
Abstract
Background:
The study aimed to conduct a contextual analysis of interviews intended to assist with the future design of a feasible and relevant leadership and management course for undergraduate medical students at King Abdulaziz University (KAU), Saudi Arabia.
Methods:
This was a cross-sectional study conducted at King Abdulaziz University (KAU), Saudi Arabia, during 2019. An exploratory qualitative approach, utilizing systematic content analysis, was used. Data were collected using semi-structured interviews that were conducted with 10 leaders who were stakeholders at KAU, health service providers at KAU hospital, and stakeholders in the Ministry of Health.
Results:
This study revealed critical findings that highlighted the areas in which KAU could instill better and adequate leadership and management skills in their undergraduate medical students. Multiple core categories for a leadership and management curriculum emerged with many interrelated themes. Most participants mentioned that leadership can be taught and that early exposure is beneficial for developing skills. Additionally, they stated that leaders should have a vision and the ability to articulate that vision.
Conclusions:
Different implementation challenges were described in relation to the availability of human resources, the current short supply of suitable teachers, and program design. Teaching methods recommended included simulations, lectures, and a project-based approach. Assessment methods that were recommended included objective structured clinical examination (OSCE), formative and summative assessments, self-assessments, and portfolios.
Keywords
Introduction
Medical students are tomorrow’s doctors who are the future leaders, and their ability to lead in the 21st century will be critical to providing quality healthcare. Leadership and management skills are important for the graduates entering the workplace, particularly when they are entering the medical field for the first time. One of the important outcomes of leadership training is that the graduates who receive adequate training are potentially more creative and perform better in their workplace. 1 Regardless of the level within an organization, new graduates should be familiar with key leadership and management skills. Leadership skills are important for every student completing university education, regardless of their field or their role upon joining the workforce.2,3 For medical education, as with other disciplines, developing effective leaders is necessary to maintain professional autonomy and ensure continuous quality improvement. However, its values and ethics are unique because patient safety is always prioritized in medicine. 4 Effective clinical leadership has been associated with a wide range of functions and is an integral part of healthcare systems with superior outcomes for both patients and organizations. 5 Effective clinical leadership is also critical to improving quality and safety. 6 Bohmer stated that practicing physicians’ leadership and management skills play a central role in their ability to deliver high-quality, cost-effective care. 7 Further, he affirmed that patient safety, healthcare quality, and cost containment depend mainly on practicing physicians’ abilities to not only make decisions about their care services, but also to manage the delivery of these services. In the 2009 version of Tomorrow’s Doctors, the General Medical Council (GMC) stated that “Medical students are tomorrow’s doctors.” In accordance with good medical practice, graduates should prioritize care of the patients as their first concern, applying their knowledge and skills in a competent and ethical manner, and using their leadership abilities, and analyze complex and uncertain situations. 8 Despite the recognized need for teaching management and leadership skills in medical curricula, few institutions have adopted a formal leadership curriculum. 9 Recently, it was reported that no evidence exists in the literature for the development or integration of formal leadership curricula in medical colleges in the Middle East or Asia. 10 Therefore, these medical programs urgently need to develop leadership curricula that focus on the development of the knowledge, skills, and attitudes needed to be effective leaders in an already resource-constrained setting.
Statement of the problem
Healthcare management and leadership education are important gaps in undergraduate medical education at King Abdulaziz University (KAU) in Saudi Arabia. Medical curricula at KAU is composed of a 6-year traditional curriculum, which comprises of 3 years of basic and medical science courses, 3 years of clinical training, followed by a 1-year internship. In 2006, the curriculum was reformed to integrate problem-based learning. 11 Still, medical college at KAU does not have a leadership and management course as a part of its medical curriculum. Therefore, graduated physicians at KAU lack formal management and leadership training to prepare them for the challenging role of delivering high-quality medical care. This deficiency in management and leadership education requires innovative solutions. It is the responsibility of the medical college to determine how to teach management and leadership program to the medical students; the topics include defining the subject area, specifying the skills and knowledge that should form the bases of the program, and optimizing training for integration into an already overcrowded undergraduate medical curriculum. The main purpose of this study is to help a future design of a feasible and relevant leadership and management course, which addresses the current demands of a developing healthcare system. To the best of our knowledge, this is the first time study such has been attempted at KAU. To accomplish this, a contextual analysis of interviews with leaders related to the KAU medical program was performed. This study investigates the following research questions: (a) What should be the management and leadership program’s goals? (b) What management and leadership knowledge should be included? (c) What are the specific leadership skills to teach? What teaching methods should be used? (d) What are the challenges or barriers to such a curriculum?
Methods
This study was a cross-sectional study conducted at King Abdulaziz University (KAU), Saudi Arabia, during 2019. Semi-structured interviews were conducted with 10 leaders who were stakeholders at KAU, health service providers at KAU hospital, and stakeholders in the Ministry of Health. Based on Inui and Frankel’s standards for qualitative research 12 and the conclusions from the critical evaluation of the literature, we developed a qualitative semi-structured interview-based design using an inductive data analysis approach to identify themes. This is particularly effective at answering the “why”, “what” or “how” questions. This design is commonly used in healthcare settings where they are seen to “reach the parts other methods cannot reach” and are important methods in health services research.13,14 As described earlier, the medical curriculum at KAU is composed of a 6-year traditional curriculum, which consists of 3 years of basic and medical science courses, 3 years of clinical training, followed by a 1-year internship. Based on this, it appeared that our medical school did not have explicit leadership curricula. But, clinical care teams were used to demonstrate the principles of leadership, which is also done in the majority of the medical schools around the world.
Semi-structured interviews
This type of qualitative interview was conducted using a loosely structured set of predefined open-ended questions and an interview schedule that defined the area to be explored. From these predefined questions, the interviewer or the interviewees could diverge from pursuing an idea or response in greater detail. 15 The preparation of these open-ended questions was based on the research questions outlined above. This assisted the interviewer in maintaining control over the interview process and keeping interviewees on a topic while allowing for some level of exploration within the established framework of thoughts and perceptions. 16
Development of the interview schedule
The interview schedule was developed based on the study aim, objectives, and research questions, with the help of a spider diagram or mind map. 17 Due to the nature of the interview and time constraints, the number of questions was fixed at 10. The following questions were used to stimulate the discussion during the interviews:
What is your position as a leader? How do you define management and leadership?
What do you think will be the leadership and management challenges in the healthcare services over the next 10 years?
In light of your experience in management and leadership, do you think that management and leadership development is important to our undergraduate medical students and why?
What do you think about clinical leadership in hospitals?
What should be the management and leadership program’s goals?
What should we be teaching our undergraduate medical students about leadership and management?
What would be the best way to teach management and leadership to our students?
What are the challenges or barriers to implementing such education?
What do you think is the best way to assess this course to ensure the best outcomes?
How best can the management and leadership course be incorporated into an already crowded medical curriculum?
Pretesting and piloting the interview schedule
The interview schedule was created, and the piloted interview was attended by a local advisor who reviewed the interview technique and ensured that the research questions were answered from the perspective of the conversational partner.
Sampling
The population under investigation in this study included leaders from the undergraduate medical program, such as vice deans, deans, and leaders on the curriculum committee. The sample also included administrative leaders and stakeholders at the Ministry of Health (MOH), physician educators with leadership roles in medical curriculum development and teaching, and residency directors to cover management and leadership roles of the students in their first 3 years of basic medical sciences (phase-I).
The administrative stakeholders included in the sample were chosen through a purposive sampling strategy. This technique is widely used in qualitative research for the identification and selection of information-rich cases. 18
Subjects of the Study
To be qualified for inclusion in the sample, administrative stakeholders were selected using the following criteria:
(a) Administrative stakeholders at KAU were identified as playing a “significant” role as student affairs administrator, program director, quality improvement director, or program coordinator, all positions that influence undergraduate medical students at KAU.
(b) Health service providers at KAU hospital who held academic positions in medical education, residency directors with leadership roles in curriculum development, consultant physicians, and professional health service managers were identified as having the knowledge of the significant leadership and management skills needed in medical graduates to improve patient outcome.
(c) Stakeholders who had significant leadership roles at the MOH (ministry leaders) were identified. The healthcare sector in the Kingdom of Saudi Arabia (KSA) is primarily managed by the government through the MOH, which is responsible for the supervision of healthcare and hospitals in both the public and private sectors.
Ethical approval
The study was approved by the Research Ethics Committee (REC) of the Faculty of Medicine, reference no-398-18. The informed consent form was designed using the consent form recommended by the WHO and was sent to participants by email. 19
Data collection method
Semi-structured interviews
Semi-structured interviews were conducted with the administrative stakeholders. Here, qualitative interviews were conducted with the help of predefined open-ended questions of the defined area to be explored. From these predefined questions, the interviewer or the interviewees are allowed to diverge in order to pursue an idea or response in more detail. 15 The preparation of these open-ended questions was based on the previously mentioned research questions. These questions assisted the interviewer to maintain control over the interview process and keep the interviewee to the point while allowing them to explore some areas within their frameworks of thoughts and perceptions. 16 Important probing questions are identified for the interview, which could add the required additional information about the topic. Interviews also allow to understand people’s opinion, behavior, and experiences in the past and derive a clear explanation from interviewed leaders and their experiences in management and leadership.
Interview conduction
Start date of data collection: April/2018; End date of data collection and analysis: September/2018. The interviews were conducted individually, face to face. All interviews were conducted by the same interviewer (the principal investigator), and the interviews were recorded by a digital IC Recorder (ICD-PX720-SONY). An invitation letter was sent to the preselected participants, which included the prepared questions together with informed consent form. The letters were sent by email before the interview, or in the case of a participant’s limited access to email, verbal consent was obtained. Participants were informed about the aim of the study and the purpose of the interview and how the data would be handled to ensure their anonymity. All participants signed a consent form for recording the interview before the interview started. Once the interview finished, all recorded interviews were backed up immediately using Digital Voice Editor Software (ver.3.2.00) provided by the manufacturer of the IC recorder. The average duration of an interview was 45 minutes.
Data analysis methods
The most appropriate analytical framework seemed to be an inductive approach of “thematic analysis” 20 and “content analysis”. 21 The trustworthiness of the data analysis was established by checking inter-rater reliability only to validate the categorization process until at least 80% agreement was reached.
The key thematic data analysis process consisted of the following 6 stages;
Familiarization with the data
Transcription of verbal data
With audio recorded interviews, the data was transformed into a written form to conduct a thematic analysis. Reading a transcribed note of data can be an excellent way of familiarizing with the data. 22 Reading and re-reading of data is time-consuming, but it also allows to check the transcripts back against the original audio recordings for “accuracy”. 20 We took the assistance of a professional transcriber, from KAUH medical records, to transcribe the findings of the interviews verbatim into English.
The transcripts were reviewed and checked against the original audio recordings for accuracy. Memos and summaries were prepared before the beginning of a formal analysis. Each interview was assigned a number or code, and interviewees were assigned pseudonyms and code numbers.
Generating initial codes
Data were coded manually by writing notes in the transcriptions or by using highlighters to indicate potential patterns. These codes could be modified later but began the process of categorizing and analyzing the data.
Searching for themes
This phase began when all data were initially coded and collated, and an extensive list of different codes was generated. This phase involved sorting the different codes into potential themes and collating the relevant coded data extracts within the identified themes.
Reviewing themes
The set of potential themes was refined to ensure that thematic data were coherent in a meaningful manner, and clear and identifiable distinctions between themes should exist. To complete the content analysis process, we categorized statements, quantified the qualitative data and interview transcripts, which are called indicators. 23 For each category, there was evidence (indicator) in the data in the form of participants’ responses to the interview questions. Consequently, a grid was constructed in which the first column contained the categories, and the next column showed participants’ statements that exemplified the category. Participants’ statements were re-read, and new categories and statements were identified until no new categories were identified (saturation).
Categorization
During this stage, we identified whether any one participant in a dataset (the leader’s dataset) displayed each category, using an Excel spreadsheet in the form of a marking grid.
Validation of the categorization
To validate the categorization process, simple inter-rater reliability was used. This validation was done by 2 of the study investigators independently identifying themes and coding categories for each data set. Then, their categorization was compared.
Statistical analysis application to the final categorization of category marking grid
The results were reported in the form of a percentage of participants agreeing to each category, subgroup comparison, or category comparison.
Results
Demographic data of participants
As shown in Table 1, 4 male leaders and 6 female leaders in different specialities (n=10) participated in this study.
Demographic data of participating leaders, including roles and departments.

Content analysis and findings
The core categories or topics were identified through an analysis of participants’ comments and were clustered into 7 overarching areas: (1) General versus clinical leadership, (2) Can management and leadership skills be taught? (3) The importance of formal leadership training, (4) Leadership and management development in undergraduate medical education, (5) Challenges during the curriculum design stage, (6) Challenges during the implementation stage, and (7) Delivery of the program. For each core category, we identified several relevant codes that were grouped into themes or categories related to the research questions. We then stated the number of participants who mentioned each code in their interviews.
General leadership versus clinical leadership
As shown in Table 2, plotting the result for the first identified core category (General leadership versus clinical leadership) led to the identification of 8 different themes. Under the theme of “Concepts of leadership and management”, most of the respondents mentioned that leaders have a vision (Table 2). Also, half of the informants mentioned that managers organize an activity to achieve the objectives. Leadership is an attitude that was the least mentioned. Further, under the theme of “Necessity for doctors to learn leadership and management skills”, most of the participants believe that doctors are leaders by default. For example, Dr. D stated the following: “Actually, doctors by default, they like it or they do not like it, they are leaders” Dr. D (148-177).
Quantification of the first core category: it shows how themes have contributed in forming the first core category (General leadership versus clinical leadership) and the number of informants who mentioned each code.

Also, half of the participants opined that there must be an alignment with internationally recommended competencies. However, 4 participants mentioned that the juniors see seniors as their role models (Table 2). In addition, 3 of all the participants mentioned that leadership and management skills are necessary to run medical departments successfully. Other identified codes under this theme were as follows: “Usually the team leader is the doctor”, “The service will always need good leaders”, “All doctors’ work contains management components” and “Seniors mold juniors”. These themes recorded the least number of participants’ agreement (Table 2). Regarding the theme “Benefits to the individual”, 4 participants mentioned that self-management skills—time management was the most important benefit (Table 2). For example, Dr. D stated that: “I think a leader has 3 levels. There is self-leadership, there is a people leadership, and there is an organizational leader.” Dr. D (151-163). Also, Dr. F stated: “The whole concept of personal leadership, all the traits of personal leadership, starting from having the insight, having the trait of how a person can contribute to an institutional vision, a country vision, and the traits of time management.” Dr. F (283-340). Under the theme “Better performance in the workplace by self and others”, 3 participants mentioned that leadership provides better quality of performance of team (Table 2). As Prof. G stated that: “A leader should inspire people to move on, to do the job well, to have a good practice, to become the best they can be as a group working together toward a common goal.” Prof G (6-31).
Further, under the theme “Improving care for patients”, improving quality and safety of the services constitutes the most important outcome for leadership by half of all participants (Table 2). The themes “Improved care for patients” and “Better understanding of patients” were the least mentioned. Finally, under the theme “Promoting effective inter-professional team working”, 4 participants mentioned the code “Articulating the vision”, and 4 of them agreed that leadership results in “Improving communication with the team” (Table 2). The remaining codes under this theme constitute the least mentioned, such as; “Staff need to feel ownership with goals imposed by others”, “Understanding why”, and “Better environment for healthcare workers and avoiding stress” (Table 2).
Can management and leadership skills be taught?
Under this core category, 3 themes were identified. The first theme, “Are leaders born or made?”, 3 of the participants mentioned that leadership can be taught, and 2 only mentioned that leadership is an inherent trait (Table 3). For example, Dr. F stated that:“ I think there are well known leadership skills that could be taught, but you will find people who are more, let us say, easier to be taught compared to others, but at the end of the day, everyone can be taught the leadership skills.” Dr. F (9-81). Also, Prof. G stated that “Leaders are born? No. I would say 50-50. Some people, they have the trait, but depending on environment and how they have been raised, these traits are being developed. The way they are living, their schools, lots of things supposed to go into these. I would say that none of us have been born a leader, but you will find that the more you give a person more responsibility, the more you give him action.” Prof.G (6-31).
Quantification of the second core category: it shows how themes have contributed in forming the second core category (Can management and leadership skills be taught?) and the number of informants who mentioned each code.

Under the second theme, “Personal strengths and weaknesses”, emotional intelligence was the most important personal strength mentioned by most (8) participants (Table 3). For example, 1 of the Dr. D mentioned that: “Emotional intelligence is a tool that will enable them to understand the feeling of the people around them, and they will have a self-awareness. Accepting feedback from other and these things. When they reach self-awareness, they will know their emotions and they will know the emotions of others and try to control it in order to reach a level that is in the harmony of relationship”. Dr. D (228-238). Also, Dr. A mentioned that “A leader is an emotionally-intelligent person that is able to detect the strengths”. Dr. A (31-36).
Other personal strengths such as “Humility”, “Commitment”, and “Ethics & morals” constitute the least mentioned codes (Table 3). The remaining personal strengths, such as honesty, integrity, team player, and knowing one’s limitations, were least cited (Table 3). Importantly, under the third theme “Skills regarded as good management and leadership qualities,” 4 participants mentioned that influencing others, motivating others, and effective team-working were the most important skills (Table 3). Communication skills and soft skills—communication, collaboration were the second important skills mentioned. Other remaining skills, such as empowering others, bringing people together, constituted only the least agreement (Table 3).
Importance of formal leadership
Under this core category, 1 theme was identified “Importance of leadership and management training for undergraduates’ (Table 4). Six of the participants described that early exposure is beneficial for developing skills in leadership (Table 4). One of the participants stated the following: “. . .Conflict management, all of these. If we were told at their level, at the undergraduate level, things would have been different. The way you would see at the end of that course, you know. I attended those courses with undergraduate students and I was a fellow. The medical school is 7 years. I was 35 I think and the students were 19. Okay, and you can see how, we are learning the same thing, but I am delayed 15 years. . .” Dr. F (147-247):
Quantification of the third core category: it indicates how themes have contributed to forming the third core category (Importance of formal leadership and management training in undergraduate medical study) and the number of informants who mentioned each code.

Leadership and management development in undergraduate medical education
As shown in Table 5, while describing themes for this important core category, 4 themes were identified. Under the first theme, most of the participants mentioned that there is a need to convince students about the importance of leadership and management skills (Table 5). Under the second theme of this core category, 2 participants mentioned that there are “Leadership opportunities in current curriculum”. Under the third theme, “Developing leaders who can meet healthcare challenges”, only 3 of the participants mentioned that there is an increasing demand on service from patients. The remaining codes constitute the least mentioned (1-2 of participants) (Table 5). For the important theme “Desired knowledge and skills in an undergraduate leadership program”, most of the participants (9) mentioned that communication skills are the most important (Table 5). Dr .I mentioned that: “Communication skill is the most essential skill that people have to get. So, communication skills, technology skills. I think the generation, they are very smart with the technology, but some of the leaders they need more advanced technology that they have to learn with the leadership, because the word is just changing”. Prof I (130-177). Further, conflict resolution constitutes the second most important skill mentioned. One participant mentioned that: “Conflict resolution is extremely important in the medical career and also in other careers. These are extremely important for the leader to be equipped with plus the ethics and professionalism”. Prof B (341-356):
Quantification of the fourth core category: it shows how themes have contributed in forming the fourth core category (Leadership and management development in undergraduate medical education) and the number of informants who mentioned each code.

Self-management skills and importance of attitude were mentioned by more than half of the participants who were interviewed. Effective team-working, leadership types and styles, lifelong learning, core management skills, and administrative skills were mentioned by 3 of those interviewed (Table 5). The remaining needed skills were mentioned by 1 to 2 of those interviewed, which are as follows: how to be a role model, understanding situational leadership, personal qualities (eg, humility, confidence), interviewing others, teach personal leadership at the undergraduate level and leader as teacher and learner, etc. (Table 5).
Challenges at the design stage
Eight themes were identified under this core category (Table 6). Under the first theme, “Getting agreement for the program”, most of the participants (9) mentioned that there is a need to convince faculty (Table 6). Some of the probing questions were conducted here to explore participants’ responses further. Further, only one participant mentioned that there is a need to convince the Government. One participant mentioned that: “You have to make people understand the concept first. If they agree even the teachers, they have to be on board really. So, everybody has to be on board to start the thing.” Dr. E (318-362).
Quantification of the fifth core category: it shows how themes have contributed in forming the fifth core category (Challenges at the design stage) and the number of informants who mentioned each code.

Under the second theme, “Goals and objectives need to be clear”, 2 of the participants mentioned the need for clear goals and educational objectives (Table 6). Further, the third theme of this core category was “Program planning: timescale”, where 3 of the participants agree that the curriculum changes take a long time to implement. Importantly, under the fourth theme, “Fitting leadership and management into an already-crowded curriculum”, the majority of the participants mentioned “Curricular versus extra-curricular” as an important factor (Table 6). Also, the codes “Current curriculum is already crowded” and “Presented as an individual subject or as a part of other courses in the curriculum?”, were mentioned by half of the participants (Table 6). For the code “Preference for integrating leadership skills in every course”, 4 participants mentioned it (Table 6). The least detected codes were as follows: “Easier to fit in as vertical integration and horizontal integration rather than a standalone block” and “Remove unnecessary content to make space in the curriculum were” (Table 6). Under the fifth theme of this core category, (Program content seen as something new), only 2 participants mentioned that “Little focus given to leadership and management in the past/present curriculum”. The remaining codes that constitute the least agreement are as follows: “Non-cognitive skills are not tested before admission”, “Medical colleges currently concentrate on knowledge and skills with less focus on attitudes”, “Medical curriculum emphasis is on clinical knowledge with little on population and ‘Behavioral issues’ and ‘Currently no leadership programs in medical colleges in Saudi Arabia” (Table 6). For the sixth theme, “Need for collaboration with other parties”, only 1 of the participants mentioned the importance of inter-professional collaboration (Table 6). For the seventh theme, “Cultural/contextual factors”, 4 participants mentioned “Based on what is really required of Saudi graduate physicians” and “Tailored to Saudi culture and society”. (Tables 6 and 7).
Excerpts from narratives related to challenges of program design and implementation.

Challenges at the implementation stage
Six themes were identified under this core category (Table 8). The availability of human resources was the first theme to be identified. Seven leaders described the pros and cons of bringing in teachers from elsewhere. Half of the leaders mentioned “Suitable teachers currently in short supply” (Table 8). Two of the participants mentioned that there is a need to train faculties to deliver the course to expected levels and outcomes (Table 8). The remaining codes were the least, mentioned such as; “Lack of role models for learners”, “Lack of mentorship, Students” view of credibility of teacher’, “Learners need to see role models in action to confirm what they have learned”, and “Academics seem to have less enthusiasm for teaching, guiding and mentoring than in the past” (Table 8). Under the second theme “Availability of other resources”, only 1 participant mentioned “Availability of non-human resources” (Table 8). Further, under the third theme (Cost), 3 participants described “Funding needs”. Support from senior administrators was the fourth theme under this core category and 2 participants mentioned lack of top level support (Table 8). Also, for the theme variation in leadership styles and practice and the traditional leadership style, 2 of all participants agree for “Lack of clear definition of the leadership role in different settings”, “Lack of openness among current leaders to co-workers”, and “Authoritarian leadership is the norm”. “Differing visions” and “Some leaders appear resistant to change” were the least mentioned (Table 8).
Quantification of the sixth core category: it shows how themes have contributed in forming the sixth core category (Challenges at the implementation stage) and the number of informants who mentioned each code.
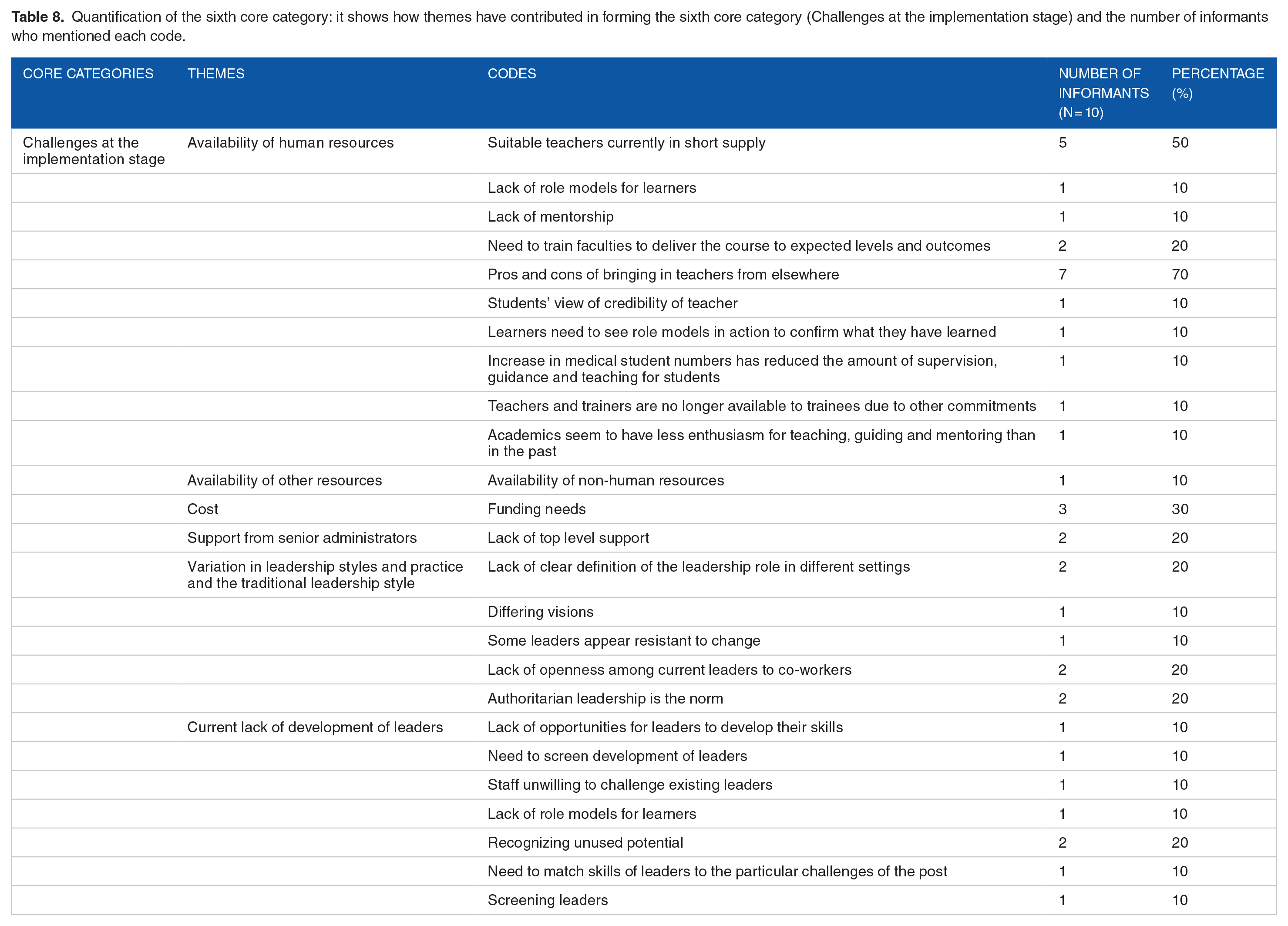
Under the theme of “Current lack of development of leaders” only 2 of participants agree that Recognizing unused potential. The remaining codes were the least mentioned, such as; “Lack of opportunities for leaders to develop their skills”, “Need to match skills of leaders to the particular challenges”, “Screening leaders”, and “Staff unwilling to challenge existing leaders” (Table 8).
Delivery of the program
The last identified core category is the delivery of the program. Under this core category, 5 themes were identified (Table 9). Under the theme (program design), 2 of participants preferred “Longitudinal design”, and 1 participant mentioned “Use spiral curriculum design” (Table 9). Under the theme “Curriculum design”, 3 of the participants mentioned that it must be connected to clinical context/activities (Table 9). Further, 2 of the participants mentioned that curriculum design must start with the theoretical part, then go on to the practice part (Table 9). Additionally, 2 of the participants agreed that curriculum design must “Build on strengths of students”, while 1 participant mentioned that “Practical as well as theoretical elements” are required in program implementation (Table 9).
Quantification of the seventh core category: it shows how themes have contributed in forming the seventh core category (Delivery of the program) and the number of informants who mentioned each code.

For the third theme, “Teaching methods”, 5 participants mentioned that “Simulation” is the best method of teaching (Table 9). Also, 3 participants mentioned that to use lectures for theoretical knowledge objectives and use a project-based approach (Table 9). Three participants mentioned for learning by practice. Further, 2 participants mentioned for use attachments to role models in clinical practice to learn skills, provide mentors, expose students to how the operational part of the institution or organization is run, use attachments to role models in clinical practice to learn skills, role play, and teaching method depends on objectives (Table 9). The least (1) mentioned workshops, videos, make it fun, start by agreeing on your goals and the curriculum elements and teaching methods will follow (Table 9).
For the theme “Assessment methods”, half of the participants (5) mentioned there should be a rationale for the choice of assessment methods (Table 9). Also, 4 participants mentioned for “OSCE”, and 4 participants described “Who will do the assessment, Self-assessment, peer assessment and assessment by others” (Table 9). Three participants mentioned formative or summative assessments. Two participants mentioned aligning assessment with teaching and program goals/objectives (Table 9). “Traditional exams for assessing knowledge”, “Case-based assessment”, and “Portfolio” were the least mentioned codes.
For the last theme under this core category, “Program evaluation”, 4 participants mentioned that evaluate the program to identify outcomes and changes during or after. Further, one participant mentioned the quality of assessment, assessment is a necessity to validate the knowledge gained, and the critical point is how to assess it (Table 9).
Summary of results
The study provided a contextual analysis of management and leadership skills derived from key informants in KAU, KAUH, and MOH. We attempted to investigate the needed competencies and challenges in the Saudi context, with an aim for informed course design in the future and to provide awareness of areas that need further investigations. The study identified leadership and management competencies needed for the future design of leadership and management course for undergraduate medical students by exploring different obstacles or challenges in developing a leadership curriculum in the medical college of KAU. The study revealed that a leadership development program is mandatory for our medical education because of the shortage of decisive leadership and management skills in our graduates, which affects their health care delivery and teamwork. Most participants of our study agree that leadership can be taught, and early exposure is beneficial for developing skills in leadership. Doctors are leaders by default, and leaders should have a vision and ability to articulate their vision to the followers. The most important outcome for the leadership curriculum should be to improve the quality and safety of services. Also, leadership leads to improving communication with the team. Further, there should be an alignment with internationally recommended competencies.
Emotional intelligence was the most important personal strength mentioned, and communication skills are the most essential skill to be developed, followed by conflict resolution, self-management, and appropriate attitude and teambuilding. Most of the participants mentioned that it is required to convince faculty to develop this program, and others emphasized the need to convince students. Most participants recommended the leadership development and management program to be a part of curriculum. Regarding challenges at the implementation stage, most of the participants described the availability of suitable human resources as a challenge, and emphasized the need for bringing in teachers from elsewhere. Regarding the design of the program, there was a mixed opinion between narratives with a low agreement, which included longitudinal design, spiral curriculum design, and connected to clinical context/activities, and this needs further evaluation. Also, regarding teaching methods, there was a mixed opinion with a low agreement between narratives, simulation, lectures, a project-based approach, and provide mentors. For the assessment methods, participants described with low agreement the different methods of assessment (OSCE’, formative or summative assessments, self-assessment, peer assessment, case-based assessment, and portfolio). Furthermore, there must be a rationale for the choice of assessment methods and alignment of assessment method with teaching and program goals/objectives. Finally, program evaluation to identify outcomes and changes during and after, was noted with low agreement.
Discussion
In the interviews, participants had the opportunity to express their views and share their stories, which gave us a deeper understanding of the leadership and management competencies that are important for our medical students. The data obtained from this study has helped to characterize the knowledge and competencies necessary to design a management and leadership curriculum. The result of the content analysis of the semi-structured interviews justified 7 core categories or areas.
General leadership versus clinical leadership
Stanton et al. defined “clinical leadership” as referring to a physician’s ability to serve as both a manager and a leader of diverse teams in pursuit of maximally effective patient care. 24 Hence, under this core category, the related concepts between general leadership and clinical leadership were identified. Eight different themes were identified from interviews.
Leaders have a vision
Our findings revealed that participants most often believed that leaders should have a vision. McKimm and O’Sullivan defined leadership as “about providing a coherent vision for the future and setting out the strategic direction which enables the organization or team to move forward or effect change”. 25 Hence, a leader should have a clear vision for the future. Likewise, the definition of the new CanMEDS leader competency stated that “As leader, physicians engage with others to contribute to a vision of a high- quality healthcare system and take responsibility for the delivery of excellent patient care through their activities as clinicians, administrators, scholars, or teachers”. 26
Managers organize activity to achieve objectives
Our findings revealed that half of our participants agreed that managers organize activities to achieve objectives. Although there is no universal definition of management, 27 management is defined as the “act or skill of controlling or making decisions”. 28 In agreement with our findings, it was confirmed that “managers are leaders in an organizational sense whereas all doctors are leaders”. 29 In contrast, it was also observed that much overlap exists between management and leadership. 25
Doctors are leaders by default
Most of our participants believed that doctors are leaders by default—a view that the literature supported, as reflected in a quote reported by Levenson et al.: 29 “Obviously, leadership is an important part of management but every doctor is a leader. . . even the junior doctors are leaders in respect to the medical students, a 4th year (student) is a leader in respect to a 3rd year. . . managers are leaders in an organizational sense whereas all doctors are leaders”. Further, in agreement with our findings, it has been acknowledged that medical leadership is not the exclusive domain of any particular professional group. 30
Alignment with internationally recommended competencies
Half of our interviewees believed that there should be an alignment with internationally recommended competencies. This agrees with our findings, which are supported by other work in the field, medical education, and training programs today are based on a national or international competency-based framework. 31 Such frameworks include CanMEDS 32 and The Scottish Doctor. 33
Can management and leadership skills be taught?
Under this core category, our findings revealed that interviewees identified 3 important themes: whether leaders are born or made, personal strengths and weaknesses, and skills regarded as good management and leadership qualities.
Are leaders born or made?
Our narratives show that leadership skills can be taught. This finding is consistent with other work in the field. A study by Clark et al. showed that students participating in a management skills program reported an increase in emotional intelligence, supporting that training can enhance emotional intelligence. 34 In contrast, early in the scientific research on leadership, 35 traits were reported as innate or heritable qualities of the individual. Based on our findings, we would like to highlight the deficiency of the Saudi medical curriculum, in general, and at KAU in particular, in providing clear and adequate competencies that can make future doctor leaders. Because we believe that leaders are made and not born, we can advise stakeholders and decision-makers in medical curricula to start teaching management and leadership to their undergraduates.
Emotional intelligence
Our findings revealed that most participants supported the qualities of emotional intelligence as the most important strengths of a physician leader. Emotional intelligence (EI) is a new criterion for assessing people’s well-being and is an important competency for improving job performance. 36 Further, it was argued that emotional intelligence is related to the competencies of self-awareness, self-management, social awareness, and relationship management. 37 Despite the presence of different definitions of EI, investigators believe that if we aim to improve individuals’ performance, then we should increase their emotional intelligence. 38
Skills regarded as good management and leadership qualities
Participants described most frequently other important leadership and management qualities, such as influencing others, effective teamwork, motivating others, communication skills, and inspiring others, where were in line with other reported studies. In a recent study, 39 4 groups of essential skill sets were identified from an analysis of the data: teamwork, communication, management, and community advocacy. Additionally, in the previous study, all participants identified a leader’s ability to work with others in a team as important, as were communication skills. Another study 40 reported the importance of team leadership in particular for those working in health-related fields, where graduates are expected to work in a team environment in the workplace.
Importance of formal leadership
In our study, 6 of our participants stated that “Early exposure is beneficial for developing skills” (Table 4). In agreement with this finding, in a study of participants in Leadership Education Advocacy Development Scholarship (LEADS) 41 tracked complete courses in advocacy skills, perform a summer internship, and complete a mentored scholarly activity addressing population health. Students were paired with a faculty mentor and a community-based organization. The results of the LEADS study 41 reported that students showed empowerment, improved self-efficacy, and increased likelihood of future engagement in leadership and health advocacy.
Undergraduates need to understand the importance of leadership and management skills
Most of our interviewees believed that we need to convince students to study leadership and management. In agreement with this finding, a group in the School of Nursing at Edith Cowan University discussed a leadership program implemented to develop leadership in nursing students. 42 Students were invited to apply to undertake the program during their extracurricular time. The leadership program focuses on the student-participant’s ability to self-reflect on their leadership qualities, engage in critical appraisal, and work within a team and take responsibility for ensuring the achievement of team goals as a leader. Conversely, studies show that students might not understand the importance of leadership and management training for their disciplines. 43
Developing leaders who can meet healthcare challenges
Under this theme, our participants described eleven codes. All constitute a low priority (10–30%). This low agreement might be explained as follows. Despite growing support for the importance of leadership development practices in medical colleges, our participants knew little about the challenges in leaders’ development. Despite the improvement in and expansion of the healthcare sector in Saudi Arabia, several issues pose challenges to the healthcare system, such as a shortage of Saudi health professionals, changing patterns of disease, high demand for services, poor accessibility to some healthcare facilities, lack of a national health information system, and the underutilization of the potential of electronic health strategies. 44 The Saudi healthcare system is challenged by a shortage of local healthcare professionals, such as physicians, nurses, and pharmacists. Most health personnel are expatriates, leading to high a turnover rate and workforce instability.
Obtaining agreement for the program, getting others to “buy into” the program
Most of our interviewees believed that we need to convince the faculty. A very small proportion of narratives were coded to “Need to convince government” and different perspectives on how things should be done. This finding is in agreement with a recent study 45 that found that major stakeholders such as governing bodies, deans, lecturers, and students must be consulted to develop the curriculum in terms of both contents and the practicalities of incorporating it into the medical course. As previously mentioned, the government should take responsibility and invest in developing these important programs to improve the outcomes of graduates and the KSA’s healthcare sector.
Fitting leadership and management into an already-crowded curriculum
Our findings showed that most interviewees believed that leadership courses should be integrated into the medical curriculum. A review of the literature showed that 2 different approaches were reported by medical schools for offering leadership and management education to students. The first approach is to offer a program that involves cohesive leadership and medical degree prospectuses. However, doing so will require additional years of training. 46 Conversely, a unique study was conducted at KAU (Jeddah) as an extracurricular leadership development program to prepare future Saudi physicians as leaders. It was found that participants’ satisfaction with the overall program was high, with more than 75% of the students reporting an improvement in the group leaders’ leading skills after the program. 47 As a reflection of this theme on the KSA leadership curriculum, of course, curriculum designers should be fully cognizant of the range of options for design and delivery not to copy or import but to inform judgment. 48
Proposed action plan for the implementation of the future designed leadership and management curriculum
We have previously addressed some of the challenges in the delivery of the leadership program. Here, we suggest a potential action plan for the implementation of the future designed leadership and management program.
1. Establishing the need for change by developing leadership for the program and generating support. Broad support is needed, whether internal support from those with administrative authority (dean’s office, program director, faculty, learners, and other stakeholders) for personnel, resources, political support, or, external support from the government, professional societies, philanthropic organizations or foundations, accreditation bodies for funding, political support, external requirements, curricular or faculty development resources.
2. Plan for change: curricular goals should be clearly conveyed to the stakeholders.
3. Identification of resources:
(a) Personnel: faculty, audiovisual, computing, information technology, secretarial & other support staff.
(b) Time: faculty, support staff, and learners.
(c) Facilities: space, equipment, clinical sites, virtual space.
(d) Funding/costs: direct financial costs and hidden costs.
4. Develop administrative mechanisms to support the curriculum; the administrative structure is important to assume responsibility, to maintain communication and to make operational—policy decisions and scholarship (for presenting and publishing about curriculum).
5. Anticipating and addressing barriers: Can relate to finances, other resources, or people.
6. Plan to introduce the curriculum: Pilot, phase-in, and full implementation.
Conclusions
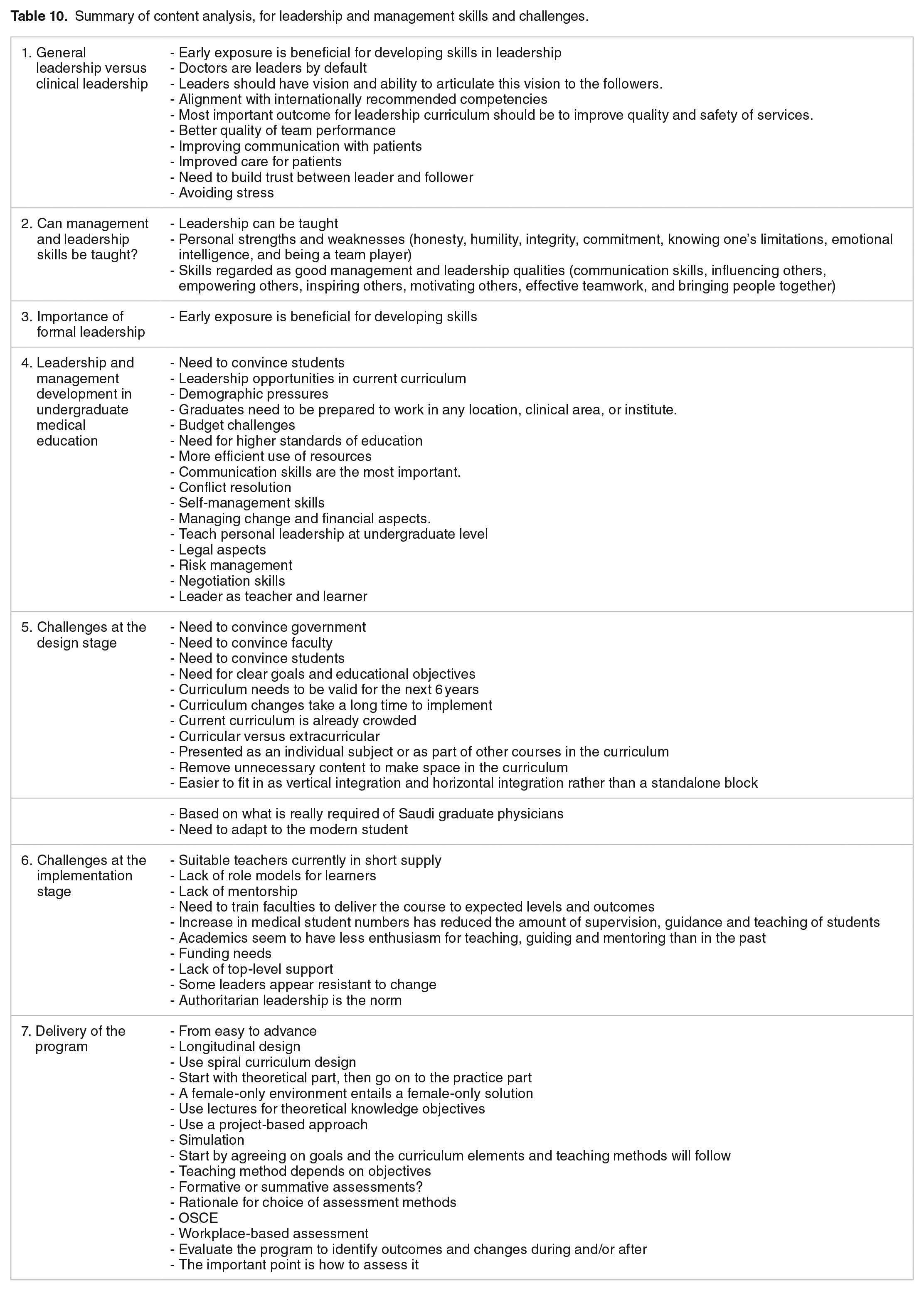
The study revealed significant and detailed information on undergraduate medical education leadership development programs in the Saudi context and the required skills, design, methods of teaching and delivery, and challenges of implementation. Some of the interviewees’ descriptions were in strong agreement, and others were in low agreement. Most of our findings are supported by existing work in the field. Importantly, interviewees described the urgency of such program development because they frequently observed graduates’ insufficient skills to meet the required healthcare delivery. Furthermore, this study provided for the first time, in the context of Saudi medical schools, the required competencies to develop a leadership and management program fit for Saudi Medical Schools (Table 10).
Summary of content analysis, for leadership and management skills and challenges.
Recommendations
Based on the content analysis of the collected data and the literature review on medical leadership and management in general with the noted inadequacy of the data in the literature regarding the Saudi context, the result of this study can help key stakeholders in medical education view the different competencies needed to develop a contextual leadership and management programs for undergraduate medical education at KAU. In addition, we characterized many challenges regarding the design and implementation of such a program in our medical curricula. We recommend government investments in the development of leadership and management programs in medical colleges in the KSA. Further studies are needed to analyze the outcomes of such programs and how to assess these outcomes.
Research implications
The findings of this research are based on the content analysis of the 10 interviews conducted with the stakeholder leaders. These findings need to be further studied to generate high-quality evidence on the urgency of a leadership curriculum and the strengths and weaknesses of the current medical education system in the KSA in general and the medical education at KAU in particular and how it can be improved. To bring evidence-based changes to the medical education of 1 of the Saudi universities, rigorous studies need to be conducted as part of the strategic plans for the improvement and advancement of medical education.
The findings of this research can be helpful in designing a leadership and management course in medical education by characterizing the knowledge, competencies, and methodologies necessary for a management and leadership curriculum. This study’s findings are not meant to be generalized because they specifically target medical education at KAU. However, for researchers who need to conduct studies on leadership and management in a medical education in a similar setting, some of the findings may be of assistance when thinking about the existence of possible problems and potential in that setting.
Limitations
Despite providing many interesting observations, our study has certain limitations. First, the literature review had limited utility in understanding the state of the leadership curricula in Saudi Arabia or among Saudi medical colleges. Hence, the search criteria considered studies that focus on leadership development skills from the USA, the UK, and Canada. Additionally, the participants in the study comprised a select small group, although they had different academic backgrounds. The researcher focused only on undergraduate medical education. The interviews were completed only in the English language, which was limited the potential participants. Because the investigated sample in this study was comprised of leaders holding different responsibilities at the medical college at KAU, finding the appropriate knowledgeable individual to share in interviews was challenging and time-consuming. Additionally, the researcher was inexperienced in conducting effective interviews. Although the researcher was trained for the data collection process, there may have been some element of reporter bias on behalf of the faculty. Finally, the sample size was limited to the size of the interviewing leaders, and the number of qualified respondents within that area.
Footnotes
Acknowledgements
Nisreen Rajeh thanks the medical education department, King Abdulaziz University, for the continued support during the study.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.