
Abstract
OBJECTIVE
This study was conducted as part of a curricular reform process in Faculty of Medicine (FOM), King Abdul Aziz University Jeddah Saudi Arabia. It explored the perspective of FOM stakeholders on the challenges and factors in the teaching and learning domains that are affecting achieving learning outcomes.
METHODS
Faculty teaching in the second and third year, students in third and fourth year, and administrative personnel were included. An electronic survey was created. Chi-Squared test for independence was used to test the association between the correspondent group and different statements. Kruskal-Wallis ANOVA was used to examine the differences in medians among the questions utilizing ranks to evaluate different questions, followed by post hoc pairwise comparison with Bonferroni-corrected alpha.
RESULTS
A strong association was seen between the correspondent level and perspective on time allocated for modules and vertical integration of the curriculum. Among the most highly ranked challenges for using various teaching strategies were the loaded curricula content and the limitation of time, with an overall median rank of 8. Student readiness and motivation were also significant factors, however, students considered motivation less of a challenge.
CONCLUSION
Continuous assessment of factors affecting teaching and learning will bridge gaps in curriculum.
Introduction
A curriculum can be defined as “a statement of the intended aims and objectives, content, experiences, outcomes, and processes of an educational program, including a description of the training structure and of the expected methods of learning, teaching, feedback, and supervision.” 1 Over the years, there has been a shift in medical education from a process of simply delivering knowledge to a process of developing skills and competencies. In addition, accreditation bodies worldwide require clearly stated program goals and objectives, educational strategies to achieve these goals and evaluation. 2 This has all put great responsibilities on educators in the health profession in planning and assessing educational experiences. Nowadays, curriculum evaluation and development are considered a purposeful activity of any educational institute, with growing demands for dealing with it as an active process that truly involves all stakeholders rather than an every seven-year event.
A Brief History of the Medical Curriculum at King Abdul Aziz University (KAU)
Since the establishment of the Medicine and Surgery educational program (MBBS) in 1975 at King Abdul Aziz University (KAU), Jeddah, Saudi Arabia, the curriculum has experienced several phases. The first phase lasted for over three decades. Within this era, it was a six-year traditional curriculum, which consisted of three years of basic and medical science courses, three years of clinical training, followed by a year of internship.
Since the 2000s, there were several concerns of the disadvantages of the traditional curriculum, limited opportunities for more effective student-centered learning, overload of the curriculum, overemphasis on certain subjects, and the inclusion of some less relevant subjects. This fueled a call for change within the Saudi medical community in general and extended to the Faculty of Medicine (FOM) KAU. 3
The second phase of the curriculum witnessed a movement toward innovation, with a drive to excellence and recognition by international agencies and institutions. In 2007, KAU FOM changed its curriculum from a teacher-centered model of teaching to a student-centered model of learning. Didactic lectures and structured classroom time were decreased. 4
The MBBS curriculum consists of 261 credit hours. Students join the program after passing a mandatory preparatory year that consists of 11 courses that prepares students in the English language, general biology, general physics, general chemistry, computer science, and communication skills. The second year of the student's academic journey starts in the FOM where the students have 14 courses that are taken throughout the academic year (Table 1). These courses are basic science courses that are prerequisites to third year modules. During the third year, students study system-based modules. In addition, they are required to take early clinical experience and communication skills modules and an Islamic culture course (Table 2).
Second-Year Timetable.

Third-Year Timetable.

The Effect of Various Stakeholders
Faculty
Curriculum development has traditionally been an essential responsibility of external experts; excluding faculty members from active participation in the curriculum development process. 5 Through their knowledge, skills, and experiences, faculty members’ role is becoming more prominent. 6 Usually, faculty members participate by working with curriculum development teams and specialists to organize and create martial, textbooks, and content. 7 Besides their role in planning and delivering content, their pedagogic perspectives on learning can determine the choices they make in their teaching. These perspectives embody the theories and beliefs they hold about teaching and learning. 8
Students
The traditional role students played in any curriculum development initiative was through the evaluation of the teaching process. Recently, it was noted that engaging learners in the design of the teaching and learning strategies contributed significantly to the advancement in the quality of education. 9 This finding encouraged the development of more dynamic student roles in curricular development where students brought in broad and unique knowledge of the curriculum, shared their perspectives and provided ideas for improvement. 10
Administrators
Teaching practices are shaped by a variety of factors and evidence suggests that some education changes fail to develop because of excessively top-down approaches that ignore the current knowledge and expertise of faculty. 11
In 2017, the Saudi National Commission for Academic Accreditation & Assessment NCAAA accredited the Medicine and Surgery program. This accreditation extends from 2017 until 2024. Since accreditation was granted, FOM has been continuously working on its curriculum. Although the assessment of teaching and learning of the curriculum was assigned to Medical Education department (MED), studies describing the needs assessment and curriculum development of MBBS program were lacking. The first step was forming committees to plan and execute needs assessment initiative. The committee consisted of faculty members from both the MED and curricular supervisors of basic sciences departments. The committee met several times and followed a specific curriculum development process. The aim was to explore how the curriculum was taught, what were the major challenges facing both faculty and students to attain learning outcomes, and suggest several initiatives for improving teaching and learning.
Several factors may influence the teaching learning process in higher education. However specific research on the factors that affect students from achieving their learning outcomes in Saudi Arabia is limited. This paper aims to explore stakeholders’ perspective of the current situation on teaching and learning since the implementation of the new curriculum. We aim to understand what are the main factors and challenges in teaching and learning domains that affect attaining learning outcomes. We hope the findings will inform stakeholders and impact policies to improve faculty development and other support structures essential for curricula success.
Methods
Study Design and Setting
This was a cross-sectional study conducted by MED at KAU, FOM, Jeddah, Saudi Arabia, during the academic year 2021–2022. It was conducted as part of a needs assessment for curriculum development in the teaching and learning domains.
Participants
All faculty members of basic medical sciences departments teaching in the second and third years were included. All undergraduate medical students (pursuing their third- and fourth-year studies), were also asked to participate. An invitation to participate was extended to administrative personnel including the dean, vice deans, members of MED, members of the quality unit, and members of the assessment unit. The reason we excluded faculty teaching in clinical years is because a second study is still undergoing, exploring perceptions of faculty members and students in clinical years. Exclusion criteria were demonstrators, whom are the newly appointed teaching assistants due to lack of involvement in the teaching process. The requirement of an informed consent was waived off by the Biomedical Ethics Research Committee at the FOM, at King Abdul Aziz University reference # 25-21 on 14–12–2021.
Description and Data Collection (Survey)
At the beginning of the study, FOM curriculum executive committee assigned the MED to create a task force responsible to assess certain aspects of the teaching and learning domains in the curriculum. The main themes agreed upon were course nature and plan, teaching strategies, achieving learning outcomes and resources. A 17-item electronic survey was created for faculty and administration and a 12-item survey was created for students. For initial validity evidence, we shared the questionnaire with statisticians and experts in the curriculum development area to evaluate the psychometric characteristics of the survey. The survey was also pretested on smaller population of faculty (5%) of total 235 faculty members and on students (4%) of 472 students. For further validity, a pilot test was conducted on a subset of faculty members and students to evaluate the content and clarity of items.
An apriori sample size calculation for proportion with a correction for a finite population was conducted to achieve a 95% confidence interval and a 5% maximum margin of error using the following equation:
where nf is the sample size for a finite population, n is sample size for an unlimited population, z is the z-score for the suggested confidence interval, p is the expected response rate (proportion), e is the accepted margin of error, and N is the population size. Based on previous studies, a response rate ranging between 30% and 60% is expected to be achieved.12–14 Here, we opted to use a lower response rate of 30% to calculate an adequate sample size. The table below lists the required sample size for each population accordingly.

While the required sample was met for faculty members, nearly met by the administrator faculty members, and almost met by students, the response rate exceeded the expected proportion set in the sample size calculation. Furthermore, a post hoc power of 0.97 or larger based on the smallest effect size (Cramer's V = 0.220) in the study validated the sampling method at the desired margin of error.
To ensure maximum dissemination and participation of faculty members and students, both heads of departments and student team leaders were involved in distributing the anonymous survey using an official communication interface.
Statistical Analysis
The quantitative data were entered into the Statistical Package for the Social Sciences (SPSS, v. 26.0, Chicago, USA). For statistical data analysis, Chi-Squared test for goodness-of-fit was used to verify the equal distribution of sampling whenever applicable. Chi-Squared test for independence was used to test the association between the correspondent group (Administrative faculty, faculty, or student), and different statements. Post hoc examination of the adjusted standardized residuals was used to pinpoint the source of significance. Kruskal-Wallis ANOVA was used to examine the differences in medians among the questions utilizing ranks to evaluate different questions, followed by post hoc pairwise comparison with Bonferroni-corrected alpha. The effect of gender on ranks was evaluated using the Mann-Whitney U test. Data adherence to normal distribution was evaluated with the Shapiro-Wilk test when applicable.
Results
Participants Characteristics
The survey was sent to all faculty members teaching in second and third—a total of 235 faculty members—and all third year and fourth year medical students—a total of 472. All in all, 188 faculty and 167 students responded. Descriptive statistics of participants are summarized in Table 3.
Descriptive Statistics of Participants.

Participant opinion on the Suitability of Allocated Time, Course Order, Vertical Integration, Teaching Strategies, and Available Resources for Teaching and Learning
When evaluating if the assigned time allocated to the courses or modules was suitable, the answers of the correspondents significantly deviated from the expected equal distribution (χ2 (8, 365) = 190.36, P < .001; Table 4). Post hoc examination shows that the students either significantly strongly disagreed (P < .001) or disagreed (P < .001) with the statement, on the other hand, the faculty strongly agreed that the allocated time was suitable (P < .001). Cramer's V value indicates a very strong association between the correspondent level (administrative, faculty, or student), and their opinion about the allocated time (Cramer's V = 0.511, P < .001). When the correspondents were asked if the order of the courses or modules was suitable and required no changes, the answers significantly deviated from the expected equal distribution (χ2 (8, 365) = 91.51, P < .001). Post hoc examination shows that students significantly disagreed (P < .05) or were not sure (P < .001), whereas the faculty significantly agreed that the order was suitable (P < .001). Interestingly, significant differences were found in correspondents’ opinion regarding the vertical integration of the curriculum into the clinical years (χ2 (8, 365) = 80.08, P < .001). Students strongly agreed with it (P < .001) unlike the faculty who surprisingly were not sure and did not know (P < .001). Interestingly, 50% of administration personnel seemed to disagree and strongly disagree with this statement. Overall, Cramer's V value indicates a strong association between the correspondent level (administrative, faculty, or student), and their opinion about vertical integration (Cramer's V = 0.331, P < .001). When assessing if correspondents believed that other teaching strategies other than lectures were used, most participants agreed; however, upon post hoc examination a small number of students (15), significantly and strongly disagreed that other teaching strategies are also used (P < .001; Table 4).
Participants Opinion on the Suitability of Allocated Time, Course Order, Vertical Integration, Teaching Strategies, and Available Resources on Teaching and Learning.

Significant increase from the equal distribution, determined by pos hoc testing by examining the adjusted standardized residual and appropriate Bonferroni-adjusted alpha, are written in bold numbers. ***Extreme significant (<0.001), **Very significant (<0.01), *Significant difference (<0.05).
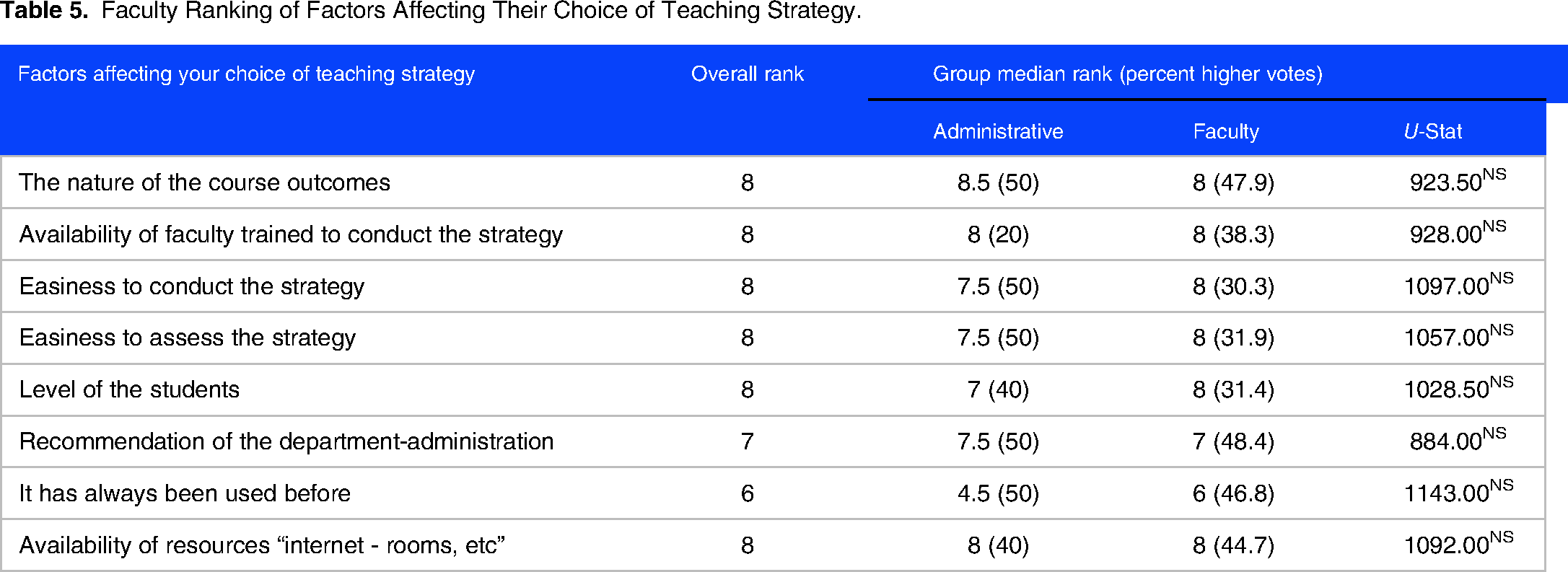
Faculty Opinion on Factors Affecting Their Choice of Teaching Strategy
When asked to rank factors that affect their choice of teaching strategies, faculty ranked whether the strategy has been used before and whether it is recommended by the department and/or administration as the least considered factor in affecting their choice, with an overall median rank of 6 and 7 respectively (Table 5). While all the other factors ranked an overall median rank of 8. To evaluate if there were any differences among the votes of the administrative faculty and teaching faculty when ranking, a Mann-Whitney U test was used. However, no significant difference was found between the two groups in all questions.
Faculty Ranking of Factors Affecting Their Choice of Teaching Strategy.
Participants’ Opinion About Challenges in the Use of Teaching Strategies
Overall, out of all the nine possible challenges provided, the highest-ranking challenges for using various teaching strategies were the loaded curricula content and the limitation of time for courses or modules, with an overall median rank of 8 (Table 6). To evaluate if there are any differences among the three groups (administrative, faculty, or students), when ranking the challenges, a Kruskal-Wallis H-test was used followed by Post hoc test. Notably, faculty significantly ranked resources (P < .001), students’ level and readiness (P < .001), administrative support (P < .001), and technical and logistic issues (P < .001), above the overall median rank. Students, on the other hand, significantly ranked overloaded curricula (<0.01) above the overall median rank.
Participants Ranking of Challenges to the Use of Teaching Strategies.a

Numbers written in bold indicates a significant score above or below the overall median rank. ***Extreme significant (<0.001), **Very significant (<0.01), *Significant difference (<0.05), NS not significant.
Participants Opinion About Challenges to Achieving Learning Outcomes
We were also interested in studying participants’ perspectives on the challenges to achieve learning outcomes. Like challenges of using teaching strategies, the loaded curricula content and the limitation of time for courses or modules ranked the highest, with an overall median rank of 8. When evaluating if there are any differences among the three groups (administrative, faculty, or students) when ranking the challenges, it was noticed that the faculty significantly ranked students’ abilities (P < .001) and resources (P < .001) above the overall median rank. Also worth noting, students appeared to consider student's motivation less of a challenge and of less importance ranking it 5 which was significantly lower (P < .01) than the overall median rank.
The Effect of Faculty Gender and Academic Status on Voted Ranks
Given the significant differences that were seen with faculty responses in the ranking questions, we asked whether gender and academic status influenced the ranking votes. Mann-Whitney U test was used to examine the effect of gender and academic status on the voted ranks. We found that male faculty significantly (P < .01) chose teaching strategies based on whether it had been conducted before more than the female faculty. Similarly, but to a lesser extent, male faculty ranked nature of learning outcome, and easiness of conducting and assessing the strategy higher than females (P < .05) as factors affecting their choices of teaching strategy. When assessing challenges in using teaching strategies, female faculty found that the lack of enough allocated time in the course/module was a more significant challenge (P < .001) compared to the male faculty. In addition, female faculty considered students’ abilities as a more significant challenge to achieving learning outcome (P < .05). When evaluating if academic status effected ranked votes, group votes significantly differed only in the item “not enough allocated time in the module” among the challenges affecting the choice of teaching strategy (P < .01). Pairwise Post hoc comparison shows that associate professors significantly voted a higher rank (9) than professors (7).
Discussion
The process of developing a medical education curriculum can seem overwhelming but when broken down into specific tasks can become easy to achieve. We adopted the integrated framework for curriculum development in higher education, which consists of five stages. 15 In our study, Stage 1 was initially triggered internally by clinical faculty members complaining that students who finished the basic years (second and third year of the MBBS curriculum) are not well-prepared and lack essential knowledge. Both students and administrators were also encouraging the need for curricular evaluation and development. Externally, there was a need to assess the curriculum since NCAAA accreditation expires in 2024. In Stage 2, competencies to be developed were adopted from the Saudi Medical Education Directives Framework (SaudiMEDs). In Stage 3, based on data triangulation from all needs assessment initiatives, the curriculum will be designed. In Stage 4, various teaching and assessment strategies will be aligned with intended learning outcomes. At Stage 5, implementation, monitoring, and evaluation will be conducted. Currently, we are at Stage 1, and we aim for the results of this study to inform other universities that are exploring the teaching and learning domains.
This study assessed what factors might affect the teaching and learning experience at KAU. The results were analyzed with an eye on areas that will require further development whether in the knowledge, skills, and/or attitudes domains. Several perspectives were used to explore the challenges; academic roles, academic status, and gender. The themes that emerged repetitively were curriculum content overload, time allocated for courses, teaching strategies, and student readiness and motivation.
Looking at curricular content overload it was interesting to find that all stakeholders (students, faculty members, and administrators) agreed that this negatively affected achieving learning outcomes. This was even more profoundly seen as a challenge by students. Research has shown that processing information might indeed cause potential problems because of the great demands induced by learning tasks as complex as those in medical training, and this might surpass the processing capability of the students ‘cognitive system. 16 However, strategically addressing and incorporating content overload in improving learning has also been discussed. One of the approaches is using cognitive load theory where teaching and learning activities are strategically planned with consideration to the mental effort used in the working memory when dealing with specific tasks. This requires that both faculty members and curriculum planners take three issues into consideration: Task fidelity, task complexity, and instructional support. 17
When exploring vertical integration in curriculum content it was interesting to find out that students were able to recognize where integration is present; faculty were not sure if there was evidence of vertical integration and administrators believed that no integration existed. The latter finding can be explained because administrators are seeing the full curricular picture and continuously aim to establish both horizontal and vertical integration. The ongoing efforts to refine the program should not be guided by administrators alone. Curriculum planning and development requires more consistent and regular dialogue among both administrators and faculty members. This collaboration is starting to emerge in KAU with the recent changes in creating task forces that include heads of departments of both basic and clinical sciences. Whether these task forces will affect better communication and collaboration is yet to be assessed. Faculty members’ inability to recognize the integration might also signify poor communication among the basic science faculty (second and third year) and clinical years faculty (fourth, fifth, and sixth year). It might be advisable to ensure communication to institute monthly meetings between basic and clinical sciences departments, where coordination of content is the main theme to explore. Other factors that might cause faculty members uncertainty of integration are the invisibility of learning trajectories, lack of curricular alignment, and/or lack or misuse of curriculum mapping tools. 18
What is thought-provoking is that students—the front-line stakeholders—were able to recognize integration. It could be that that realization has emerged as a personal student effort. Additionally, many students may connect with older peers as part of a university society or in their own time.
Engaging students in curriculum development is a growing trend in medical education. Usually, the role of students in curriculum development has been just providing feedback about current courses, serving as liaisons between faculty and students, and focusing on quality assurance.19,20 Brooman, found out that listening and responding to the student voice in curriculum development improved students’ grades, students’ perceptions of the curriculum, and attendance. 21 Assuming that curriculum design will be accepted by students as a default is a misconception that we need to address.
When addressing curriculum content as a factor affecting achieving learning outcomes it is important to address how this curriculum is being taught. Teaching strategies used in KAU were not seen as determinantal factors in the learning and teaching experience. This was odd because when we asked faculty members about challenges facing them when choosing a teaching strategy, they were able to specifically mention availability of resources, level of students, administrative support, and technical support. There is a missing link here, which is faculty recognizing the importance of curriculum planning but failing to recognize the effects of teaching strategies.
Students were also not able to recognize the effect teaching strategies have on achieving their learning outcomes. Could this be a response to what student experience with the increased cognitive effort associated with teaching strategies that use active learning? Deslauriers et al 2019 explained that students tend to initially take the increased cognitive effort as a sign of poorer learning. Perhaps explaining the advantages of working hard during active learning should be shared with the students early in the semester. 22 Students’ inability to recognize the benefits of teaching strategies is not greatly surprising if some teaching activities used are passive, not well designed or executed to enhance learning through collaboration. 23 This might necessitate teaching faculty to have a consistent approach to design teaching activities, minimizing the ambiguity of the teaching strategies used, and realizing its effect on the learning experience. Will knowledge of the teaching strategy positively affect the student learning experience? Would we see more appreciation, attendance, and involvement from the student side if they understand the rational for using certain teaching strategies?
Faculty members’ role surpass explaining benefits of active learning and extends to deliberately plan active learning sessions that allow integration, self-reflection, experimenting, and self-assessment. 24 Administration, on the other hand, should provide faculty development programs that ensure the consistent deployment of active learning strategies within the curriculum. 23
Although both faculty and students agreed that time is a major challenge to achieving learning outcomes, there was yet a different opinion regarding allocated course time in the curricula. Both faculty members and administrators thought that time was sufficient while students significantly disagreed. A shortcoming of this research was an agreed upon definition of “time.” Are stakeholders referring to time allocated to teaching sessions or time students need to study? In 1876, Thomas Huxley stated that “The burden we place on the medical student is far too heavy and it takes some doing to keep from breaking his intellectual back.” One must be honest; with the vast amount of knowledge, accreditation demands, and daily emerging trends in medical education, are we breaking the students’ intellectual backs? Are we allowing enough time for the student to self-regulate and reach learning outcomes?
Another interesting finding was that although both faculty members and administrators were able to recognize the role of student motivation in achieving learning outcomes, students could not. What makes students unable to connect motivation to their learning experience is alarming. It is agreed upon that it is the faculty and administrators’ responsibility to provide the climate for the development of optimal motivation and provide resources for developing aspiration, independent learning, and achieving goals. 25 A suggested approach is through planning learning sessions which include both in-class and out-of-class experiences that involve students in hands-on application or use of their learning. These applied learning experiences can be presented within a discipline or interdisciplinary, and they can befall within or outside of coursework. 26
Limitation of the Study
Despite achieving a high response rate with faculty members, one of the limitations of this study was the relatively low response rate of students (40%) which might increase nonresponse bias. In addition, demonstrating students’ grades and program learning outcomes’ achievement within the last five years would have added more value to the study, driving specific action plans and restructuring teaching and learning methods accordingly. One of the other limitations is the missing correlation between the views of the faculty of basic sciences with clinical sciences faculty. This would enrich how curriculum is viewed and help bridge the gap between basic and clinical departments. Exploring student experience through their perception is a good starting point. More studies are needed to ensure the reliability and validity of the needs assessment findings.
Conclusion
The process of developing and improving curriculum is one of the cornerstones to achieve academic accreditation. The goal is to confirm that the curriculum is effective in promoting improved quality of student learning. Through this study, stakeholders were not only given a voice to represent the assessment of teaching and learning domains at KAU but also were able to realize the importance of open communication among each other. Some of the findings show that there are different perceptions about curriculum among stakeholders. Although students were given a seat on most curricular committees their voice is not clearly incorporated in curricular design. This study acts as an initial step in exploring what the stakeholders at KAU perceive. However, more studies are needed to explore the actual experience. For example, a correlation between objective learning outcome achievements and perceptions.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231212297 - Supplemental material for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia
Supplemental material, sj-pdf-1-mde-10.1177_23821205231212297 for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia by Aliaa Amr Amoudi and Lana Adey AlShawwa in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205231212297 - Supplemental material for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia
Supplemental material, sj-pdf-2-mde-10.1177_23821205231212297 for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia by Aliaa Amr Amoudi and Lana Adey AlShawwa in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205231212297 - Supplemental material for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia
Supplemental material, sj-pdf-3-mde-10.1177_23821205231212297 for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia by Aliaa Amr Amoudi and Lana Adey AlShawwa in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-4-mde-10.1177_23821205231212297 - Supplemental material for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia
Supplemental material, sj-pdf-4-mde-10.1177_23821205231212297 for Factors Affecting Achieving Learning Outcomes in Basic Years in Medical School at King Abdul Aziz University, Jeddah, Saudi Arabia by Aliaa Amr Amoudi and Lana Adey AlShawwa in Journal of Medical Education and Curricular Development
Footnotes
Abbreviations
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Authors’ Contribution
LA conceptualized and designed the study, acquired, and interpreted the data, drafted the initial manuscript, revised the manuscript, and approved the final manuscript. AA contributed to the conceptualization of the study and revised and approved the final manuscript. All authors have read and approved the manuscript.
Availability of Data and Materials
Data available on request due to privacy restrictions.
Ethics Approval and Consent to Participate
This study was exempted from getting a formal ethical approval by the Biomedical Ethics Research Committee at the Faculty of Medicine, at King Abdul Aziz University reference # 25-21 on 14–12–2021. No verbal or written consent was obtained.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.