
Abstract
Objectives
Morning Report is a prevalent classroom learning activity in residency programs. Yet, its contribution to resident education remains unclear. Our objective was to explore pediatric residents’ perceptions of the purpose of Morning Report as well as their experiences at Morning Report both as learners and resident presenters.
Methods
We performed a qualitative study with a grounded theory approach using semi-structured focus groups of pediatric residents (November 2016-July 2017) from a large academic health center. We analyzed data with the constant comparative method, generating codes using an iterative approach and collecting data until reaching saturation. We identified major themes and resolved disagreements by consensus.
Results
Twenty-six residents participated in five focus groups. Data analysis yielded four themes: Morning Report is Multipurpose, Socialization and Engagement Influence the Learning Environment, Potential for Emotional Discomfort, and Barriers to Prioritizing Morning Report Attendance. Residents felt the primary purpose of Morning Report was acquiring medical knowledge, but also acknowledged Morning Report's added benefits of providing an opportunity for socialization and a mental reprieve before work rounds. Residents felt Morning Report was educational when engaged in interactive discussion; however, it was challenging to meet the differing needs in this mixed learner level format. Some resident learners were hesitant to participate due to fears of being judged, and some resident presenters perceived a need to be topic experts. Clinical responsibilities and exhaustion following busy service rotations often precluded Morning Report attendance.
Conclusion
Pediatric residents described numerous purposes of Morning Report, including opportunities for valuable learning. Self-perceived learning was positively influenced by engagement and a sense of connection and challenged by emotional discomfort at times. Future work can explore how to best promote engagement and foster a safe learning environment.
Introduction
Morning Report, a case-based conference in which learners and faculty interact to discuss patient care, has been a traditional and prevalent activity in graduate medical education (GME).1,2 Morning Report has varied purposes, 2 although education is most frequently cited. 1 Educational conferences occupy significant time in GME, 3 and the Accreditation Council for Graduate Medical Education (ACGME) requires that residency programs provide regularly scheduled didactic sessions. 4
However, medical educators continue to debate the value of scheduled didactics versus experiential learning. 5 Situated learning theorizes that learning occurs by performing authentic activity (eg, caring for real patients),6,7 and residents may miss valuable patient care experiences by leaving the workplace to attend conferences. 8 Studies describing the contribution of resident conferences to knowledge acquisition report conflicting results.9–14 Additional evaluation of the educational value of conferences in a workplace-based training environment is needed in an era in which duty hour restrictions and high clinical workload impede conference attendance and learner participation,15–17 and more recently, during a pandemic that has forced medical educators to reconsider how curricula are delivered.
Two systematic reviews found Morning Report has heterogeneous purposes, methods, and settings with difficult to measure outcomes.1,2 Thus, despite its prevalence, the contribution of Morning Report to resident education is ill-defined. Morning Report typically differs from other educational conferences in that it is anchored on the care of real patients; thus, we chose situated learning as a conceptual framework to inform our study.6,7 A better understanding of the value of Morning Report will benefit educators tasked with developing effective and efficient curricular strategies in the current health care environment. The aim of our qualitative study was to explore pediatric residents’ perceptions of the purpose of Morning Report as well as their experiences at Morning Report both as learners and resident presenters.
Methods
Study design
We conducted a qualitative study (Figure 1) using focus groups of University of Colorado pediatric residents at a large academic health center (COREQ checklist, 18 Supplementary File). We chose qualitative methodology because it is well suited to answer questions about complex learning environments, 19 and employed a grounded theory approach, which is appropriate for situations in which the research question involves social interactions. 20 Three investigators (LL, JW, MT) were Chief Residents. One investigator (BS) was a pediatric hospitalist and associate pediatric residency program director with experience conducting qualitative research. Participants provided verbal consent (by agreement to participate in focus groups), and the Colorado Multiple Institutional Review Board approved the study protocol (#16-1693) on October 7, 2016.

Qualitative study flow diagram.
Setting
Our Pediatric Residency Program, consisting of 103 learners across three institutions, holds Morning Report in a hospital conference room every weekday from 7:30 to 8:00 AM, with video conferencing to ambulatory and off-site locations. Attendees include residents, students, fellows, and faculty. A senior resident (postgraduate level 2 or 3) presents a self-selected case, and a Chief Resident facilitates the discussion. Fellow and faculty are expected to help answer questions and provide teaching pearls. The format of our Morning Report is similar to the structure employed by other programs—it involves a case-based conference between learners and teachers. 2
Sampling strategy
Pediatric residents who attended at least one Morning Report were eligible for study inclusion. Investigators recruited residents by email to participate in focus groups. Residents were sampled as two groups—interns and senior residents—to account for likely differences in their Morning Report experiences. Residents were sampled over several months of the academic year to allow for multiple Morning Report experiences and varied clinical contexts. Sampling continued until we reached thematic saturation—the point at which ongoing analysis did not provide any new insights relevant to emergent theory.20,21
Data collection
We developed a semi-structured focus group guide (Table 1) based on our study aim, our personal prior experiences at Morning Report, and from review of the literature. As the study progressed, questions were iteratively added to the focus group guide to further explore resident comments with subsequent participants. Two chief resident investigators (LL, JW) conducted five focus groups from November 2016 to July 2017. Each focus group consisted of 4-7 residents and lasted approximately one hour. Two focus groups consisted of interns only, two of senior residents only (postgraduate year 2 or 3), and one was a mix of interns and senior residents. Data were audio recorded, transcribed verbatim, and de-identified. Residents completed a demographic data sheet.
Semi-structured focus group guide.
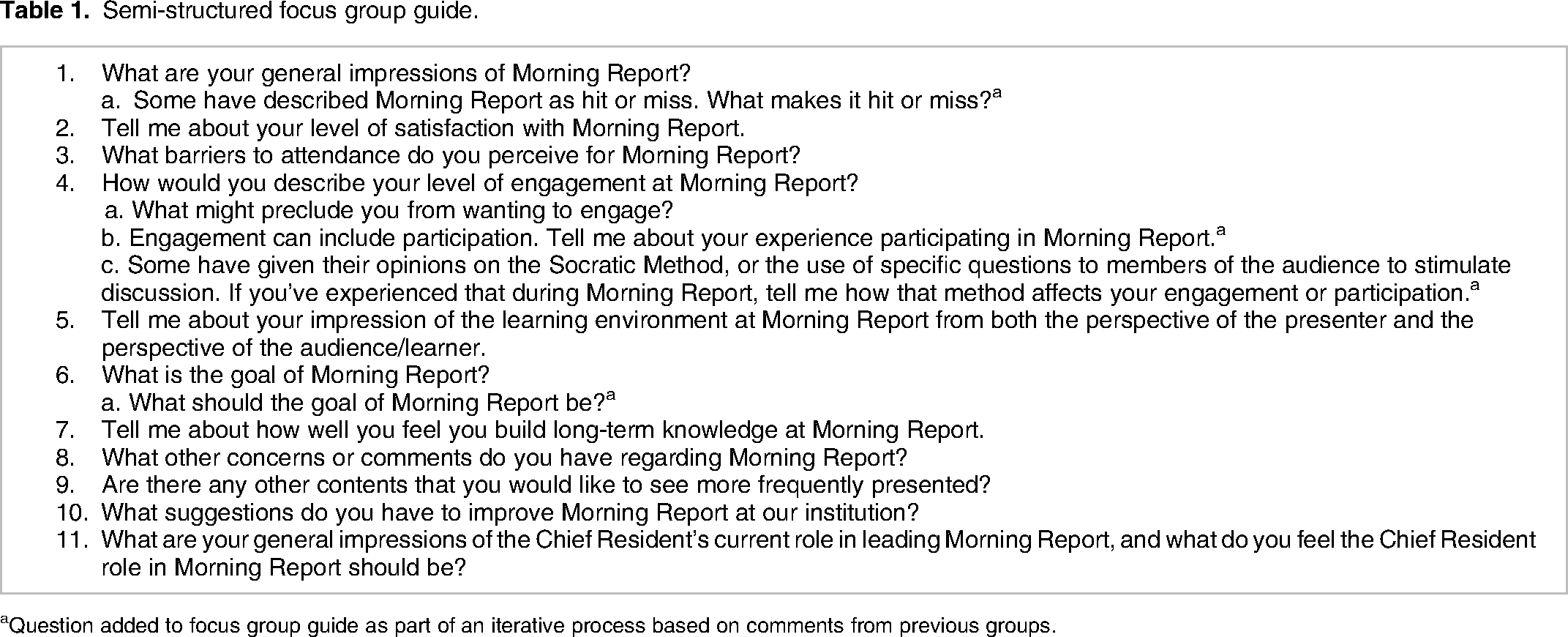
Question added to focus group guide as part of an iterative process based on comments from previous groups.
Data analysis
In accordance with qualitative methodology, we analyzed the data using the constant comparative method.20,21 Following transcription of the fourth focus group, each investigator individually read through and began coding transcripts. Lists of codes were compared and a coding scheme was agreed upon as a group. Emerging themes were further explored with the fifth focus group. Three investigators then returned to the data and applied the coding scheme to all transcripts, comparing codes in mixed pairs (LL/JW, LL/BS, JW/BS) through an iterative approach in which initial codes were modified and others added to best reflect data content. Consistency across pairs was achieved by including one investigator from previous pairs into the new pair, and discrepancies were resolved through discussion among the three investigators. Codes were then organized into categories describing themes. HyperRESEARCH (Boston, MA) was used to organize the data and facilitate the construction of thematic summaries. In the final analysis, a conceptual model was created to describe relationships between the themes. Throughout the study, the authors examined their own reflexivity as chief residents and program leaders, acknowledging how the potential for personal biases and relationships with the study participants could influence the study.22,23 Trustworthiness of findings was established by having multiple researchers participate in data analysis, peer debriefing, and member-checking, in which we discussed themes and the accuracy of our interpretations with a subset of study participants (convenience sample, n = 5). 19
Results
Twenty-six out of 103 (25%) residents (10 interns, 16 senior residents) participated in five focus groups. All senior residents had presented at Morning Report at least once. Most participants (73%) attended Morning Report 2-3 times per week. Analysis yielded four themes: Morning Report is Multipurpose, Socialization and Engagement Influence the Learning Environment, Potential for Emotional Discomfort, and Barriers to Prioritizing Morning Report Attendance. Themes with representative quotations are presented in text and in Table 2.
Themes with illustrative quotations.

Morning report is multipurpose
Residents felt the primary purpose of Morning Report was knowledge acquisition and development of clinical skills to be used during and after training and to become competent general pediatricians. If you are alone in Wyoming, and you have someone who comes in with vaginal bleeding, it would be nice to [know] I would have a way to survive that situation.
Interns and senior residents felt Morning Report should focus on clinical reasoning. Senior residents felt discussing patient history was beneficial when they were interns; however, as senior residents, they became frustrated when too much Morning Report time was spent determining what questions to ask on history or what findings to look for on physical examination as they preferred to focus on the acute management of patients. As an intern it was really nice to think about what questions would you ask the patient. As time goes on, I know what I would ask. I don’t need to spend 20 min figuring out what I’d ask the patient. (Senior resident)
Morning Report also provided opportunities to learn how to collaborate and communicate with interdisciplinary team members to care for patients. We have a group of people from different fields in the same room focused on one thing. We have the opportunity to learn through collaboration and how to communicate with each other from different fields on a case.
Residents felt Morning Report provided opportunities to practice and develop teaching, public speaking, and case-presentation skills. It is good for our professional learning to get used to presenting in front of a group.
In some instances, residents utilized Morning Report for the purpose of decompression before rounds without a focus on learning. You were already feeling tired and stressed and this is finally my time where I can breathe and sit down, have coffee, and not think for 10 min before we start rounds.
Socialization and engagement influence the learning environment
Residents described how socialization at Morning Report affected the learning environment. There is a social aspect. The learning environment is better the more people that are there. More of my friends and my peers and my co-PL-2 s.
However, for some residents, it was a greater challenge to socially connect when they started the year at an off-campus site and had not yet gotten to know Morning Report attendees (faculty, fellows, peers). I started intern year [at another site]. When I came here to Morning Report, not knowing other people, that sense of camaraderie was not there for me. All these people have been here, and I’ve never participated. I don’t know 90% of these people sitting in the room.
In addition, residents described a learning environment in which limited interaction occurred. It was like pulling teeth to get people to engage. (Senior Resident Presenter)
The learning environment was significantly influenced by faculty and fellows who provided teaching pearls and answered questions. The presence of many faculty and fellows from diverse specialties supported resident learning; however, their attendance was inconsistent. It's really a unique learning opportunity. You have a nice collection of experts who throw out learning pearls. At its best, it can be my favorite type of learning. Because it is engaging.
The mixed learner level format that included students, interns, and senior residents resulted in educational challenges. Interns often hesitated to speak in the presence of senior residents or were still mentally processing information when senior residents answered questions. Additionally, senior residents complained about topics that were too repetitive or lacking. Students would say the material was too over their head. Interns really liked it. For second and third year [residents] it was like I’ve heard this before. (Senior Resident)
Finally, residents described how preoccupation with upcoming clinical duties negatively impacted their ability to engage with Morning Report. It is hard for me to pay attention when I am thinking about all the other things I have to do. Especially when it is a stressful situation like rounding coming up. (Intern)
Potential for emotional discomfort
Several residents described how Morning Report felt intimidating. They feared incorrectly answering a question in front of attending physicians and others. They described feeling anxious about the possibility of getting individually questioned in front of the group. The ideal environment would be everyone is very comfortable speaking up even if they are totally wrong. It is OK and you talk about why and move on. But there is a fear of not getting the right answer. (Senior Resident) You can just be sitting there and feel attacked. That only adds to the anxiety. (Intern)
Resident presenters described a self-perceived expectation to be the topic expert, feeling isolated and alone in front of the room, and uncomfortable being able to ask questions for their own learning. I don’t feel I’m in a position as the presenter to ask a question. I’m not going to ask a question I don’t know the answer to. [It] would be great to say this came up and I don’t know the answer, what do you guys think? (Senior Resident)
Barriers to prioritizing morning report attendance
Residents felt that clinical responsibilities often precluded Morning Report attendance. On inpatient wards, timing of patient handoffs and pre-rounding made it difficult to get to Morning Report on time. I went zero times when I was [ward] senior. Because sign out is at 7:00 and I have to pre-round on my patients. I just never saw how it was possible. (Senior resident)
There were times when I was just really, really exhausted coming off really hard rotations. I didn't go [to Morning Report] and I didn’t feel bad about it. I need to recover, and I need to sleep in. (Intern)
The potential for a suboptimal learning experience from lack of interactive discussion, repetitive topics, and concern for educational safety detracted from attending Morning Report. I think coming up with a safer environment and [ensuring] discussion will help with getting people excited to go to morning report and not sit through a lecture where you have seen the same document, in the same font, every day.
Discussion
Pediatric residents described Morning Report as an educational activity whose primary purpose was the acquisition of medical knowledge to care for patients both during and following completion of residency. A secondary goal was to develop case presentation and teaching skills. Residents described how engagement in interactive discussion among a diverse group of resident peers, fellows, and faculty optimized their learning at Morning Report. However, inconsistent faculty/fellow presence, an occasionally intimidating learning environment, mixed learner format, resident attendance barriers, and varied resident presenter facilitation skills resulted in contrasting perceptions of resident learning.
Our study adds to the existing literature by highlighting how the social aspect of Morning Report promotes self-perceived learning. Findings from our study align with a communities of practice framework, in which learning is a social activity situated in the community. 24 A community of practice is defined as a “persistent, sustaining social network of individuals who share and develop an overlapping knowledge base, set of beliefs, values, history, and experiences focused on a common practice.” 24 Three key elements characterize a community of practice: domain (prevention and treatment of human disease), practice (knowledge and skills the community shares and develops), and community (members who interact and learn together).24,25
Through the lens of a community of practice framework, the primary goal of Morning Report is to help residents competently care for patients (domain); knowledge needed for patient care is shared and skills developed (practice); and attendees interact and learn together (community). The effectiveness of the community as a learning system depends on the strength of all three components. 25 Our study's findings illustrate how resident-perceived learning at Morning Report occurs when a community of practice is successfully created. However, barriers to attendance and feelings of emotional discomfort are prevalent factors that impede the ability to form a community of practice. Figure 2 depicts the themes and their relationships, identified in our study, that illustrate how a community of practice framework provides a theoretical basis for learning at Morning Report.

Conceptual model of morning report as a community of practice. Self-perceived learning at Morning Report can be fostered when a community of practice is created but is challenged by attendance barriers and the potential for emotional discomfort.
As a conceptual framework, communities of practice have been proposed to serve as the comprehensive foundational theory for medical education. 24 Yet, literature describing the use of communities of practice framework to guide curricular development in medical education is scarce. 26 Using communities of practice as a foundational theory does not exclude the role of other learning theories as they can provide the theoretical basis for curricular interventions within the community. 24 Evidence-based guidelines for creating a community of practice are needed. Published recommendations include actively engaging learners to join the community; emphasizing role modeling and mentoring; charting progress toward full membership within the community; and creating a learning environment that is respectful, welcoming, and supportive. 24
However, creating a welcoming and supportive learning environment remains a challenge. A previous study found that Morning Report was anxiety-provoking and described as a fearful place that prevented effective learning. 27 The potential for residents to feel emotional discomfort at Morning Report raises concern that many residents may not feel psychologically safe in this learning environment. Psychological safety is the perception that a workplace training environment is safe for learners to express concerns, ask questions, and acknowledge mistakes without fear of humiliation or blame. 28 Some resident learners in our study described an intimidating educational climate in which they worried about answering incorrectly or feared judgment, which detracted from robust discussions and inhibited their engagement and perceived learning. Resident feelings of being judged in the presence of peers and faculty align with a performance-oriented climate in which learners are concerned about the appearance of competence and are likely to hide their uncertainty and avoid feedback out of fear of negative consequences. 29 Fostering psychological safety in medical education shifts the emphasis from evaluation to professional growth and skill-building. 28 A safe climate for group learning has been identified as a crucial element for effective Morning Report facilitation. 30 Still, further work is needed to improve emotional comfort and foster psychological safety to successfully create a community of practice and optimize potential for learning. Additional challenges for medical educators are how to create a Morning Report community of practice for residents in the current health care era of high workload for both residents and faculty, duty hour restrictions, and more recently a pandemic that has limited in-person educational activities.
Our study's findings may have broad implications for medical education. We show how a communities of practice foundational framework promotes learning at a Morning Report educational conference. Additionally, our study illustrates the necessary integration of other learning theories (situated learning at Morning Report to discuss patient care) within this foundational framework. We speculate that this curricular approach would likely apply to other venues in undergraduate and graduate medical education and include classroom and clinical (joining an inpatient health care team) settings. Further work is needed to identify strategies that foster a community of practice while mitigating the barriers that impede its development.
This study has several limitations. Study participants were residents from a single residency program at a large academic children's hospital and findings may not be transferable to other types of institutions/programs. Residents with high or low levels of satisfaction with Morning Report may have been more likely to participate introducing bias into our study. Some participants may have attended few Morning Reports and it is possible comments may have differed with additional Morning Report experiences.
Conclusions
Pediatric residents described opportunities for valuable learning at Morning Report when they were effectively drawn into its community of practice. Interactive discussions foster self-perceived learning but can be challenged by a lack of psychological safety. Future work can explore how best to mitigate the challenges that preclude the cultivation of this community to optimize resident learning.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231211467 - Supplemental material for A Qualitative Study of Pediatric Residents’ Experiences at Morning Report
Supplemental material, sj-docx-1-mde-10.1177_23821205231211467 for A Qualitative Study of Pediatric Residents’ Experiences at Morning Report by Laura Z. Lockwood, Joshua T. B. Williams and Melisa Tanverdi, L. Barry Seltz in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We thank the University of Colorado, Department of Pediatrics Office of Medical Education for the funding provided for this study. We thank Sheilah Jimenez (program research assistant) for her review of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Provided by the University of Colorado, Department of Pediatrics Office of Medical Education. The funding source did not have any role in study design, collection, analysis, interpretation of data, the writing of the manuscript, or the decision to submit the manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.