
Abstract
Burnout has become an increasingly recognized problem in higher medical education and is particularly prevalent within the field of Neurology and its training programs. Many previously reported wellness initiatives in other residencies focused mainly on community/team building. We developed a comprehensive Wellness Curriculum (WC) and established a new role of Resident Wellness Liaison in order to facilitate wellness across the department and training program. Here we present a 6-step outline of our WC which can easily be adapted to the needs of other programs. The steps include creating a Wellness Committee with a Resident Wellness Liaison, identification and optimization of institutional resources, identifying and troubleshooting barriers to wellness, providing education and reflection on wellness, showing appreciation to each other, and assessing the impact of the implemented strategies. In order to measure the impact of our WC and to perform a needs assessment for future directions, we posed questions—grounded in the theory of drivers of burnout and engagement—to our residents (N = 24) at a noon conference in the summer of 2020. Interventions implemented at our institution have been very well received by residents, as evidenced by their comments and feedback. Themes that were highlighted by residents include enjoying flexibility, having a welcoming social support system at work, and being able to find meaning in the day-to-day work. The creation of a comprehensive WC is a feasible and meaningful intervention for addressing resident wellness in a Neurology training program and could be adapted to other programs.
Introduction
Psychological, emotional, and physical well-being are critical in developing competent, caring, and resilient physicians. Well-being’s converse is “burnout,” which entails: emotional exhaustion, depersonalization, and career dissatisfaction. 1 Neurology rates third highest in burnout amongst 25 medical specialties. 2 Burnout is even more prevalent in Neurology trainees, with 73% of residents and 55% of fellows experiencing at least 1 symptom of burnout. 3 In 2017, the Accreditation Council for Graduate Medical Education (ACGME) issued a requirement of all accredited residency and fellowship programs to address well-being comprehensively. Burnout among residents and fellows negatively impacts the learning environment, incidence of medical errors, personal life, and ability to provide care. 4 Additionally, physician wellness impacts the doctor-patient relationship. 5 In response to the above, we developed a Wellness Curriculum (WC) and established a new role of the Resident Wellness Liaison. Here we present a 6-step outline of our WC which can easily be adapted to the needs of other programs.
Methods
The Neurology WC was designed to address well-being in the setting of a Neurology training program and included 6 steps to improve the resident training environment (which includes the community of patients, colleagues, and families). We aimed to minimize administrative tasks, promote progressive autonomy, enhance professional relationships, and educate residents and faculty on identifying symptoms of burnout and assisting those who experience symptoms of burnout, fatigue, depression or other related conditions.
Step 1: Development of Wellness Committee and Resident Wellness Liaison
A Wellness Committee was created in July 2017 to better facilitate wellness across the department. This comprises the Neurology Program Director (PD), Associate Program Director (APD), additional faculty (including Fellowship Directors), Chief Residents, and Resident Wellness Liaison, a role formalized in June 2018. The Resident Wellness Liaison is a second year Neurology resident, selected yearly in the early Spring, responsible for planning wellness-related activities, attending committee quarterly meetings, creating the wellness newsletter, alerting residents to wellness-related events and resources, and evaluating for structural and organizational changes within the residency to optimize wellness.
Step 2: Identification and Optimization of Institutional Resources
Utilizing preexisting resources from the parent medical system and GME office avoids redundancy of efforts. At our institution, this includes free mental health support and resources (including marriage counseling) covered by the trainee insurance plan. Additional wellness benefits include sleep services, napping and fitness rooms, gym memberships, and wellness classes. It is important to ensure residents are aware of these institutional resources and how to access them—this is done at orientation.
Step 3: Identify and Troubleshoot Barriers to Wellness
To better serve our resident community, the Wellness Committee identified key barriers to wellness, via survey, literature analysis and resident work groups. We then brainstormed interventions, as seen in Table 1, which focus on specific aspects of daily life that are identified by the residents as most likely to induce burnout. This has been an iterative, ongoing process since the inception of the Wellness Committee in July 2017. Less stressful job demands, finding meaning, strong social support, and accessibility to give feedback are important. Within the category of job demands, our residency program transitioned in July 2018 from having a single resident on-call overnight covering all services to a “buddy system” where a junior resident is paired with a senior resident, both of whom are in-house. This 2-person night float system allows the junior to see cases up front and then staff with the senior resident, simultaneously affording both residents unique learning opportunities (eg, active management decisions for the junior and learning to staff a case for the senior). Additionally, the change ensured greater resident availability in the case of simultaneous neurologic emergencies, for example, 2 stroke codes occurring at once, which has obvious benefits to patient care. This shift from single resident to buddy system overnight coverage was made solely as a result of direct resident feedback to program leadership and thus is a good example of the importance of accessible feedback mechanisms in reducing stressful job demands.
Identified barriers to wellness within our neurology residency and the interventions that were implemented to combat against them.

Another example of an iterative change made through resident feedback was elimination of the 24-hour call in the spring of 2020, which previously took place at the end of a week of night shifts. Given the challenging transition from night shifts to a 24-hour shift occurring during the day (as well as the inherent challenges of a 24-hour shift), our former wellness liaison worked with the chief residents and program leadership to restructure this system. We now have a separate resident on-call for the day shift portion of that previously 24-hour shift. One unanticipated challenge that arose from this new system was that this day-call shift tends to be very active (frequently greater than 10 new consults per shift). The chief residents and wellness liaison thus polled the residents for potential solutions at a noon conference in spring 2020, and we instituted in-house backup for the day-call resident via the resident covering stroke and ICU consults that day.
Other interventions addressing barriers to wellness have taken less of a structured approach but are nevertheless important. For instance, as major life events come up throughout the year, our residents can coordinate shift swaps with one another in order to attend these crucial events. Additionally, the scheduling chief resident takes such events into account at the beginning of the academic year when making the schedule.
Step 4: Provide Education and Reflection on Wellness
Residents and faculty are given the tools to identify burnout, access mental health resources, and evaluate variables in our environment that either promote or impede wellness. One intervention was “joy rounds,” first initiated on our inpatient services in spring of 2020, where teams would pause daily to reflect on what had brought them joy. 6 We also engaged faculty through half-day retreats during which clinics are cancelled that create awareness of the importance of resident wellness. At Neurology resident orientation, there are dedicated lectures geared toward identifying burnout, sleep hygiene, and wellness principles. The residency program also provided monetary support by purchasing books, snacks, fleeces, and arranging wellness retreats. Our program receives dedicated funds from GME for resident wellness/social events, and we additionally have a social budget through our Neurology department. The PD, APD, and other faculty also contribute ad hoc.
Step 5: Show Appreciation
The Wellness Newsletter was developed in July 2018 to recognize praiseworthy actions by residents to increase self-efficacy and decrease burnout. It is a monthly periodical with photographs of trainees having fun both in and outside of work, kudos for noteworthy patient interactions or professional accomplishments, and congratulations on major life events. Residents who have difficulty finding meaning in day-to-day work are logically more likely to experience burnout. As with joy rounds, sharing praise from patients, nurses, peers, and attendings can impact how residents perceive their importance. Small gestures such as snacks and beverages provide small, yet crucial moral support throughout the day and free lunches also allow for residents to pause, refuel, eat, and learn together.
Step 6: Assess the Impact of Your WC
In order to measure the impact of our WC and to perform a needs assessment, we utilized subjective reporting from our residents. We chose a qualitative approach given its overall strengths compared to the significant limitations of a quantitative approach in the study of well-being. 7 We developed questions to pose to our residents (N = 24) at a noon conference in the summer of 2020, grounded in the theory of drivers of burnout and engagement by Shanafelt and Noseworthy. 8 These questions were posed after the described interventions were already enacted; however, as described above, similar noon conference polling and other more informal discussions have taken place in an iterative fashion since the inception of the Wellness Committee in July 2017. The project was deemed by authors to be exempt from institutional review board (IRB) review based on Northwestern University IRB Exempt Review Category 1 (https://www.irb.northwestern.edu/exempt-review/), as the surveys were conducted in an educational setting involving curricular changes that were unlikely to adversely impact residents. The intervention was thus not taken to the IRB.
Results
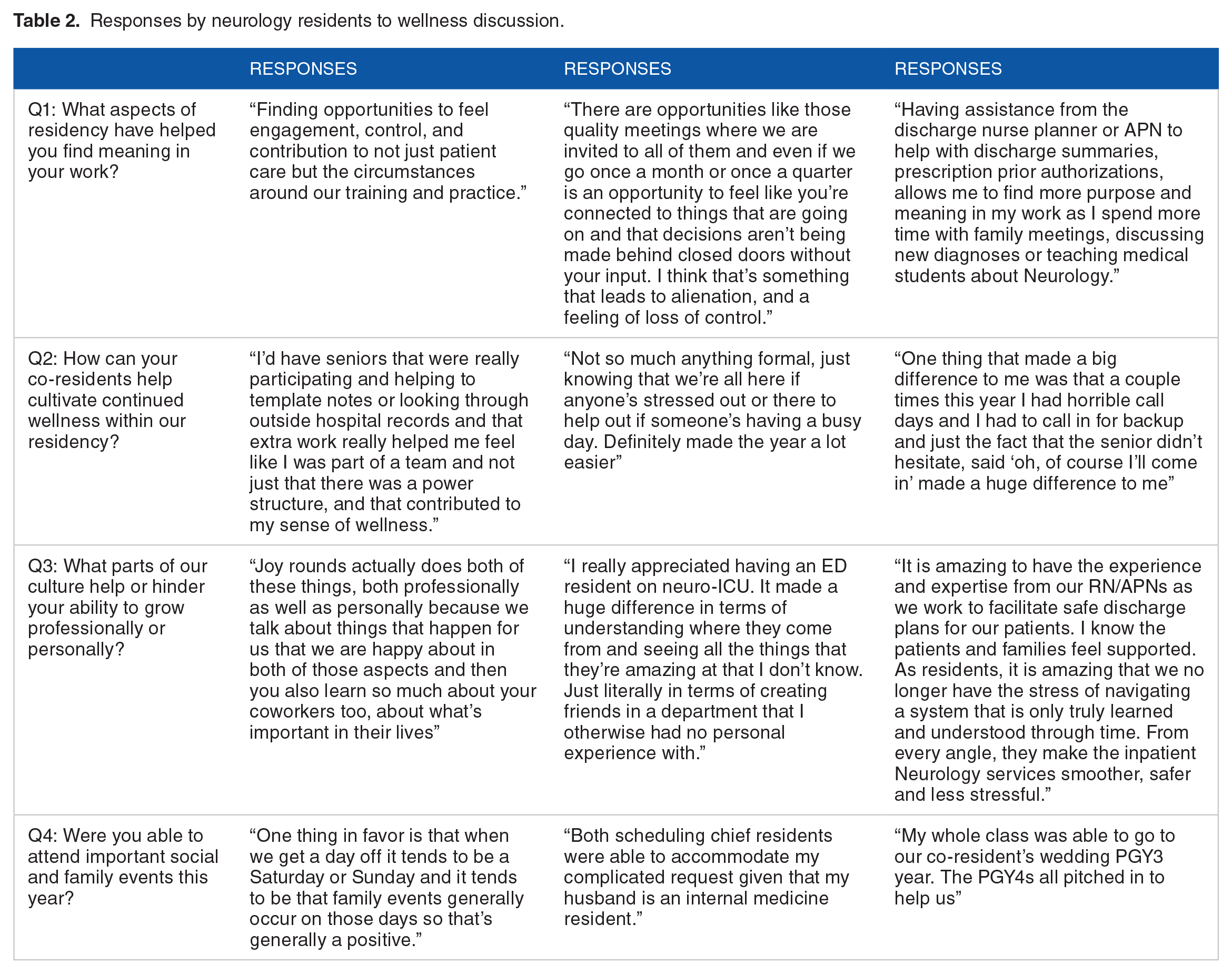
Representative responses from our Neurology residents are highlighted in Table 2, and full list of responses is found in Supplemental Appendix, paraphrased for brevity. Themes that were highlighted by residents include enjoying flexibility, having a welcoming social support system at work, and being able to find meaning in the day-to-day work.
Responses by neurology residents to wellness discussion.
Discussion
Our program has successfully designed and implemented a 6-step WC that can be shared with other programs. The steps include creating a Wellness Committee with a Resident Wellness Liaison, optimization of institutional resources, identifying and troubleshooting barriers to wellness, providing education and reflection on wellness, showing appreciation to each other, and assessing the impact. Many previously reported wellness initiatives in other residencies seemed to primarily focus on community/team building.9-12 A dedicated WC should make use of institutional resources but also be innovative in engaging residents and faculty in meaningful reflection and identifying/preventing signs of burnout. Support from faculty at the highest level of departmental leadership is important for the sustained success of a wellness program 13 and this model was recently demonstrated in the Department of Neurology at the Mayo Clinic. 14 Neurology is associated with high rates of burnout, and culture shifts need to take place at the organizational level to address aspects of training which lead to this burnout. From the trainee perspective, this includes emphasis on work-life balance, and dedication to education. Having wellness events and retreats are can be helpful in forming community. Ultimately, finding ways to make daily work more meaningful (such as joy rounds and kudos newsletters), and creating a culture of kindness is at the core of this curriculum. Additionally, accessible feedback mechanisms to receptive program leadership are crucial to making iterative changes to a residency program.
A qualitative approach was chosen to evaluate our residency program’s wellness initiative and to gather resident input on future directions. Qualitative approaches are in many ways ideal for the study of wellbeing—they promote discussions, raise questions, and the topic of wellbeing itself is inherently a subjective one. However, it is important to recognize the limitations of such an approach, namely that qualitative findings are often less clearly interpretable than quantitative data. Additionally, qualitative data—particularly in narrative and opinion format—are prone to bias though we attempted to limit this by framing our questions in a neutral fashion. 7
Due to the respective limitations of either a solely qualitative or quantitative approach to the study of wellbeing, a hybrid approach may ultimately be the most effective means of evaluation. However, in the current setting of the COVID pandemic, administration of a standardized wellbeing assessment, for example, Maslach burnout inventory, 15 was too susceptible to confounders. After the pandemic, we hope to perform combined qualitative and quantitative assessments—ideally at spaced time intervals—to measure the impact of any future iterations or additions to the WC.
Another limitation of our study is applicability across other residency programs, given differences in resources. However, the general principles are applicable even if the details vary.
Conclusion
A successful WC implementation requires buy-in from resident, faculty, and administrative stakeholders. Our WC relies on input and collaboration at each of these levels. Our WC begins with identification and optimization of existing resources at department and institutional levels, and the formation of a dedicated Wellness Committee and Liaison to facilitate implementation of wellness goals.
Supplemental Material
sj-pdf-1-mde-10.1177_2382120520978238 – Supplemental material for Six Steps to Achieve Meaning, Wellness, and Avoid Burnout in a Residency Program
Supplemental material, sj-pdf-1-mde-10.1177_2382120520978238 for Six Steps to Achieve Meaning, Wellness, and Avoid Burnout in a Residency Program by Brian Stamm, Margaret Yu, Christina M Lineback and Danny Bega in Journal of Medical Education and Curricular Development
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
BS, MY, CML, and DB contributed to the design of the project, review of survey responses, drafting, and revision of manuscript drafts. All authors have read and approved the final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.