
Abstract
The relevance of pre-registration programs of nursing education to current and emerging trends in healthcare and society could have a significant future impact on the nursing profession. In this article, we use a PESTEL (politics, economics, society, technology, environment, and law) framework to identify significant current and future priorities in Australian healthcare. Following the PESTEL analysis, we conduct a review of the curriculum content of current Australian undergraduate pre-registration nursing curricula. The data were analyzed to determine how nursing curricula were aligned with the priorities identified in the PESTEL analysis. Findings suggest that preparation–practice gaps are evident in nursing curricula as the broad priorities identified were poorly reflected in undergraduate pre-registration programs. The study recommended (a) the establishment of a nationally consistent mechanism to identify current and emerging trends in healthcare and higher education, and (b) an evidence-based framework that enhances forward planning in the design of undergraduate pre-registration nursing curricula.
It is a truth very certain that when it is not in our power to determine what is true we ought to follow what is most probable.
The dynamism that will inevitably mark unfolding future events over the next decade and beyond will shape and shift healthcare in new and unexpected ways. Nursing must be a key player if it is to continue to evolve and develop as a profession. Nursing education, particularly at the level of undergraduate pre-registration programs, will form a vital part in informing the direction of the profession. Designing nursing curricula to be proactive rather than reactive to future events is essential in future-proofing nursing education. Nevertheless, the process of translating a myriad of contextual factors to inform future directions for nursing education is as difficult as it is necessary. This article proposes a means of future-proofing nursing education by incorporating current and emerging trends relevant to the Australia context into curriculum design.
Background
The profession of nursing is influenced by a complex myriad of political, economic, social, technological, environmental, and legal factors. For instance, political machinations have heralded initiatives such as the 2010 launch of Australia’s National Registration and Accreditation Scheme (NRAS) to improve health workforce mobility and offer a nationally cohesive and consistent approach to the registration of health professionals and accreditation of health curricula (NRAS, 2012). The political agenda is closely associated with economic forces as governments struggle to ensure that healthcare expenditure is both effective and fiscally sustainable.
Beyond politics and economics, the shifts in the social fabric of all nations are exerting influence on priorities in global healthcare. As westernized nations become healthier and live longer, significant challenges are expected to present in the near future as an aging population, the demand for health services, and the identification of major health issues relating to chronic illness become pressing areas of need.
In the Australian scene, technology continues to play a central role in addressing areas of need and easing some of the challenges faced as the complexity of the healthcare environment increases. Initiatives such as remote patient monitoring and “telehealth” will become more commonplace modalities of treatment in healthcare. Nevertheless, one challenge that technology may not be able to overcome occurs in a broader, more concerning context—climate change. Climate change is expected to have a significant impact on health over the coming decades with a greater incidence of natural disasters and the endangerment of residences and food and water supplies. This global issue has been identified as the most significant risk to health in the 21st century by the World Health Organization (WHO; 2014c, 2014d).
Ongoing changes in broad global and national contexts raise questions about the position of nurses and nursing education and whether the legal framework of practice in which nurses operate should evolve with the same momentum that marks healthcare. Health Workforce Australia (HWA) are working toward expanding the professional roles of the current health workforce including advancing nursing practice through the use of nurse practitioners, promoting nurses and midwives work to full scope of practice and the development of that career pathways that accommodate and promote practice enhancement (Gallagher, Fry, & Duffield, 2010). Schober and Affara (2006) assert that advancing nursing practice is a global phenomenon. They highlighted that promoting this reform agenda has required a global debate within and external to nursing (Barton, Bevan, & Mooney, 2012; Schober & Affara, 2006), a debate that has occurred and continues in Australia (Adrian, 2005; Nursing and Midwifery Board of Australia, 2013).
It is in this dynamic and complex environment that nursing operates; an environment that demands professional responsiveness to factors, seemingly distanced from the profession of nursing and nursing education. So much is clear; nursing and nursing education faces considerable challenges in light of the influence of political, economic, social, technological, environmental, and legal factors both now and in coming decades. With these matters at hand, an analysis of current and emerging factors, extrinsic and intrinsic to nursing education, was undertaken to evaluate the alignment of undergraduate pre-registration nursing education with the future needs of Australian healthcare.
Method
The authors employed a two-phase process to (a) identify future directions of healthcare relevant to the nursing profession using a PESTEL (politics, economics, society, technology, environment, and law) analysis framework to categorize the coded data, and (b) conduct a basic online survey of each discrete subject in every undergraduate pre-registration nursing curricula in Australia to assess the level of alignment with the PESTEL results, nationally. Although other entry-to-practice pathways were considered for inclusion in the survey, the variability of entry points to graduate pre-registration programs was considered to be a confounding factor—particularly when pre-requisite requirements and credits awarded for previous study are not routinely published in curriculum documents online.
First Phase
Literature pertaining to the future directions of Australian healthcare was retrieved such as strategic plans, future projections, white papers and annual government, and other relevant organizational reports (e.g., Australian Institute of Health and Welfare [AIHW], Australian Nursing & Midwifery Accreditation Council [ANMAC], and HWA). A search of peer-reviewed literature from July 2001 to July 2013 was conducted using Google Scholar, Medline, ProQuest, and EBSCOHost. The following search terms were entered: future health, future healthcare, future Australia, future Australia health, future nurs*, future economic*, future politic*, future environ*, future population*, future, future politic*, future economic*, future soci*, strateg* AND health AND Australia. Gray literature was also searched with attention given to government reports and future projections.
A PESTEL analysis framework has been utilized in macro-environmental analyses (Gillespie, 2011) and in strategic planning for future contingencies (Walsh, 2005). PESTEL is a mnemonic used to group factors in the macro-environment to enable the identification of general opportunities and risks that impact on future outcomes (Issa, Chang, & Issa, 2010; Kotler & Armstrong, 2004). Analyzing macro-environmental factors is especially valuable when used to understand how external influences, drivers, and hurdles impact on a particular area of focus such as nursing education (Johnson, Whittington, Scholes, & Pyle, 2011). As such, the PESTEL analysis framework was used to codify and categorize current and emerging trends relevant to nursing education and the broader healthcare environment. Data were assigned a code and categorized according to their relevance to one or more PESTEL factors. Two authors, to ensure inter-rater reliability, assessed relevance. Where two authors were unable to agree on relevance, a third author was used to facilitate agreement. Conceptual connections were made while analyzing the data resulting in the development of categories within the PESTEL factors.
Second Phase
A search was conducted of the Australian Health Practitioner Regulation Agency (AHPRA) website for Australian undergraduate pre-registration nursing programs leading to registration (AHPRA, 2012). The following search parameters were entered: Profession—Nurse, Division—Registered Nurse; Qualification Type—General; Country—Australia; Course Type—Bachelor Degree. Ninety programs of study were revealed with double-degrees, post-graduate programs, conversion courses were eliminated from the results. Where an institution offered more than one variation of an award, only the primary program was included. Curricula from the 34 institutions remaining were retrieved and subject titles, subject synopses, and subject learning outcomes were obtained and analyzed to assess their alignment with the PESTEL analysis results from the first phase of the study. Subjects clearly addressing categories pertaining to the PESTEL analysis were assigned a code. Where subjects had a non-descript title such as “Nursing 1” and a subject synopsis or learning outcomes were not available, the data were coded as invalid. A code was also assigned to subjects where investigation of title and/or content synopsis failed to clearly identify a match with PESTEL categories (e.g., those that provided foundational content only such as anatomy, physiology, and pharmacology subjects).
Findings
Findings are presented according to the phases of the research process.
First Phase
Clear categories were developed following coding and analysis of the data retrieved using the search terms. The data were selectively coded for information relating to current and emerging trends in healthcare and higher education (Table 1).
Results of PESTEL Coding and Analysis.

Note. PESTEL = politics, economics, society, technology, environment, and law.
Second Phase
Following the completion of the PESTEL coding and analysis, an analysis of curricula was undertaken to align the content of nursing programs with the results of the PESTEL analysis undertaken in the preceding phase.
The analysis was performed to ascertain nursing students’ quality of exposure to the future needs of the Australian healthcare system. Seven hundred seventeen discrete subjects were identified across all curricula sourced. Fifty-one subjects were coded as invalid data leaving 666 discrete subjects for analysis. Table 2 relates to the incidence of alignment between PESTEL categories and subject content.
PESTEL Factors Across Undergraduate Pre-Registration Nursing Subjects.
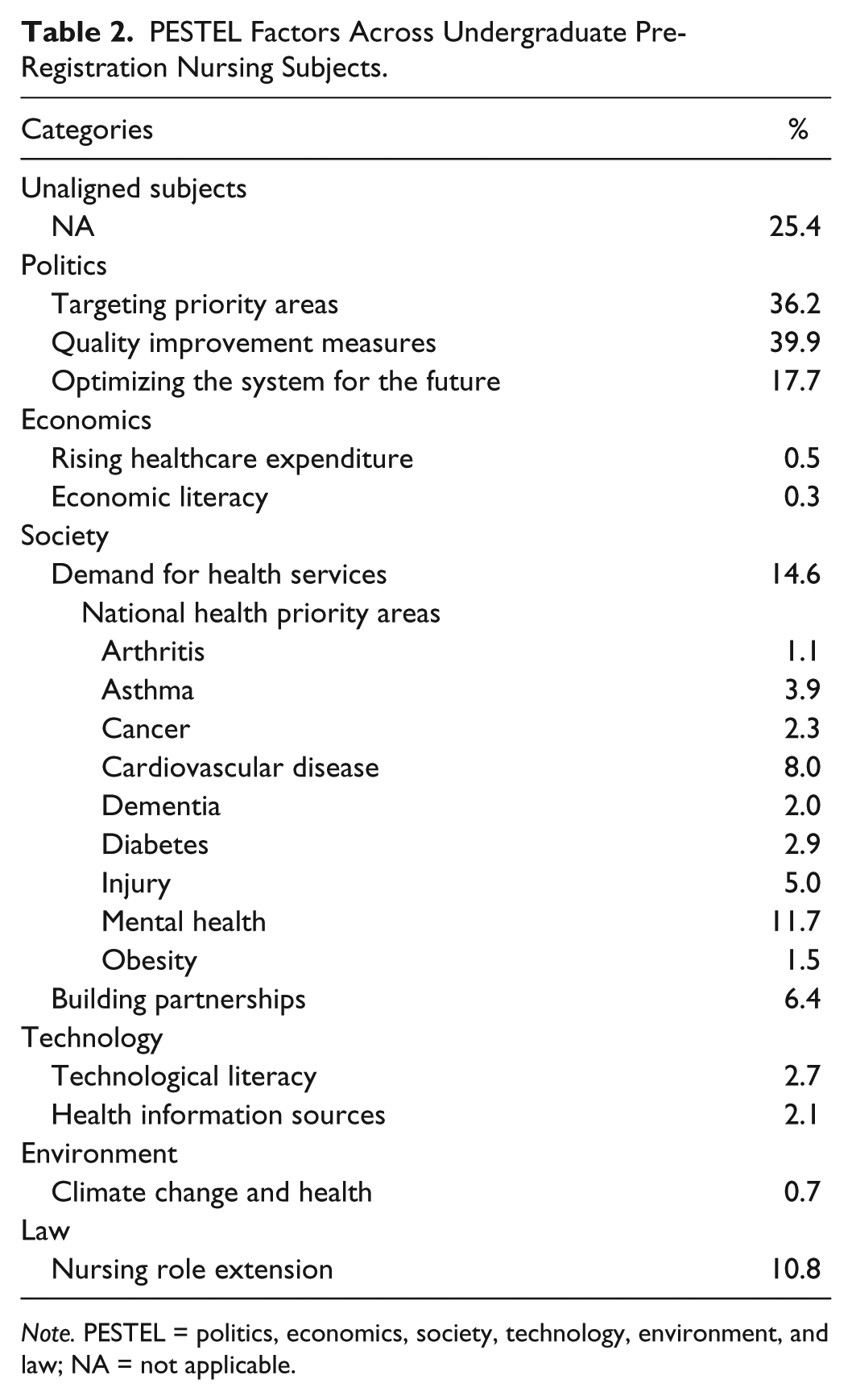
Note. PESTEL = politics, economics, society, technology, environment, and law; NA = not applicable.
Although the overall percentage of subjects aligned with the PESTEL analysis is indicative of the national emphasis on the emerging requirements for future nursing practice, an institution-by-institution breakdown of curriculum content was conducted to highlight the manner in which institutions prepare nursing students for future nursing practice. As such, PESTEL factors across institutional programs were graphed (Figure 1) to present the data on an institutional basis. The total number of institutions offering undergraduate pre-registration programs leading to registration was 34.

PESTEL factors across institutional programs.
Discussion
Politics
Although the findings have illustrated some clear challenges relevant to the nursing profession, the political landscape in relation to health is largely marked by reform. For instance, the National Health Reform Agenda features principally in the political macro-environment and offers insight into the present path dependencies of Australian healthcare in the future. Reform is centered on targeting priority areas such as Aboriginal and Torres Strait Islander (ATSI) health, remote and rural health outcomes and mental illness (AIHW, 2012). Further attention is given to quality improvement measures designed to enhance access, efficiency, and performance such as improved access to dental care, public hospital admission times, the establishment of national access targets, and the integration of strategies to embed prevention and early intervention (Australian Government, 2010). Strengthened consumer engagement and voice is central to this aspect of reform as the aim is to establish a healthcare system that is innovative, research centered, knowledge-led, and continuously improving (AIHW, 2012). Of note, is the reform agenda’s focus on optimizing the health system for the future as reference given to the need to respond to emerging challenges? Specifically, these challenges are seen as connecting and integrating health and aged care services; the arrival of the “next generation” of Medicare (Australia’s publically funded healthcare service); creating an agile and self-improving health system for long-term sustainability using data, information, and communication intelligently; improving the funding design and strategic purchasing throughout the system: all of which will be underpinned by a well-educated modern, learning, and supported workforce (AIHW, 2012; ANMAC, 2012; Australian Government, 2010).
The political agenda in higher education since the Bradley Review (Australian Government, 2008) has provided impetus for structural reform, increased funding and improved quality, equity, and access. Concurrent to reforms in the higher education; the healthcare sector has focused on building a sustainably funded, nationally unified, and locally controlled health system to achieve the goals of improving accessibility to health services and enhancing performance, transparency, and accountability (Australian Government, Department of Health and Ageing, 2010). Although time has not revealed the full effect of reform and its relationship to nursing and nursing education, the national trajectory of political direction is apparent. In optimizing the health system for the future, there is an expectation that health economics, health informatics, technology, health systems, quality improvement, performance, and care coordination will be featured more in undergraduate nursing education (ANMAC, 2012).
Registered nurses (RNs) will also need knowledge and experience in complex care, community, primary, and sub-acute health contexts as well as possess expert communication, teamwork, leadership, and coordination skills (Australian Government, 2010). Given the emerging priorities in education and health, it is certain that nursing education will need to be reviewed with renewed emphasis placed on ensuring programs of education are inclusive of the key priorities of reform. Already, changes are evident in pre-registration nursing education with the expectation that all curricula will include leadership and management, globalization of healthcare, and advanced level of clinical knowledge skills (HWA, 2012a). Embedding the political agenda as an informant of nursing education is essential to ensuring the congruency of direction for nursing education nationally.
Political agendas globally impact on health workforce recruitment and retention initiatives and drive education and training reform. The WHO, for example, responded to the identified global shortage of health professionals by developing a framework for action titled Transformative Scale Up of Health Professional Education (International Council of Nursing Education Network, 2013; WHO, 2011). This initiative heralded the need for changes to the education of health professionals and argued for the alignment of curricula with community needs, promoted the strengthening of graduates social accountabilities, and advocated the use of enhanced teaching technologies (WHO, 2011). The International Council of Nurses (ICN) Nursing Education Network in 2010 reported on the global nursing and health professional shortage highlighting the international trend for entry to practice for RNs at the bachelor’s degree level with a move from 3- to 4-year baccalaureate degrees (International Council of Nursing Education Network, 2013).
The implications of the political agenda for nursing education in Australia point to a healthcare sector undergoing significant changes, where clear service priorities are addressed in a more efficient, streamlined, performance driven system. The Australian Government predicts that RNs will need to prioritize knowledge and experience in complex care, community, primary, and sub-acute health contexts as well as expert communication, teamwork, leadership, and coordination skills (Australian Government, 2010). Whether there will be a gap between the preparation of nurses and the realities of practice in the future remains to be seen; however, the identification of different models of nursing education by leading bodies such as the ICN is a sign that structural changes are at the very least, being considered. Although a 4-year degree might appear an attractive solution, a better strategy might be to first explore what a generalist philosophy of education entails. Such an option may involve more prudent, evidence-based insertions of content into pre-registration curricula rather than simply extending the preparation over a longer period of time.
Economics
In recent years, the economics of Australian society and Australian healthcare have changed immensely. The global financial crisis has offered a timely reminder that economic forces ultimately influence the fiscal situation of any country, developed or otherwise. Healthcare is an expensive endeavor for any government, particularly those that fund national health schemes (Heller, Oros, & Durney-Crowley, 2014). In the coming years, the impact of economic forces will have an evident influence on the health of Australians. Kirigia, Nganda, Mwikisa, and Cardoso (2011) contend that there is significant evidence indicating that economic downturns result in reduced spending on healthcare, ultimately leading to poorer health outcomes with the most vulnerable most at risk.
Chiefly, the rising cost of healthcare is of great concern to the sustainability of funding the health system. Furthermore, the health workforce is growing exponentially with a 26% increase in size in the 5 years between 2005 and 2010 although the workforce is still experiencing shortages, particularly in nursing (AIHW, 2012; HWA, 2012b; Productivity Commission, 2005). Also contributing to rising healthcare expenditure are key cost drivers such as an emerging emphasis to educate and train even more health workers to adequately staff the health workforce not to mention the costs of concertedly addressing national health priority areas relevant to chronic disease, injury, and mental health (AIHW, 2012). A sustainably funded health system is top priority for all governments and health funding has become a contentious issue globally as well as nationally (Henry, Harmer, Piggot, Ridout, & Smith, 2009). The reality is that health funding is at a critical point and the Australian government continues to hotly debate its future. Nevertheless, there is no doubt that nurses will be central role-players in this environment as the rollout of local activity-based funding models are introduced across the nation (Independent Hospital Pricing Authority [IHPA], 2011). At an educational level, ANMAC have an expectation that nursing education will increasingly address the cost drivers of healthcare (ANMAC, 2012). The educational imperative for nurses to develop economic literacy is foundational to charting a course for a future in which the value of nurses is understood. In addition, the advancing practice agenda for nursing is a means of addressing other health professional number deficits. As nurses represent the largest proportion of the health workforce (HWA, 2012a) and are a more stable workforce, investing in up-skilling the profession is an economically savvy strategy, albeit one which is an untested assumption.
The cost of such a sizable nursing workforce—despite its shortages—is clearly problematic. Given that nurses are now financially recognized as a tertiary-educated, highly specialized profession there is—and will increasingly be—a clear political and economic expectation across the nation that their role in the healthcare system is filled rather than merely occupied. As the acuity of hospital care rises and moves toward enhancing the delivery of early intervention strategies to prevent the progression of illness via health promotion and primary healthcare, the nursing profession must become more specialized, expert, and lead increasingly complex care pathways in a technologically orientated setting.
These issues raise the question of size in the nursing workforce and whether at current levels, nurses are a sustainable entity. Questions should be asked about the position of the nursing profession in the health system and whether workforce growth has continued through a belief that the profession can be all things to all people. Further concern is found in the up-skilling of second- and third-level nurses to take on traditional RN roles; a situation that represents fiscal constraint at all costs. Although advancing the baccalaureate-educated RN workforce may be a costly exercise on the face of it, in reality, the result is a cost efficiency given the lower mortality rates comparative to settings where patients were cared for by non-baccalaureate educated nurses (Aiken et al., 2014). To this end, finding a way forward is essential for the nursing profession as it must avoid a situation that sees a decision-by-proxy made regarding future directions of nursing education in Australia. A recent international study examined the impact of patient to nurse ratios and nurse qualifications on risk adversity and patient outcomes in hospital settings. The findings confirmed that an increase in nurse workloads by one patient increased the likelihood of an inpatient dying within 30 days of admission (Aiken et al., 2014).
Society
In Australia, a number of social trends are emerging that will impact on the direction of nursing education across the nation. Primarily, the growth in Australia’s population from 22 million to 36 million by 2050 will result in a significant increase in the demand for health services (Australian Government, 2010). Heightened demand will coincide with an environment where the acuity of hospital admissions is intensifying as is the complexity of service delivery in the aged care sector (Productivity Commission, 2008). In particular, the nursing workforce requires a doubling of graduate completions to cope with expected demand (Australian Health Workforce Advisory Committee [AHWAC], 2004). Demand for hospital bed days is projected to grow faster and be increasingly allocated to older Australians with peak demand occurring as the baby boomer cohort pass into old age (Schofield & Earnest, 2006).
Another emerging priority is that of Australia’s aging population with more than 23% of the nation expected to be 65 years or over in 2050, up from 14% in 2010. Aging populations are a global phenomenon (Lutz, Sanderson, & Scherbov, 2008) forcing nations to reprioritize the focus of health policy, expenditure, and service delivery (National Research Council (US) Panel on a Research Agenda and New Data for an Ageing World, 2001; WHO, 2014a, 2014b). The AIHW contend that an aging population will require further attention from healthcare services and extend an already stretched aged care sector (AIHW, 2012). Practically, people living longer will see a trend toward briefer periods of morbidity prior to death meaning the onset of illness to death will be shorter than it is a present. Some perceive this trend as leading to an offset in health expenditure across the lifetime (Caley & Sidhu, 2011; Coory, 2004). Irrespective of the results, the need to urgently expand the health workforce is apparent. In particular, enhancing the aged care workforce to remediate the age-induced tightening of the labor market and competition from the hospitals sector is a priority (Productivity Commission, 2005).
Although the current system can be applauded, it is not without its challenges. In some areas, significant improvements have been made such as the reduction in smoking rates while action is needed in improving the health of ATSI people (AIHW, 2012). Of great concern are the nine National Health Priority Areas identified, namely, arthritis and osteoporosis, asthma, cancer, cardiovascular disease, diabetes, injury, mental health, obesity, and dementia (Australian Government, 2012). That arthritis, asthma, cancer, cardiovascular disease, dementia, diabetes, and obesity do not feature in the subject titles, subject synopses, or learning outcomes of over half of the 34 nursing programs in Australia is a significant concern. That mental health features in 57 discrete courses is an oddity given the mortality and morbidity more strongly associated with other national health priority areas. Historically, mental health has always attracted the attention of a discrete subject; however, if the relics of the past are informing our planning for the future, the foundations on which nursing education is built are treacherous at the least.
Part of the response to build a workforce for the future will be to approach healthcare through building partnerships with the wider community, which was championed as the way forward by the WHO in 2011 (WHO, 2011). The need to afford health consumers more choice and to make health information more accessible and translatable to the wider public is essential because demand for services is projected to rise (Koch, Nay, Mcauliffe, & Koch, 2008). Although some may express unease that social action smacks of social engineering, the nurse has a responsibility to do what they can to improve the health of society and address health inequalities (Marmot, Allen, Bell, & Goldblatt, 2011; WHO, 2011). By functioning as natural attorneys of a nation’s health, partnerships between nurses and citizens must be established in the continuum of decision-making processes where the delivery of healthcare is concerned. The mainstream healthcare system must effectively extend its accessibility to those living in outer metropolitan, rural, and remote areas and in indigenous communities (Productivity Commission, 2005).
Despite efforts to enhance access to health services, the means of achieving this goal are unclear as the future of the nursing profession is marked by significant projected workforce shortages that could impede any meaningful response. The nursing workforce is experiencing shortages that are projected to worsen despite significant increases in graduate numbers and an increasing reliance on overseas-trained health workers to overcome shortfalls (HWA, 2012a; Productivity Commission, 2005). The shortages are even more acute in rural and remote areas and in certain special needs sectors (HWA, 2012a).
In this context, nursing feasibly has three options: (a) continue on its current trajectory, (b) massively increase student intake in undergraduate pre-registration programs, or (c) redefine the nursing role to that of a highly specialized, more focused profession. In view of present and emerging challenges, nursing might not be able to provide expertise in as many contexts as it presently does. These options contrast with the position of the Council of Deans of Nursing and Midwifery (2005) who state that the nursing shortage can only be addressed by changes to workplace relations and conditions. Given the lack of discussion around the future of nursing and nursing education, any decisions may well be colored by politically expedient quick fixes to workforce shortages rather than a serious debate on the strengths and limitations of the nursing workforce nationally.
Fundamentally, the Australian nursing profession must decide whether they wish to be seen politically and professionally as a highly expert, tertiary-educated profession or whether they wish to be seen as a political quick-fix to national workforce shortages. Whatever the course, nursing education will be central to shaping the future foci of the profession and defining the extent and scope of the nursing role in a healthcare system confronting significant emerging and future challenges.
Technology
Central to the future directions of healthcare nationally is the widespread acceptance that technology will play a crucial role in the success of implementing reform and enhancing efficiency, safety, and the continued sustainability of healthcare in Australia (Banks, 2008). Already, significant movements toward the “technologification” of healthcare are happening in response to the increasing expectations that Australians have toward healthcare accessibility (FitzGerald & Ashby, 2010). At a national level, geo-tagging the health of Australians is informing the creation of an Australian Diabetes Map, while “big data” projects such as the Western Australian Data Linkage system are influencing the delivery of state-based healthcare by informing approaches to research, planning, and evaluation through the identification of health trends within the population (“Australia’s Digital Economy: Future Directions,” 2009).
The role of technology as an efficient connecting interface between clinician and consumer is foundational to the partnerships that must be built to enhance the accessibility and effectiveness of healthcare throughout Australia. Central to this process is the requirement for investments to be made in developing the technological skills of the health workforce along with the improving the quality of models of care used in a technology centric environment (Banks, 2008) and of renewing required infrastructure. Given the continued reliance on manual processes and information flows in a system that daily reports 342,000 visits to general practitioners, 742,000 medications dispensed in pharmacies, 23,000 hospital admissions, and 17,000 emergency department presentations (AIHW, 2012; National E-Health Strategy, 2008), the opportunity to utilize technology to reduce errors and system inefficiencies is an exciting prospect.
Clearly, technology will play a significant role in the future delivery of Australian healthcare with emphasis placed on information sharing, developing service delivery tools and providing meaningful health information sources for clinicians and consumers (National E-Health Strategy, 2008). Technological literacy will center on ways of improving information flows between care providers to provide a foundation for enhancing care planning, coordination and decision making at the point of care. Already in the current technological environment, healthcare practitioners are able to send digitized medical images of patient records to where the patient is. Such records are now stored online and networked throughout the facility giving clinicians opportunity to check and update patient information anywhere in the facility at any time (“Australia’s Digital Economy: Future Directions,” 2009). Technology literacy will be central to enhancing clinical decision making to reduce adverse events, or enable timely identification and monitoring of care needs (National E-Health Strategy, 2008). At its most advanced, this concept embraces the detection and treatment of disease through technological advances (National E-Health Strategy, 2008), while the pragmatic side of service delivery tools leads to the integration of evidence-informed knowledge in the care process using technology (Pfeiffer, 2009).
Although it is an expectation that graduates are able to use information systems, preparing nurses for the technological contexts in which they will work does not feature in many curricula. Axley (2008) reported that there has been a rapid expansion of the use of technology in healthcare in the United States and highlighted that nursing curriculum has not kept pace with this phenomenon. She asserted that skill levels of academic staff teaching nursing students was a barrier to technology featuring in nursing curriculum (Axley, 2008). The digital age is a feature of the 21st century (Heller et al., 2014) and mandates that educators adopt new practices in preparing nursing students for the realities of the workplace (Simpson, 2011). Johns Hopkins University School of Nursing introduced electronic patient records as a feature of their simulating learning spaces and teaching techniques following recognition that their program was failing to prepare students adequately for practice as graduate nurses (Birz, 2005). Whatever the solution, answers to any lack of technological literacy in nursing will likely focus on enhancing the abilities of students and staff in becoming more adept at responding to increasingly technologically demanding contexts of care.
Environment
The broader environment in which we live has and continues to have a profound impact on the healthcare of all Australians. At a global level, climate change and health is inextricably linked as it will bring changing patterns of disease, natural resource insecurity, extreme weather events, and population growth and migration (Costello et al., 2009; Hughes & McMichael, 2011). Environmental events will likely drive an emphasis on building capacity in the nursing profession to respond to natural disasters, vector-borne illnesses; food shortages and occasions when infrastructure breakdowns impact on health (Costello et al., 2009; Oven et al., 2012). Catastrophic events will not require a team of disaster nurses but huge numbers of the nursing workforce to provide a sufficient response to the situation and maintain appropriate levels of operation on the “home front.” Already Pacific Islanders are seeing the effects of global warming and communities are preparing for eventual evacuation and consequent destruction of their societies. As a leading nation in the Pacific region, Australia will be central to the regional expectations of our neighbors as the first responder in times of crisis. As the future will be characterized by deepening stresses between human activities and wider ecosystems (Henry et al., 2009), some of the onus for responding to the impacts of climate change will fall to nurses. It will therefore be necessary for nurses to develop environmentally conscious curricula in view of such looming stressors in the form of disaster nursing. Given the geographically distributed nature of the workforce—the relative number of health professionals other than nurses diminishes as the distance from cities increases (Productivity Commission, 2005)—it is critical to increase the efficiency and effectiveness of the available health workforce, and to improve its distribution if nursing is to position itself as a responsive, mobile, highly expert profession central to the health of the nation.
Law
The presiding dominance of the medical profession over many elements of the healthcare system and by implication, the nursing role, needs to be strongly questioned. Although medicine has and continues to answer vital questions with respect to the future context of healthcare, its undue influence on nursing and nurses’ scope of practice is limiting. It is an unfortunate state of affairs when it is recognized that nursing role extension usually occurs as nursing knowledge and roles develop. Role extension has occurred as a mechanism for medical staff shortages in rural and remote areas; in response to changes in models of care; and as a means of answering unmet patient needs requiring different skills; and in reaction to the introduction of new technology (Duffield, Gardner, Chang, Fry, & Stasa, 2011). Any expansion in scope of practice may present complex legal and ethical dilemmas; however, nurses should not act as a stopgap to limitations in the service delivery capacity of the medical profession (Linsley, Kane, Mckinnon, Spencer, & Simpson, 2008). Nevertheless, the versatility of the profession is such that nurses assume the function of stopgaps with regularity. The premise of teaching nurses their legal and ethical obligations in the context of the health system (ANMAC, 2012) should be expanded to include their responsibility to agitate for legislative reform to legitimate the development and expansion of the nursing role in Australia. At a fundamental level, the challenges ought to be addressed with the patient as the center of care while acknowledging the basic right of access to healthcare for all Australians (Bennett, 2009).
Furthermore, nurses can no longer hide behind the traditional hierarchical dominance of the medical profession as protection from civil or criminal legal action. The pursuit for professional status has brought with it an accountability that sees nurses liable for actions performed as part of the normal scope of their professional role. If we are to respond to the multiplicity of health priorities in Australia while ensuring the integrity of our professional identity, we must start with the basics and empower a new generation of nurses to be legally and politically savvy. Legal impetus for the establishment of a future direction for the professional position must start at educating nurses so as to prevent the passive attitude that has led to legal restrictions being placed on nurses’ scope of practice. We must recognize that legally, the profession cannot optimally facilitate the transformation of healthcare in the future while being dominated by the legal restrictiveness that ties the nursing role to a level subordinate of medicine or any other health profession. Whether nursing education can be tailored to form the foundations of such legal impetus, transformative of the nursing role is unknown. Without doubt, it must at least be attempted.
Limitations
The main limitation in this study related to the diversity of quantity and quality of publically available information pertaining to pre-registration nursing curricula. Differences in the minimum information requirements of course profiles, objectives, and synopses among higher education providers may have limited the analysis, as it is difficult to determine the coverage of PESTEL factors in teaching resources outside of formalized curriculum documents. Nevertheless, when factors such as national health priorities are prescribed by the national accreditation standards (ANMAC, 2012) yet not included in available program information, it opens up the possibility for preparation–practice gaps within undergraduate pre-registration nursing programs.
Recommendations
Although solutions to any complex problems are often clear, simple, and wrong, we propose a number of recommendations to address the issues raised in this article:
A nationally consistent approach is needed to systematically identifying current and emerging trends impacting on healthcare and higher education, including a means of interpreting their relevance to undergraduate pre-registration nursing education programs.
An evidence-based framework should be implemented that can facilitate undergraduate pre-registration nursing curriculum design to future proof the current system of nursing education. The framework would cater to the modification of curricula only where it is relevant to verifiable current and emerging trends; congruent with the nursing role; in keeping with the generalist philosophy of nursing education; and according to the priorities of health consumers’ needs.
Conclusion
The nursing profession must—if it is to successfully transition into the 21st century—decide what nursing education and indeed nursing, needs to be. The belief that nurses can be all things to all people is unrealistic. The expectations of political, economic social, technological, environmental, and legal agendas are centered on nursing evolving into a highly educated, expert, specialized, mobile, well-remunerated nursing workforce. En masse, such an ideal is not financially sustainable. Philosophically, a shift away from anything else but role extension professionally, is anathema to the core reasons for shifting nursing into the university sphere of education. The array of confusing, paradoxical, and inconsistent approaches to undergraduate pre-registration nursing programs is evidence of a profession unsure of itself and largely unaware of how to establish a system of quality education that underpins a quality profession. In this context, the sensibility of a nationally consistent approach to nursing seems apparent. As a new system of national accreditation is ushered in, the time is right to establish a cogent strategy founded in the national domain that offers solutions to nursing’s position in the Australian healthcare context. As little and as much is necessary if we are to ensure that the future-proofing of nursing education in Australia is a successful process. Ensuring that Australia’s nursing workforce is well prepared to meet the demands of the future may mean either extending the minimum course length or enhancing the decision making around what content should be included. Investing in post-graduate education of nurses and development of an appropriate career pathway will support alignment of the workforce capacity with national need. Curriculum content must be nationally and globally relevant to future-proof nursing education in Australia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.