
Abstract
Objectives
This pilot study evaluated the feasibility of a live, interactive, synchronous, online, manualized intervention, Breath–Body–Mind Introductory Course (BBM-IC), for medical students. BBM-IC includes breathing, movement, and attention-focus techniques for stress management and better emotion regulation, energy, sleep, and mental focus.
Methods
Medical students attending a 2-h BBM demonstration were invited to participate in the 12-h BBM-IC and weekly 45-min 6-week group practice. Measures were obtained using Survey Monkey: patient health questionnaire (PHQ9), generalized anxiety disorder-7 (GAD-7), exercise-induced feeling inventory (EFI), sleep quality scale (SQS), and body perception questionnaire-short form (BPQ-SF) at pre-BBM-IC (T1), post-BBM-IC (T2), and 6 weeks post (T3). Perceived stress scale (PSS) and meditation practices questionnaire (MPQ) were measured at baseline (T1) only.
Results
Twelve medical students participated in BBM-IC 4-h daily for 3 days. Six attended practice sessions and completed 6-week post-tests. Mean scores comparison identified two variable sets with significant improvements: EFI tranquility (p < .005) and supradiaphragmatic reactivity (p < .040). Two measures reached near significance: SQS (p ≤ .060) and PHQ9 (p ≤ .078).
Conclusion
This pilot study provided preliminary evidence that BBM-IC may reduce stress and anxiety symptoms while improving mood, energy, mental focus, and other correlates of psychophysiological state in medical students. Taking time for self-care is challenging for medical students, as reflected in the small study enrollment. Designating time for BBM as a requirement within the medical curriculum would probably enable more students to participate and acquire skills to reduce the effects of stress on their physical and psychological health, as well as the health of their patients.
Introduction
Stress significantly impacts human psychophysiology, particularly when it is too intense or prolonged, or when it affects vulnerable individuals.1,2 High rates of psychological distress across the medical education continuum and later during professional life are well-documented. 3 − 9 The COVID-19 epidemic added significant stress to compound this situational stress.6,9 Such chronic, stressful conditions are associated with overactivity of the sympathetic nervous system and underactivity of the parasympathetic system, manifested by a more defensive psychophysiological state in which the individual may be afraid, angry, emotionally dysregulated, less flexible, hypervigilant, overreactive, and have reduced capacities for social engagement, empathy, connectedness, closeness, and bonding. 10
Studies presenting strategies for teaching mindfulness-based interventions can range from short online self-directed modules to courses and retreats. Numerous reports focus on medical students, attending physicians, or health professional groups. 11 − 16 Published studies provide evidence that the implementation of mind-body interventions has been effective at reducing medical student stress, depression, and anxiety, as well as improving self-awareness, emotional competence, and empathy. 17 − 22 For example, Karpowicz et al 17 describe the development of a mind-body medicine course for medical students and faculty that includes self-awareness, meditation, guided imagery, biofeedback, autogenic training, art, journal writing, and movement. The findings indicate that incorporating a course in mind-body medicine skills in medical school helps increase student empathy and mindfulness while reducing students’ perceived stress. Motz and colleagues 18 assessed the impact of a mind-body medicine skills course on several behavioral measures in first-year medical students. They found a significant decline in perceived stress among all participants. Furthermore, Williams et al 22 reported at another medical school that participation of first- and second-year medical students (N = 24, 3 cohorts over 2 years) in a mind-body medicine elective positively impacted medical student well-being, with noteworthy improvements in coping skills and perceived support, as well as decreased isolation. Romcevich et al 5 found that training pediatric residents in brief mind-body interventions, including mindfulness skills, was associated with improvement in burnout and stress.
Breath–Body–Mind™ (BBM) is a relatively simple, easy-to-practice, evidence-based, breath-centered mind-body program designed to rapidly reduce stress and anxiety and improve sympathovagal balance, stress reactivity, awareness, and social engagement. 23 BBM includes coherent or resonant breathing that can quickly and safely balance, strengthen, and increase the adaptive flexibility of the autonomic nervous system and other stress response systems, potentially counteracting the detrimental effects of excess stress. BBM techniques have been found to improve emotion regulation, mood, energy, sleep, anxiety, PTSD, physical health, and mental focus. 24 − 27
This study aimed to evaluate the effects of a live, interactive, synchronous, online, manualized intervention called Breath–Body–Mind Introductory Course (BBM-IC) on reducing the stress levels of medical students at San Juan Bautista School of Medicine (SJBSM) in Caguas, Puerto Rico, and assess the feasibility of offering this or a similar course on a regular basis to students in the future. We hypothesized that the medical students participating in this program would quickly gain the knowledge and skills to reduce stress and anxiety.
Methods
The study used a repeated measures design assessing the effects of the BBM training using pre-post comparison of dependent measures in a convenience sample along with the further impact of continued practice of the BBM skills for 6 weeks after the training ended. We obtained independent measures of perceived stress and prior experience with meditative practice before the workshop to understand better subject differences that might impact study results.
Recruitment, consent
On June 23, 2021, after the SJBSM Institutional Review Board approved the study (IRB-11-2021), participants were recruited for the 12-h BBM-IC program by first offering a 2-h BBM demonstration. Students were notified by email about the demonstration, which was delivered via Zoom by Drs. Brown, Gerbarg, and Braña during orientation week for the first-year SJBSM medical students (MS1). The BBM demonstration was also listed on their orientation schedule. Second-year medical students (MS2) were also invited by email to participate. After attending the demonstration, students interested in registering for the 12-h program completed Online Registration and Informed Consent forms via surveymonkey.com.
The consent form included a complete description of the background, purpose, and methodology of the pilot study, participant rights, data confidentiality/dissemination, and a description of possible risks, discomforts, and benefits of participation, along with contact information and whether they were MS1 or MS2 students. Students were asked to indicate their choice regarding participation in the study (ie, “yes,” “no,” or “not sure”). Electronic signatures were collected as evidence of their intentions. Those electing “yes” received an information packet via their student email, which included a link to a surveymonkey.com questionnaire to submit baseline data (see below). Further, those who selected “not sure” were sent information on whom to contact with questions about the study. Every effort was made to avoid coercing students to participate and to make it clear that participation in the program, the associated assessments, and their performance would not be linked to their academic success at SJBSM.
Intervention
12-h breath–body–mind introductory course
The 12-h BBM-IC consisted of three consecutive training days, 4 h each day (June 28–30, 2021). In addition, after completing the 12-h workshop, participants were asked to continue practicing the BBM exercises for 6 weeks. Standard ethical practices for student research were observed throughout the process. Participants completed a written informed consent authorization, after which they were assigned a participant identification code and were given a link to complete a baseline self-report questionnaire online before the BBM-IC started.
Participants attended a 12-h synchronous live online BBM-IC by Zoom for 4 h a day on three consecutive days taught by BBM leaders and two Assistant Certified Senior BBM Teachers (AST). The medical students were taught a set of manualized BBM techniques. Participants were observed and trained to a level of proficiency such that they could practice independently. The program included group processes and discussions to enhance learning, increase communication, and foster awareness of themselves and the other members of their group. In addition to whole group teaching, participants were assigned to small groups of 4 or 5 students with an AST to assess proficiency with each technique, whether they needed more instruction, and whether they showed any signs of emotional distress that required one-on-one support. Participants were encouraged to practice Coherent Breathing, gently breathing through the nose with equal duration of inhalation and exhalation at a rate of 5-breath cycles per minute, with the goal of 20 min practice per day.
Table 1 presents a description of the BBM-IC practices and sequences. Follow-up group practice sessions were offered on a voluntary basis for each of the following 6 weeks and conducted via Zoom by experienced BBM teachers. Each practice session lasted 45 min, and was scheduled in a time slot that was least likely to conflict with student classes. It used a previously validated online synchronous training format.28,29
Description of the BBM practices and sequences.

Assessments
Demographic data included medical school class (eg, first year, second year) and sex at birth. All questionnaires were administered online via surveymonkey.com, using a unique URL for the school. Participants received a unique identification code assigned and maintained by BBM researchers who managed the course registration by a process independent of the school's administration. Only the deidentified summary analysis of the data was shared with members of the SJBSM faculty and administration.
Test measures
The baseline assessment (T1) included the independent measures, that is, meditation practices questionnaire (MPQ) and perceived stress scale (PSS), as well as the dependent measures: generalized anxiety disorder-7 (GAD-7), patient health questionnaire (PHQ-9), exercise-induced feeling inventory (EFI), sleep quality scale (SQS), and body perception questionnaire-short form (BPQ-SF). All the dependent measures were retaken post-BBM-IC (T2) and 6 weeks post-BBM-IC (T3).
MPQ was used to assess the effects of previous experience with practices that are similar to the BBM exercises.
30
PSS10 is a widely used 10-item self-report rating scale soliciting how often a participant experienced stress-related feelings and thoughts in the past month. Cohen and Williamson (1988) report the PSS-10 demonstrates adequate internal consistency (α = .78) and moderate concurrent validity with the amount of stress experienced during an average week (r = .39, p < .001) and a range of other self-report behavioral criteria. Scores ranging from 0 to 13 would be considered low stress, 14 to 26 moderate stress, and 27 to 40 high stress.31−33 GAD-7 is used to assess baseline levels of generalized anxiety disorder and the changes resulting from interventions using self-report data.
34
GAD-7 has excellent internal consistency (Cronbach α = .92) and good test-retest reliability (intraclass correlation = .83).
35
PHQ-9, a self-administered version of the PRIME-MD diagnostic instrument for common mental disorders, assesses baseline levels of depression and the changes resulting from interventions using self-report data.
36
Kroenke et al also report internal consistency ranging from α = .86 to .89 among different samples (p .608). A study of the “Operational Characteristics” at various PHQ-9 cutoff points demonstrated useful sensitivity, specificity, and likelihood levels for predicting major depression (p .609). EFI has four subscales: positive engagement, revitalization, tranquility, and physical exhaustion. Measures of internal consistency vary among the subscales (ranging from α = .72 to .91).
37
Data support construct validity through correlational studies with measures of depression, self-efficacy, and well-being.
38
SQS is a self-report, one-item 7-point rating, whose reliability and validity are supported by studies of insomnia patients demonstrating strong concurrent criterion validity (convergent, divergent, and known-groups) and adequate test-retest reliability.
39
BPQ-SF, a self-report measure, uses a Likert scale (never, occasionally, sometimes, usually, always) on three subscales: body awareness (26 items), supradiaphragmatic autonomic reactivity (15 items), and subdiaphragmatic autonomic reactivity (5 items). Subscales showed strong internal consistency, test-retest reliability, and convergence with various validation measures.
40
Statistical analysis
The IBM SPSS Statistics (SPSS) 27.0 was used to generate frequency data for each variable and to calculate paired sample t-tests. A time-series analysis was performed for T1, T2, and T3 measurements using analysis of covariance (ANCOVA) with the baseline perceived stress scale (PSS) scores as the covariate.
Results
Of 126 medical students, 75 (55 MS1 and 20 MS2) participated on June 23, 2021, in the 2-h BBM demonstration during orientation week. All 75 students were invited to participate in the 12-h BBM-IC. Fifteen registered to attend, including 12 MS1 and 3 MS2, of whom 13 (7 women and 6 men) signed the Informed Consent Form. Of the 13 students who signed Informed Consent Forms, 12 completed the Pretest questionnaires at baseline before participating in the BBM-IC (T1).
Baseline measures for perceived stress (T1)
The participants included 10 first-year and 2 second-year medical students. PSS baseline scores revealed that 11 of the 12 students (92%) were experiencing “Moderate” perceived stress, and one reported having “High” perceived stress before starting the BBM-IC. PHQ-9 scores indicated that 2 of the 12 (16.6%) were “Moderately Depressed,” and another 2 were experiencing “Moderately Severe” depression. One of the 12 students (8.3%) fell into the “Severe” anxiety category; one (8.3%) showed “Moderate” anxiety, and the remaining 10 (83.3%) registered “None to Mild” anxiety.
Pretest–posttest paired comparisons
A paired-comparison t-test of the pretest (T1) and posttest (T2) means for the 10 dependent variables (Table 2) revealed a statistically significant increase in the EFI Tranquility Scale (t = -3.609, p = .005), and a decrease in supra-diaphragmatic reactivity (t = 2.352, p = .040). Improvements in sleep quality, depression, and anxiety approached significance but did not achieve the p = .05 criterion level. As indicated in Table 3
Pairwise comparison of pre- and post-test means for all dependent variables

*p < .05.
**p < .01.
Paired sample effect sizes for pretest and posttest means.

aStandardizer is the denominator used in estimating the effect sizes.
Cohen's d uses the sample standard deviation of the mean difference adjusted by the correlation between measures.
Time series analysis and progression
Six of the initial 12 students completed questionnaires 6 weeks after finishing the BBM-IC course (T3). This participation allowed us to perform a time series covariance (ANCOVA) analysis across the 10 sets of dependent measures. Estimated marginal means were computed for all ten dependent variables at the three time periods (pretest-T1, posttest-T2, and 6-week follow-up-T3). These results are illustrated as line graphs in Figure 1a (EFI), 1b (GAD-7 and PHQ-9), and 1c (BPQ). The baseline values for PSS were used as the covariate. Within-subject comparisons showed statistically significant improvements in the GAD7 scores from T1 to T3 (p = .029) and the PHQ-9 from T1 to T3 (p = .031), as per Table 4.
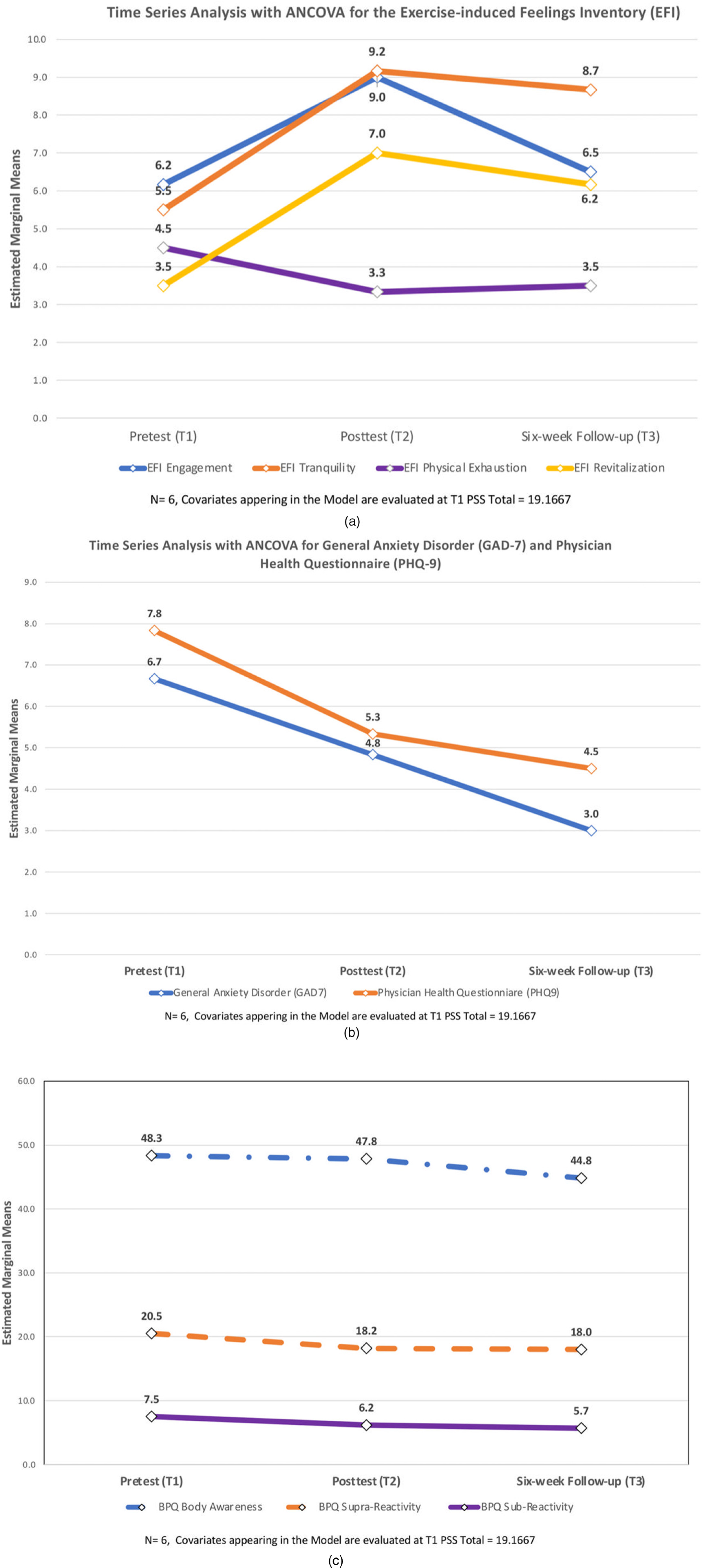
(a) EFI time series. (b) GAD and PHQ9 time series. (c) BPQ time series.
ANCOVA of 10 Dependent Variables with Baseline PSS scores As Covariate (N = 6)

*The mean difference is significant at the .05 level. b. Adjustment for multiple comparisons: Bonferroni.
Based on estimated marginal means.
Discussion
Multiple studies have shown that mindfulness-based interventions and mind-body practices are beneficial for reducing stress, depression, and anxiety in medical students and students of other healthcare professions. 11 − 22 Worldwide, there is interest in studying these effects, particularly for stress management programs that enable medical students and physicians to rapidly relieve stress and enhance performance while studying and working. 42 − 46 Interventions that rely on cognitive methods occupy the thought processes; meditative practices induce a calm but less alert, less task-oriented state. In contrast, BBM techniques induce a unique state of calmness with mental alertness. For example, coherent breathing, which entails breathing gently through the nose with an equal duration for the inhalation and the exhalation, can be done with eyes open while studying, taking tests, and engaging in clinical work.10,23− 26
BBM-IC has been shown to significantly reduce stress, anxiety, depression, and symptoms of PTSD while improving mental focus. 23 −29,47,48 In this pilot feasibility study, the participating medical students had elevated stress and anxiety levels at baseline. Within subject comparisons of the effect of time before and after the BBM-IC showed improvements in mean scores on all 10 test variables. Despite the small number of participants, statistically significant improvements occurred on the EFI tranquility subscale, and in BPQ-supradiaphragmatic reactivity indicating positive changes in autonomic reactivity. Improvements in sleep quality, depression, and anxiety approached significance.
The results of the current study of medical students at SJBSM are consistent with what has been demonstrated in previous studies of BBM programs for healthcare providers under stress, such as following the 2010 Deepwater Gulf Horizon oil spill and during the COVID-19 epidemic among staff of the Regional Integrated Support for Education of Northern Ireland.26,44,45
One strength of this SJBSM study was that the evidence-based, manualized BBM-IC was designed and taught by experienced BBM teachers. The use of live online synchronous training enabled the BBM team, located in several U.S. states, to train medical students in Puerto Rico. Also, the use of Survey Monkey and the coding of participants made the study de facto confidential. Furthermore, the participants were carefully monitored, and no adverse effects were reported. All of the participants reported improvements in multiple indicators of psychophysiological states.
The study's limitations were the small size of the participant group, the difficulty of getting some participants to complete test measures, and the lack of a control group (a consequence of the small number of enrollees). ANCOVA suggested that the small number of participants attenuated the power of the tests to achieve significance. Despite the small number of students, statistically significant improvements were documented, a testament to the high impact of the program. Similar studies with pediatric residents have observed these limitations and strengths when participation is voluntary. 5
It is likely that, in general, medical students, although they recognize their need for stress reduction, prioritize academic studies at the expense of their health, self-care, and time to develop greater stress resilience. For BBM to be feasible in medical school settings and to achieve the desired results, it may be necessary for medical school curriculum committees to designate specific times for training that do not compete with academic requirements and/or to integrate BBM into the regular curriculum.
Conclusions
This pilot study provided preliminary evidence that BBM-IC may reduce stress and anxiety symptoms while improving mood, energy, mental focus, and other correlates of psychophysiological state in medical students. Taking the time for self-care is challenging for medical students, as reflected in the small voluntary enrollment in this study. Designating time for BBM practices as part of the regular curriculum would likely enable more students to participate and acquire the necessary skills to reduce the effects of stress on their own physical and psychological health. Subsequently, these future physicians could better maintain their well-being over years of stressful work. Furthermore, they could learn how to integrate the mind-body practice skills acquired in BBM into patient care to enhance outcomes.
Footnotes
Acknowledgements
The authors thank Dr Yocasta Brugal, President and Dean of the San Juan Bautista School of Medicine, for her trust and support in carrying out this research pilot project and integrating the BBM program into Orientation Week. They also appreciate the support and assistance received from: Dr Yolanda Miranda, Associate Dean of Students Affairs; Dr Yaritza Inostroza, Associate Dean of Biomedical Sciences; Dr Shirley Valentín, First Year Curriculum Coordinator; Dr Sandra Chinapen, Second Year Curriculum Coordinator and Ms. Ilsa Centeno, Counselor.
Declaration of Conflicting Interest
Richard P. Brown, MD, and Patricia L. Gerbarg, MD, receive financial remuneration for teaching some Breath–Body–Mind Programs. Dr Brown and Dr Gerbarg serve on the Board of the Breath–Body–Mind Foundation, Inc., a not-for-profit 501(c)3. They received grants from NIH research studies on the effects of yoga and breath practices on Major Depression and thalamic GABA levels; The Mississippi Dept. of Mental Health for research on the effects of BBM train-the-trainer program on healthcare providers serving populations affected by the Gulf Horizon oil spill; START Clinic Toronto, Canada, for the study of the BBM-IC on patients with treatment-resistant Generalized Anxiety Disorders and comorbidities; Weill Cornell Medical College Jill Roberts IBD Center, The Jill Roberts IBD Center Patient Support Fund, and the Weill Cornell Medical College Griffis Faculty Club for a study of the effects of BBM on physical and psychological symptoms of inflammatory bowel disease.
Funding
This study was funded by a San Juan Bautista School of Medicine grant and a matching grant from The Breath–Body–Mind Foundation, a 501(c)(3) not-for-profit.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.