
Abstract
OBJECTIVES
Virtual care (VC) is increasingly becoming a part of emergency medicine (EM) physician workflows, yet no formal digital health curricula exist within Canadian EM training programs. The objective was to design and pilot a VC elective rotation for EM residents to help address this gap and better prepare them for future VC practice.
METHODS
The current work describes the design and implementation of a 4-week VC elective rotation for EM residents. The rotation consisted of VC shifts, medical transport shifts, one-on-one discussions with various stakeholders, weekly thematic articles, and a final project deliverable.
RESULTS
The rotation was well received by all stakeholders, and the quality of feedback and one-on-one teaching were highlighted as strengths. Future work will consider the optimal delivery timing of this type of curricula, whether all EM residents should receive basic training in VC, and how our current findings may be generalizable to other VC sites.
CONCLUSION
A formal digital health curriculum for EM residents supports competency development for delivering VC as part of future EM practice.
Introduction
While emergency medicine (EM) physicians have engaged in telemedicine through paramedic patching for direction and oversight of delegated medical acts and transport services for decades, 1 the COVID-19 pandemic catalyzed digital healthcare access. 2 Virtual care (VC) is becoming integral to many specialties’ practices. Physicians are now expected to demonstrate VC competency, yet few have received any formal training in this area.2,3
Throughout the pandemic, a likely fallible assumption is that healthcare providers can simply shift their in-person skills to virtual encounters immediately.2–5 While some clinical and nonclinical skills may transfer quite readily, other elements of VC are less intuitive and require new skill acquisition (ie, virtual doctor–patient communication, conducting a virtually facilitated physical exam, and troubleshooting technology challenges). No formal digital health curricula within Canadian EM residency training programs have been previously reported.
Purpose/Rationale
Throughout the pandemic, multiple residents from both EM certification programs reached out seeking opportunities to learn about digital health and VC delivery. This led to a local needs assessment of current VC EM physicians that revealed opportunities for further training. Consequently, we designed and piloted a VC elective rotation for EM residents to help address this gap and better prepare them for future VC practice.
Methods
A 6-step approach to curriculum development, similar to Kern's model, was used. 6 Ethical approval was received from the Sunnybrook Health Sciences Centre Research Ethics Board (REB). Verbal informed consent, as approved by the REB, was obtained from participants to comply with institutional pandemic physical distancing guidelines.
Performing a needs assessment and writing a rationale statement
A literature review to identify current training programs and organizational guiding documents (eg, the College of Physicians and Surgeons of Ontario and the Canadian Medical Protective Association) revealed a lack of formal training and highlighted expectations for physicians practicing in VC. A mixed-methods needs assessment was completed by a convenience sample of 8 EM physicians who regularly work in the VC ED. Results showed a neutral comfort level before starting VC (median of 3 on a 5-point Likert scale) increasing to a very comfortable level after a few months of VC practice (median 5). Some of the identified themes included learning how to conduct VC assessments, knowing the limitations of VC, navigating VC in the context of the broader healthcare system, and expressing medico-legal concerns (online Supplemental material file 1).
One-on-one meetings and email correspondence were used to determine the resident's learning goals and needs. These learning goals, such as “becoming comfortable with providing virtual consultations” and “exploring academic possibilities in this field, including research and curriculum development”, were incorporated into the curriculum.
Determining and prioritizing content
The core topics for the rotation were developed from the needs assessment, organizational guiding documents, and local expertise in VC. These included confidentiality, medico-legal considerations, quality and patient safety, and digital equity.
Writing goals and objectives
Goals and objectives were developed, balancing resident perceived needs with the needs assessment feedback and expectations from guiding organizations. While competencies from both EM certification streams may apply to the VC domain, there were no specific VC competencies to help guide the rotation's objectives.7,8
Selecting teaching/educational strategies
The rotation combined clinical, didactic, and self-directed learning. VC shifts allowed for practical application with real-time feedback from faculty who directly observed the resident's assessment of patients and reviewed proposed management plans. One-on-one meetings with VC physician providers, operational leaders, and policymakers around selected topics provided insight into designing, implementing, and evaluating VC at different sites. Weekly themed articles were assigned with the opportunity to discuss these in further detail with the rotation preceptor.
Implementing the curriculum
The 4-week elective was piloted from April to May 2022 with a University of Toronto EM second-year resident (Toronto, Canada) (Figure 1). The rotation consisted of 8 VC shifts (at two different hospital sites), 4 medical transport (Ornge) shifts, 8 one-on-one discussions with various VC stakeholders, weekly VC-themed articles, and a final project (a presentation or reflection piece at the resident's discretion).

Emergency medicine (EM) virtual care (VC) curriculum outline with rotation goals and weekly themes.
Results
Evaluating and applying lessons learned
Evaluation of the rotation consisted of multiple sources, including a rotation evaluation questionnaire (compulsory for all University of Toronto residency program rotations), faculty feedback from each provider who directly observed the resident for both VC and medical transport shifts including entrustable professional activity (EPA) completion, an exit interview with the rotation preceptor, and a review of the final project. While the rotation evaluation questionnaire is not validated, it is the standard evaluation tool for postgraduate residents to provide feedback on their rotations. Overall, the rotation was well received by all stakeholders. The resident gave the rotation 5 out of 5 on their final program evaluation (Table 1 for narrative feedback). The resident valued the opportunity to target the elective toward their learning goals and appreciated the broad exposure and diversity of the elective. This experience highlighted the importance of involving residents as key stakeholders in their learning, especially in emerging fields like VC, where creativity and innovation are encouraged.
Selected resident narrative comments from the rotation exit interview.
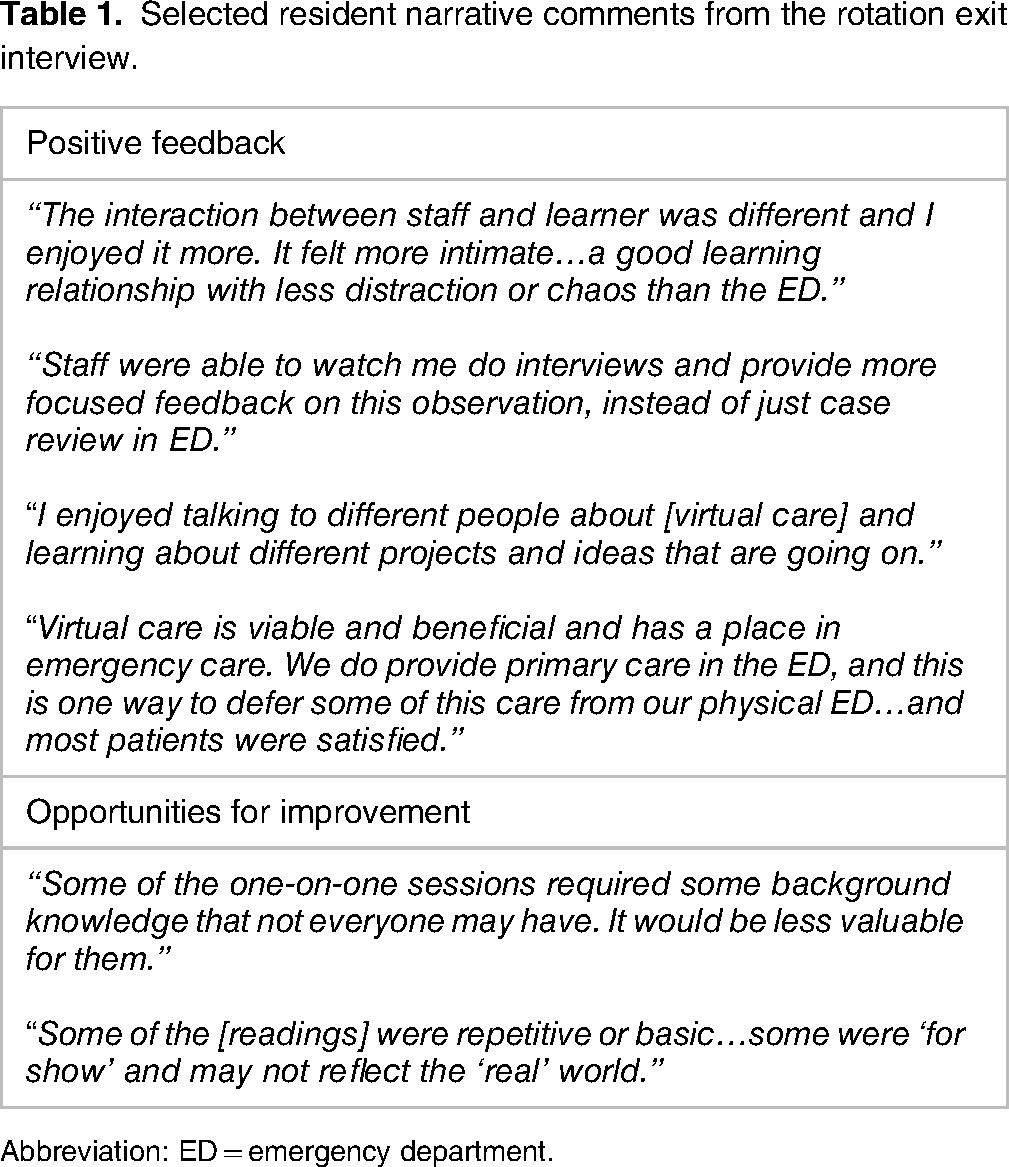
Abbreviation: ED = emergency department.
The resident valued the opportunity to target the elective toward their learning goals and appreciated the broad exposure and diversity of the elective. In the exit interview, they stated: “I really enjoyed coming up with the learning objectives together. It didn’t feel like they were just forced on me.”
Moreover, they valued the close interaction with faculty. They noted it was a more intimate environment with fewer distractions and less “chaos” than the emergency department. As a result, they felt that the learning environment was improved and that supervisors were able to provide closer observation and more meaningful feedback. Furthermore, they appreciated the differences in approaching clinical presentations in this unique setting and how to overcome some of the challenges associated with VC (eg, learning how to instruct a patient to conduct a self-examination).
The resident also provided constructive feedback to help improve the rotation. They noted there was variation in the one-on-one meetings with VC physician providers, operational leaders, and policymakers with respect to required background knowledge. They felt that some of these meetings required a baseline knowledge of the area to gain the most value from the discussion. In addition, they noted that coming to these sessions with questions about the faculty's role or area of expertise were helpful in driving the conversation. They stated: “People may come to just ‘check the rotation out’ and won’t know what they don’t know. So they may need more structure for these [one-on-one] sessions.”
VC faculty member rotation feedback was largely positive. In general, faculty members indicated they would welcome residents on future shifts and saw the value in offering this type of training to our EM trainees as an important competency for future practice (and one that they had not received themselves). A couple of VC faculty members indicated that this type of training would be most suitable for senior residents or those transitioning to practice. One representative quotation is: “Senior residents are likely to benefit most from this type of rotation where they have to think critically about management plans that balance timeliness, risk, and quality of care.”
Discussion
The implementation of an EM VC elective offered multiple lessons. First, this experience highlighted the importance of involving residents as key stakeholders in their learning, especially in emerging fields like VC, where creativity and innovation are encouraged. The resident was engaged and motivated as they felt they were an active member in their learning. Furthermore, the elective provided the resident with a foundational understanding of the critical role that EM physicians play as gatekeepers of the healthcare system. Specifically, they refined their knowledge and decision-making around the urgency of presenting complaints and the need for follow-up (eg, transfer to in-person emergency department (ED), arrange urgent follow-up, reassurance, or recommendation to wait for their primary care provider). Moreover, having both the resident and staff physician present during the assessment enhanced the efficiency of the case review. An unexpected lesson learned was how valuable it was for the resident to directly observe staff EM physicians conduct assessments and then apply their observations to subsequent patient encounters. Iterative direct observation and then timely application resulted in a positive feedback loop for improved resident performance. This finding provides support for the importance of direct observation as related to EPAs and demonstration of competence. 9 Finally, the depth and quality of shift feedback were perceived to be more focused and helpful than on regular in-person ED shifts. This was likely due to a more controlled environment with fewer interruptions and less noise than the typical ED.
Several opportunities exist for future enhancements. As part of this experience, the junior resident completed 2 core EPAs related to differentiating, diagnosing, and managing patients with emergent, urgent, and nonurgent patient presentations. There is an opportunity to align rotation objectives to more senior-level competencies, such as departmental management and integration of health informatics to enhance patient care and safety. Another potential advantage of this shift in timing is that case discussion would be centered around the capabilities and challenges of VC delivery and the use of digital tools as part of healthcare assessments rather than reviewing core medical knowledge. Similarly, the rotation coordinators can review future residents’ foundational knowledge in VC to determine appropriate articles and one-on-one discussion topics to meet their needs. A further consideration is to determine the degree of integration within residency training that is most appropriate: core block content for all residents, longitudinal exposure across multiple stages of training, or as an elective rotation.
There are a few important limitations of the current work. First, if the VC curriculum were to become core EM content, careful consideration is needed given competing curricular content and limited time within residency training programs. If a core rotation is not possible, programs could consider integrating this training longitudinally or combining VC with a core in-person EM rotation. The second limitation is that local VC programs are not available to all EM training program sites, and even if one is accessible, there may not be sufficient faculty expertise or resources to take on trainees. The digital nature of the rotation could mitigate this as residents do not need to be physically present in the same location as the local VC site. While the rotation evaluation questionnaire used in this study is standard for all rotations within the residency program, it is not a validated tool, which may limit its applicability in other settings. Finally, the pilot elective involved 3 different VC sites and 1 EM resident. While we believe our curriculum could be adapted elsewhere, the generalizability of our findings and transferability of the rotation is unknown.
Conclusion
As VC becomes increasingly integrated into EM, our elective rotation provides residents with an opportunity to better prepare themselves for future VC practice. Other sites may use this rotation as a foundation to implement VC in their EM training programs. As VC evolves, further consideration should be made to align residency training with the needs of our future practicing EM physicians.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231165183 - Supplemental material for Training Residents for the Future: A Virtual Care Rotation for Emergency Medicine
Supplemental material, sj-pdf-1-mde-10.1177_23821205231165183 for Training Residents for the Future: A Virtual Care Rotation for Emergency Medicine by Justin N Hall and Lorne L Costello in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank all of the team members who worked with the resident to make this rotation a valuable learning experience.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.