
Abstract
OBJECTIVES
This study aimed to investigate how effective self-assessment training is in improving the self-regulated learning (SRL) ability of operative dentistry students. The secondary aim was to explore students’ attitudes towards self-assessment in clinical settings.
INTRODUCTION
Self-assessment has been the focus of dental education research for decades and has been claimed to be cornerstone in the SRL process.
METHODS
This is quasi-experimental study conducted at Damascus University Faculty of Dental Medicine, Syria. A modified direct observation of procedural skills (DOPS) assessment protocol with a self-assessment component was applied to a convenience sample of students across five clinical encounters in 2022. Data were collected during clinical training on the DOPS form and at the end of the experiment using a structured questionnaire with a single open-ended question. The qualitative part of the study followed a deductive theory-informed content analysis approach, relying on Zimmerman SRL theory.
RESULTS
A total number of 32 students participated in the study, eight of whom were male. During the experiment assessment, participants showed overwhelming positive attitudes towards the utility of self-assessment (m ≥ 3.5; max:4) and the overall assessment method (3.3 ≥ m ≥ 3.5; max:4). Cronbach's alpha for the post-experiment questionnaire was 0.888. A total of 84.4% of the participants strongly agreed that self-assessment is useful in clinical training. Data collected (qualitative and quantitative) from participants revealed the positive effects of self-assessment on all three phases of SRL, especially the reflection phase.
CONCLUSION
Self-assessment practice and training showed positive results in terms of improving SRL and performance in a clinical context; SRL appeared to be affected by self-assessment in all phases (forethought, performance, and reflection). Participants’ perceptions of self-assessment were generally very positive. These findings imply the potential benefits of applying self-assessment training interventions to foster the SRL ability of learners within the clinical context.
Keywords
Introduction
Self-assessment has been a focus of research for decades, transcending beyond one field and spreading into various fields such as social psychology, medical education, and dental education.1–3 In dental education, self-assessment importance was emphasized in 2013 when the Commission on Dental Education (CODA) in the United States stated in its standards for dental school accreditation that “graduates must demonstrate the ability to self-assess…” 4
Self-assessment is contemporarily defined as “a wide variety of mechanisms and techniques through which students describe (ie, assess) and possibly assign merit or worth to (ie, evaluate) the qualities of their own learning processes and products.” 5 This definition highlights the variety of ways self-assessment can be implemented, which can be as simple as self-assigning a grade (self-grading) or more complex, such as the deep analysis of weaknesses and strengths and making constructive feedback in relation to explicit standards.5,6
Self-assessment is thought to increase educational gains by affecting self-regulated learning (SRL). In Zimmerman's model, SRL is divided into three phases: the forethought phase, the performance phase, and reflection phase 7 ; each phase has processes and subprocesses. Self-assessment has been claimed to affect SRL in all phases. 8 For instance, self-monitoring (performance phase) and self-evaluation (reflection phase) have clear similarities to the concept of self-assessment. Moreover, self-assessment could affect SRL by increasing the clarity of learning goals (forethought phase). 9 However, all these studies were conducted in a classroom setting and not in a clinical setting.
In clinical settings, the objective of learning is secondary to the provision of healthcare, making it very different from that in classroom settings. 10 A person who is capable of self-regulating learning in an academic setting might face challenges when trying the same thing in the complex clinical context. 11 Research has shown that SRL in the clinical environment is shaped by various positive and negative factors than can be put under one of the following three categories: individual, contextual, and social; 11 several studies reported motivation and goal setting skills as positive factors;12,13 difficulty with personal reflection, goal generation, and/or plan development were some of the individual negative factors reported in the literature. 14 Patient care has been frequently depicted as a positive influence on SRL as it is stimulates residents’ SRL as a starting point for learning.15,16 The majority of studies on SRL reported time limitations as a negative contextual factor;14,17 the influence of teachers and peers was found to be a positive social factor. 16 Educators have tried to support learners’ SRL by stimulating positive factors and mitigating the effects of negative factors. Providing the support of mentors 18 and recording learning goals 15 showed desirable effects on SRL. George et al study showed that mentor-guided SRL approach helped improve independence in goal setting. 18 Similarly, use of learning plans in recording goals facilitated focus during learning by improving awareness of the learning process. 15 Other interventions included the use of supportive tools, such as the online environment which showed to affect self-monitoring in a positive manner by facilitating the ability to track progress. 19 Nevertheless, all interventions mentioned in the literature affect only the forethought and performance phases, and none of the studies focused on the reflection phase. 11 The last phase of the SRL is important for completing the SRL cycle. Therefore, there is a need for interventions such as self-assessment to support the reflection phase. 11
The current study aimed to evaluate the effectiveness of self-assessment training in improving SRL in clinical operative dentistry. The hypothesis being tested was that self-assessment of clinical performance can affect students’ SRL. The secondary aim was to assess students’ attitudes towards self-assessment in clinical settings.
Materials and methods
Ethical approval was obtained from the ethical committee of Damascus University Faculty of Dental Medicine on January 15, 2022 (no. 98735). Verbal informed consent was obtained from all participants prior to the study, and this mode of informed consent was approved by the ethical committee.
Study design
This study is part of a longitudinal quasi-experiment with a post-intervention assessment. 20 This is mainly a quantitative study but it has a small qualitative component which followed a deductive approach based on content analysis. This study introduced a modified workplace assessment method, in which self-assessment was sought and recorded via a structured form in five clinical encounters between March 2022 and June 2022. Thereafter, a self-administered structured questionnaire with a single open-ended question was used to evaluate the effectiveness of the introduced intervention in supporting SRL as theoretically conceptualized by Zimmerman. 7 The questionnaire was developed using the popular SRL framework 7 which supports its content validity; the face validity was tested using a panel of experts in the field who approved the final version. As for the qualitative part, this study used a deductive theory-informed content analysis approach; Zimmerman SRL theory 7 was used to design the pre-defined codebook which was later used to analyze the qualitative data.
Participants and settings
This study was conducted in a clinical setting at Damascus University Faculty of Dental Medicine, Damascus, Syria. The target population was dental students in their fifth year of training. In Syria, dental education comprises three preclinical years and two final clinical years, in which students engage in patient treatment in authentic workplace settings. The sample was selected using convenience sampling. Students were invited to participate via an electronic survey, and those who consented were contacted via social media/telephone to confirm their participation. The sample size was calculated for an effect size of 0.64, 21 power of 90% and an alpha value of 0.05. 20 The required sample size was 28. Data saturation was not discussed, as the sample size was predetermined according to the pilot study.
Self-assessment training
Participants underwent a rigorous self-assessment training protocol. Direct observation of procedural skills (DOPS) with a self-assessment component was conducted across the five encounters. The DOPS form contained 22 items related to steps of operative dental procedures (eg clinical knowledge, professionalism, cavity preparation and restoration). 20 The evaluation form in full was provided in the supplementary files in a recently published study. 20 A grading rubric was specially designed to illustrate the assessment criteria for each item in the DOPS form. 20 The grading rubric and the DOPS form were sent to participants in electronic form before the beginning of the term. Moreover, an instructional video and an electronic quiz were sent to participants to familiarize them with the assessment form and criteria. Thereafter, a brief mandatory orientation session was organized for the participants to answer any questions and quickly review the assessment process. All participants attended the orientation session.
Each DOPS encounter was divided into three phases: before, during, and after the procedure. Before the dental procedure, a feedforward session was undertaken to highlight common pitfalls from previous encounters and to revise the treatment plan with the supervisor. During the procedure, the supervisors observed the participants during the operative dental procedure and directly assessed them using the DOPS form. After the procedure, participants completed a self-DOPS form in which they assessed their own performance; the self-DOPS form of trainees was identical to that of supervisors. Once the self-DOPS forms were completed, a feedback session with supervisors took place; in this session, supervisors first evaluated students’ self-assessment against theirs; then, supervisors corrected students’ self-assessment in a collaborative conversational manner. Before the feedback session, participants were required to write down an action plan on the self-DOPS form to address the areas of improvement they identified in item I (Figure 1). The action plan was adjusted by the supervisor. This was done to actively engage participants with adaptive inferences and enable them to set sub-goals that can help them acquire the skill highlighted in item I (Figure 1).

The back page of the self-DOPS form which include, identification of areas of improvement and excellence, action plan design for addressing the areas of improvement, and attitude assessment. DOPS: direct observation of procedural skills.
In summary, at each clinical site, where a dental procedure was carried out by a trainee, a single self-DOPS and a single supervisor DOPS were completed. This means that there were two completed DOPS forms, one completed by the trainee who carried out the procedure and the other was completed by the supervisor. Basically, the two forms are meant for assessing the same thing—the trainee's performance at that given clinical site.
Every clinical procedure performed by any participant during the academic term was evaluated using self-DOPS/DOPS-each participant had to perform five clinical procedures at each clinical site.
The self-DOPS form not only allowed participants to self-grade but also allowed them to analyze areas of improvement and areas of excellence which the authors thought to activate more complex levels of self-assessment (I, II, Figure 1).
Supervisors were trained and calibrated to use the DOPS assessment method. Inter- and intra-rater reliability were calculated, and they were of acceptable values (>0.7). The measurement of reliability for the supervisors is illustrated in detail in Alfakhry's et al 20 study.
Data collection
At the end of the term self-administered online questionnaire was used to evaluate the effect of self-assessment training on SRL processes. Google Forms, an open-access tool, was used to collect the questionnaire data. 22 The questionnaire consists of closed-ended items and a single open-ended question. Responses were recorded using a forced 4-point Likert scale (strongly disagree, disagree, agree, and strongly agree). Responses were not sent back to participants for correction. Several questionnaire items addressed each phase of the SRL model, as depicted by Zimmerman. 7 The last item was open-ended, and asked participants to comment on their experience with self-assessment in the educational experiment. For the participants’ attitude measurements, several items were designed by the researchers. Moreover, at each assessment encounter, participants’ attitudes towards the assessment method and the utility of self-assessment were recorded on a 4-point Likert scale on the self-DOPS (Figure 1a, b). The questionnaire was checked for face validity by a panel of experts and its internal consistency was evaluated using Cronbach's alpha.
Qualitative data, either from the post-course questionnaire or the self-DOPS form (action plan section, Figure 1), were processed using closed coding as informed by Zimmerman SRL theory. 7 Pre-defined categories and subcategories are illustrated in Table 4.
The questionnaire and responses were written in Arabic to overcome language barriers. Participants’ comments were coded and analyzed in Arabic. Thematic analysis was conducted, and certain comments were selected to represent the main themes and are presented in this paper, which were double translated from Arabic to English and vice versa to ensure language accuracy.
Data analysis
Cronbach's alpha was used to measure the internal consistency of the post-experiment questionnaire; negatively phrased items were coded in reverse before the analysis. GA was the single data coder used in this study. Themes were identified in advance in accordance with Zimmerman's SRL theory. 7 MAXQDA 2020 was used to code and conduct the thematic analysis by a single coder-GA.
For the closed-ended questions, data processing and analysis were conducted using Microsoft Excel (2019) and IBM SPSS Statistics for Windows version 26 (IBM Corp., Armonk, N.Y., USA). Google Forms was used to conduct screening and post-experiment questionnaire surveys.
Results
The target population consisted of 182 dental students in their final year of training (fifth year). A total of 87 trainees completed the recruitment survey, but only 39 students were accepted in the study due to resource limitations. Seven participants were excluded from the analysis because they did not complete all five self-DOPS assessment sessions. The final sample included 32 dental trainees; each of whom completed five clinical procedures (five self-DOPS encounters) during the academic term. The characteristics of the sample are illustrated in Table 1.
Demographic and academic information for the 32 participants (self-report).

During experiment
Participants agreed (with item a-, Figure 1) that their experience with the self-DOPS was positive at all five encounters, with a mean score ranging between 3.3 and 3.5 (maximum:4, ie, strongly agree). Similarly, scores on item b- (Figure 1), which addresses self-assessment utility, scored consistently ≥3.5 at every encounter (maximum score:4, ie, strongly agree).
Post-experiment: questionnaire survey findings
At the end of the experiment, a questionnaire survey was used to examine participants’ perceptions of the assessment method, its benefits, and its effect on SRL subprocesses. All the participants completed the questionnaire. Cronbach's alpha for the questionnaire was 0.888.
Perception of self-DOPS
Responses to the items related to participants’ perceptions of self-DOPS are shown in Table 2. A total of 84.4% of the participants strongly agreed that self-assessment is useful in clinical training. The item that had the highest percentage of disagreement were items no. 3 “This assessment method was fair” and 5 “Your self-assessment was accurate” respectively.
Students’ perception of the self-assessment method and its benefits.

As for participants’ responses to the open-ended question (Please leave a comment regarding your experience with the self-assessment method implemented during this semester), all except for one participant expressed positive to a very positive attitude towards the assessment method and have described it as “very good,” “useful”, “unique”, “fun”, “valuable”, and “successful”. The following responses were echoed by many others.
Participant 1: It was one of the richest and most valuable experiences I ever had; I wish it was implemented before.
Despite this general positive attitude, the participants mentioned some challenges they faced with the assessment method. Nonetheless, none of the mentioned challenges were directly related to the assessment method, but rather to other factors related to Damascus University Faculty of Dental Medicine, such as the large number of students, the limited number of dental units, the limited time at the clinic, and considerable number of clinical cases they have to treat. The following comment was echoed by 11 others.
Participant 7: The assessment method as a concept is good but in better working conditions, less number of students, and more dental units at the school… The work pressure, number of cases, and limited time makes applying this assessment method challenging. As for my personal experience, I became more able to evaluate myself and gained lots of practical knowledge…I evaluate my experience as very positive and I benefited a lot from it.
The above comment highlights the poor working conditions at Damascus University Faculty of Dental Medicine, which made implementing the assessment protocol more difficult for participants in terms of the additional time and effort required. Despite this, the trainee expressed how positive the experience was. Another participant noted that it took time to adapt to the new assessment system.
Another response revealed that the achieved accuracy in the assessment process was not appropriate in light of the lack of sufficient resources. “The accuracy of the assessment process is not suitable with the work environment and available resources”
Effect of self-DOPS on SRL subprocesses
According to participants’ responses to the SRL-specific items in the post-experiment questionnaire (
Students’ responses on the items related to the perceived impact of the SA method on self-regulated learning subprocesses.
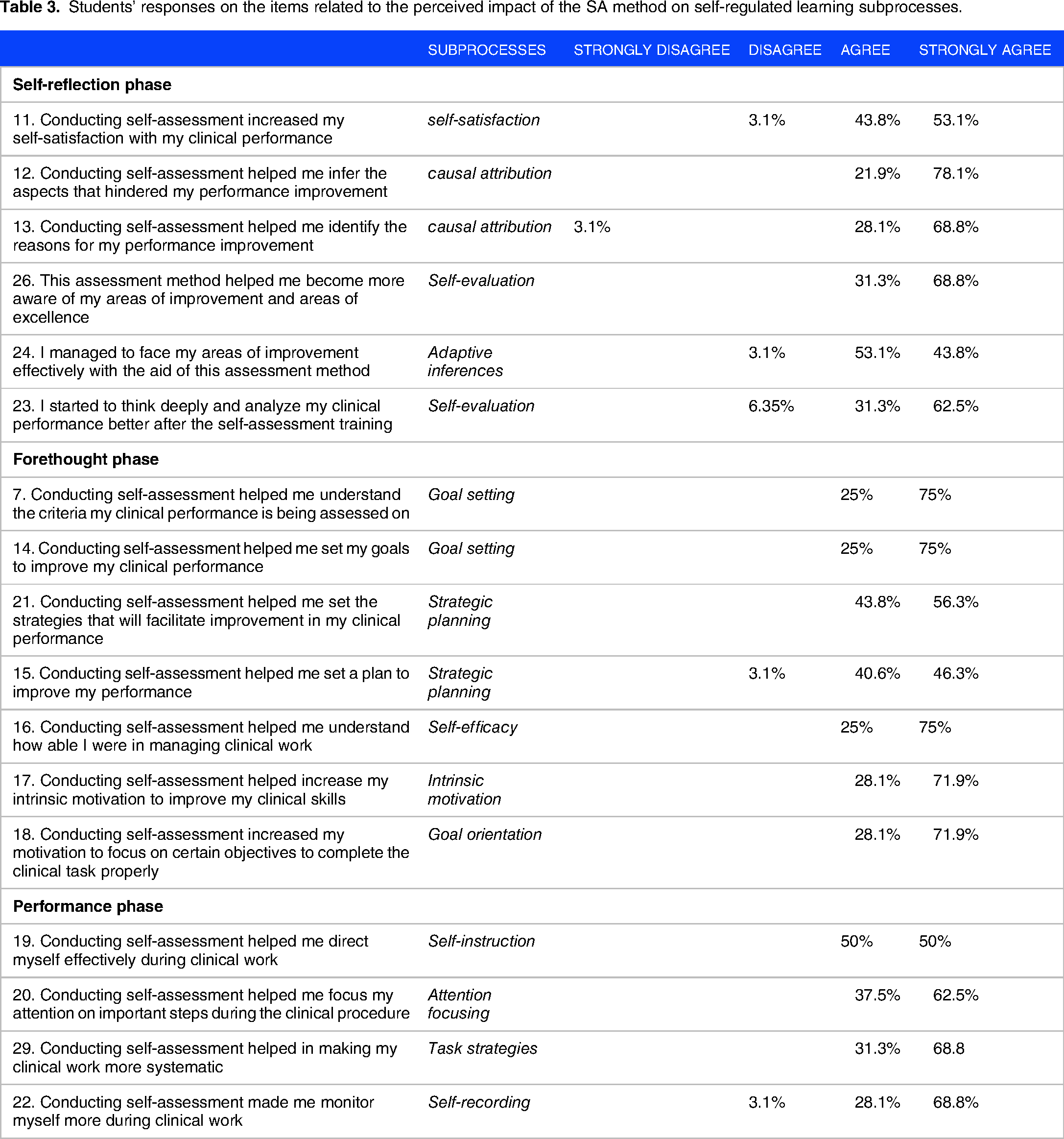
The themes extracted from the open-ended questions also indicated the SRL-related benefits of using self-DOPS. Themes were categorized according to the SRL phase they referred to (reflection phase, forethought phase, and performance phase), and example responses were coded according to the process/subprocess to which they belonged. Sample responses are listed in
Major themes and sub-themes as informed by of Zimmerman self-regulated learning theory with representative quotes.

SRL: self-regulated learning.
Action plan data extracted from self-DOPS forms completed by participants also indicated the activation of two SRL subprocesses: goal setting (forethought phase) and adaptive inferences (reflection phase). Sample responses are listed in
Examples of participants’ written action plans on the self-DOPS form categorized under either goal setting or adaptive inferences (subprocesses of task analysis in the forethought phase).

DOPS: direct observation of procedural skills.
Discussion
This study aimed to evaluate the effectiveness of self-assessment training in improving SRL abilities in operative dentistry. To this end, a self-assessment DOPS protocol was applied to 32 dental students in five encounters. Thereafter, a questionnaire survey was used to examine the perceived effect of self-assessment on SRL subprocesses; a Cronbach's alpha value of 0.888 indicated good internal consistency of the questionnaire. Both qualitative and quantitative self-report measures showed that self-assessment training helped improve or activate the SRL abilities of participants across all phases. Qualitative data indicated that participants were able to set their learning objectives more accurately, and they became more self-efficient and motivated; in the performance phase, attention focusing and self-recording were improved; in the reflection phase, participants reported better ability to evaluate themselves and improved self-satisfaction. Regarding the perception of self-DOPS, overwhelmingly positive attitudes were expressed by participants who perceived it as acceptable, fair, fun, and beneficial. Moreover, many participants reported improvements in their clinical performance and contributed it to the self-DOPS assessment.
Participants who disagreed with the statement “This assessment was fair” attributed the unfairness to the time pressure and the work environment. These aforementioned barriers were also cited by participants who disagreed with the statement “Your self-assessment was accurate” in addition to the time needed to acclimate and familiarize oneself with the self-DOPS.
In clinical education, one of the most cited individual SRL-related difficulties is personal reflection, goal orientation, and plan development and implementation. 15 Other barriers were difficulty in concentration and undertaking too many tasks at the same time. 13 To address these issues, researchers and clinical educators designed a variety of interventions to facilitate SRL development 11 ; these interventions can be categorized into one of the following 11 : (a) coaching or mentoring, (b) use of learning plans, and (c) utilizing supportive tools such as the online environment. The first approach of mentor-guided SRL was reported to improve independence in setting learning goals 18 as well as practice habits and skill development. 23 In comparison, the current study showed that self-assessment improved various areas of SRL including, goal setting, goal orientation, attention focusing, and reflection. As for the use of learning plans in SRL development, studies have shown improvement in setting learning objectives and increased focus during performance (forethought and performance phase).24,25 Similarly, the proposed self-DOPS method also enabled participants to set their learning objectives but not arbitrarily; goal setting was done after, and in accordance with, structured reflection on performance facilitated by the clinical supervisor; areas highlighted as “areas of improvement” became learning objectives, and an action plan was co-devised with the supervisor to address these specific areas; moreover, participants reported better attention focusing ability during the performance phase. All interventions reported in the literature target only the forethought or performance phases. 11 In contrast, the current self-DOPS intervention emphasizes activation of the reflection phase in the SRL cycle.
What adds to the reliability and validity of this study is that the other published part of this experiment compared supervisors’ scores and participants’ self-assessment scores, showing improvement in participants’ self-assessment ability 20 ; the aggregated total absolute difference between supervisors’ scores and self-assessment decreased consistently from 18.0 ± 5.4 to 14.7 ± 5.1 with a significant difference and high observed power (0.763). 20 Participants also became more calibrated to pinpoint areas of improvement and excellence as defined by supervisors 20 ; there was also evidence supporting participants’ improved clinical performance. 20 Moreover, similar findings were reported in the pilot phase of the current study conducted in 2021 in terms of holistic activation of the SRL cycle after conducting self-DOPS assessment. 21
In the current study, the participants demonstrated the ability to implement SRL processes. Several elements of this assessment method may have facilitated this development. First, the effect of conducting self-assessment can be considered a subprocess of SRL. As a cyclical process, it has been argued that SRL processes are mutually dependent, meaning that a change in one process could lead to a change in another. 26 Therefore, self-assessment, which can be considered a subprocess of SRL, could have led to a change in the SRL processes. Second, participants’ interaction with supervisors’ experience and feedback might have affected their recruitment of SRL processes; this argument is supported by the findings of a previous study demonstrating how surgical trainees can optimize their SRL by relying on supervisors’ expertise and feedback. 27
Theoretically, there is a strong relationship between SRL and self-assessment 6 ; however, this is yet to be confirmed by empirical research. In a meta-analysis review of the general education field, self-assessment interventions had a positive impact on students’ SRL strategies. Even though the majority of researchers conform with the idea that self-assessment happens at the last SRL phase (reflection phase), 28 other researchers advocate the idea that self-assessment happens at each SRL phase and process, 28 making it not only an aspect of SRL but a fundamental cognitive process underlying SRL processes. 28 Support for this notion could be deduced from the distinction between two types of reflection “reflection in practice” and “reflection on practice.”29,30 The former is impeded within the performance phase, whereas the latter occurs afterwards. Regardless of what is mentioned above, the relationship between self-assessment and SRL remains understudied in learning sciences. 9 To the best of our knowledge, no previous study in clinical education has examined this relationship.
Implications for practice and future research
The current research sheds light on the benefits and advantages of training students to self-assess, providing support for the notion that self-assessment can boost SRL and performance in the clinical context. Further, the relationship between self-assessment and SRL is understudied in clinical education; therefore, we recommend that researchers design studies to explore this intricate relationship and how it manifests in a multilayered clinical context. Moreover, it could be of interest for clinical educators to explore the benefits of applying the self-DOPS, as proposed in this study, to other clinical fields similar to operative dentistry, such as surgery.
Strengths and limitations
The significance of this study lies in its focus on supporting SRL in the clinical environment by fostering reflection skills (the last phase of the SRL process), in which learners evaluate their progress towards their learning objectives. To the best of our knowledge, and according to a systematic review, no studies have attempted this before. 11 The reflection phase in the SRL process is important to complete the cycle. Without it, the starting point in new learning endeavors might be misidentified. In addition, this study adds to the dental education literature, which is lacking in studies exploring attitudes towards self-assessment in clinical settings. 31 Another strengths of this study was the utilization of longitudinal data collection, where data were collected during clinical training from the self-DOPS form and from the questionnaire survey conducted at the end of the experiment. Nonetheless, this study is limited by its reliance on self-reported data, which might not reflect the actual behavior of students. Thus, future research should endeavor to find concrete objective evidence of SRL behavior after self-assessment-focused interventions.
It is worth mentioning that implementing this assessment protocol is not easy in the overcrowded and underequipped working environment at Damascus University, as indicated by the participants’ comments. The limitations encountered in our study could be somewhat generalizable to any clinical environment where there are time constraints and patient care pressure. Hence, attempts should be made to mitigate the limiting factors, as long as they do not affect the provision of care.
Conclusion
The study findings support the educational impact of self-assessment training in improving SRL and performance in the clinical context. This impact was apparent in all SRL phases: the forethought phase, performance phase, and especially the reflection phase. Participants’ perceptions of self-assessment were generally very positive. Taken together, these findings encourage the implementation of interventions targeting self-assessment and reflection in the process of fostering learners’ SRL ability in the clinical context.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241226820 - Supplemental material for Scaffolding Self-Regulated Learning in Operative Dentistry Through Self-Assessment Training
Supplemental material, sj-docx-1-mde-10.1177_23821205241226820 for Scaffolding Self-Regulated Learning in Operative Dentistry Through Self-Assessment Training by Ghaith Alfakhry, Khattab Mustafa, Kamal Ybrode, Bashar Jazayerli, Hussam Milly, Khaled Alhomsi and Issam Jamous in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205241226820 - Supplemental material for Scaffolding Self-Regulated Learning in Operative Dentistry Through Self-Assessment Training
Supplemental material, sj-pdf-2-mde-10.1177_23821205241226820 for Scaffolding Self-Regulated Learning in Operative Dentistry Through Self-Assessment Training by Ghaith Alfakhry, Khattab Mustafa, Kamal Ybrode, Bashar Jazayerli, Hussam Milly, Khaled Alhomsi and Issam Jamous in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors would like to extend their sincere thanks to Prof. Jorge Tricio, who helped us to revise the manuscript. The authors also acknowledge the trainees who participated in the study.
Authors’ Contributions
GA: conceptualization (lead), research design (lead), data collection (co-lead), formal analysis (lead), investigation (lead), methodology (lead), project administration (lead), supervision (lead), writing—original draft preparation (lead), writing—review and editing (lead). KM: methodology (co-lead), data collection (co-lead), project administration, writing—review and editing. KY and BJ: data collection (co-lead); project administration, writing—review and editing. HM: data collection, writing—review and editing. KA: project administration, writing—review and editing. IJ: supervision (co-lead), methodology (co-lead), writing—review and editing.
Availability of Data and Materials
The English version of the questionnaire survey data is available in figshare, DOI:10.6084/m9.figshare.23047181
The qualitative data (participants’ open comments) are in Arabic, and an English version can be made available upon reasonable request.
Consent for Publication
Not applicable.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the ethical committee of Damascus University Faculty of Dental Medicine on January 15, 2022 (no. 98735). Verbal informed consent was obtained from all participants prior to the study, and this mode of informed consent was approved by the ethical committee.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.