
Abstract
OBJECTIVES
Most teaching activities pivoted to virtual during COVID-19. Demanding schedules necessitated brief, asynchronous, and widely disseminated professional development to encourage connection and reinforce educator identity. We created and disseminated micro virtual asynchronous educator development while engaging educators from interprofessional backgrounds to co-create teaching tips. We undertook educational evaluation to understand the impact of our educational initiative, measured along 2 professional development dimensions offering contexts for learning—the individual or independent experience, and the group or collective experience—which served as an organizing framework from which to interpret our results.
METHODS
Between June 2020 and July 2021, 74 educators at our institution were asked to participate in our “One Minute Teaching Tips” initiative by providing a brief tip or pearl. Each tip was edited, prepared as a high-quality infographic, and shared via: (1) website; (2) digital monitors; (3) newsletter; and (4) Twitter (now X). Quantitative metrics measuring website and Twitter engagement were analyzed descriptively and to determine distinctions among key variables. Participants answered a brief survey and directed content analysis was utilized to analyze the open-ended responses.
RESULTS
Fifty educators (67.5%) participated. Among those, 45 (90%) completed the survey. Tips were accessed via website 1447 times, averaging 28.9/week. The average tweet garnered 43.2 engagements. Six categories aligned with the individual dimension: participants engaged meaningfully, considered prior experience, relied on educational principles, focused on interest or passion, reflected on teaching practices, and experienced reinforced professional identity. Six categories aligned with the collective dimension: participants felt the initiative supported institutional need, was visible to the community, encouraged engagement with other tips, supported inclusive participation, brought value within the community, and showcased education.
CONCLUSION
Our initiative aligns with a contemporary understanding of professional development and was impactful along individual and collective dimensions. Similar initiatives could be developed in alignment with accreditation requirements.
Keywords
Introduction
A majority of teaching and learning activities pivoted to the virtual space during the COVID-19 pandemic, limiting the ability to provide face-to-face, synchronous teaching, and professional development to busy clinicians and trainees. 1 Demanding and rapidly evolving clinical and teaching schedules further challenged the ability of faculty, staff, and trainees to seek professional development, even among those who desire to strengthen their skills as educators.2,3 Even prepandemic, educators and clinicians have found it challenging to prioritize their own professional development, in part due to time constraints and competing demands.4,5 This lack of connection to a larger education community can hinder knowledge sharing and collaboration and challenge perceptions of self as an educator. 6 As professional identity formation is influenced by engagement with community, lack of connection may stifle educators’ ability to adequately develop and further integrate their professional identity. 7 Notably, there is a considerable body of literature that has long noted that professional development is often received informally during the course of professional duties, ideally as part of a workplace community.6,8 This authentic workplace learning can support performance and has been important long before the COVID-19 pandemic. 8
Time-intensive professional development activities such as synchronous seminars or asynchronous videos can be impactful for those who attend, but require a reasonable time commitment as well as activation energy to participate.5,9 Moreover, many formerly in-person events transitioned to the virtual setting, leading to a noted “Zoom fatigue.” 2 Professional development initiatives that are brief, purposefully designed, and easily delivered have the potential to reinforce professional identity, support feelings of community, and reinvigorate educators. Microsized, bite-sized, or just-enough-information approaches are an emerging trend in continuing education.10,11 While no standard definition exists, these approaches champion small lesson modules or short-term activities intended to teach or reinforce course objectives and are a means of facilitating participant learning, training, or continuing education.3,11 These approaches are intended to emphasize creativity, flexibility, and ability of learners and supports self-direction and self-determination. 11 When developed asynchronously, it allows the participant to determine how and when they want to engage with the modules or activities.3,10,11 Indeed, time-efficient, asynchronous delivery can make participation easier for busy clinicians.3,10,12 Moreover, pivots to asynchronous professional development opportunities which incorporate social media to encourage sharing and reflection can help support health professions educators while connecting them to a larger virtual community.3,10,13
To address these challenges, the Brigham Education Institute 14 developed an initiative to engage health professions educators in the creation and dissemination of micro virtual asynchronous educator development content during COVID-19. This content was shared with faculty, staff, and trainees throughout our institution and broadly through Twitter (now X). We engaged these health professions educators from interprofessional backgrounds in the co-creation of teaching tips, intended to showcase our community of educators while also highlighting the importance of the educational mission at a challenging clinical time.
Methods
Setting and participants
Between June 2020 and July 2021, 74 physician, nursing, and interprofessional education leaders at the Brigham and Women's Hospital in Boston, Massachusetts were contacted via email up to 3 times to request participation in the Brigham Education Institute “One Minute Teaching Tips” initiative. 15 We intentionally requested participation from a diverse group of interprofessional educators representing multiple disciplines and clinical specialties, ranging from trainees to senior leaders. Inclusion criteria included being known to institute leadership for having an education leadership role, serving on educational committees, engaging with our institute, or general work and involvement as an educator at our institution. While there was no specific exclusion criteria, preference was given to those having an active Twitter account. Our intention was to recruit enough participants to create and disseminate our micro virtual asynchronous educator development for approximately 1 academic year. Each participant provided their best teaching tip or pearl, intended to be read in between 30 and 60 seconds, as well as their professional photo. This information was utilized to create the micro virtual asynchronous educator development content.
Initiative
A graphic designer created a series of 5 infographic templates in complementary colors, establishing a theme, focusing on simplicity and clarity, and branding each infographic as part of the larger initiative. 16 Ten interchangeable icons—representing broad concepts such as clinical, surgical, or online teaching, research, or evaluation and assessment—were created to represent core educational concepts. Infographics were high-resolution and had an aspect ratio appropriate for Twitter as well as for widescreen monitors. 16 Each infographic included a QR code linking to the initiative's website. Figure 1 displays an exemplar.
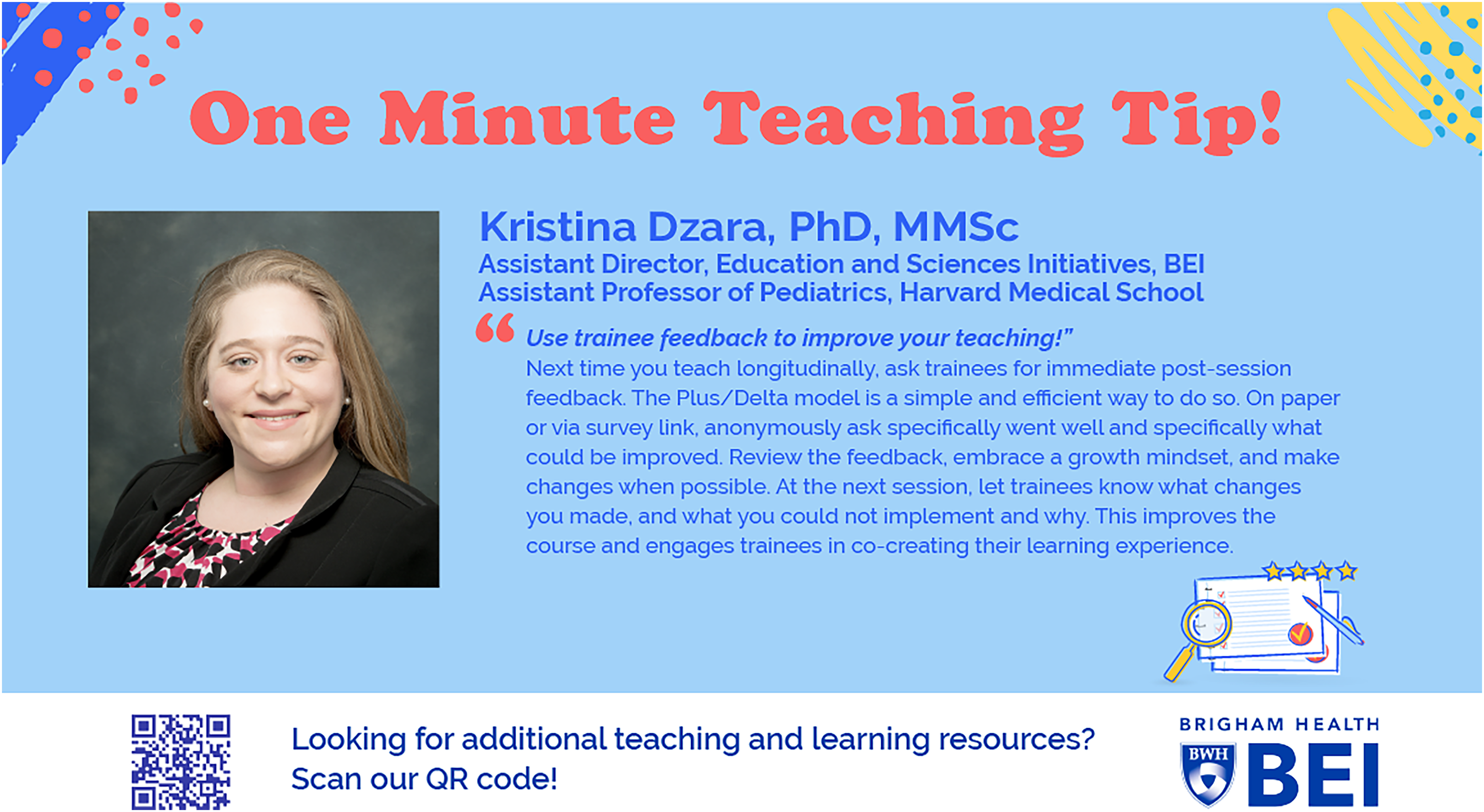
Exemplar “One Minute Teaching Tips” infographic.
Topics were identified by participants, who also provided draft tip text. Tips were then edited by the first author (KD) to ensure they aligned with evidence-informed teaching and learning practices, as well as for clarity, coherence, and grammar. No 2 tips were exactly the same. The text and professional photo were placed by the graphic designer into the template, and the relevant interchangeable icon applied. All participants reviewed their infographic and were provided the opportunity to provide formative feedback or edits, which were incorporated prior to finalization. Tips were aligned with a high-quality resource for additional self-directed learning. All participants were provided the opportunity to select the resource aligning with their tip; not all chose to and resources for those tips were selected by the first author.
Each participant's “One Minute Teaching Tip” infographic was publicly disseminated for 1 week in the following ways, all of which were alignment with current Institute communication strategies: (1) collated on our Brigham Education Institute website 15 ; (2) displayed on the Brigham and Women's Hospital digital monitors with changing displays spotlighting news, events, and opportunities throughout the hospital multiple times per day; (3) included in our Brigham Education Institute newsletter; and (4) shared from our highly active Brigham Education Institute Twitter account twice in 1 week. 17 Participants with a Twitter handle were tagged in each tweet and encouraged to have program, department, or institution Twitter handles retweet it.
Educational evaluation
Routine educational evaluation is the methodology we used. We did so to better understand the impact of the initiative, and so that we might improve the quality of future program iterations. We focused our efforts in 2 areas: (1) quantitative evidence of reach to and engagement with our broad community of educators and (2) open-ended responses from participants via a brief survey relating to the experience each participant had in helping create the content.
Quantitative metrics offering evidence of reach to and engagement with our community of educators were collected. These include total retweets and likes, and number of bit.ly link clicks to the “One Minute Teaching Tips” website per tip on Twitter.
The brief survey was developed by the lead author—a social scientist and educator with training in survey design—and thus has no known validity evidence. It was intended to understand factors taken into account when developing their tip, how their involvement in the initiative made them feel, and how they would improve the program in the future. The 3 open-ended questions included: 1) How did you choose your “One Minute Teaching Tip;” 2) How did it feel to participate in the “One Minute Teaching Tips” initiative; and 3) How would you improve the “One Minute Teaching Tips” initiative. Each participant was contacted via email up to 3 times, with a request to complete the survey after their tip was released. Participants were informed that their completion of the routine educational evaluation was voluntary, and that interesting findings might be shared broadly with our community. Thus, survey completion was taken as implied consent.
We employed 2 professional development dimensions offering contexts for learning documented in the faculty development literature as an organizing framework from which to interpret our results. 18 First is the individual or independent experience dimension—for example, reflecting on experience, learning by observing, or learning by doing. Second is the group or collective experience dimension—for example, work-based learning or participating in a community of practice. 18
Data analysis
Quantitative data were analyzed in SPSS version 28. 19 Descriptive statistics were obtained. Differences between or relationships among key variables were determined via independent samples t-test or spearman correlation.
Directed content analysis was utilized to analyze the open-ended responses from participants. 20 This approach is appropriate when starting with a theory or relevant prior research findings as guidance for initial codes. 20 We directed our analysis through the organizing framework of the 2 professional development dimensions—the individual or independent experience and the group or collective experience—to help organize and interpret our results.
We analyzed our open-ended question responses by first aggregating responses in Microsoft Excel. Then, 2 coders (KD and CD) familiarized themselves with the data, each independently reviewing 10 responses to the 3 questions and creating independent preliminary code lists. Then, the coders independently identified whether early codes fell into each of the 2 professional development dimensions—the individual or independent experience and the group or collective experience—and confirmed them together. While the authors coded, they iteratively collapsed codes, refined definitions, and discussed recurring data patterns. After codes were applied to all data—continually organized within the 2 professional development dimensions—codes were combined into categories. We did not specifically look for sufficiency as all available data were analyzed. Trustworthiness of the data was appraised as the data analysts reflected upon how their roles as PhD educator (KD) and an educational program planner (CRD) may have influenced data interpretation. The senior author (EKA) reviewed findings, appraised interpretations, and confirmed results.
The educational evaluation was considered exempt by the Mass General Brigham Human Research Committee (Protocol #: 2021P001205).
Results
Participant engagement
A total of 59 educators (79.7%) agreed to participate in the initiative. Five educators (6.7%) declined participation and 10 educators (13.5%) did not reply to the invitation. Among those who agreed to participate, 50 (84.7%) completed their tip. These included 41 physicians, 5 clinicians from nursing, physical therapy, speech therapy, and physician assistant specialties, 2 education specialists, and 2 fellows. A total of 45 participants (90%) voluntarily chose to complete the survey. Most participants (N = 43; 86%) had professional Twitter handles; most (33 = 73%) retweeted their tip and nearly a third (N = 13; 29%) quote tweeted or replied to their tip, generally in support of the initiative, or to further elucidate the importance of their tip. As indicated in Table 1, tips were created in 7 overarching education topics: feedback and debriefing (N = 8), learner engagement (N = 10), mentoring and role modeling (N = 4), science of learning (N = 3), surgical teaching (N = 4), teaching strategies (N = 18), and teamwork (N = 3).
List of all tips by overarching education topic.

Quantitative results
A total of 100 tweets were sent; the first tweet for each week was sent on a Thursday and the second on a Sunday. The average tweet garnered a total of 43.2 engagements (16.1 retweets and 27.1 likes). Compared to the second tweet, the first tweet resulted in higher engagement (t = 10.16; P≤.001). Bit.ly links to the website containing the collated tips were clicked a total of 1447 times over the duration of our initiative, averaging 28.9 clicks per week over time. Tweet engagement and link clicks were mild to moderately correlated (spearman's correlation = .477; P≤.001). Tweets received engagement from local, national, and international Twitter accounts.
Directed content analysis results
Individual (independent) experience dimension
The 6 categories coded within the individual or independent experience are displayed in Figure 2. As would be expected of the dimension, these categories relate to participants engaging meaningfully, considering prior experience, relying on educational principles, focusing on interests or passions, reflecting on teaching practices, and experiencing reinforcedprofessional identity.

Visual depiction of the 12 categories aligned by individual and independent experience and group or collective experience dimensions.
Importantly, being a part of the initiative was meaningful to participants (Category: Engage Meaningfully). It felt nice to be asked to participate and to be perceived as an educator from others. (P #26)
I thought about my personal experience—things I found useful as a learner and implemented as a teacher. (P #9)
As they developed their tips, they drew upon known and trusted educational principles (Category: Rely on Educational Principles).
This was a teaching pearl I learned while participating in an ACGME course on assessment in medical education. (P #40)
They focused their tip on an area of professional interest or passion, which they wanted to share with others (Category: Focus on Interest or Passion).
My tip is one of my favorite topics in education and something I strive to live by in both my personal and professional life! (P #23)
The process of developing the tip encouraged them to reflect upon their teaching practices with learners (Category: Reflect on Teaching Practices): It was revealing to me as I had to think through my teaching practices and that process was very helpful for me internally to improve my teaching. (P #45)
Participation encouraged educators to think about their own identity as educators (Category: Reinforce Professional Identity).
It helped me feel recognized as a teacher. (P #18)
Group (collective) experience dimension
The 6 categories coded within the group or collective experience are displayed in Figure 2. As would be expected of the dimension, these categories relate to participants feeling the initiative supported institutional need, recognizing visibility to the community, engaging with other tips, supporting inclusive participation, bringing value to the community, or showcasing education.
Our participants offered broad appreciation or praise for the initiative, and lauded the brevity and response to institutional need (Category: Support Institutional Need). Creating a resource of bite-sized pearls that are responsive to current teaching needs is a great idea. (P #1)
It keeps education in front of the community. (P #5)
They also appreciated the free and open sharing of tips in multiple ways (Category: Visible Community Initiative).
It is a great way to gain visibility—presenting this broadly and freely via social media is brilliant. (P #10)
They valued seeing other educator's tips, and some noted sharing tips as resources to other colleagues or educators (Category: Engage with Other Tips).
I enjoyed reading the pearls of wisdom shared by colleagues. (P #20)
Educators noted that it was easy to participate, and supported the inclusive approach (Category: Inclusive Participation).
I especially appreciate the inclusiveness of people being recruited. (P #33)
Participants noted feeling honored, grateful, or valued to be part of the community and included in the initiative (Category: Value within Community): I felt fortunate to be included in the initiative! It is great to be a part of such a robust medical education community. (P #28)
For some, this encouraged an expectation or desire for future participation in the community (Category: Value within Community).
I look forward to more sharing and learning. (P #1)
They also lauded the initiative as being high quality and refined, and that each tip was aligned with a scholarly reference for further self-directed learning (Category: Showcase Education): The result was a very polished end-product. (P #24)
Participants also offered improvement suggestions, such as the inclusion of learner perspectives. Others desired additional guidance regarding how to further disseminate their tip via Twitter. Additional suggestions included expanding tips such that they included an audio or video component.
The introduction of one minute concept videos or visual abstracts briefly outlining the teaching tip would help with engagement and visibility. (P #13)
Figure 2 displays the 12 categories identified through our analysis and detailed above. We organized those categories as they fit into the individual or independent experience dimension, for example, by feeling engaged, drawing on experience, sharing interests or knowledge, or reflecting. It also makes note of the group or collective experience dimension, for example, by supporting or highlighting the institution or colleagues, learning through the workplace, or showcasing education. The arrows suggest that when taken together, the dimensions reinforce each other and support the educator in feeling valued through illustrating their engagement within our community.
Discussion
We developed an initiative to deliver micro virtual asynchronous professional development to faculty, staff, and trainees throughout our institution and broadly through Twitter. Our intention was to showcase our community of educators, by inviting a group of interprofessional health professions educators to co-create a series of teaching tips. We also endeavored to highlight our institution's educational mission at a challenging clinical time.
We measured outcomes along 2 professional development dimensions: individual or independent experience and group or collective experience. 18 We found that educators were grateful to participate and the initiative encouraged them to draw on prior experience as learners, mentees, or teachers, rely upon known and trusted educational principles, focus on interest or passion for education, reflect on teaching practices, engage meaningfully in the education community, and experience reinforced professional identity. Participants pointed to its’ timely alignment with institutional need for brief, visible, open, and easy to access professional development. They also appreciated engaging with other educator's tips, supported the inclusive participation, recognized the importance of showcasing education at a difficult time, and appreciated that it brought value to the community. We also find that our initiative was well-received by those who benefitted from the micro asynchronous virtual learning, with each tip garnering engagement on social media and link clicks to the website; we note that the first tweet was more impactful and that there was a relationship between tweet engagement and link clicks.
Importantly, our participants reflected on their prior teaching and learning experiences, and their roles as educators, which aligns with prior literature. 18 This reflecting on experience encourages educators to distill the complexities of teaching into understandable pieces, consider personal assumptions, encourage the use of new teaching approaches, and enhance intentionality as an educator. 18 Moreover, seeing colleagues reflect on their actions as educators can trigger additional reflection, 18 in concordance with the prior literature and as reported by our participants.
There are implications beyond our local setting. The Accreditation Council for Graduate Medical Education (ACGME) requires that faculty annually receive professional development in areas including educator development, quality improvement and patient safety, and in fostering wellbeing. 21 Each of these topics is amenable to a similar style of delivery across specialties and groups. Tips could be created by faculty in a division, department, or even institution and then shared via asynchronous channels such as email, Teams or Slack, WhatsApp, newsletter, app, podcast, or social media.2,3,10 Other than personnel costs, program costs are limited as infographics could be created in online infographic programs. Asynchronous delivery methods could be determined based upon current institutional license, with a secondary benefit of faculty already using those technologies. With monitoring and evaluation to ensure that learning outcomes are translated into practice, such initiatives could support ACGME compliance.
An additional benefit of an initiative such as this is that it may inspire participant confidence in being an educator because they can publicly share their passion and expertise within a broader workplace community. 22 Indeed, our educators indicated that they were able to focus on their interest or passion through creating and sharing their tip. Moreover, because the initiative is so visible, it may heighten the importance of being an educator to those within the institution who have not yet embraced their educator identity. 23 This also serves as a collegial way to encourage faculty to value the community of which they are a part, by showcasing education, members, and resources.18,23 Finally, a planned initiative such as this aligns with more contemporary viewpoints which assert that professional development can occur in a variety of contexts and settings. 18 Adopting modern digital technology to deliver faculty development can engage educators while still following known principles of teaching and learning, as evidenced by our initiative as well as prior literature.2,3,10
However, our initiative has limitations. First, we implemented our initiative only at our institution, and findings may not extend to other settings. Second, while we intentionally requested participation from a diverse group of interprofessional educators representing multiple disciplines and clinical specialties, we acknowledge a potential selection bias, as those we contacted may have desired connection and were more likely to participate as a result. Third, recruitment was at times challenging, and one lesson learned was that the initiative required diligent followup to finalize tips. Fourth, we evaluated our initiative via a brief, open-ended survey among participants rather than through more time-intensive interviews or focus groups, which might have allowed us a deeper or more meaningful understanding of their perceptions of programmatic impact. Moreover, because our intention was to recruit enough participants to deliver our micro virtual asynchronous professional development for approximately 1 academic year, we did not conduct a power analysis or undertake efforts to determine whether our sample of 50 participants represented our institution's broader population of educators. Fifth, while we measured outcomes along both the individual or independent and the group or collective experience, we were unable to elucidate changes in teacher or learner behavior as a result of this initiative, and would need more rigorous measurement at a higher outcome level to do so. We also acknowledge that micro virtual asynchronous professional development has downsides, which can include but are not limited to the time burden to fit these activities into otherwise busy clinical and teaching schedules, feelings of digital or technology overload, or limited engagement among those who struggle with self-directed learning or who are not intrinsically motivated to learn.11,24 Relying on a framework such as Mayer's Principles of Multimedia Learning or the Analysis, Design, Development, Implementation, and Evaluation model for instructional design may have resulted in a stronger initiative or more robust engagement with our community.25,26 Future initiatives should consider how these limitations can be minimized to result in even more meaningful workplace learning and engagement.
Importantly, while our initiative was developed and deployed during the early phase of COVID-19 in the United States, the results of our evaluation remain relevant. The healthcare workforce continues to have staffing shortages which can lead to increased expectations for clinical time among practicing clinicians and subsequently increased burnout and exhaustion. 27 Thus, these clinicians may forgo or limit the time they have to prioritize synchronous educator development. Microsized, bite-sized, or just-enough-information approaches such as this offer succinct opportunities to highlight better practices in teaching and learning and encourage educator identity, which can make participation easier for busy clinicians.3,12 Moreover, maximizing learning opportunities—even small ones—has the potential to reinforce to clinicians that they work in a safe and protective educational community which values their work as educators, potentially leading to reduced feelings of burnout. 28 Importantly, authentic yet informal workplace learning can support performance and encourage feelings of connection to other colleagues and the institution.8,28 This may become even more important as geographically dispersed academic medical centers continue to grow, which will drive the need for creative, virtual, and asynchronous educator development resources.3,10
Conclusion
We developed an evidence-informed initiative leveraging existing technologies to engage health professions educators in the delivery of micro virtual asynchronous and widely disseminated professional development during COVID-19. Our educational program evaluation revealed a multitude of ways in which the initiative was successful, both for the individual educator who participated, but also as part of a broader, collective experience. Ultimately, our initiative meaningfully supported educators in reflecting on their experience as educators, drawing on known and trusted educational principles, sharing their passion for education, and pondering their own identity as educators. More broadly, the initiative was responsive to current need, supported inclusivity, and kept education visible to the larger education community at an otherwise challenging time.
Footnotes
Acknowledgements
We acknowledge the health professions educators who participated in our initiative.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Review
The educational evaluation was considered exempt by the Mass General Brigham Human Research Committee (#2021P001205).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.