
Abstract
OBJECTIVES
Improved knowledge of hepatitis C virus (HCV) screening, linkage to care, and treatment is needed among nonspecialist medical professionals to combat the HCV epidemic. The authors sought to implement and analyze the impact of an HCV curriculum for primary care professionals (PCPs) across the state of Vermont, USA.
METHODS
This investigation was a retrospective analysis of uptake of a Vermont HCV educational curriculum and its impact on HCV direct-acting antiviral (DAA) prescribing rates within the state before and after the study period. The curriculum was delivered online and in-person over 2 years from 2019 to 2020. The primary outcome was health care professional performance on a pre- and post-curriculum short-term knowledge assessment exam. The secondary outcome was assessing the number of unique healthcare professionals within a single payor database prescribing DAA treatment for HCV in Vermont before and after the study intervention, from January 1, 2017 until December 1, 2021.
RESULTS
There were 31 unique respondents on the pre- and post-intervention examinations, which represented 9% of known participants. Respondents included physicians (n = 15), nurse practitioners (n = 8), and nurses (n = 8). Pre- and post-intervention knowledge scores increased significantly across all provider groups, from 3.2 (SD 0.6) to 4.5 (SD 0.4) 1 to 5 scale (P = .01). The total number of unique HCV DAA therapy prescribers decreased over the study period, from 17 in 2017 to 9 in 2021.
CONCLUSIONS
A Vermont statewide HCV curriculum for PCPs was successful at increasing short-term HCV-related knowledge. However, this did not obviously translate to an increase in new professionals treating HCV.
Introduction
Hepatitis C virus (HCV) infection continues to be a large public health burden. 1 More than 185 million people are infected with HCV globally, 4 million of whom live within the USA, and it remains a leading cause of cirrhosis, liver cancer, and liver transplantation nationally. 2 After a steady decline in new infections over the previous two decades, the incidence of HCV has rapidly risen since 2011. In particular, rural areas are seeing an especially steep rise in new HCV cases, with by some estimates twice the incidence of new HCV infections compared to urban areas. 3 In Vermont, a rural northeastern state, the prevalence of HCV was estimated to be 1.45% in 2010, decreasing to 0.41 to 0.70 by 2016.4–6 This epidemic has been linked to the explosive increase in injection drug use, with the prevalence of HCV among younger persons aged 20 to 39 years old and women of child-bearing age increasingly significantly in recent years. 7 Additionally, there has been an increase in newly reported HCV among those who are 60 and older, so-called baby boomers, attributable to national screening efforts. 8 Thus, the burden of HCV infection cuts across a wide swath of patients. A striking feature of chronic HCV is the absence of symptoms, and if not diagnosed and treated, infected individuals are at risk for progressive liver disease and premature death. 9
Once HCV is diagnosed, however, successful treatment with direct-acting antivirals (DAAs) reduces disease-related morbidity and mortality. 9 DAA treatment is straightforward and highly effective; nearly all patients with chronic infection can be cured with 8 to 12 weeks of once-daily oral therapy with minimal side-effects. 10 However, data suggest that fewer than 10% of HCV-infected patients nationally are appropriately diagnosed, linked to HCV professionals, and given curative therapy. 11 Thus, the key to eradication of HCV infection is improved screening, diagnosis, and linkage to treatment. Rural areas face additional challenges related to a lack of medical professionals with expertise in HCV recognition, treatment, and engagement.3,12
Given the rapidly changing HCV landscape, there is currently a significant national HCV knowledge deficit.13,14 There is an unmet need for efficient strategies for HCV screening, diagnosis, and treatment within primary care professionals (PCPs). 15 Additionally, there is increasing data that treatment of uncomplicated HCV by PCPs may result in increased patient retention in care than with subspecialists, with patients more likely to achieve HCV cure.16–18 Thus, educating and training PCPs on HCV care, particularly in rural areas with a dearth of specialists, is a critical step in the eradication of HCV. 19
We sought to enact a Vermont statewide curriculum for PCPs on HCV diagnosis, workup, linkage to care, and treatment. We created a free, open-access, online curriculum pertaining to HCV care specifically in Vermont, which was then widely disseminated to PCPs. 20 We also traveled throughout the state and gave didactic sessions on HCV both in-person and remotely. We hypothesized that we would be able to show improved HCV knowledge among healthcare professionals throughout the state, and that this would increase HCV treatment across Vermont.
Methods
Study Design
This investigation was a retrospective analysis of uptake of a Vermont HCV educational curriculum and its impact on DAA treatment within the state. Our work was supported by the Vermont Department of Public Health and the Vermont Viral Hepatitis Taskforce.
Study Setting and Population
Location
This was a statewide intervention within Vermont, which is a small state in the northeast United States with a population of 623 989 (49th rank nationally), a median household income of $57 513 (28th rank nationally), and where 61.1% of the population lives in a rural area (second rank nationally). 21
Description of the curriculum
The curriculum was designed by the authors, who are Hepatology (SL) and Infectious Diseases (AH) specialists at the University of Vermont Medical Center, Burlington, VT, USA with experience in treating HCV, and took place in 2019 to 2020. The curriculum consisted of four free and open-access online modules; (1) HCV basics, (2) screening for HCV, (3) care for patients who screen positive for HCV, and (4) linkage to care and HCV treatment basics. 20 The curriculum was designed for practicing healthcare professionals at the physician, nurse practitioner, physician assistant, and registered nurse levels to learn how to appropriately identify and move toward treatment patients with HCV, and was structured around the HCV guidelines. 10 The HCV basics module included information on the epidemiology, structure and pathogenesis, hepatopathic effects, and natural history and consequences of HCV and HCV infection. The screening for HCV module covered who should be screened, why screening for HCV is important, barriers to HCV screening and how to address them, and how to appropriately screen for HCV. The post-screening Process module covered what to do after a positive HCV screen, screening for co-infections, and how to accurately assess hepatic fibrosis. The linkage to care and HCV treatment basics module covered who should be treated for HCV, the basics of HCV DAA regimens, what testing is needed during and after treatment, how to test for HCV cure, and what to tell patients after HCV cure has been achieved. Continuing Medical Education credits were made available for professionals completing the curriculum. The curriculum was distributed to healthcare professionals via three mechanisms: (1) the Vermont Viral Hepatitis Taskforce, which comprises about 30 multidisciplinary professionals representing every county of Vermont; (2) OneCare Vermont, which is the state-wide accountable care organization; and (3) didactic presentations by the authors, both in person and remotely, to locations throughout the state.
HCV education assessment survey
To test short-term HCV knowledge, we developed a 40-question multiple choice examination administered at baseline and after completion of the curriculum. These examination questions were created by the authors and not externally validated, though designed to test basic HCV knowledge. Qualitative comments were also captured in the post-intervention exam. In parallel, we submitted to participating health professionals a questionnaire, using Likert-style questions from 1 to 5, that sought to determine the utility of the curriculum and the extent to which it would change their HCV management. Only health professionals in Vermont were eligible to participate. Other than CME credit that was made available for completing the curriculum, there was no explicit incentive to complete the survey.
Outcomes
The primary outcome was health care professional (MD, NP, PA, RN) performance on a pre- and post-curriculum short-term knowledge assessment exam. The secondary outcome was assessing the number of unique healthcare professionals prescribing DAA treatment for HCV in Vermont before and after the study intervention. We obtained data from Vermont BlueCross/BlueShield (BC/BS), the largest private health insurance provider in Vermont, on the number of DAA prescribers per Vermont zip code per year from January 1, 2017 until December 1, 2021.
Statistical Analysis
For the primary outcome, pre- and post-test performance was compared with paired t-tests. A P-value of <.05 was deemed to be significant. Because of low overall values, analysis of statistical significance on the secondary outcome was not performed and results are presented descriptively.
Results
Results of the primary outcome are shown in Table 1. There were 342 unique website hits during the study period, of whom 31 unique respondents completed the pre- and post-intervention examinations (9.1%). Respondents included physicians, nurse practitioners, and nurses; there were no physician assistant respondents. Pre- and post-intervention knowledge scores for each of the 4 modules increased significantly for each participant degree type. Across all provider groups, the educational intervention was felt to be helpful (4.7 [SD 0.3] score on a 1 to 5 scale with 5 representing “very helpful”) and likely to change management (4.6 [SD 0.3] score on 1 to 5 scale with 5 representing “very likely”). Sample qualitative comments on the curriculum are shown in Table 2.
Results of pre- and post-intervention examinations.
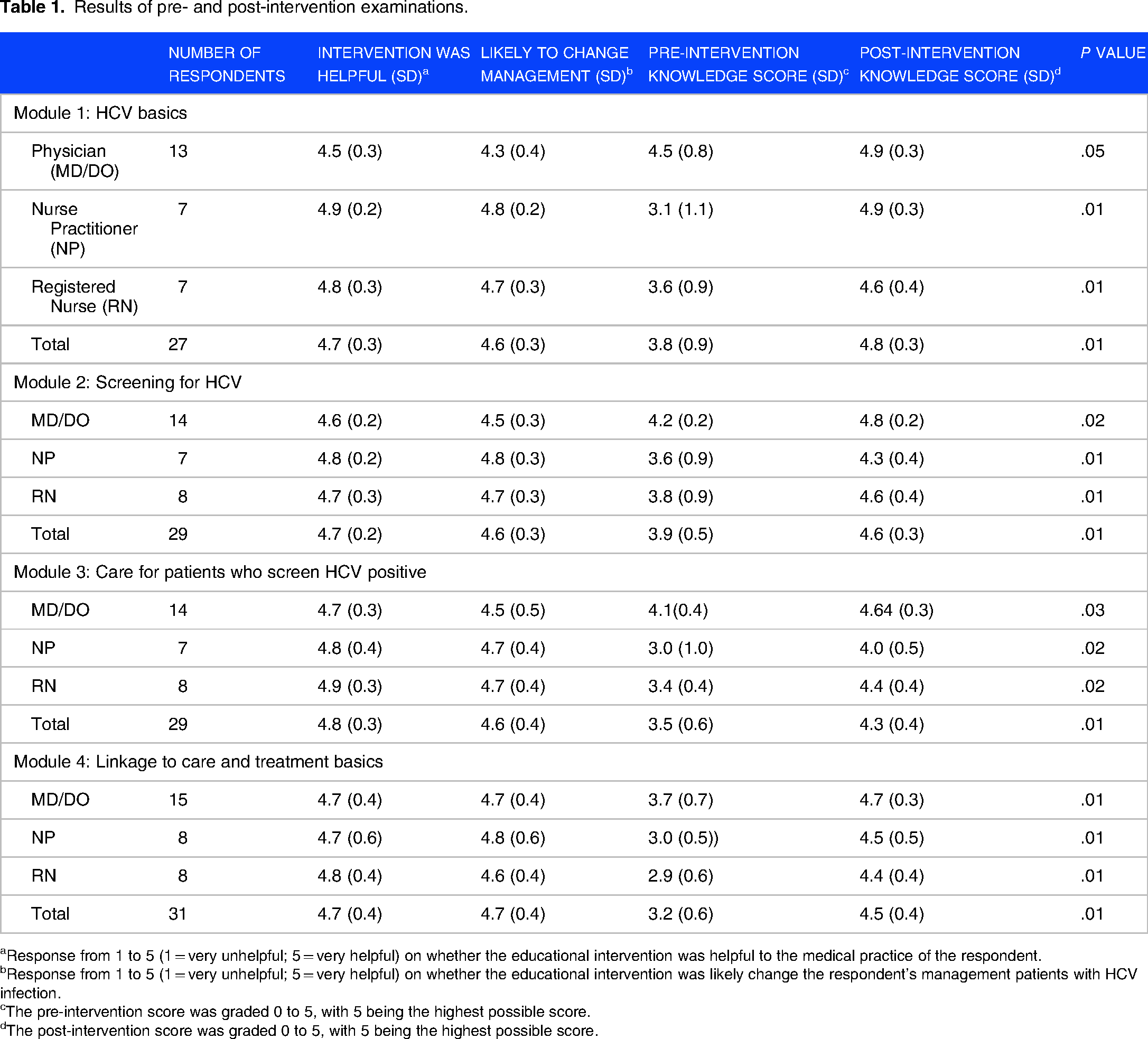
Response from 1 to 5 (1 = very unhelpful; 5 = very helpful) on whether the educational intervention was helpful to the medical practice of the respondent.
Response from 1 to 5 (1 = very unhelpful; 5 = very helpful) on whether the educational intervention was likely change the respondent's management patients with HCV infection.
The pre-intervention score was graded 0 to 5, with 5 being the highest possible score.
The post-intervention score was graded 0 to 5, with 5 being the highest possible score.
Sample qualitative responses from respondents on the educational intervention.
Results of the secondary outcome, the number of unique professionals prescribing HCV DAA therapy per year per Vermont County to BC/BS patients, are shown in Table 3. The total number of unique HCV DAA therapy prescribers decreased over the study period, from 17 in 2017 to 9 in 2021.
Unique HCV DAA prescribers and HCV DAA prescriptions per 1 000 000 population by Vermont county and year.

Discussion
In this study, we have assessed the impact of an internet-based curriculum on health professional knowledge about HCV and the extent to which it influenced treatment of this disease. An internet-based curriculum has distinct advantages in a largely rural state like Vermont, since a preponderance of its health professionals are located at considerable distances from centers in which in-person learning can be delivered. In addition, it provides educational opportunities at times that do not conflict with clinical responsibilities. Moreover, the curriculum design permits timely revisions in response to evolving updates in HCV management, which would not be possible in a static lecture format. The success of this curriculum is supported by the improvement in short-term HCV knowledge scores across a broad spectrum of responding health professionals, particularly among nurses and nurse practitioners, who completed the program. More importantly, they suggest that the curriculum would likely change their management of HCV.
Despite these positive findings, the impact of the curriculum on HCV treatment was less clear. Based upon our analysis of a subset of patients with BC/BS health plan coverage, neither the number of DAA prescriptions nor the number of individual DAA prescribers increased after the curriculum was launched. This finding must be interpreted with caution, however. First, the data are confined to HCV treatment, and they do not capture the extent to which HCV screening or specialty referral changed during the study period. Second, not all HCV patients in Vermont have health coverage through BC/BS, and it is possible that the trajectory of DAA prescriptions issued for HCV patients with other forms of health coverage was distinct. Because patients with lower socioeconomic status may be higher risk for HCV acquisition, this is a significant limitation of our data. 9 Third, the post-curriculum study period coincided with the emergence of the COVID-19 pandemic, and this could have had an unexpected influence on patterns of HCV management during this time. This is supported by observations in multiple studies, which have shown decreased rates of HCV treatment during the COVID-19 era.22,23 While the prevalence of HCV in Vermont appeared to be decreasing from 2010 to 2016, it is unclear at this time what impact the COVID-19 pandemic had on Vermont's HCV prevalence.4–6 Clearly, additional information and study beyond the COVID-19 emergency would be required to address the relation between curriculum availability and the scope of HCV treatment in Vermont. Fourth, prior authors have demonstrated the complexity of HCV screening and care, and the need to engage primary care physicians; a highly successful curriculum may require a multifaceted approach.24,25
Several additional points and limitations merit comment. Although we recorded 342 unique website hits during the study period, we do not know how many of these completed the curriculum but did not take the assessment test. Our proportion of users who completed the pre- and post-tests were low. Rather, our analysis of the educational value of the HCV curriculum was confined to the 31 health professionals who completed the questionnaire and examination, and we do not know what impact it may have had on others who may have viewed it but did not respond. There were statistically significant short-term educational gains across this group, but the low number of respondents precluded an analysis of its impact according to health professional type (eg, physician, nurse practitioner) or location (eg, rural vs nonrural). There was not a power analysis performed, though we were able to show statistically significant short-term educational gains. An additional caveat is that our HCV knowledge assessment examinations pre- and post-intervention were not externally validated and do not assess for long-term retention. To address these issues would require revision of the website to foster greater participant interaction while connected, improved tracking of participants, and to seek strategies to engage participants subsequently for educational re-assessment. A method of tracking long-term educational and HCV DAA prescribing practices would be valuable. This would be worthy of study in the future.
Conclusion
Treatment of HCV is a public health priority, though there is a significant gap between patients who need treatment and the number of prescribers who treat HCV. This is particularly true in rural areas like Vermont. Educational websites hold the promise to expand HCV knowledge among health professionals. The experience we describe here supports this concept. Additional studies will be needed to clarify what interventions are necessary to translate this knowledge to fill a persistent and pervasive care gap, in order to effectively combat the HCV epidemic.
Footnotes
Acknowledgment
Dr Hale and Dr Lidofsky would like to acknowledge and thank the Frymoyer Scholarship program at UVM LCOM for its outstanding support.
Author Contribution
Andrew J. Hale, MD is an infectious diseases physician at the University of Vermont Medical Center and Assistant Professor of Medicine at Larner College of Medicine at the University of Vermont, Burlington, VT.
Steven D. Lidofsky is chief of hepatology at the University of Vermont Medical Center and Professor of Medicine at Larner College of Medicine at the University of Vermont, Burlington, VT.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported with an internal University of Vermont Larner College of Medicine medical education grant called the Frymoyer Scholarship. Dr Hale and Dr Lidofsky were co-recipients of the Frymoyer Scholarship.
Authorship Verification
All coauthors have seen and agree with the contents of the manuscript and have contributed significantly to the work.
Declarations
The Institutional Review Board at the University of Vermont approved this protocol as medical education and quality improvement work and waived the requirement for informed consent on February 23, 2018 (UVM STUDY00001386).
Informed Consent
N/A.