluntary research experience,” was also divided into 2 subsections, assessing the following:
The student's perceptions of 6 different aspects of the VR experience, using 2 to 4 5-point Likert-scale questions for each aspect. These aspects were knowledge score, research usefulness for the profession, positive attitudes towards research, relevance to life, facilitators of research in college, and difficulties with research. The motivators and demoralizing factors affecting VR, using multiple-answer questions, which allowed the students to choose from a set of options or type their own answers. 5. The fifth section, titled “Limited research experience,” assessed the factors that contributed to a lack of research experience, using 5-point Likert-scale questions. The factors included personal and college-related reasons. These questions were used to compute a mean score (out of 5) of the “Negative attitudes towards research” variable for each student. This variable was later used in our multivariable logistic regression analysis.
The interpretation of each of the scores on the 5-point Likert-scale question was as follows: 1 = strongly disagree; 2 = disagree; 3 = neither agree nor disagree; 4 = agree; 5 = strongly agree.
We categorized the 5-point Likert-scale questions into positive and negative in order to clarify the interpretation of these scores. For statements not favoring medical research (such as “I do not like research”), a negative response corresponded to strongly agreeing or agreeing, which would convert to a high Likert-scale score, while a positive response corresponded to strongly disagreeing or disagreeing, which would convert to a low Likert-scale score. For statements in support of medical research, the opposite was true.
Data collection
The questionnaire distribution and data collection were performed over a 76-day period (from 12 April to 26 June 2022) via link using the Google Forms platform. The questionnaire link was sent to all Year 2 to 6 students through the WhatsApp groups of each cohort. Furthermore, barcodes for scanning were distributed in multiple visible spaces of the CMED building where students attended their main lectures.
Sampling strategy and study size
A convenience sample was used for this cross-sectional study. At the time of the questionnaire distribution, 352 students were enrolled in Years 2 to 6 at the CMED at QU. The total number of responses received was 179 (a 51% response rate). A sample size of 184 participants was calculated using the Kish-Leslie Formula for finite population, assuming a population proportion of 50% and a margin of error of 5% at 95% confidence interval. We sent the questionnaire to all the 352 students and received 179 responses.
Study tool validation and reliability
The assessment of the content and face validities of the questionnaire was performed in 2 steps. First, we asked for feedback from expert faculty who are members of the research leadership in the college and from faculty who had supervised students for more than 2 years. Five expert faculty responded and commented on the tool. The feedback obtained mainly concerned the structure of the questionnaire and the clarity of some of the original questions. The tool was modified accordingly. The second step was ensuring reliability by piloting the study on 10% of the students; a Cronbach's alpha score was calculated for each of the 3 sets of 5-point Likert-scale questions used in Sections 3, 4, and 5 of the questionnaire. The Cronbach's alpha scores for the Likert-scale questions were 0.94, 0.94, and 0.84, respectively, indicating that our tool was acceptably reliable. The data from the pilot study were not included in the final data and were not considered for statistical analysis.
Statistical analysis
Using Microsoft Excel 2022, the data were cleaned, coded, and exported to STATA 17.0 for analysis. Demographic characteristics, research experience details, MSR facilitators, MSR challenges, and voluntary-research motivational and demoralizing factors were summarized in tables or bar charts with frequencies and percentages.
The scores for the 5-point Likert-scale questions on each aspect of the MSR and VR experiences were combined to generate arithmetic means and medians. To test the association between the median scores and the demographic variables (ie, year of study and gender), the normality of the distribution of the scores was checked using the Shapiro–Wilk test, and the Mann–Whitney U test was used accordingly to test the association of MSR and VR experience scores with demographic information. Lastly, multivariable logistic regression was performed to assess the association between negative attitudes towards research score, age, gender, and research participation beyond the mandatory MSR. A p-value < 0.05 was considered statistically significant.
Ethics
Our study obtained ethical approval from QU Institutional Review Board (QU-IRB) under reference number QU-IRB 1701-E/22. Upon approval by the ethics committee, informed consent was digitally collected from the participants. The consent form was displayed on the first page of the questionnaire; those who read it and clicked on “agree” were directed to the questions, and those who clicked “disagree” were thanked with no further action required. The consent form provided participants with information about the study's aims and risks, the rights of participants, and the contact details of the lead principal investigator. Students were informed of the inclusion/exclusion criteria and their right to withdraw at any stage of the questionnaire. Students who did not meet the inclusion criteria were removed.
Results
The study included 179 participants, of whom 32.4% were male and 67.6% female. The highest number of responses was from Year 3 (26.3%), while the lowest was from Year 6 (12.3%). Around 113 (62.8%) of the study participants had taken part in one or more research projects, compared to 67 (37.2%) who had not. The sociodemographic characteristics of the study participants are presented in Table 1.
Demographic characteristics of participants.
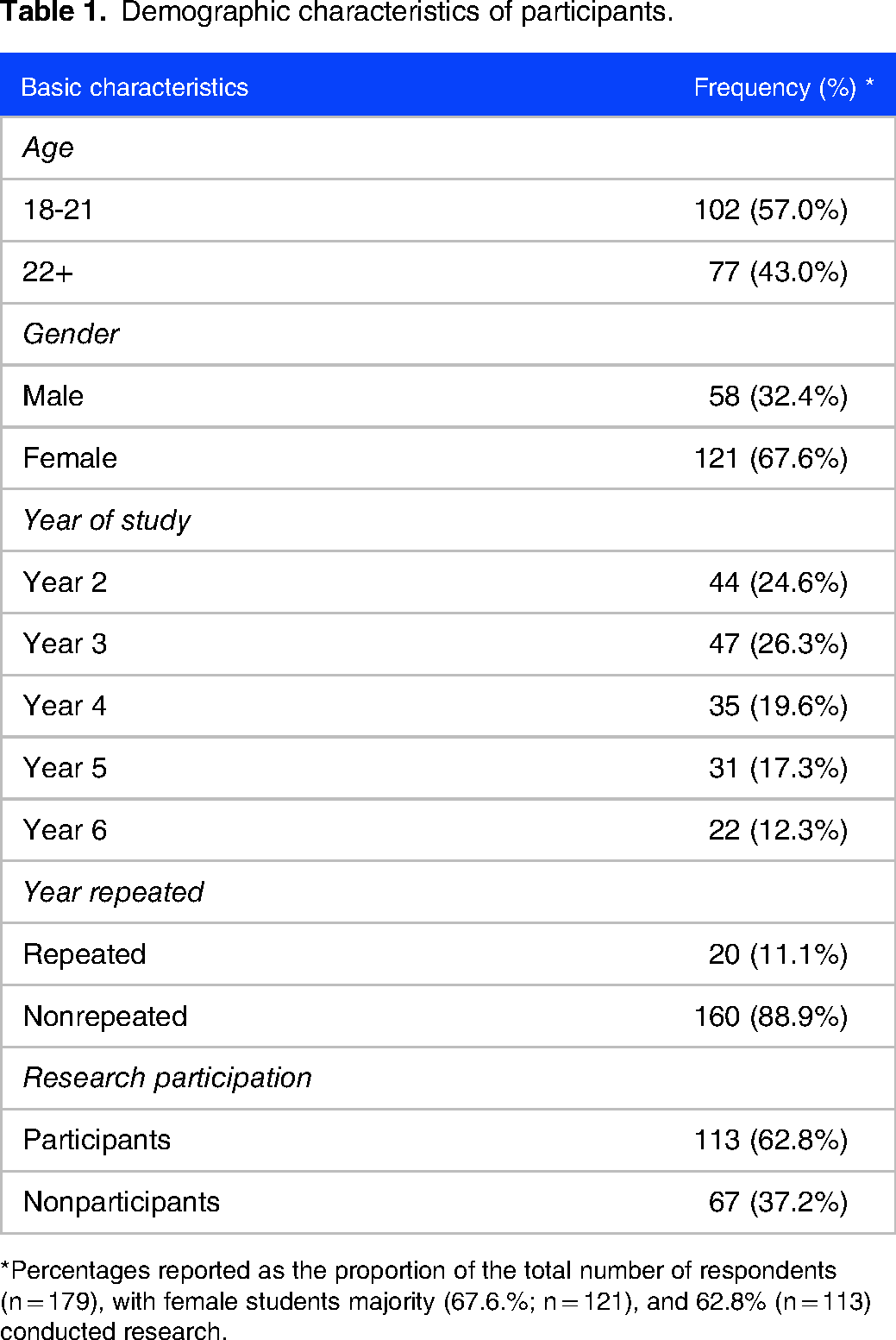
*Percentages reported as the proportion of the total number of respondents (n = 179), with female students majority (67.6.%; n = 121), and 62.8% (n = 113) conducted research.
Research output
The outputs from the research conducted were measured in terms of the number of publications, first-author publications, and publications with an impact factor greater than one. Out of the total number of those who had conducted research (n = 113), approximately half had published research, with most having produced a single publication (37.17%), followed by a smaller number of students with 2 publications (8.85%). Twenty-five (43.9%) of the participants who had published their research were the first authors in one or more of their published research projects.
Forty-three (75.4%) of the participants who had published their research had 1 publication in a journal with an impact factor greater than one, while 7 (12.3%) had published 2 or more research articles in a journal with an impact factor greater than one (Table 2a).
Among those who had completed their MSR projects, 24 students (27.6%) had managed to publish their research, while 63 (72.4%) had not for various reasons; 13 (14.9%) were able to present their projects at local or international conferences (Table 2b).
Research output.
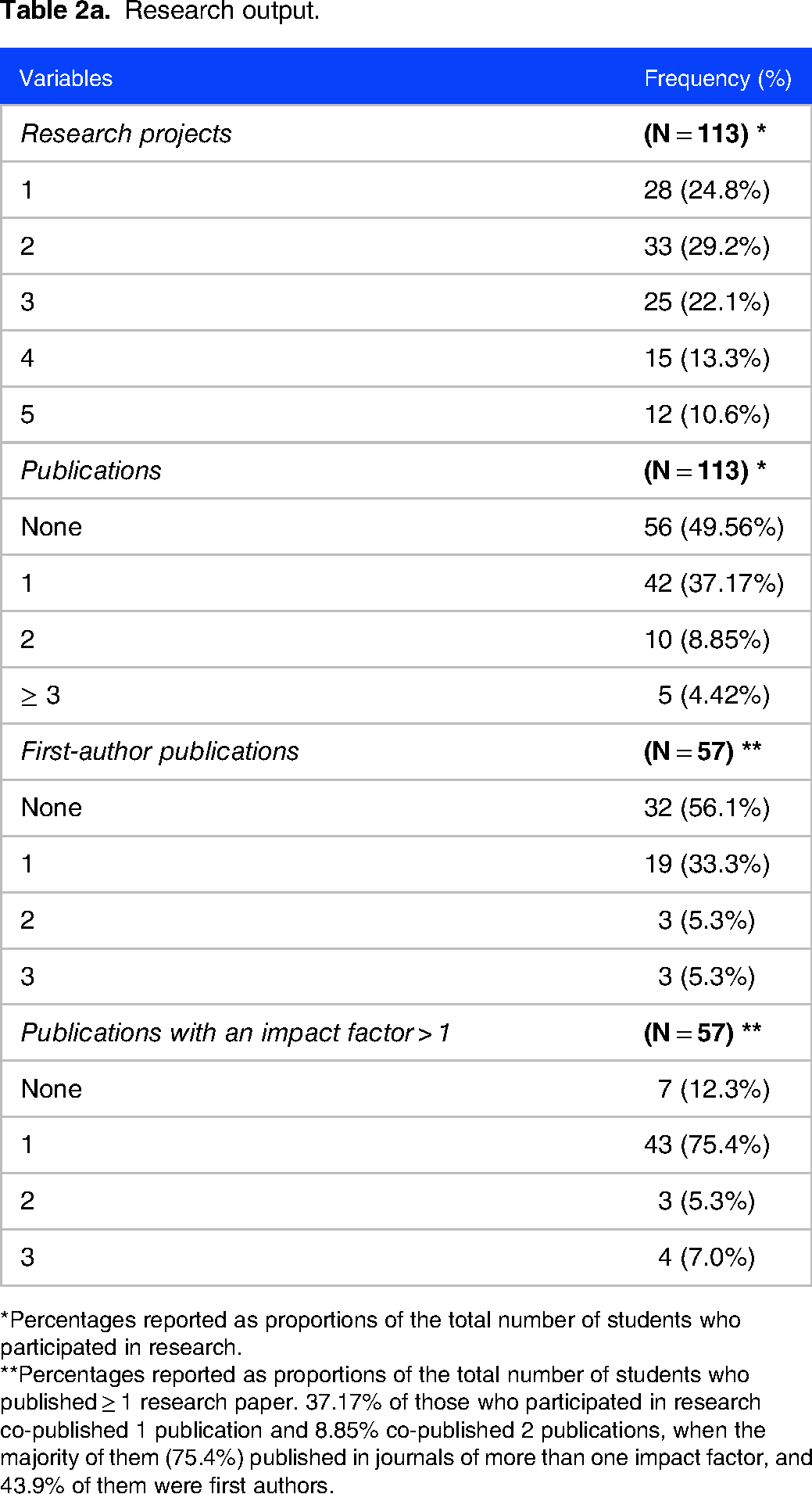
*Percentages reported as proportions of the total number of students who participated in research.
**Percentages reported as proportions of the total number of students who published ≥ 1 research paper. 37.17% of those who participated in research co-published 1 publication and 8.85% co-published 2 publications, when the majority of them (75.4%) published in journals of more than one impact factor, and 43.9% of them were first authors.
Medical student research (MSR) output.

*Percentages reported as proportions of the total number of students who had completed their MSR. The majority of students (72.4%) could not publish their MSR projects, and a minority of them (14.9%) have presented at conferences.
Motivating and demoralizing factors in conducting research
We measured the motivating and demoralizing factors among CMED students with prior research experience and compared the students based on their phases of study (Table 1, Supplemental material 2).
Overall, the most commonly reported motivators were a passion for doing research, at 59.3% and 47.2% in Phases 2 and 3, respectively; positive past research experience, at 14.8% and 41.6%, respectively; and the availability of opportunities in the college, at 44.4% and 31.5%, respectively. Figure 1a displays the motivators and the frequency with which each one was reported.
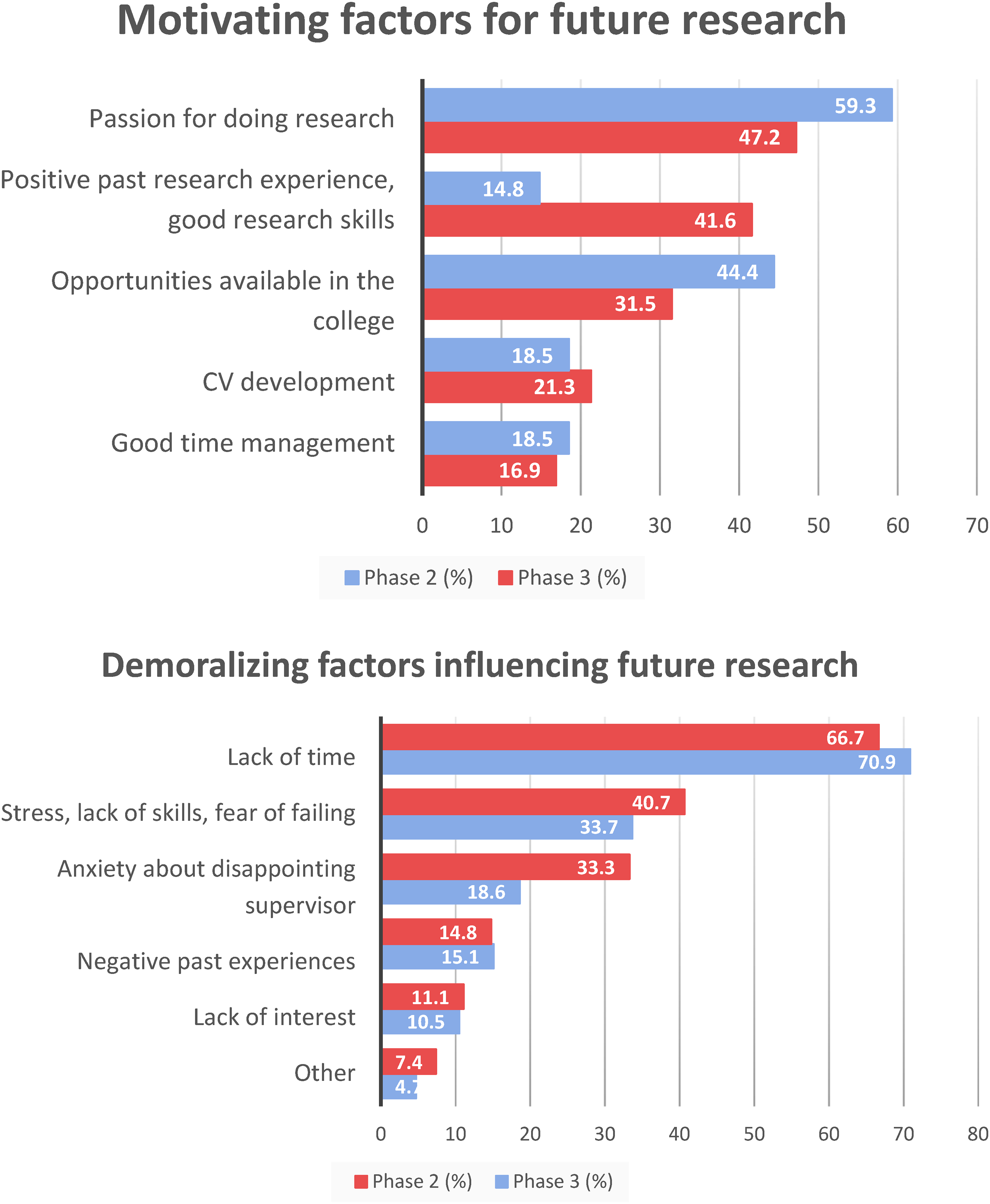
(a) Motivating factors for future voluntary research. The most motivating factor for both preclinical (phase 2) and clinical phases (phase 3), is passion for doing research, followed by availability of opportunities for phase 2 and positive past experiences for phase 3 students. (b) Demoralizing factors influencing future voluntary research. The strongest demoralizing factor for both phases is lack of time, and the weakest is lack of interest in pursuing research. Note: Because these were multianswer questions, the proportions do not add up to 100%.
The most frequently reported demoralizing factors were lack of time, at 66.7% and 77.9% in Phases 2 and 3 respectively; stress and lack of skills, at 40.7% and 33.7%, respectively; and anxiety about disappointing the supervisor, at 33.3% and 18.6%, respectively (Figure 1b). However, anxiety about disappointing supervisors was reported in particular by students in the preclerkship phase (Phase 2).
Barriers to and facilitators of MSR publication
In this section, we measure the barriers to and facilitators of MSR publication that students encountered. These were assessed via multiple-answer questions (Table 2, Supplemental material 2).
Of the barriers to MSR publication named in the questions, the most frequently reported were rejection by several journals (24.6%), students’ lack of confidence in the merit of their research (20.3%), and a lack of supervisor encouragement (17.4%) (Figure 2a). However, it must be noted that the most common response to this question was provided by respondents through the “Other” response option (31%). Further elaboration of these responses is provided in the Discussion section. Meanwhile, the most frequently reported facilitators of MSR publication were supervisor help (74.1%) and continued attempts until the research paper was accepted for publication (55.6%) (Figure 2b).

(a) Barriers to medical student research (MSR) publication. The most frequently reported barriers to publish MSR outcomes were factors related to the process of publication (45%), followed by rejection by several journals (24.6%). (b) Facilitators of MSR publication. Note: Since these were multianswer questions, the proportions do not add up to 100%.
The strongest facilitator to publish their MSR outcomes was supervisors’ encouragement (74.1%) and continued attempts until the research paper was accepted for publication (55.6%)
MSR experience
In this section, we measure the facilitators and challenges that the students experienced while conducting their MSR. These were assessed via multiple-answer questions (Table 3, Supplemental material 2).
Factors associated with research participation at QU's CMED based on multivariable logistic regression.
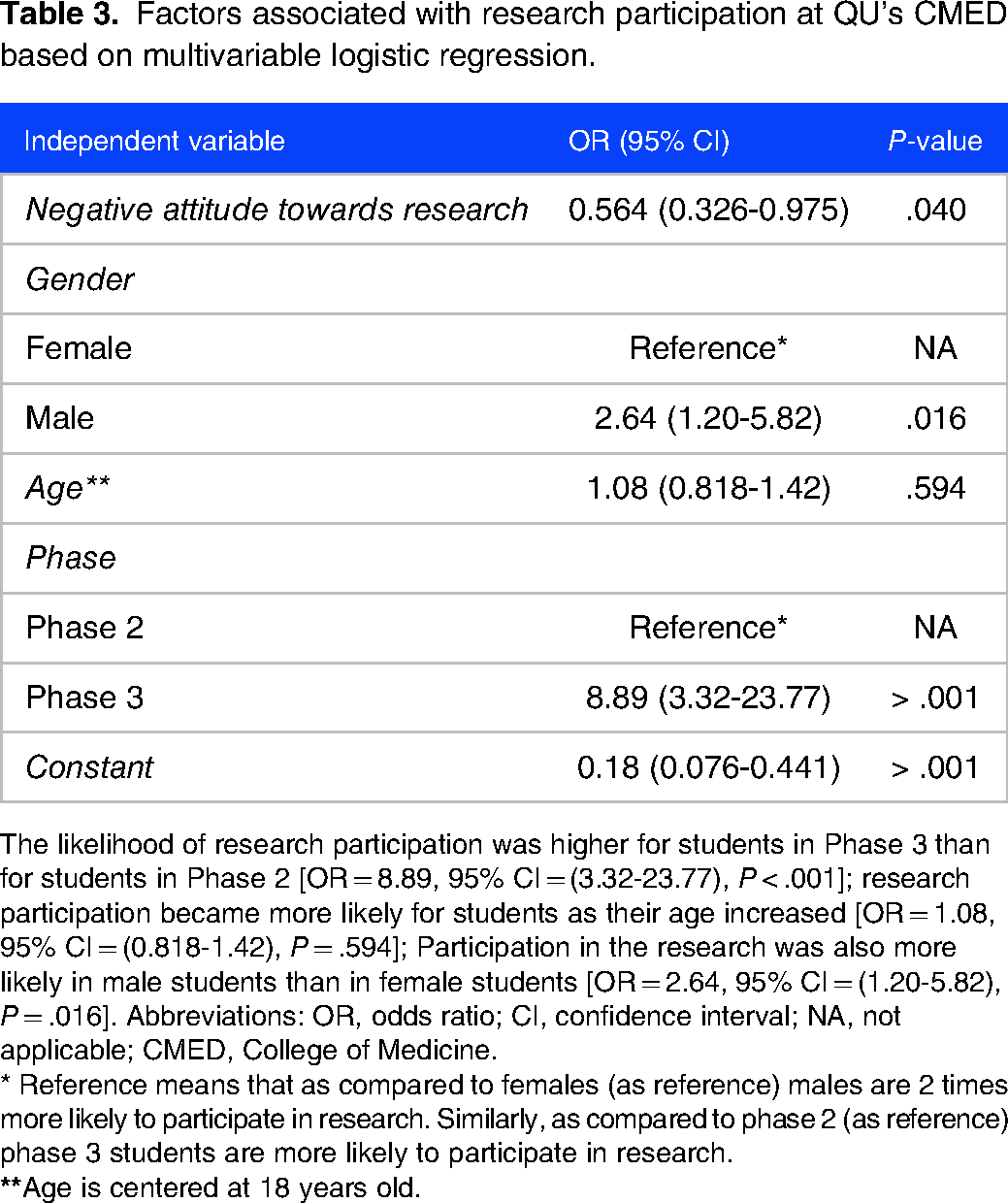
The likelihood of research participation was higher for students in Phase 3 than for students in Phase 2 [OR = 8.89, 95% CI = (3.32-23.77), P < .001]; research participation became more likely for students as their age increased [OR = 1.08, 95% CI = (0.818-1.42), P = .594]; Participation in the research was also more likely in male students than in female students [OR = 2.64, 95% CI = (1.20-5.82), P = .016]. Abbreviations: OR, odds ratio; CI, confidence interval; NA, not applicable; CMED, College of Medicine.
* Reference means that as compared to females (as reference) males are 2 times more likely to participate in research. Similarly, as compared to phase 2 (as reference) phase 3 students are more likely to participate in research.
We found that the most commonly reported challenges were academic load and lack of time (66.7% among those who had published their MSR and 85.2% among those who had not); lack of data availability (3.3% and 59.3%, respectively); and lack of help from the supervisor (29.2% and 38.3%, respectively). Overall, these challenges were more commonly reported by students who had not published their MSR (see Figure 3a).
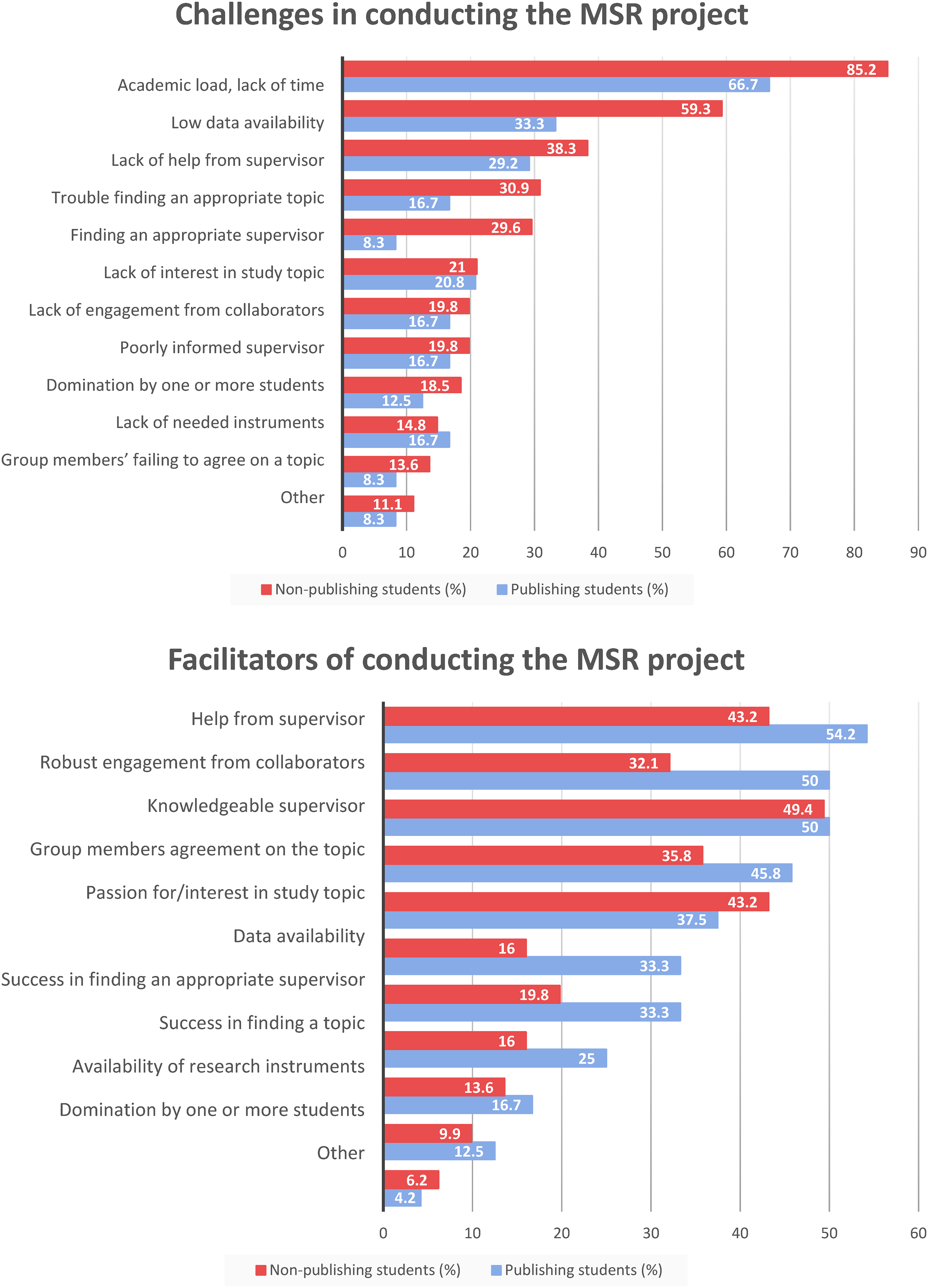
(a) Barriers to conducting the medical student research (MSR) project. Because of the multianswer question format, the proportions do not add up to 100%. The most commonly reported challenges were academic load and lack of time (66.7% among those who had published their MSR and 85.2% among those who had not); lack of data availability (3.3% and 59.3%, respectively); and lack of help from the supervisor (29.2% and 38.3%, respectively. (b) Facilitators in conducting the MSR project. Because of the multianswer question format, the proportions do not add up to 100%. The most frequently reported facilitators were help from the supervisor (54.2% among those who had published their MSR and 43.2% among those who had not); robust engagement from collaborators (50% and 32.1%, respectively); and having a knowledgeable supervisor (50% and 49.4%, respectively).
The most frequently reported facilitators were help from the supervisor (54.2% among those who had published their MSR and 43.2% among those who had not); robust engagement from collaborators (50% and 32.1%, respectively); and having a knowledgeable supervisor (50% and 49.4%, respectively). Overall, these facilitators were more commonly reported by students who had published their MSR (Figure 3b).
The challenges that showed the highest disparities between those who had published their MSR and those who had not were, first, academic load and lack of time, at 66.7% and 85.2%, respectively; second, lack of data availability, at 33.3% and 59.3%, respectively; third, trouble finding an appropriate supervisor, at 8.3% and 29.6%, respectively; and fourth, trouble finding an appropriate topic, at 16.7% and 30.9%, respectively.
The facilitators who showed the highest disparities between those who had published their MSR and those who had not were helped by the supervisor, at 54.2% and 43.2%, respectively; robust engagement from collaborators, at 50% and 32.1%, respectively; data availability, at 33.3% and 16%, respectively; and success in finding an appropriate supervisor, at 33.3% and 19.8%, respectively.
Predictors of research participation
A multivariable logistic regression was conducted to understand the factors associated with research participation among CMED students (Table 3). The results showed that the likelihood of research participation was higher for students in Phase 3 than for students in Phase 2 [OR = 8.89, 95% CI = (3.32-23.77), P < .001]; the association is statistically significant. Furthermore, research participation became more likely for students as their age increased [OR = 1.08, 95% CI = (0.818-1.42), P = .594], although the association was statistically insignificant. There was a decrease of approximately 44% in the odds of research participation with every unit increase in the mean score for negative attitude towards research [OR = 0.564, 95% CI = (0.326-0.975), P = .040]; the association is statistically significant. Participation in the research was also more likely in male students than in female students [OR = 2.64, 95% CI = (1.20-5.82), P = .016]; this association is also statistically significant.
Regarding the logistic regression diagnostics, the regression had strong goodness of fit, as demonstrated by a receiver operating characteristic curve of 82% (Figure 1, Supplemental material 2). In addition, the link test was conducted and showed that our model explained 25% of the variance in research participation, with the students’ phase of the study found to be the most important predictor of research participation among the explanatory variables (Table 4, Supplemental material 2).
Perceptions of VR
In this section, we assessed students’ perceptions of 6 different aspects of VR using 5-point Likert-scale questions (Table 5, Supplemental material 2).
Being a student in Phase 3 was associated with significantly higher median scores for positive attitudes towards research, relevance to life, and facilitators of research in the college. However, the differences between the median scores of Phase-2 and Phase-3 students were minimal for knowledge score, research difficulties, and research usefulness for the profession (Figure 4).

Perceptions of voluntary research experience based on students’ phase of study. Being a student in Phase 3 was associated with significantly higher median scores for positive attitudes towards research, relevance to life, and facilitators of research in the college.
The reasons students reported for lack of motivation to pursue future research are illustrated in Figure 5.

Reasons for lack of motivation to pursue future research. The strongest reason for lacking motivation was found to be prioritizing their academic studies over conducting research, followed by a lack of familiarity with available opportunities, and the least reported reason was they tried to join research projects but were not welcomed.
Perceptions of MSR
In this section, we assessed the students’ perceptions of 6 different aspects of MSR using 5-point Likert-scale questions (Table 6, Supplemental material 2).
Overall, female students had a more favorable perception of MSR than male students. Female students had higher median scores for gain in statistical analytical skills, gain in general research skills, gain in literature-writing skills, and satisfaction with the MSR experience (eg, supervisor and group-member collaboration) compared to their male counterparts (Figure 6). The association between female gender and more favorable MSR perception is statistically significant, as indicated by the p-values computed via a Mann–Whitney U-test.
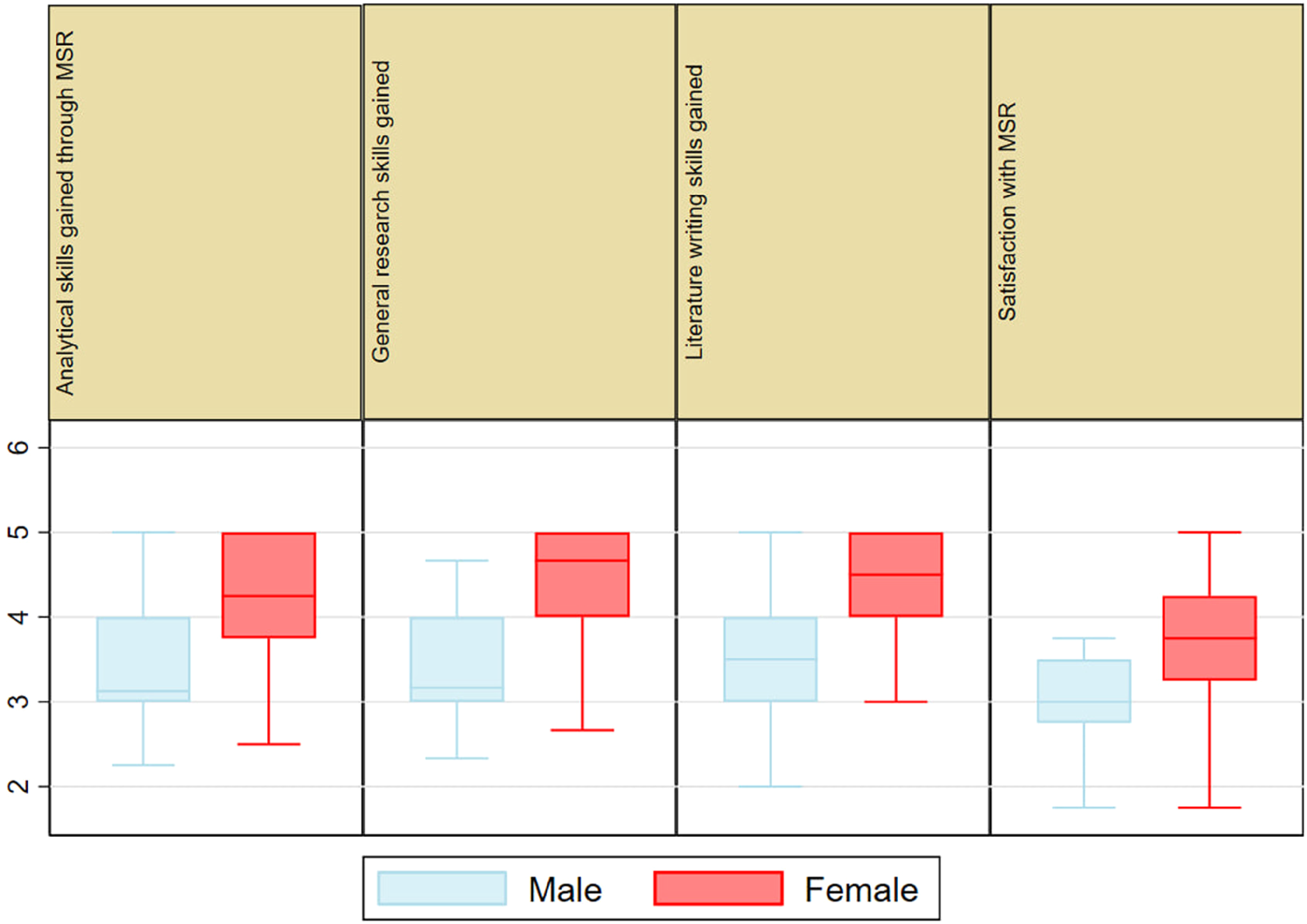
Medical student research (MSR) experience based on students’ gender. female students had a more favorable perception of MSR than did male students. The association between female gender and more favorable MSR perception is statistically significant, as indicated by the p-values computed via a Mann–Whitney U-test.
Discussion
This study has explored the main facilitators of research by medical students, the challenges that they face in conducting research, and the outcomes of their engagement in research. The study found that high publication rates (∼50%) have been achieved by the students. This might be one of the long-term positive implications of promoting research culture in medical schools. Publication rates from the mandatory MSR projects show that only 27.6% of those who completed their projects were able to publish their research. This implies that making research a mandatory requirement is not the only reason to promote research among medical students, but other factors contribute to the publication of students’ work. External and internal factors have been identified in different studies. For instance, a mixed methods study at the University of Western Sydney found that motivation to do research is associated with increasing internalization of intrinsic motivators; in particular those associated with competence (Confidence) and relatedness (Clinical Relevance, Research as a Social Activity). 7 Our study identified a lack of support and encouragement from the supervisor and discouragement from unsuccessful attempts to publish as the most common factors for low publication rates. A recent study in Saudi Arabia similarly reported that support from supervisors was a key factor in achieving the publication of a paper. 8 Studies from other regions identify various factors such as lack of training in writing and seniors’ attitudes9,10−
Motivators and demoralizing factors affecting future VR: Preclinical vs. clinical phases
Our study found that the most common motivating factor for conducting future research was a passion for doing research, followed by a positive experience of research. Similar motivators have been found in other studies.4,7,11 For instance, a recent study carried out in medical schools in Uganda showed that for certain students, passion for research serves as the main driver of research engagement. 12 Furthermore, Kiyimba et al 12 revealed that guidance on manuscript writing and publication can serve as a motivator for many students. Several studies reported that having publications on students’ resumes, which was found to be helpful in being accepted into a good residency program, serves as a major motivation for their research involvement.6,13 For instance, a study conducted in Australia discovered that CV enhancement was the primary motivator for research participation among medical students. 13 Moreover, that study found that students who wanted to enter competitive residency programs were more inclined to participate in research. Similar findings were reported in British medical schools where the main motivation for research and publication was for career progression. 9 In our study, several students reported CV enhancement as a motivator in the “Others” part of the multiple-choice questions.
This study found that the most common demoralizing factors deterring students from future research were lack of time and lack of skills, which ultimately led to stress and feelings of anxiety. Lack of time was also identified as a demoralizing factor by many other studies in different Euro-American and Asian regions.14–16 In our study, although lack of time was equally reported in both phases, lack of skills and stress due to fear of disappointing the supervisor was strikingly higher among Phase-2 students. These findings demonstrate the importance of the CMED's research program in improving students’ research knowledge and involvement rates as they transition from Phase 2 to Phase 3 through electives, weekly research discussions, research grants, research-related courses, and the mandatory MSR project. According to Rosenkranz et al, 17 these opportunities promote students’ autonomy, competence, and perceptions of clinical relevance, encouraging them to do research throughout their undergraduate careers. Other studies in other regions found further demotivating factors, such as financial constraints, lack of experience, lack of mentorship, difficulty in choosing topic, difficulty in collecting data, or lack of interest and motivation.11,16,18,19
Phase-2 students had comparatively lower levels of knowledge and confidence, a difference that may be attributable to Phase-3 students’ completion of their compulsory MSR project. For instance, a study from Saudi Arabia found that one of the factors contributing to high levels of research involvement was having a compulsory research project to participate in. 6 Studies from other regions such as Brazil and Pakistan identified time constraints and a lack of mandatory research projects as obstacles to conducting research, demonstrating the importance of such mandatory research projects in medical schools.13,20
Facilitators and challenges within the MSR experience
This study found that the most common challenges faced when conducting MSR were a lack of time, the academic load associated with the medical curriculum, trouble finding an appropriate supervisor, and a lack of the data needed to complete the study. These challenges have been consistently reported in other studies.7,9,11,15 However, Al Kuwaiti and Subbarayalu's study listed the most commonly reported barriers as lack of institutional motivation, lack of infrastructural activities, and lack of faculty involvement. 21 Others reported inadequate internet connection, language barriers, and insufficient financial support as the main challenges. 22 We believe that addressing these challenges, which constitute barriers to the successful completion and publication of research, would further improve the MSR experience and its output.
The most frequently reported facilitators of MSR in our study were support from the supervisor and robust engagement from outside collaborators. Similar facilitators of research have been noticed in several other studies.5,12 For example, Sayedalamin et al 6 asserted that sufficient mentorship, adequately trained faculty, and financial support from the government are the main facilitators of research. MacDougall and Riley 23 reported on several ways in which supervisors can support medical students’ research. Among these: encouragement, support in planning and writing, creating a sense of accountability, connecting students with research communities, and cultivating self-efficacy. 23 It is worth noting that the challenges, barriers, and facilitators reported earlier not only reflect the MSR experience but also play a role in MSR publication.
Perceptions of research among the students
In this study, student perceptions of 6 different aspects of the VR experience were assessed, using 5-point Likert-scale questions for each aspect. These aspects were making a contribution to students’ knowledge, research usefulness for the profession, positive attitudes towards research, relevance to life, facilitators of research at the college, and difficulties of research. This study found higher scores among Phase-3 students than among Phase-2 students. This can be attributed to higher involvement of phase 3 students in research.
Similar aspects have been assessed in a study conducted in 6 Middle Eastern countries. However, unlike our study, they did not report students in the clinical phase as scoring higher for these aspects on the 5-point Likert scale. 24 In Assar et al, 24 scores for knowledge, research difficulty, and relevance to life issues were remarkably low compared to the scores in our study. However, we assume that these differences are the result of using different questionnaire tools. Globally, studies in other regions report different perceptions. For example, a study from Queens’ University reported that students perceived research as an opportunity for the development of critical appraisal, information literacy, and critical thinking skills; and the opportunity to select an area and form contacts for postgraduate training. 25
Additionally, studies have shown that students become more inclined to take part in research as they advance through the medical school curriculum.4,12 This can be explained by an increase in positive attitudes toward research over time as a result of students’ gaining an understanding of the value of conducting research through completing research tasks and going through research processes. The positive perception of research further contributes to research participation as part of a positive feedback loop. Another explanation can be the better understanding of medical students in the clinical phase of what to expect in doing research. Murdoch-Eaton et al 26 argue that although undergraduates recognize the benefits of research, they still need a realistic understanding of the research process. Undergraduates require training to recognize the skills required for research and enhanced transparency in potential project outcomes.
Investigating the students’ perceptions of MSR showed that female students had significantly more favorable perceptions than male students in terms of literature-writing skills and general research skills. As for the 2 other categories, analytical skills and satisfaction with the MSR experience, gender-based differences in perceptions were not statistically significant, perhaps this is a result of the sample size. Regarding perceptions of the various aspects of VR, female students generally reported a higher gain in skills and greater satisfaction than did male students. Perceptions of research depend on several personal, institutional, and social factors that may have contributed to this gender difference. While female participants have reported a more favorable perception of research in several Middle Eastern countries, 24 male participants have shown a more favorable perception in other countries, such as Pakistan. 27 Furthermore, recent studies in Lebanon as well as in Australia and several other countries showed no gender differences in terms of knowledge, perception, or attitude towards research,3,13,28 indicating that this disparity in perception may not be intrinsically gender-based.
Predictors of participation in research other than MSR
Our logistic regression showed that being male, in a clinical year (Phase 3), and aged at least 22 is strongly associated with more extensive participation in research activities other than the compulsory MSR project.
Similar determinants were reported to be predictors of research participation in a regression model in Uganda, where being aged ≥ 25, being male, and being in a clinical year were found to have positively influenced participation in research activities. 12 Studies from different cultural contexts reported different findings. For example, a study from Australia reported no gender differences in research engagement and/or outcomes. 29 However, they report similar findings in relation to being in a higher year of study as a factor associated with higher research participation.24,27 Studies from the Euro-American contexts, did not report on gender as a factor, 30 indicating the impact of cultural hierarchies on academic dynamics in some contexts such as Middle Eastern ones. Higher levels of research participation have, however, also been linked to several other characteristics, such as regularly reading medical journals, parental education level, university rank, university type, and mode of learning in college.24,31 Meanwhile, this study found that the “negative attitude towards research” score was associated with lower levels of research participation.
Limitations of our study
Our study has several limitations. The study was conducted in only 1 medical school, with 1 type of curriculum; including other medical schools with different curriculum types may lead to different results. We believe that PBL programs require a high level of self-directed learning, making the pursuit of research more challenging for medical students enrolled in this type of curriculum. For future research, we thus recommend including different medical schools with different types of curricula and a broader set of participants, such as graduates and residents/interns, who can inform about the impact of their research experience and its contribution to their clinical practice. Another limitation of our study is the sample size. Although we were able to reach more than half the eligible research population, including more students would give a broader, more accurate indication of student research experiences. Additionally, a variety of circumstances made it challenging to reach students, such as hybrid teaching due to the coronavirus disease 2019 pandemic at the time of data collection, which resulted in lower attendance at many academic activities.
Conclusion
Although this is not the first study of its kind in the Middle Eastern region, it is the first study to focus on understanding the factors that influence attitudes toward research among medical students in Qatar. Our findings suggest that in addition to the sociodemographic factors that influence perceptions of and participation in research, several motivating and demoralizing factors may promote or hinder the conducting of research in medical schools. Being aware of these factors, both demoralizers and motivators, can help medical schools build tailored research programs that meet students’ needs. We also believe that providing a supportive environment and highly trained supervisors for students will improve the quality of, and their confidence in, their work. Positive experiences will attract more future doctors to research, which may result in improved medical practice in the region.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241227327 - Supplemental material for Perceptions and Experiences of Pursuing Research Among Medical Students in Problem-Based Learning Curriculum: A Cross-Sectional Study from Qatar
Supplemental material, sj-docx-1-mde-10.1177_23821205241227327 for Perceptions and Experiences of Pursuing Research Among Medical Students in Problem-Based Learning Curriculum: A Cross-Sectional Study from Qatar by Reem R Al-Subai, Muhammad Z Kaleem, Doaa Hassanien, Meral Eldestawy, Mahmoud N Hamwi, Engy Elsayed, Amal S Al-Kawari, Habib H Farooqi and Suhad Daher-Nashif in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205241227327 - Supplemental material for Perceptions and Experiences of Pursuing Research Among Medical Students in Problem-Based Learning Curriculum: A Cross-Sectional Study from Qatar
Supplemental material, sj-pdf-2-mde-10.1177_23821205241227327 for Perceptions and Experiences of Pursuing Research Among Medical Students in Problem-Based Learning Curriculum: A Cross-Sectional Study from Qatar by Reem R Al-Subai, Muhammad Z Kaleem, Doaa Hassanien, Meral Eldestawy, Mahmoud N Hamwi, Engy Elsayed, Amal S Al-Kawari, Habib H Farooqi and Suhad Daher-Nashif in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors thank Professor Suhail Doi and Dr Giridhara Babu—Population Medicine Department—for their support and valuable consultation on statistical components of this study. We also thank all the students who agreed to respond to this survey, and to help in improving medical students’ experiences in pursuing research.
Author's contribution
Conceptualization was done by all authors. Building and validating the questionnaire were contributed by SDN, HHF, RRS, MZK, and DH. Data collection was done by RRS, MZK, DH, MD, MNH, EE, and ASK. Statistical analysis was carried out by HHF, MZK, RRS, and DH. Supervision was done by SDN. Co-supervision was done by HHF. All authors contributed to writing the first draft. Review and editing were done by SDN. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.