
Abstract
OBJECTIVES
Coaching is an interactive process of performance improvement accomplished by fostering a coachee's ability to critically self-evaluate, create goals, and develop a plan for action. It is being increasingly used in medical education, both at the undergraduate and graduate levels. The American Medical Association (AMA) recommends robust faculty development for any coaching program. Our institution created a mandatory coaching program for students starting in August 2022 with 22 faculty coaches.
METHODS
We used Kern's 6-step model for curriculum development to create our institution's faculty development for coaches. This manuscript describes the process of development, implementation, and early program evaluation for the curriculum for faculty coaches for the first 4 months of our mandatory coaching program. The objectives and teaching strategies are outlined. Our program evaluation consisted of immediate and follow-up surveys of faculty attendees.
RESULTS
Content in the faculty development program describing the medical student curriculum, assessment, and student resources improved faculty perceived knowledge and confidence. Specific training in coaching skills, including a simulation using standardized students was used and found to be essential. We offer lessons learned from our coaches regarding timing and content for any faculty development curriculum for new coaches.
CONCLUSIONS
Considerations for future faculty development curricula for academic coaching programs include timing of the faculty development, content consideration after three coaching sessions, and potential content additions and deletions. The curriculum outlined can be taken and immediately adapted for any school of medicine embarking on a coaching program for students.
Introduction
Coaching has an important and growing role to play in medical education. The increasing complexity and rate of change in modern medical practice tells us that learning should not and cannot be confined to medical school and residency, but must be continued throughout a medical career.1,2 Therefore, medical education must foster the skills and attitudes essential to lifelong learning and continuous professional development with curricula that are increasingly learner-driven, time-variable, and competency-based.1–5 Coaching's bottom-up, individualized, performance-driven approach makes it especially well-suited to supporting these educational goals.1,4
Coaching is an interactive process of performance improvement accomplished by fostering a coachee's ability to critically self-evaluate, create realistic goals, establish a plan of action, and then reassess.1,3,6 Coaching is distinguished from didactic and small group teaching, mentoring, or advising, each of which is characterized by information flowing from senior to junior with a goal of conveying discrete facts and information (teaching), broader career perspectives and lessons learned (mentoring), or proven approaches to specific problems (advising).1–3,6 In contrast, coaching is coachee-centered, characterized by probing questions and focused on individual improvement.1–3,6
Coaching relationships are mutually beneficial. Students benefit from the development of self-regulated learning skills and sustainable work practices that will enable lifelong learning and reduce burnout.4,7–10 Additionally, coaching feedback supports professional identity development, prompting students to reflect on their growing competence and encouraging them to “think, feel, and act” like a physician. 10 Faculty coaches, in turn, benefit from greater connection to and meaningful interaction with incoming classes, 7 a feature which is likely to be of particular importance as more schools shift to distance and hybrid learning models reducing the opportunities for incidental encounters.
The transition from teaching and mentoring to coaching requires effort at the institutional and individual levels. Among surveyed institutions with coaching programs, just two in three selected a description of coaching (help the student develop their own strategy with clarifying questions) in describing their programs. 11 For faculty, the adoption of a learner-centered approach using reflective listening and probing questions takes practice and discrete skills development. 7 In one study new coaches reported role tension between the coach role and supervisory/mentorship responsibilities. 7 Additionally, coaches describe a challenge balancing structured coaching sessions against individual student needs, which tend to become more divergent as medical training progresses. 7
The goal of a faculty development curriculum for new coaches is to bridge the gap between existing and desired coaching capabilities for a particular institution. A shared vision of roles and goals is paramount for success. 12 The American Medical Association (AMA) Coaching in Medical Education faculty handbook broadly recommends a mix of asynchronous self-regulated learning for content knowledge (e.g. policies, guidelines, students’ curriculum) and in-person workshops and experiential learning to develop skills (e.g. asking probing questions, reflective listening, goal setting, giving feedback). 12 In order to facilitate a shared vision, part of the faculty training needs to convey coaching as a construct and introduce the use of the master adaptive learner model to support the concepts of self-regulated habits. 13 Ongoing programmatic feedback and needs assessments can be used to iteratively refine the faculty development curriculum. 12
Despite these recommendations and generalized suggestions, the authors could not find a detailed coaching curriculum published. In current coaching programs coach training ranges widely, from a single day to ongoing monthly sessions. 11 As such, this manuscript will describe the development of an 18-h faculty development curriculum, using Kern's framework for curriculum development, for new faculty coaches in undergraduate medical education. 14 The description of the development and implementation of the curriculum provides a practical approach to training faculty coaches as medical schools launch more coaching initiatives. The local IRB reviewed this curriculum, Protocol DBS.2022.371, and determined as a program evaluation it did not meet criteria defined as research.
Methods
Needs Assessment and Literature Review
Our medical school matriculates 170 students annually. The first 16 months are completed at the school. Our core clinical rotations occur at 23 outlying teaching sites at military hospitals spanning the United States over the next 12 months. The remainder of the curriculum is a combination of clinical electives, research opportunities, and military leadership development exercises.
A working group of local faculty charged with strategically planning and implementing our coaching program performed problem identification and local needs assessment. We identified numerous stakeholders of the program to include the students, faculty, Department Chairs, Student Affairs, and the institution as a whole. 15 For the local needs assessment, one of the authors created a list of potential topics derived from our literature review. Members of the group reviewed the list for potential addition and deletions. A subsequent discussion refined potential material to ensure enhancement of faculty understanding and appropriate allotment of time needed to complete the curriculum.
Creation of Goals and Objectives
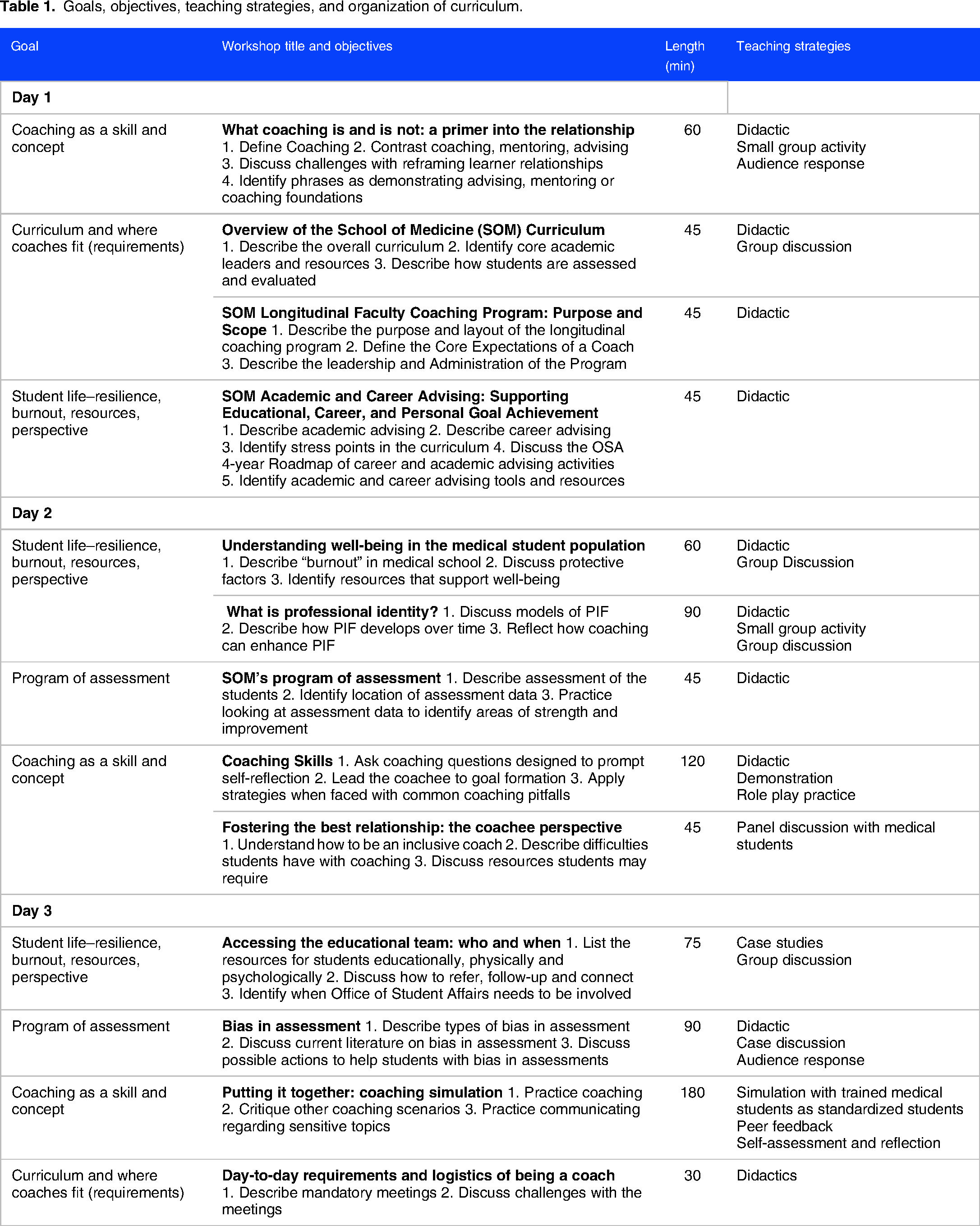
Four overarching goals were created for the curriculum to guide its individual objectives. Two of the goals were to clearly understand the four-year curriculum and grasp the assessment plan. Many coaches were not familiar with the balance of lecture and small group instruction, order of content, and grading criteria of individual module and courses. We believed if a coach fully appreciated the curricular elements, they could more effectively set short-term academic goals including studying effectively. The other overarching goals included appreciating student life and well-being, and coaching as a construct and skill. An ancillary fifth goal was to actively create a coaching community; this underpinned the decision to have all in-person mandatory training. The specific objectives and the workshop length were developed and listed in Table 1.
Goals, objectives, teaching strategies, and organization of curriculum.
Teaching Theory and Strategy
Kolb's experiential learning framework guided the teaching methods. 16 A constructivist approach was used to purposefully build on a participant's prior experience with coaching and student life. Kolb required us to consider prior concrete experience and add information for abstract conceptualization and also ample real-world cases for reflection throughout the curriculum. We also utilized simulation to give opportunity for the faculty learning to become coaches with active experimentation.
The coaching curriculum contained numerous items many faculty had not been introduced to previously. As such, lectures were used as a major strategy. Active learning was introduced with discussions that included both large group and small group (e.g. buzz groups and think/pair/share) opportunities. Audience response was polled often with Poll Everywhere. Simulation was used to allow faculty to practice coaching skills both in short peer coaching sessions and as an objective structured teaching evaluation with standardized learners. The longer simulation allowed for self-reflection and peer feedback as additional educational strategies. Table 1 shows the workshops with the strategies used.
Implementation
In our initial year, 22 coaches attended the 2.5 days of training spread across several months. Timing was based on resource availability. Several experts were asked to deliver content. Department chairs were asked to make their faculty coaches available to attend all trainings in-person. There was no recording of sessions to review later.
Program Evaluation
Paper surveys designed by one of the authors (JS) were administered to all 22 participants at the conclusion of each day of the curriculum (three separate surveys). A fourth survey was sent via email after three initial coaching sessions, and 5 months after the conclusion of the curriculum. All surveys consisted of between four and 11 Likert-style questions with one or two open-ended free-text questions. All surveys were anonymous. The response rate for the paper, end of day, surveys was 81% (18/22), 54.5% (12/22), and 45% 10/22. The response rate for the follow-up survey was 95.4%, (21/22). Consent was implied with survey return.
The surveys were designed based on Kirkpatrick's levels to evaluate educational programs.17,18 Outcomes are described in four levels: level 1 is the learner's reaction, level 2 is learning and is subdivided where 2a is change in attitude and 2b in skills, level three is behavior change subdivided into a self-assessment (3a) and what is observable by others (3b), and level 4 is a change in the organization. 18
Level 1 Reaction: All respondents rated the activities either “good” (12%) or “excellent” (88%) and the materials as “mostly organized” (10%) or “very organized” (90%). Regarding timing of the training, participants thought it should either be 3 full days spread over 3 months (39%) or as 6 half-days spread over 1-2 months (33%) and that these days should take place within 3 months (58%) to 6 months (37%) of the start of the academic year. 95% of respondents found the time allocated to coaching skills was adequate.
Level 2 Learning: Knowledge was assessed with pre- and post-self-assessment questions on the individual days of training. 67% of coaches were “not at all” or “slightly” familiar with career advising. After the session, 100% were “somewhat” or “very” familiar with career advising (Figure 1). Similarly, 73% were “not at all” or “slightly” confident in their ability to explicitly discuss professional identity formation. After the session, 100% were “somewhat” or “very” confident (Figure 2).

Pre- and post-self-assessment of familiarity with career advising, N=18.

Pre- and post-assessment of confidence explicitly discussing professional identity formation. N=12.
Participants entered the program with varying degrees of familiarity with the School of Medicine (SOM) curriculum, with 39% “not at all” or “slightly” familiar and 61% “somewhat” or “very” familiar. After the first day of training, 100% were “somewhat” or “very” familiar with the curriculum (Figure 3). Eleven months later, reflecting on a completed coaching session, 100% of respondents “agreed” or “strongly agreed” that they “understood [their] students’ comments, discussion and perspectives about the curriculum.”

Pre- and post-assessment of familiarity with the School of Medicine curriculum. N=18.
Level 3 Behavior: Regarding coaching skills, faculty were asked level 2 pre- and post-self-assessment questions and later self-report questions about coaching behavior. Coaches entered the curriculum in December 2021 with either no previous formal coach training (59%) or a few readings (41%). After their third coaching session in November 2022, 95% “agreed” (57%) or “strongly agreed” (38%) that they could engage in coaching to elicit students’ goals and create plans, while 5% disagreed. All respondents reported either “greatly improved” confidence or “feel[ing] ready” immediately after the coaching simulation. Five months later and reflecting on completed coaching sessions, 90% “agreed” or “strongly agreed” the simulation aided their preparation for coaching and 81% “agreed” or “strongly agreed” the simulation was realistic regarding student situations and perspectives.
Qualitative comments were overall positive. The day-of feedback is organized by session in Table 2 (December 2021; March and June 2022). In the follow-up survey, we received comments about “things I wish I knew” shown in Table 3.
Qualitative comments from day of training (directly after session) surveys.

“Things you wished you had known” responses from faculty coaches.

When asked to identify which sessions could be omitted in the future, career versus academic advising, professional identity formation, and bias in assessment were each selected three times, which was the most of any sessions.
Discussion
Over the past decade increased interest, support and recommendations have been published for coaching in medical education. Despite compelling advisement for faculty development, no in-depth description of that requirement is described. 8 We describe a curriculum to train new faculty coaches with immediate and 3-month follow-up data from our coaches.
Our inaugural course was two full days (April and June 2022) and one half-day(December 2021) spread over 6 of the 8 months prior to the start of the academic year. This configuration was driven primarily by resource availability, namely room and faculty availability. On reflection, participants preferred three full days spread over three months, or six half-days spread over no more than two months, taking place within 3-6 months of the start of the academic year. For an institution that, like ours, starts in August, training could be accomplished with one day each in May, June, and July; or, alternately, six half-days spread over May and June. Summer months are particularly challenging for faculty availability, both for personal reasons and curricular reasons. Often faculty are working on curricular updates or scholarly work during the students’ break. Additionally, at our institution, approximately 40% of our faculty, as military physicians, periodically relocate globally. The added burden to participants of coordinating periods of non-availability on six separate occasions versus three may drive the curriculum toward the less impactful option.
Coaches identified specific sessions which could be eliminated from the curriculum: career versus academic advising, professional identity formation, and bias in assessment. It is worth noting this feedback occurred 3 months into an anticipated 42-month coaching relationship and the value of having covered these topics may yet manifest as the program continues. Encountering bias in assessments is more likely to occur in subjective workplace assessments during clinical rotations. Professional identity formation struggles and discussion is also more likely to occur once students begin rotating in clerkships with opportunities to wrestle with the challenges of each medical specialty. One consideration this raises is the possibility of shifting some of the faculty development from before coaching to ongoing development timed to coincide with relevant milestones in the School of Medicine curriculum. The challenge may be ensuring all coaches attend where faculty had Chair support at the beginning of their coaching time.
All prospective coaches came to the program with minimal prior coaching training, either “none” or a “few readings.” After completing the curriculum and reflecting on three actual coaching sessions, almost all (95%) were able to successfully engage in coaching. While the reaction to the simulation immediately after the session was uniformly positive and all participants felt either “greatly improved” or “ready,” reflection on behavior after the first coaching session revealed some opportunities for improvement. 10% of respondents found that the simulation did not aid their preparation, 19% thought it was unrealistic, and at least one thought the session could be omitted altogether. The authors consider simulation a central aspect of preparation to assume the coaching role and align well with Kolb's experiential learning. In faculty development, role playing is seen as effective when following best practices. 19 It is worth nothing that only one of the four simulation cases (example simulation in the supplemental material) addressed the early medical curriculum. The other three simulation cases will occur as the coaches move through the curriculum. Simulation is an additional active strategy for learning. As with our learners, faculty need a variety of teaching strategies to learn new skills and we recognize dichotomous faculty opinions of the strategy.
Coaches noted difficulties arising from the mindset of some early medical students, where the students’ perception of very high stakes placed marked pressure on coaches to provide “The Answer.” This dynamic exists in significant tension with the coach's role of asking probing questions and allowing students to develop their own solutions. One specific challenge which coaches should be prepared for: how to address the age-old question, “will this be on the test?”
Quantitatively, the single biggest deficiency in preparing new coaches was the 37% who were not comfortable reviewing provided assessment information prior to coaching sessions. In short, when compared to the sample student packets provided during the coaching simulation, the actual student packets had less information, and were more difficult to interpret. Our full program of assessment and student dashboards were being developed during the training, so this feedback was expected. In the next session we will need to reevaluate this specific aspect.
Coaches requested more information regarding student resources in order to be effective in goal setting. In the next cycle we will be adding this content.
Our program has some limitations. As most curricula, this took place in one institution. Although the global curriculum could be implemented at any university, a few alterations will be needed in specific content and implementation. With our lack of resources, we were not able to perform a more rigorous analysis of faculty coach learned skills. With the second cohort, our peer observers may be able to perform some sort of checklist of coaching behaviors. However, updated views of Kirkpatrick's level 3 evaluation of training include self-assessment of application of learning. 18 A third limitation is the lack of validated program evaluation. Since this is the first in-depth coaching curriculum for faculty development evaluated, to our knowledge, we created surveys to assess our specific questions regarding knowledge attainment.
Conclusions
Coaching in medical education has gained momentum over the last several years. We based our coaching curriculum on the needs of our faculty while using suggested published content for coaching programs in medical school. We used a known theoretical educational theory to underpin our curriculum, followed best practices for curriculum development, and used variety of teaching strategies to make content tangible to faculty learners. The session titles and objectives are generalizable with another school of medicine describing specific curricula, advising plans, assessment programs, and logistics of their specific coaching program. The other sessions are foundational and applicable to all schools of medicine such as coaching skills with simulation, bias awareness, and professional identity formation. Local resources would affect implementation considerations such as instructors, timing, and method of teaching. This curriculum could be adapted for faculty development at any medical school.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231217896 - Supplemental material for A Model Curriculum For New Faculty Coaches in Undergraduate Medical Education
Supplemental material, sj-docx-1-mde-10.1177_23821205231217896 for A Model Curriculum For New Faculty Coaches in Undergraduate Medical Education by Thomas Lance Tippit, Irene Chi and Jessica T. Servey in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231217896 - Supplemental material for A Model Curriculum For New Faculty Coaches in Undergraduate Medical Education
Supplemental material, sj-docx-2-mde-10.1177_23821205231217896 for A Model Curriculum For New Faculty Coaches in Undergraduate Medical Education by Thomas Lance Tippit, Irene Chi and Jessica T. Servey in Journal of Medical Education and Curricular Development
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not reflect the official policy of the Uniformed Services University of the Health Sciences, the Department of the Army, Navy, Air Force, Department of Defense, or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.