
Abstract
Objectives of this study were to evaluate an equine assisted learning (EAL) curriculum designed for medical students and resident physicians, and to determine impacts of the curriculum on participant perceptions of burnout and well-being. The EAL curriculum incorporated evidence-based skills and concepts to increase happiness and/or resilience. A pre/post intervention design was used, with 18 EAL participants receiving the curriculum within their month-long community based primary care clerkship elective, and 10 control (CTL) participants who did not receive the curriculum within their clerkship elective. Three waves of surveys tested participant responses before, immediately after, and 3 months after the intervention. Patient Health Questionnaire-4 (PHQ-4) screened for depression and anxiety, and Maslach Burnout Inventory- Human Services Survey for Medical Personnel (MBI) addressed burnout. Analysis of covariance evaluated differences between EAL and CTL groups. EAL participants rated the curriculum highly (9.2 on a 10-point scale). The evaluations were overwhelmingly positive with participants able to identify key concepts that were most helpful, how they would apply those concepts to patient care and interactions with colleagues, and how the horses added value to their learning experience. Significant positive effects of EAL on burnout were identified in terms of improved MBI personal achievement scores, as well as a trend towards improved well-being scores. There was also a trend (P < .08) towards PHQ-4 depression scores to be lower in EAL group at T3. In conclusion, this study is the first to provide AU: quantitative evidence of positive outcomes associated with an EAL curriculum designed to strengthen well-being in medical students and resident physicians.
Keywords
Introduction
The psychological well-being of medical students, residents, and practicing physicians has become an increasingly recognized cause for concern and is now a major initiative of the Accreditation Council for Graduate Medical Education (ACGME). 1 Studies show that prevalence of depression and burnout in medical students is higher than in the age-matched general population, including other US college graduates, 2 and is predictive of suicidal ideation.3,4 Up to 50% of medical students experience burnout and 10% report suicidal ideation.3,4 Few students seek help for these symptoms. 4 Furthermore, burnout in medical students is associated with self-reported unprofessional conduct, 5 less altruistic professional values, 5 and alcohol abuse/dependence. 6 Similarly, rates of depression and burnout in medical residents and practicing physicians are high and are associated with poor quality of care, reduced patient satisfaction, and increased risk of patient safety incidents, including major medical errors.7,8 With increased awareness have come increased efforts to address this problem within medical education. All medical residents are annually surveyed by the ACGME with specific questions assessing their well-being. Medical schools and residency programs are strongly encouraged to monitor well-being, and to develop ways of increasing well-being in their learners. Unfortunately, little published data exists to show changes in prevalence and efficacy of these interventions.
A variety of definitions exist for positive states of well-being. Psychological well-being is often referred to as happiness, including positive affect, low negative affect, and overall sense of satisfaction with life. 9 Others propose a state of dynamic equilibrium “the balance point between an individual’s resource pool (psychological, social, and physical) and the challenges faced.” 10 The field of positive psychology has shown that the primary drivers of happiness are internal rather than external. Factors that are modifiable such as our ability to see stress as a challenge, adopt a growth mindset, practice self-compassion, gratitude, and increase our sense of connection to others, all contribute to improved well-being.11,12
Meditation is one of the few interventions studied specifically with medical students. Meditation has been shown to reduce stress, anxiety, depression, and to create new neural pathways that increase positive emotions and the ability to see stress as a challenge.13-18 Premedical and medical students who participated in a 7-week mindfulness meditation course reported reduced psychological distress, including depression and anxiety, and increases in empathy. 19 A meta-analysis of 19 studies testing a variety of interventions to reduce burnout in medical students and residents found that self-development groups, mindfulness training, a meditation technique called the Respiratory 1 method, duty hour limitations, and conversion to a pass-fail grading system all reduced burnout in 1 or more studies. 20
Animal assisted therapy has also been explored as a therapeutic intervention to address both mental and physical health issues in human medicine, social work and educational settings. Horses are increasingly included in these activities, 21 such that the Americans With Disabilities Act includes in its definition of service animals “miniature horses that have been individually trained to do work or perform tasks for people with disabilities,” requiring reasonable accommodations in all areas of businesses where public is allowed to go. 22 Equine experiential learning includes both equine assisted psychotherapy and equine assisted learning (EAL) also known as equine facilitated learning. Equine assisted therapy involves a health professional working with a trained equine facilitator, horse handler, and/or is trained in equine assisted therapy themselves to treat people with specific mental or physical health problems, including attention deficit/hyperactivity disorder, 23 psychiatric or behavioral disorders,24-27 substance abuse,28,29 or physical disability. 30 In EAL, a trained facilitator guides people in activities using horses or other equines to promote development of life skills for professional and/or personal growth including improved wellbeing. These EAL activities provide opportunity for experiential or hands-on learning, with horses serving as a metaphor for interactions with people (Figure 1).

Horse at liberty (unrestrained) choosing to follow a participant during an equine assisted activity. Participants practiced attention to nonverbal signs using a stepwise approach to engage the horse and invite them to follow.
Research in the field of equine experiential learning is in its early stages. Whereas some published reports show benefits in terms of improved measures of psychological distress 31 and increased well-being in at-risk youth,26,27,29 and participants with mental health23-25,27 or substance misuse disorders, 28 overall the number of studies is limited and often include small sample sizes with variable results. 32 The use of EAL with medical students was pioneered by Dr. Allan Hamilton at The University of Arizona in 2001 as a way of improving interpersonal skills with patients, and further developed by Dr. Beverly Kane at Stanford University. A small number of additional programs have been offered to medical students both within the United States and internationally, however little is known about how students perceive these courses and no studies have been published measuring outcomes.
The objectives of this study were to evaluate an equine assisted learning curriculum designed for medical students and resident physicians, and to determine impacts of the curriculum on participant perceptions of burnout and well-being. We predicted that participants would positively evaluate the course, would relate key course concepts learned with the horses to their relationships with patients and colleagues, and would report a positive perceived ability to apply key course concepts 3 months after completion. We also predicted participants would report reduced burnout, increased well-being, and reduced indicators of depression or anxiety, when compared with participants who did not participate in the equine assisted curriculum.
Materials and Methods
The use of human participants for this study was reviewed and approved by the Institutional Review Board, Human Research Protection Program, UnityPoint Health (IM2019-014). Methods associated with use of horses in teaching activities received approval by the Institutional Animal Care and Use Committee, Iowa State University (#IACUC-20-082). Consent for photo use was obtained from the participants shown in Figures 1 and 2.

A participant working with a miniature donkey during an obstacle course activity. Participants used problem solving and attention to non-verbal signs to support their equine partner during the activity.
Study design
The study utilized a nonrandomized, control (CTL) group, pretest-posttest design, consisting of an intervention group that participated in the EAL curriculum and a CTL group that did not receive the curriculum. Three waves of surveys were used to test participant responses before, immediately after, and 3 months after the intervention. This design has been widely used to evaluate the impact of different interventions in situations where random assignment is often not possible.33,34
Participants
The EAL curriculum was included as part of a month-long community based primary care clerkship elective. All third-year medical students from the Carver College of Medicine at the University of Iowa (n = 15) who were completing their community-based primary care clerkship at UnityPoint Health Des Moines during the months of May to November 2019 participated in the EAL curriculum as part of their regular clerkship rotation. Since the EAL curriculum required outdoor activities, it was not offered during months where weather was likely to be prohibitive (December-April). Students rotating in Des Moines during the months of May 2019-November 2019 participated in the EAL curriculum 1 day per week for 3 weeks and served as the intervention group. Students from the same class who were completing other rotations in Des Moines during the months of May-November 2019 were invited to participate in the study and served as a CTL group (n = 12).
The EAL curriculum was also offered as an elective to internal medicine residents at UnityPoint Health Des Moines. The EAL curriculum was led 3 days per week for 2 weeks (totaling 6 days) with 3 days of content identical to that of the medical students. The second week included additional content focused on further development of leadership skills, mindfulness, and both verbal and nonverbal communication skills. Three residents signed up to participate in the EAL curriculum and were included in the intervention group.
Recruitment
All potential study participants were sent an email inviting them to enroll in a research study designed to evaluate a new curriculum. To minimize self-selection bias, the invitation email was intentionally vague. Participants in the EAL group were sent an email invitation to anonymously complete an online survey. Participants were not aware of the intent of study, or that there was another cohort participating. They were informed that their participation would require completion of 3 surveys over the next 3 months, each taking approximately 10 minutes to complete. To encourage honest responding, anonymity was repeatedly emphasized in all communications.
For each cohort of 2 to 3 EAL participants, a matching cohort of 2 to 3 participants who took the rotation without EAL were invited to complete the surveys and served as the CTL group. To control for seasonal effects, each month during May-November 2019, the 3 students participating in the EAL curriculum received an email invitation to participate in the study, and a corresponding group of students from the same class who would not be participating in the EAL curriculum received an email invitation to participate in the study.
Curriculum details
The EAL course was designed and held at the property of the course director, Certified Eponaquest™ Instructor, and primary investigator Dr. Nicole Artz. The EAL course incorporated evidence-based skills and concepts previously shown to increase happiness and/or resilience. Some of the course content and horse activities were originally developed by Linda Kohanov, author and internationally recognized innovator in the field of EAL.35,36 Content was introduced in didactic sessions, followed by experiential exercises with the horses. In general, there was 1 didactic piece for each horse activity. Much of the course content focused on increasing participants’ self-awareness, shifting from a fixed to a growth mindset, and improving both verbal and non-verbal communication skills in order to facilitate meaningful connections with patients and colleagues and productive conflict management. There was a strong emphasis on mindfulness—the ability to pay attention in the present moment from a stance that is non-judgmental and non-reactive. The course curriculum specifically addressed 2 of 6 competencies listed by the ACGME: (1) Interpersonal and Communication Skills, and (2) Professionalism.
Didactic material and experiential exercises were designed to allow the participants to explore the following concepts:
The value in showing up authentically (being genuine)
The impact of being mindful/present during encounters (vs distracted, rushed)
Noticing and responding to nonverbal cues
Valuing connection (ie, relationship) over perfection (ie, achieving a target blood pressure)
Seeing behavior as communication and approaching undesirable behaviors from a place of curiosity and problem solving
Getting the message behind common emotions and responding productively
Setting and respecting boundaries
Seeing from the other’s perspective
Recognizing vulnerability as a barrier to change
Noticing the effect of one’s energy and behavior on another
Balancing the use of compassionate, visionary and assertive energy for effective leadership
Six mature horses (1 mare, 5 geldings, ages 5 to 30 years) and 2 mature miniature donkeys (geldings, ages 12 to 13 years) were used in the program. All equine activities were conducted from the ground; there were no riding (mounted) activities. Most activities took place in a round pen with a horse at liberty (loose, without any restraining devices), and some activities were conducted using a halter and lead rope (Figure 2). All activities were supervised directly by Dr. Artz with attention to the welfare of both participants and horses. A major part of the curriculum involved guided self-reflection after each equine activity. During reflections, participants were encouraged to consider first what had been successful, 1 challenge they encountered, and how their experience may relate to patient care or relationships with colleagues and other members of the healthcare team.
Description of instruments/measures
The complete survey instrument consisted of 3 sections: (a) socio-demographics, (b) course evaluation, and (c) dependent measures. Dependent measures were identical for all 3 waves, with the exception of the key course concepts survey, which was administered only within the 3-month follow up survey to minimize survey fatigue. To minimize order effects, presentation of all scales and items comprising scales was randomized. A schedule of all survey instruments is presented in Table 1.
Schedule of surveys administered to study participants relative to interventions.
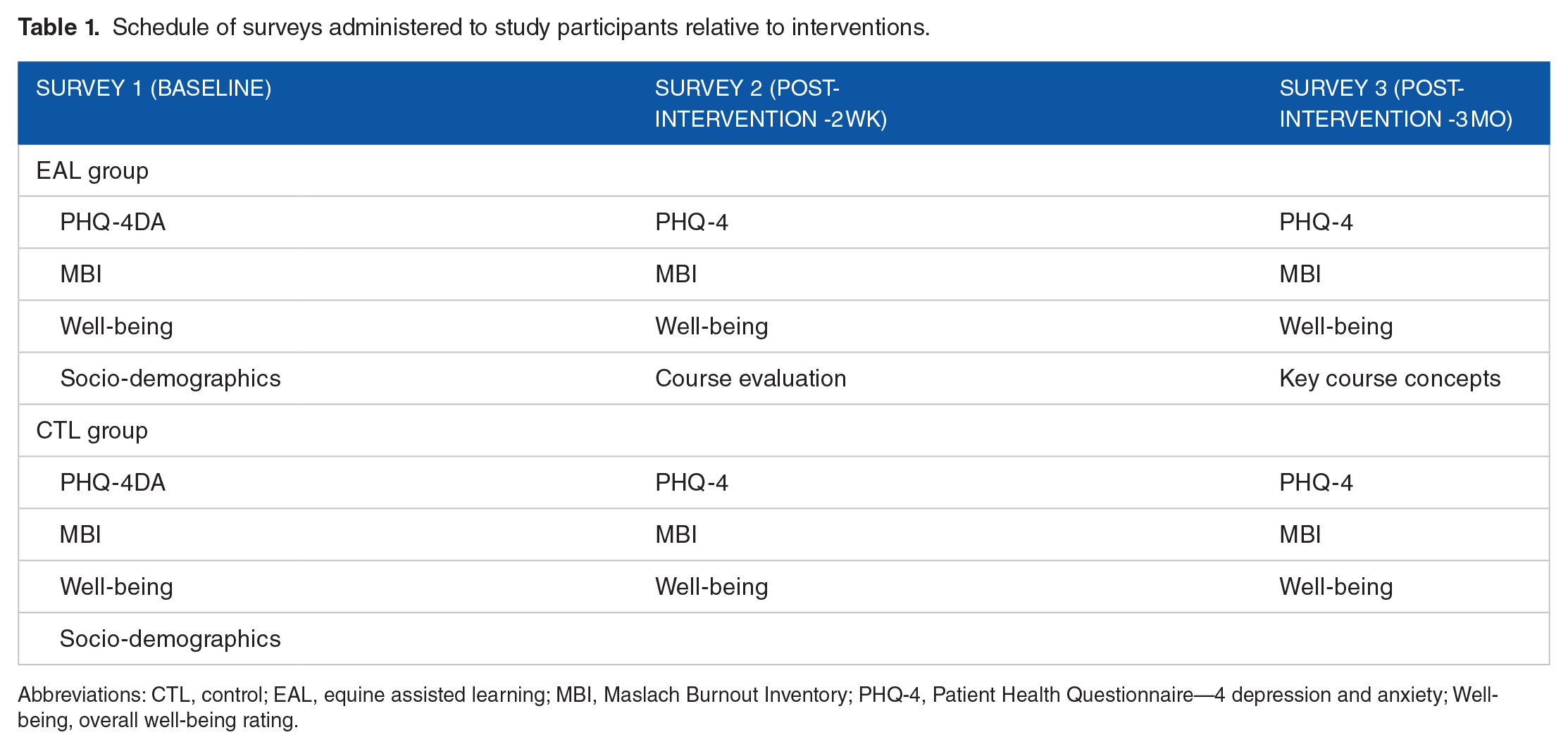
Abbreviations: CTL, control; EAL, equine assisted learning; MBI, Maslach Burnout Inventory; PHQ-4, Patient Health Questionnaire—4 depression and anxiety; Well-being, overall well-being rating.
Socio-demographics
Questions included sex, age, experience with horses, experience with meditation or other mindfulness practices, and whether they were taking antidepressant or anti-anxiety medication.
Participant well-being
The ‘Patient Health Questionnaire-4’ (PHQ-4) is a validated screening tool for depression and anxiety. Items are drawn from the first 2 items of the ‘Generalized Anxiety Disorder–7 scale’ (GAD–7) and the ‘Patient Health Questionnaire-9’ (PHQ-9). 37 Since surveys were administered at 3 different intervals, this shorter screening item was chosen instead of the longer PHQ-9 and GAD-7 in order to reduce the total number of survey questions with the goal of improving rate of completion.
The Maslach Burnout Inventory (MBI) is the most widely used validated tool to measure burnout. 38 The majority of studies assessing burnout in medical students used the Human Services Survey for Medical Personnel (MBI-HSS (MP)). 39 The MBI addresses 3 domains of burnout: Emotional Exhaustion (EE), Depersonalization (DP), and Personal Accomplishment (PA). EE measures feelings of being emotionally overextended and exhausted by one’s work, DP measures an unfeeling and impersonal response toward patients, and PA measures feelings of competence and successful achievement in one’s work. Respondents who score high on either EE or DP domains or score low in the PA domain are considered to have at least 1 manifestation of professional burnout. 38 Participants were also asked to rate their overall sense of well-being on an 11-point Likert-type scale. (0 = Very Poor; 10 = Excellent).
Course evaluation
Participants were asked to rank their experience in the EAL curriculum on a 10-point Likert scale (1 = Very bad; 10 = Very good). In addition, feedback was solicited with the use of open-ended questions encouraging free text responses in relation to key concepts that were most helpful, how they would apply those concepts to patient care and interactions with colleagues, and how the horses added value to their learning experience.
A quantitative key course concepts survey was included consisting of 10 items asking participants to rate their perceived ability to implement key course concepts using a 6-point Likert (1 = Never; 6 = Always).
Statistical analysis
Analysis of covariance (ANCOVA) was used to test for differences between EAL and CTL groups,34,40 with medication and meditation included as covariates to control for differences in these factors between CTL and EAL groups. 41 Scores at t2 were entered as the dependent variable and then regressed on a) pre-course scores (t1) and b) a treatment dummy variable (0 = CTL; 1 = EAL). This approach allowed us to test for an effect of intervention on t2 scores while holding t1 scores constant. Similarly, scores at t3 were compared with t1 and t2 scores to test for intervention effects 3 months later. Statistical difference was associated with P < .05, and 0.05 > P < .10 was considered a trend. All statistical analyses were performed by 1 author (JAR).
Results
Socio-demographics
Socio-demographic information is presented in Table 2. A total of 30 participants were initially enrolled in this study (18 in the EAL group and 12 in the CTL group. Two participants assigned to the CTL dropped out without providing any data, leaving 10 participants in the final sample and a final n = 28. The mean age of our sample was 26 (SD = 2.5) and 54% identified as female. The CTL group had a greater proportion of participants identifying as female (60% vs 50%), practicing meditation (70% vs 39%) and fewer taking medication for anxiety or depression (0% vs 22%). Age and horse experience did not differ between groups (all P’s > .05; Table 2). Of the EAL participants, 18 completed the first 2 waves of the study and 15 completed all 3 waves. Of the 10 CTL group participants, 6 completed all 3 waves of the study, 3 completed 2 waves, 1 completed 1 wave.
Demographics of study participants (n = 28) enrolled in an equine assisted learning elective (EAL) or no equine assisted learning elective (CTL).

Course evaluation
Participants rated their overall experience in the EAL curriculum highly with a mean rating of 9.2, where 1 = Not Useful and 10 = Extremely Useful, n = 15). The evaluations were overwhelmingly positive with participants able to identify key concepts that were most helpful, how they would apply those concepts to patient care and interactions with colleagues, and how the horses added value to their learning experience. Representative comments are provided in Table 3.
Representative comments provided by participants (n = 18) following participation in an equine assisted learning curriculum designed to facilitate mindfulness in medical students and residents.

Only one participant out of 18 expressed doubt about the value of the horses: “I understand how the horses have similarities to dealing with difficult patients, but overall I was unsure of how it will help me in working with patients as I think it is easier to understand patients than horses. I can see that they add value in immediately practicing a concept, but the horse application often felt far removed from the patient application to me. However, working with the horses is fun and definitely better than just talking about concepts with no application.” Suggestions for improvement focused on requests for fewer didactic pieces and more activities with the horses.
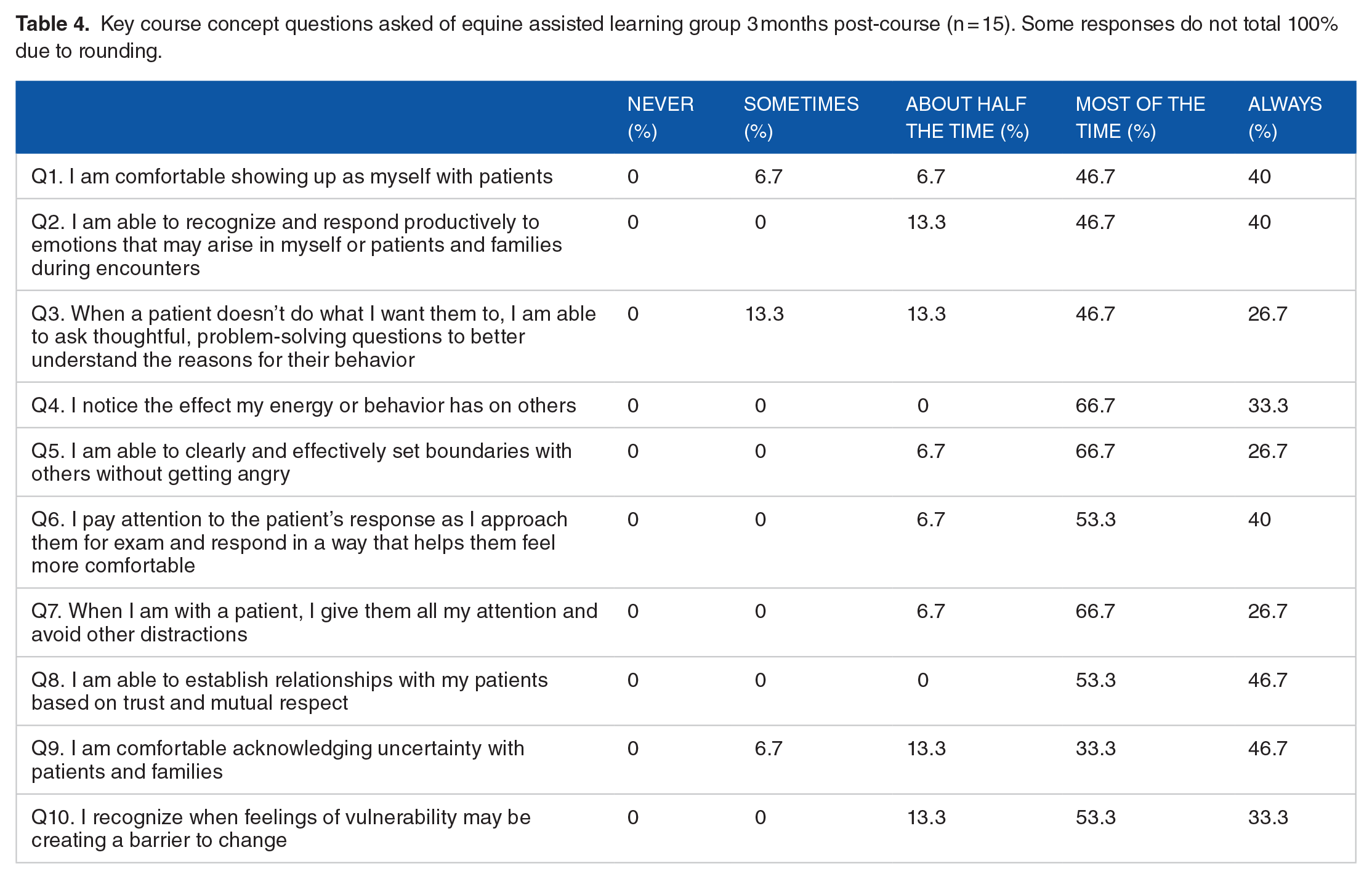
Participants perceived abilities to implement key course concepts at 3 months post course are reported in Table 4. Greater than 90% of participants reported being able to implement half of the key course concepts most or all of the time. The ability to draw out non-adherent patients through thoughtful, problem-solving questions was the concept in which implementation was weakest, but still implemented most of the time by 73% of participants.
Key course concept questions asked of equine assisted learning group 3 months post-course (n = 15). Some responses do not total 100% due to rounding.
Participant well-being
Table 5 shows complete mean scores and standard deviations associated with depression and anxiety (PHQ4), burnout (MBI) and perceived well-being for both EAL and CTL participants at the 3 time points.
Mean (SD) for all dependent measures across all 3 time periods assessed (t1, t2, and t3).

Analysis of covariance (ANCOVA) models were constructed to explore effect of course. Associations between pre (t1) and post (t2) EAL course test scores are presented in Table 6. The coefficient for MBIpa was positive and significant (ß = 3.74; P = .03), indicating taking the course predicted greater sense of personal accomplishment. There was also a tendency for well-being to improve (ß = .90; P = .08). No other MBI or PHQ4 measures were significant in our regression model.
Results of ANCOVA analysis where post test scores (t2) for each dependent variable were regressed on intervention dummy variable (0 = control; 1 = equine assisted learning). Pre-test scores, meditation and medication variables were included as covariates (n = 26).

Bolded rows indicate test was significant at P < .05, or a trend toward significance at P < .10.
Associations between pre (t1) and post (t3) EAL course test scores were also examined; no significant effects were identified, apart from a trend (P < .08) towards PHQ4 depression scores to be lower in EAL group at T3 (Table 7).
Results of ANCOVA analysis where post test scores (t3) for each dependent variable were regressed on intervention dummy variable (0 = control; 1 = equine assisted learning). Pre-test scores, meditation and medication variables were included as covariates (n = 22).
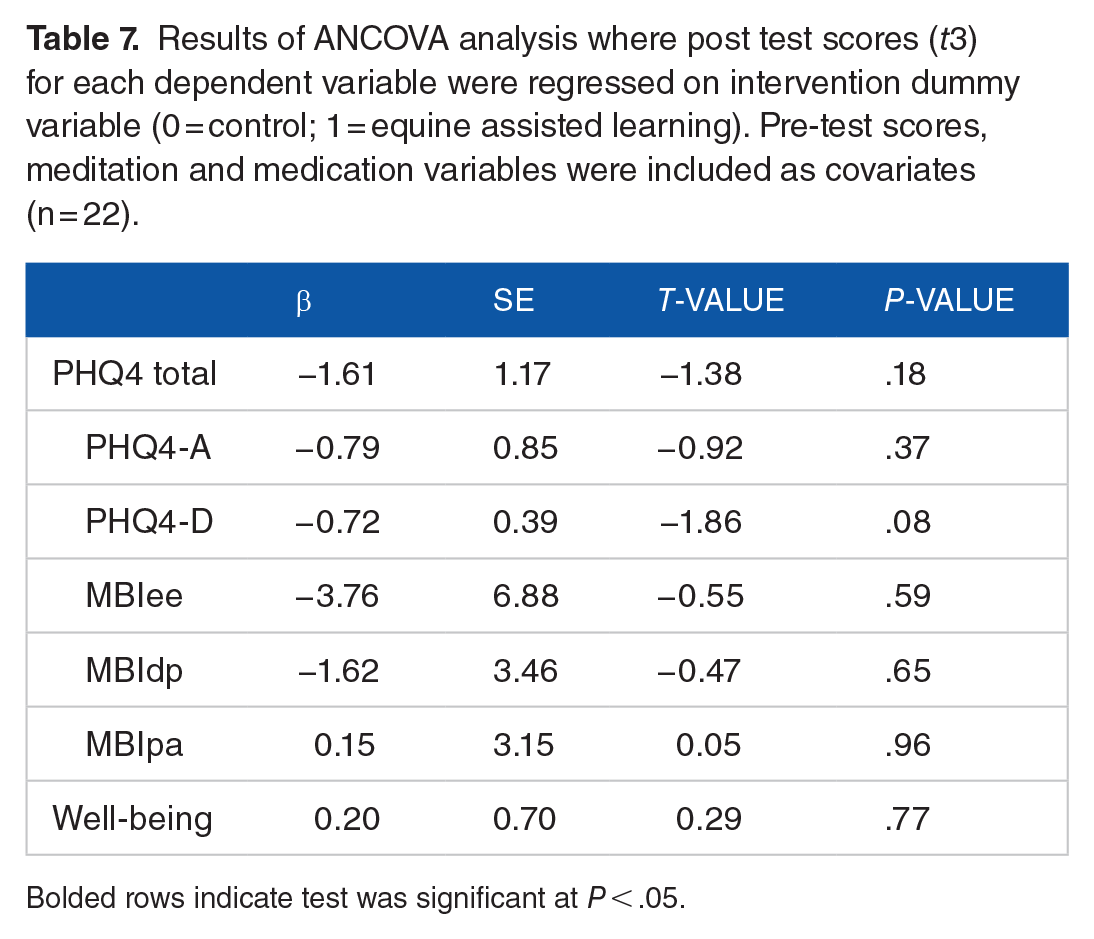
Bolded rows indicate test was significant at P < .05.
Discussion
In this study we sought to evaluate the impact of an EAL curriculum on overall burnout and well-being in medical students and resident physicians. To our knowledge, this is the first study to determine impacts of an EAL intervention on medical students and residents, using program evaluation and quantitative outcome analyses.
The course was very well received by students with overwhelmingly positive feedback. This is consistent with feedback reported from participants in other EAL studies.25,42 In the program evaluations, participants demonstrated their ability to perceive how they would incorporate lessons learned from the horse activities to their future interactions with patients and colleagues, an important goal of educational initiatives. In the 3-month follow up survey, most participants reported perceived ability to incorporate key concepts from the course into their patient interactions despite lack of any ongoing support or reinforcement following course completion.
Our participants’ scores on the MBI-HSS subscales for emotional exhaustion and depersonalization were similar to mean scores reported in a meta-analysis comparing burnout among medical students with other post-secondary education students. 39 The scores for the personal accomplishment subscale among our participants were higher than medical students in the Erschens meta-analysis, and were similar to scores of the CTL group (other post-secondary education students). 39 Our participants’ mean scores on the PHQ-4 were approximately 1 for depression and < 1 for anxiety, far lower than the positive screening threshold score of 3. Most studies evaluating depression in medical students have used longer survey instruments with an overall prevalence of around 27%. 4 It is possible that this discrepancy in results was associated with our small sample size and/or the surveys used.
Limitations of our study include the small sample size, and for this reason we included the 3 resident participants despite some differences in delivery of the curriculum for this cohort. We did not have sufficient numbers to explore possible differences between the resident and medical student participants, which may be interesting to explore in future studies. Small sample size was most evident in the CTL group. Our CTL group had some differences from the EAL group at baseline including more experience meditating, and no reported medication use for depression and anxiety. We attempted to control for these pre-study differences using regression analysis, however substantial error in estimates was likely. Our study was not designed in a way that allowed us to distinguish effects of equine activities in isolation from didactic material presented. Whether the perceived changes in participants actually translated into improved interactions or outcomes with their patients or colleagues was beyond the scope of the current study, and would be interesting to examine in future. The participants’ perception of their ability to implement key course concepts was high at completion of the course, but without a control to compare with (baseline data from the EAL participants or survey of the CTL participants) we are not able to determine whether this was due to the curriculum or not. It would have also been beneficial to survey patients who interact with participants to see if there were any differences in patient satisfaction with the encounters.
Our study has some important strengths. Although small in number, few studies evaluating outcomes of equine assisted interventions include a CTL group as ours did. In addition, we deliberately designed the study so that all participants were surveyed during the same months of the year to avoid a cold weather blues bias in the CTL group. 43 We collected both program evaluation comments, as well as quantitative outcome data using rigorous statistical methods to control for baseline group differences.
Participants reported many useful insights gained from the course. They reported a greater sense of personal accomplishment at completion of the course and a trend toward improved self-reported well-being. However, this did not translate into strong effects 3 months post course. It seems likely that these insights and concepts may take additional support and reinforcement over time to show the greatest impacts on quantitative measures, such as self-reported well-being, burnout, depression, and anxiety. Reducing burnout in physicians and trainees long term will need to address both the system, together with the individual’s internal factors, that drive the culture within which medicine is practiced. 44
In summary, this is the first study to evaluate outcomes of an equine assisted curriculum on perceived burnout and well-being in medical students and resident physicians. Participants reported positive experience with the curriculum, verbalized how concepts learned in the course would be useful in their clinical work as a physician, and demonstrated improved sense of personal accomplishment and well-being at completion of the course.
This study supports the use of diverse learning methods and experiential activities in medical education initiatives, specifically EAL, to instill concepts and practices known to support physician well-being.
Footnotes
Acknowledgements
The authors gratefully acknowledge funding by the Medical Executive Committee at UnityPoint Health to the primary author (NA) to support course development and delivery. Gratitude is also extended to Drs. John Yost, Steve Craig, and Tyler Schwiesow for their advocacy and support of this novel curriculum. Research components of this project received no specific grant from any funding agency in the public, commercial, or not for profit sectors.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The primary author, Dr. Artz was an employee of UnityPoint Health at the time of the study, who funded the first year of the equine assisted learning curriculum.
Author Contributions
All authors contributed equally to the following manuscript.