
Abstract
The number of primary care physicians in the United States is inadequate to meet current or projected needs. This is likely exacerbated by continuing increases in the cost of medical education and student debt. The Geisinger Commonwealth School of Medicine is part of an integrated care delivery system in which primary care is central to managing health, improving access, and advancing value-based care. The need for primary care providers and psychiatrists is difficult to meet despite generous recruiting incentives. To address this, the Abigail Geisinger Scholars Program (AGSP) represents a novel curricular approach linked with the provision of full tuition and fees and a living stipend to students who commit to work at Geisinger in primary care or psychiatry following residency. The support is provided as a forgivable loan. The program features preferential clinical placements, curricular enhancements, and celebration of the dedicated cohort. Fair and nonpunitive provisions allow students to opt-out. The AGSP supports 45 students in each class of 115. Outcomes monitored include withdrawals from the AGSP; academic performance of participants and their satisfaction with the program; the number who choose to repay the loan rather than fulfill the service obligation; the percentage who remain at Geisinger and in primary care following the period of obligation; and other measures. This model offers an attractive opportunity for students to experience a curriculum enhanced in primary care while receiving generous financing for their medical education. It bolsters the primary care physician workforce and aligns care delivery with new financing models.
Report
The number of primary care practitioners in the United States is inadequate to meet our country's current needs, and even less adequate to its predicted needs as the population grows and ages and as the number of insured rises. 1 In 2015 the Graham Center projected the gap over the coming decade to increase by 35,000 to 52,000 primary care practitioners. 2 This gap is particularly problematic for rural populations.3,4 This problem is a barrier to better health for populations and to the success of health systems.
To address the projected physician shortage, 31 new medical schools, including the authors’ institution, have opened since 2001, several of which have a defined curricular emphasis on addressing needs for rural and underserved populations and for primary care physicians.5,6
Medical student interest in primary care specialties has declined in recent decades. 7 Reasons include the substantially lower career earning potential relative to other specialties, lifestyle factors, appeal of specialty expertise, and perceived lack of prestige of primary care, as communicated implicitly or even explicitly by specialty-oriented medical school faculty.8–12 The proportion of medical students intending to pursue a career in primary care declines significantly over the 4 years from entry into medical school, suggesting that medical school curricula or environment discourage interest in primary care. 13
The prospect of debt, often at crushing levels, can be a factor in student specialty choice.14,15 For the past 6 decades the cost of medical school has risen at rates far exceeding inflation. 16 Despite financial aid programs, the median debt of an American MD graduate is $200,000, and 20% of them accumulate more than $300,000 in educational loans. 17 Financial stresses can contribute to academic failure in medical school, particularly for students from disadvantaged backgrounds and groups underrepresented in medicine. 18
For years the AAMC has identified student debt as a serious problem.16,19 All medical schools make scholarships a fundraising priority. Some have established endowments so that none of their students graduate with debt by providing financial aid in the form of scholarships, awards, or grants.20,21 Very few cover the cost of tuition for all students regardless of financial need.22,23 Such support, however generous, is typically not linked with career plans, workforce considerations, or community needs. The free-tuition approach has been criticized for not making these scholarships contingent upon serving societal needs such as by working in medically underserved areas or entering primary care fields.24,25
Most health systems still use a traditional fee-for-service model to generate revenue from third-party payors by filling hospital beds and performing procedures. Primary care providers represent the entry pathway to the systems through referrals. In other systems in which the payor (the health plan) and the clinical system are an integrated organization, keeping patients healthy and out of the hospital becomes a business objective by reducing expenditures, while also serving better the needs of patients. Geisinger is an integrated health system with nearly half a million of its patients insured by the Geisinger Health Plan. Keeping these patients healthy without the need for expensive procedures or hospitalizations is incentivized. Especially in integrated health systems, preventive care provided by accessible primary care providers who deliver high-value care is good for patients and populations. All systems, traditional and integrated, need more primary care providers to succeed.
The Abigail Geisinger Scholars Program
The Geisinger health system in rural Pennsylvania is an integrated provider/payor health system that has been caring for a large rural swath of Pennsylvania for over 100 years. 26 Geisinger includes the Geisinger Commonwealth School of Medicine (GCSOM; “Geisinger Commonwealth”). Formerly known as The Commonwealth Medical College (TCMC), GCSOM was founded in 2008 as an independent medical school to address the physician shortage in northeast and north-central Pennsylvania. 5 TCMC integrated into Geisinger in 2017. Geisinger has a need for primary care physicians and psychiatrists that mirrors the national gap for rural and underserved areas. 27 To address this, the system spends significant resources on the recruitment of such physicians. Nationally the cost per primary care physician recruited has been estimated to be $342,000. 28 Thus, the cost of recruiting exceeds the average debt of medical school graduates.
Geisinger has created a new model to address its primary care shortage: the Abigail Geisinger Scholars Program. In addition to its curricular emphasis on primary care, the program features a forgivable loan with a service obligation, modeled after the Armed Forces Health Professions Scholarship Program, the National Health Service Corps and the Public Loan Forgiveness Program, which carry obligations to serve in the military or other public health service.29,30 The Veterans Administration offers a similar program with a service obligation. 31 These have all been available to medical students for decades, although comparatively few students choose to avail themselves of these opportunities. Medical students at Geisinger Commonwealth who are selected for the AGSP and commit to entering primary care or psychiatry experience a curriculum with an enhanced focus on primary care, and receive full tuition and fees, plus a living stipend of $2000/month, funded by the health system. Those specialties identified as primary care are internal medicine, family medicine, and medicine/pediatrics. (General pediatrics is not currently included because of the significantly greater need in the region for primary care providers for adults.) Participants are free to match for residency at any program in these specialties, or psychiatry, at any institution, provided they return to Geisinger upon completing their primary residency to practice for the obligated period of time. That obligation is 1 year of service at Geisinger for each year of support received during medical school, with a minimum of 2 years.
This program is administered and evaluations were conducted at the GCSOM main campus in Scranton, PA and its 6 clinical campuses which are primarily at Geisinger clinical sites.
During the initial roll-out in 2019 students in their first and second years of medical school were allowed to apply for entry into the AGSP, but subsequently, all participants are admitted directly to the program upon matriculation. Initial cohorts were smaller; in 2021 the first 5 Abigail Geisinger Scholars graduated, and 9 graduated in 2022 (Table 1). Starting with the class of 2025 who entered in August 2021 there will be 45 participants among the 115 students in each medical school class.
Abigail Geisinger Scholars by Graduation Year.
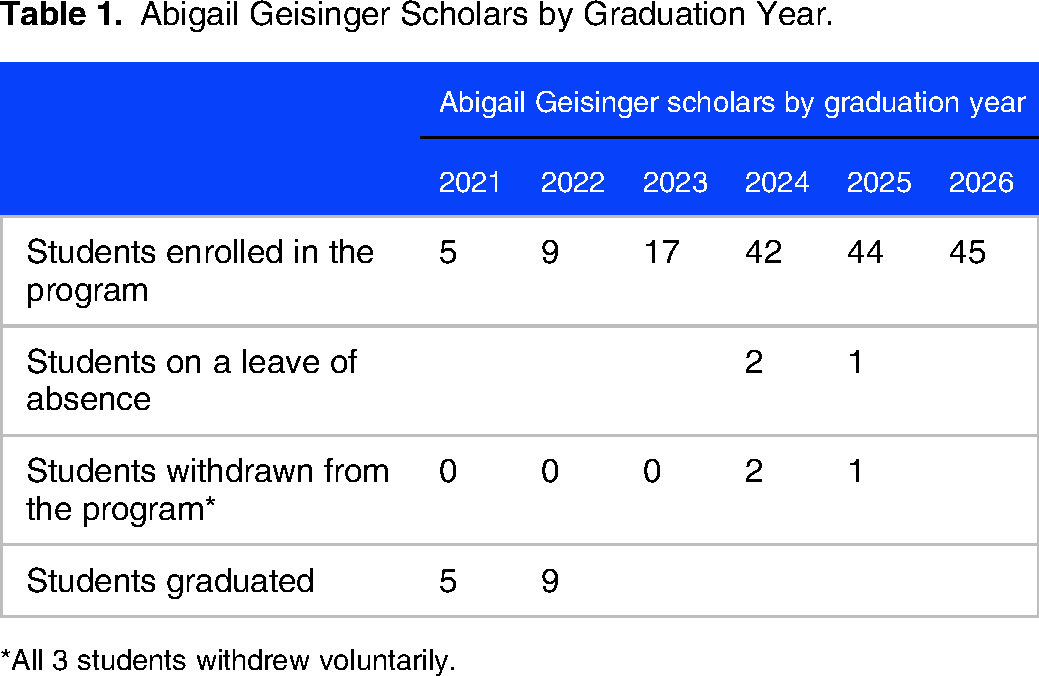
*All 3 students withdrew voluntarily.
Funding for the AGSP is provided by the clinical system with a loan administered by the medical school. The system and school are separate corporate entities within the same governance structure. Thus, the tuition is carried on the books of the medical school as a receivable until the time of employment, when the system transfers those funds to the school. Interest is calculated based on the prevailing rate for Federal Direct Subsidized Loans. Abigail Geisinger Scholars are not required to make any payments during the period of their residency. Upon employment at Geisinger, the accumulated principal and interest are forgiven evenly across the period of employment obligation (typically 4 years). (Unlike the governmental loan forgiveness programs, this forgiven amount is taxable; those taxes are withheld from the participant's paycheck.)
There are safeguards built in, for students and the school. The loan agreement stipulates that support is available only for 4-year period of medical school, and scholars must maintain satisfactory academic progress through medical school and residency. A steering committee monitors student and resident progression. Should a student leave the AGSP for reasons of academic performance or professionalism as determined by the steering committee they would continue in the traditional curriculum and the support they have received to that date would be converted to a loan with interest accumulating at the Federal Direct Subsidized Loan rate; recipients would be responsible to repay the remaining balance over 10 years. Similar terms would apply should a participant withdraw voluntarily from the commitment, whether that occurred during medical school, residency, or employment at Geisinger. If the clinical system is, unexpectedly, unable to offer the graduate employment at the time of completing their residency, the loan is forgiven.
Selection process
In applying to GCSOM prospective students submit the Association of American Medical Colleges application and the GCSOM secondary application which includes a question regarding interest in applying to the AGSP. Applicants expressing such interest then answer an additional question regarding their interest in primary care or psychiatry and are asked to describe any additional experiences relevant to the mission and goals of the AGSP. These students receive detailed information about the AGSP. They are required to attend informational sessions explaining the requirements of the program including a detailed explanation of the financial terms. Additionally, they are given an opportunity to hear from primary care physicians and psychiatrists who teach in the AGSP and current medical students in the program.
Applicants are selected to interview for the AGSP after they have been accepted for admission to GCSOM using principles based on the literature on the sustained interest in primary care and rural health care. Students are selected for the program based on the following criteria: financial need; merit; diversity; geographic ties to the region; the likelihood of staying at Geisinger beyond the period of service obligation; and alignment with the mission and goals of the program.
The AGSP was initially launched in January 2019 with 13 students then in the middle of their first and second years; since then students have entered the program upon matriculation to the first year. Those first students were not restricted to primary care or psychiatry and were free to choose any specialty, and they received no stipend. The stipend was introduced beginning in 2020 when the program became focused on primary care.
The first cohort of 5 Abigail Geisinger Scholars graduated in 2021. In the 2021 to 2022 application cycle, of 5980 applicants to Geisinger Commonwealth 1009 applied for the AGSP. Of these, ultimately 106 were offered acceptance to the AGSP and 45 committed to the program. Including these new students there are a total of 148 current Abigail Geisinger Scholars across the 4 classes in the 2022 to 2023 academic year; the number will grow to 180 in the next year.
Curricular focus on primary care
This AGSP is built on the findings in the literature regarding cultivating a rural physician workforce which includes creating cohorts with similar interests, grounded in the Community of Practice framework. 32 Abigail Geisinger Scholars are assigned to a primary care or psychiatry advisor within an advising pod of students and residents in these fields. These longitudinal supports are designed to create a sense of community and commitment to the program. Scholars proceed through medical school (and residency if at Geisinger) in these pods and when they return to practice within the Geisinger Health System will take over the leadership of an advising pod.
Scholars can participate in research under the direction of faculty mentors. Scholars have representation on the Medical Student Council to advocate for the unique interests of the AGSP students within the larger medical school class. Celebrating scholars and their contributions during medical school, residency, and as practicing physicians is an important component of retention. This includes quarterly newsletters and community-building activities that begin prior to matriculation through graduation. Collaboration between the Abigail Geisinger Scholars leadership team, GCSOM Alumni Relations, and the Geisinger Physician Recruitment Team during the residency years supports resident scholar engagement and preparation for transition to employment. Program participants will be matched to potential employment sites in the health system upon completion of training through a mutual ranking process similar to the match process in the medical school-to-residency transition.
An important element of the AGSP is a curricular emphasis on primary care. In August 2021 Geisinger Commonwealth School of Medicine launched its new Total Health Curriculum, with an enhanced focus on topics relevant to promoting health beyond merely managing disease. This curriculum integrates clinical with basic science, with meaningful clinical experiences from the first year and meaningful incorporation of fundamental science across the later years. It is structured around the 6 curricular themes of community engagement, population health, primary care, professional and personal development, health systems citizenship and health equity and justice. Each theme is found in each of the 3 successive phases of the curriculum: Principles of Medical Science and Practice (18 months), Core Clinical Immersion (12 months) and Career Differentiation and Exploration (18 months).
In the context of this new curricular direction, Abigail Geisinger Scholars experience an enhanced primary care curriculum with focused clinical experiences. A monthly seminar series features presentations by and informal interactions with Geisinger leadership including the CEO, CMO, health plan leaders, and others. Clinical experiences involve Geisinger's ‘Primary Care Redesign’ programs, which support team-based population health care. These signature programs include Geisinger 65Forward, a multidimensional program for enrollees in Medicare Advantage; Geisinger@Home, which proactively addresses patients with multiple medical problems; and the Fresh Food Farmacy, providing fresh food and training in nutrition and in food preparation to patients (and their families) with diabetes, hypertension and obesity. For all students, the opportunity to participate in these programs can reshape the perception of primary care among those who might otherwise have pursued specialist careers, and adds understanding to the concept of value-based care.
One important message in the AGSP is that primary care is a cutting-edge field, an exciting opportunity to be at the forefront of care delivery. Abigail Geisinger Scholars learn from Geisinger's data analytics team to leverage data and genomics to support disease prevention, early detection and intervention, and increased access. Expertise in the health plan informs the medical curriculum for population health and healthcare economics. Precision health is being incorporated into primary care through Geisinger's genome sequencing program (MyCode). MyCode is one of the largest and most ambitious initiatives of its kind, with more than 260,000 patients enrolled so far. Sequencing results with actionable consequences, and risk analyses, are returned to patients and entered into the medical record to inform medical care. Geisinger's pharmacy system innovations have produced dramatic improvements in anticoagulation, hepatitis C and diabetes outcomes and significantly reduced opioid prescribing, successes that inform case examples in the health system science curriculum.
Program evaluation
AGSP leadership conducts 2 evaluations of the program annually. In the fall a survey monitors commitment to primary care and psychiatry and retention in the program. The spring survey evaluates the effectiveness of the program components. Longitudinal program evaluation ultimately will include student satisfaction with the curriculum, review of retention data to specialty selection, return for loan repayment period, and long-term retention within the health system. The scholar cohorts will be compared with the nonscholar GCSOM class.
Financial support
Institutional investment in the AGSP is considerable. Geisinger forgoes tuition and fees (currently $60,250 for Pennsylvania residents and $66,675 for non-Pennsylvania residents) and disburses a stipend of $2000 per month per student. With the initiation of the AGSP other scholarship funds have not been reduced and are now allocated among the smaller pool of 70 students in each class, not in that program; thus, the school is truly forgoing the “retail” tuition price for each Abigail Geisinger scholar.
While the AGSP is expensive, the cost per student is comparable to the generous recruiting incentives that the system has traditionally offered in the form of signing bonuses, loan repayment and other support, which have not met Geisinger's needs to this point. Geisinger currently employs 186 primary care physicians and 66 psychiatrists, and projects that it will need 225 additional primary care physicians alone in the next 7 years. The system currently averages 18 net new primary care physicians (recruits minus departures) per year. Further, the Abigail Geisinger scholars will bring to their practice an experience in having been educated in the system and familiarity with the electronic medical record and other processes, and therefore the reasonable expectation that they might be more likely to remain at Geisinger long-term.
Geisinger sponsors 2 residency programs in Family Medicine with a total of 12 entry-level positions per year, 2 in Internal Medicine (30 positions per year), and a Medicine-Pediatrics residency (5 positions), and participates in an affiliated Psychiatry residency program with 5 entry positions. Thus, the number of Abigail Geisinger Scholars exceeds the system's available entry-level residency positions. But it is not felt that it is important, or even desirable, for all Abigail Geisinger Scholars to serve their residencies in the system. Regardless of where they do residency training they are contractually obligated to return to Geisinger to practice.
Outcomes
Table 1 provides the enrollment and retention information for the AGSP. Analyses of the 2 program evaluation surveys are planned with several goals including understanding factors critical to premedical students committing to specialty selection and factors that support medical student and resident engagement in their specialty selection and commitment to return to Geisinger's underserved region. A preliminary review of the data from the first 2 years indicates that both tuition support and the living stipend are critically important in committing to the program. Scholars also noted strong mission alignment with a commitment to primary care or psychiatry, rural health care, and caring for underserved populations.
For the long term, Geisinger will be using several measures of the AGSP's success. These include the number of applicants; percent of accepted applicants who commit to participate; success of participants in completing medical school and residency; academic performance of students in the program; internal and Graduation Questionnaire ratings by Abigail Geisinger scholars of the curricular experience, compared with ratings by nonparticipating students; participation in extracurricular opportunities in Geisinger primary care signature programs; percent of participants who withdraw from the AGSP, choosing to repay rather than fulfill their obligation; completion rate of participants through the full period of obligation; percent of participants completing their period of obligation who remain at Geisinger beyond that period; career choices of those who withdraw from the program; and career choices of participants after completing the period of obligation.
Limitations
The AGSP has been in place for 4 years, but the long-term outcomes will not be assessable for another decade or more. Thus, this report is limited in being able to describe only our experience to date, and only in qualitative terms.
Conclusion
While this program with its unique approach is in its early days, the fact that over 1,000 GCSOM applicants also applied to become an Abigail Geisinger Scholar in each of the past 2 years is evidence of strong interest. This is a model for medical education that bolsters the primary care physician workforce and aligns care delivery with new financing models. The AGSP recognizes that medical student specialty selection is often affected by the educational experience and concern over debt. Building on the knowledge of rural and underserved area recruitment programs, the AGSP educates future physicians to primary care and psychiatry while addressing their financial worries. This financial freedom combined with a robust community of practice environment is designed to engage students and residents to become leaders committed to the Geisinger community and provides a model for health systems to address their physician shortage needs, decrease physician recruitment expenses, and foster an engaged workforce.
Footnotes
Acknowledgements
The authors are grateful to Drs Jaewon Ryu and Karen Murphy for their critical roles in creating the AGSP, and to Drs Gerald Maloney and Kim Kovalick for their oversight of the program's operations.
Ethical Approval
These studies have been reviewed by the Geisinger Institutional Review Board and deemed to meet the criteria for exemption from the need for informed consent as defined by the US DHHS Regulations for the Protection of Human Subjects under Category 1 within the regulations (45 CFR 46.104).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work represented here was not supported by any extramural funds. As described above, the costs of the AGSP are provided by Geisinger. All authors are employed by Geisinger.