
Abstract
Nutrition is a key factor in preventing and treating long-term disease. Patients should be advised to follow evidence-based dietary patterns, such as the Mediterranean diet, which has shown success in preventing or managing a variety of long-term diseases. All health professionals can play a role in providing nutrition advice to patients; however, many have shown an overall low nutrition knowledge and self-efficacy in counseling patients. Because of this, there is a call by health professional organizations for an increase in the applied nutrition education of health professionals. Increasing Culinary Health Opportunities for Professionals is a learn-first, practice second experiential learning program with currently practicing or aspiring health professionals aimed to increase nutrition knowledge, self-efficacy, attitudes, and dietary intake. Currently practicing health professionals (n = 15) and aspiring health professionals (n = 14) were recruited to participate in a 16-week online course on culinary medicine and the Mediterranean diet followed by a 2-week cultural immersion in Tuscany, Italy. Participants were taught the Mediterranean diet and lifestyle, culinary medicine, nutrition counseling, and cultural comparisons in the online course. In Tuscany, participants completed culinary lessons, organic farm tours, food production facility tours, and various tastings of Mediterranean foods. Participants completed a 51-item survey that measured nutrition knowledge, self-efficacy, attitudes, and Mediterranean diet adherence at baseline, post-online education, and post-cultural immersion. Mann-Whitney U tests were used to determine differences in mean scores between cohort 1 (currently practicing) and cohort 2 (aspiring). Results showed that cohort 1 had a greater increase in knowledge (1.07 ± 0.40 vs −0.87 ± 0.40, P = .0069) and self-efficacy (0.74 ± 0.24 vs 0.01 ± 0.24, P = 0.0441) from pre-post course, but at the conclusion of the cultural immersion, there were no significant differences between cohorts in mean changes in attitude, knowledge, self-efficacy, or Mediterranean diet scores from baseline. These results suggest that implementation of this curriculum can be equally effective in increasing nutrition-related attitudes, self-efficacy, and Mediterranean diet adherence for both currently practicing and aspiring health professionals.
Introduction
A variety of health professionals, such as physicians, dentists, nurses, and physical therapists, can play a role in providing nutrition advice to patients.1,2 Many of the leading long-term diseases in the United States are heavily linked to nutrition habits, including cardiovascular disease, obesity, and type 2 diabetes.3,4 With 6 in 10 adults in the United States having a long-term disease, and 4 in 10 having 2 or more, improvement of nutrition habits is increasingly important. 5 In addition, long-term diseases can increase risk of oral health problems, and more than 31.6% of adults aged 20% to 44% and 16.9% of children aged 5 to 19 years in the United States have untreated dental caries, which is linked to nutrition habits. 6 Furthermore, nutrition habits, such as sugar consumption, are linked to oral health diseases such as dental caries, 1 making nutrition counseling in dental visits of extreme importance as well.7,8 Physicians have the highest exposure to patients, accessing 98% of the population, but all health care teams face a range of nutritional issues in which they should provide advice. 9 In some cases, nutrition counseling can be more effective than medication alone in improving patient outcomes. 4 Health care fields are beginning to recognize this, for example, the American Dental Association passing resolutions in 2015 to encourage dentists to maintain current knowledge of nutrition recommendations, and the American Dietetic Association prioritizing nutrition education for health professionals.1,3 Therefore, over the past few decades, there has been a call for an increase in the nutrition education of health professionals across all sectors of health care including dentists, physicians, nurses, health educators, and others.1,3
Despite the acknowledgment of the importance of nutrition education across a variety of disciplines, it is often lacking in curricula. In allopathic medical school, there is on average less than 20 hours of nutrition education in the entire 4 years of instruction and this trend is seen across different health care fields. 4 For example, the mean number of hours devoted to nutrition education among 24 US dental schools was only 15.9 hours. 1 This study also found that 70% of nursing programs did not have a clinical nutrition component, and the use of nutrition education in pharmacy schools often depended on availability of faculty members. 1 This has led to a lack of nutrition knowledge among the health care profession, with 6% of health professionals and 3% of health students achieving a desired score of 80% or higher on a lifestyle modification knowledge examination. 9 The literature is limited thus far, but in studies examining nutrition knowledge of current and future health professionals, scores are consistently low.10,11 Even in the field of dietetics, more experiential and hands-on culinary learning is needed to lead other disciplines involved in culinary medicine. 12
The poor nutrition education of health professionals has led to a lack of confidence in their ability to counsel patients. Recent studies have shown that, overall, physicians lack the confidence to provide nutrition counseling to patients.13,14 Both in undergraduate and continuing education settings, nutrition education appears to be insufficient. 15 For example, nutrition courses in health professional school are typically taught by biochemists, not individuals with training in applied nutrition.1,16 Because of the lack of nutrition knowledge and confidence of health professionals, nutrition experts have suggested that nutritional education across health care fields should focus on applied nutrition and skills such as meal planning and preparation. 16 Along with these suggestions, the field of culinary medicine has emerged and incorporates these concepts. Culinary medicine is an evidence-based field that does not have a set definition, 12 but generally blends the art of food and cooking with the science of medicine and nutrition. 2 Culinary medicine is beginning to be integrated into medical and other health profession school curriculums and often involves hands-on teaching to strengthen students’ knowledge of nutrition and culinary skills. 2
The use of curriculum that incorporates culinary medicine is important to strengthen health professionals’ knowledge in nutrition. In addition, the use of a multidisciplinary approach, with collaboration between dietetics and other health sciences, can increase health professionals’ ability to counsel patients on nutrition. 17 While these strategies are beginning to be incorporated into health education programs, this leaves the currently practicing health professionals a lack of opportunity to enhance their nutrition knowledge and skills. Therefore, finding ways to reach currently practicing health professionals to empower them to counsel patients on nutrition is needed as well. One such way is through online education, which has been found to effectively educate health professionals on nutrition in a convenient manner. 18 However, the use of hands-on learning should still be incorporated to increase self-efficacy. 17
The present study, Increasing Culinary Health Opportunities for Professionals (iCHOP), uses the above-mentioned strategies of both online and hands-on learning, culinary medicine, and a multidiscipline approach to enhance the nutrition knowledge, attitudes, and self-efficacy of future and currently practicing health professionals. 19 This program uses a learn-first, practice second approach 20 and has been implemented in both currently practicing and future health practitioners. As there is debate over at which stage of practice this type of education should occur, 21 the purpose of this study is to determine whether there was a difference in effectiveness of the program on participants’ nutrition knowledge, attitudes, and self-efficacy between 2 cohorts: currently practicing health professionals (iCHOP: Mediterranean, cohort 1) and aspiring health professionals (iCHOP: Aspiring, cohort 2). It is hypothesized that both cohorts will have significantly increased their nutrition knowledge, attitudes, and self-efficacy from preprogram to completion of the program, and no significant differences will be found between cohorts.
Methods
Study design
Target audience
iCHOP: Mediterranean was targeted to currently practicing health professionals from a variety of disciplines: medicine, dentistry, nursing, physical therapy, dietetics, and psychology. iCHOP: Aspiring was targeted to future health professionals, meaning undergraduate students in a health-related field with intentions of becoming a doctor, dentist, nurse, physical therapist, public health worker, or dietitian.
iCHOP: Mediterranean ran from January 2018 to June 2018 and consisted of a convenience sample of 15 health professionals. To participate in the study, they needed to be a currently practicing health professional in the state of West Virginia. In addition, they had to independently fund and participate in both portions of the intervention, the online learning and cultural immersion. iCHOP: Aspiring ran from January 2019 to June 2019 and consisted of a convenience sample of 14 aspiring health professionals. To participate in the study, they needed to be a currently enrolled student in a health-related field. They also had to independently fund and participate in both portions of the intervention, the online learning and cultural immersion. The cost of the intervention was about US$3000 per participant for course credit, lodging, meals, and not including airfare.
Anyone unable to meet these criteria or who failed to complete the informed consent was excluded from the study. Those agreeing to participate enrolled in a 400/500 level course. Anyone interested in taking part in the research study signed informed consent at the start of the online course. No incentives were provided for participation.
Participants were taught the concepts of culinary medicine, nutrition counseling, and the Mediterranean diet and culture on an online, 16-week course (learning component). Following completion of the course, participants traveled to Tuscany, Italy, to participate in a hands-on, experiential cultural immersion for 2 weeks (practicing component). Participants completed surveys at baseline before beginning the online course (T0), after completing the online course (T1), and after return from the cultural immersion (T2).
Program planning and study approval
The iCHOP: Mediterranean program began planning in June 2017. For several months, the itinerary, budget, and collaboration with West Virginia University’s Office of Global Affairs were established. The online course was created using West Virginia University’s eCampus portal and participants received visiting student access for the spring 2018 semester. The iCHOP: Aspiring program began planning in June 2018, using the same program activities on the itinerary, establishing the budget, and again collaborating with West Virginia University’s Office of Global Affairs. This study was conducted in accordance with the Declaration of Helsinki, and the protocols were approved by the Institutional Review Board at West Virginia University (1709753932).
Curriculum development and learning objectives
Curriculum content was developed by experts with doctoral degrees in nutrition and public health, in addition to being registered dietitians, and who have years of experience in long-term disease prevention. The iCHOP curriculum had the following learning objectives: (1) Identify the Mediterranean region and its culinary habits, (2) Explain the key features and health benefits of the Mediterranean diet, (3) Compare Italian and American food systems and further parallel Appalachia and the Mediterranean, (4) Evaluate the changes of the Mediterranean lifestyle over time, (5) Explain the slow food movement, (6) Apply knowledge of the Mediterranean lifestyle in health-related professions, (7) Implement motivational interviewing techniques in practice, and (8) Apply multidisciplinary approaches to problem-solving. The course consisted of voiced-over PowerPoints, peer-reviewed publication reading assignments, and discussions. The course was administered by the individuals who developed the content.
Setting
The online course took place through West Virginia University’s eCampus portal. Participants accessed course content remotely from their locations throughout West Virginia, although most participants resided near West Virginia University’s campus. The cultural immersion portion of the intervention was a 2-week study abroad experience in Tuscany, Italy, in May to June 2018 and 2019.
Recruitment
For iCHOP: Mediterranean, researchers connected with West Virginia chapters of health professional associations. Recruitment emails were sent to contacts found on association websites in addition to West Virginia University’s College of Health Sciences. In addition, hospitals around the state were contacted and flyers were distributed through areas surrounding the university. There were 3 informational sessions held in October to provide individuals the opportunity to learn more and ask questions.
For iCHOP: Aspiring, recruitment emails were sent to contacts in West Virginia University’s College of Health Sciences, College of Agriculture, Natural Resources, and Design, and College of Arts and Sciences to distribute to students in their programs. Flyers were also distributed through areas surrounding the university. For both programs, all applications were completed online and handled by the Office of Global Affairs. Spots were limited due to space restraints with vendors in Italy. The maximum number to recruit for each cohort was 15.
Measures
Both cohorts completed a 51-item survey created uniquely for this study but influenced by evidence-based sources. A version of this survey was originally pilot tested on a sample of West Virginia University medical students (n = 56). 22 This survey was then refined by 2 researchers based on feedback and results and agreed on a final version for these studies. To settle disputes, a third researcher acted as a tiebreaker.
Demographics
Demographic data included age, sex, height in inches, weight in pounds, and current discipline or major, all self-reported. Body mass index (BMI) was calculated by converting height to meters and weight to kilograms and plugging the numbers into the standard formula of kilograms per meters squared.
Mediterranean diet score
The Mediterranean Diet Score was compiled from multiple tools that have been validated in other populations23,24 to assess both diet and lifestyle. Participants provided a yes or no response to these 21 items, which signified whether they performed the behaviors. These included questions such as “Do you use olive oil in your cooking?” and “Do you engage in physical activity more than 30 minutes per day or 150 minutes per week?.” Responses of “yes” were scored as 1 and responses of “no” were scored as 0 and summed with higher scores indicating higher Mediterranean diet adherence.
Nutrition knowledge
The 8 nutrition knowledge questions were on the basics of a Mediterranean dietary pattern, described by cultural experts. 25 Questions were in multiple-choice format and included “If adhering to a Mediterranean diet pattern, which item should be consumed least?” with options of (1) seafood, (2) red meat, (3) poultry, or (4) eggs. Responses were coded (correct = 1, incorrect = 0) and summed for a knowledge score with a range of 0 to 8.
Attitudes
Participant attitudes toward nutrition in medicine and readiness to change were adapted from the Nutrition in Patient Care Survey. 26 This was to develop a set of 10 questions that reflected the Mediterranean focus of the online learning modules and cultural immersion. Participants were asked to rate their feelings from 10 total statements relating to nutrition in medicine on a scale of 0 to 10, with lower values meaning disagreement and higher values meaning agreement. Statements included “I have an obligation to improve the health of my patients including discussing nutrition with them” and “Nutrition counseling should be included in any routine appointment.”
Self-efficacy
Self-efficacy and practice behavior–related questions were influenced by Mihalynuk et al. 27 The survey for this study included 14 concepts or actions, such as benefits of a Mediterranean diet, knowing the MyPlate Guide, etc that participants rated their perceived level of proficiency on a scale of not applicable, not proficient, somewhat proficient, and very proficient. Responses were coded as 1, 2, 3, and 4 accordingly. Self-efficacy ranged from 0 to 56.
Procedure
Web-based education
At the beginning of spring semester in 2018 and 2019, iCHOP Mediterranean and iCHOP Aspiring participants completed informed consent and the baseline survey (T0). Participants then received 16 weeks of web-based education. The content was divided into self-paced modules with a focus on the Mediterranean diet and lifestyle, nutrition as medicine, cultural comparisons, and personal implementation. In each module, digital slide presentations, required readings, and additional sources were provided. The semester concluded in May, after which participants completed the posteducation survey (T1).
Cultural immersion
iCHOP Mediterranean’s 2-week cultural immersion began 2 weeks after the conclusion of the semester. iCHOP Aspiring’s 2-week cultural immersion began 1 month after the conclusion of the semester due to scheduling conflicts with the Italian vendors. Both cohorts participated in hands-on learning and experiential activities including multiple cooking lessons both in countryside homes and esteemed culinary schools, organic farm tours, production facility tours (ancient grains, olive oil, cheese, wine, etc), and Mediterranean tastings (wine, cheese, olive oil, etc). The group learned from cultural experts, experienced traditional Italian meal time, and experienced the culture of Tuscany. Upon return to the United States, participants completed the postimmersion survey (T2). All responses were obtained within 2 weeks.
Statistical analysis
Survey responses were reported as ratings on ordinal item scales. Results are reported as means alongside standard deviations. Differences between mean nutrition knowledge, attitudes, and self-efficacy scores between the 2 cohorts at T0, T1, and T2 were calculated using the Mann-Whitney U test. Differences between mean changes in scores from T0 − T1, T1 − T2, and T0 − T2 were calculated using the Mann-Whitney U test. In all statistical analyses, significance criterion alpha for all test was 0.05 and a statistical trend was declared when P < .1. Internal reliability of the survey scales used was measured using Cronbach alpha. All analysis was conducted using JMP Pro Version 12.2.
Results
A total of 15 individuals participated and met eligibility criteria for the iCHOP: Mediterranean study and a total of 14 individuals participated in and met eligibility criteria for the iCHOP: Aspiring study. The mean age for iCHOP: Mediterranean was 43 ± 16.92 years and the mean age for iCHOP: Aspiring was 21.9 ± 3.15 years. The mean BMI for iCHOP: Mediterranean was 28.7 ± 7.86 and the mean BMI for iCHOP: Aspiring was 24.1 ± 2.99. Student’s t test was conducted and a significant difference in the mean ages between each cohort (P = .0002) and in BMIs (P = .0483) was found. iCHOP: Mediterranean participant disciplines included nutrition, dentistry, respiratory therapy, psychology, nursing, health department IT, life coaching, and physicians. iCHOP: Aspiring participants had future aspirations of registered dietitians, obtaining a PhD in nutrition, working in the neonatal intensive care unit, obtaining a master’s in public health, medical school, becoming a neuroscientist or neurosurgeon, become a physician assistant, and becoming a policymaker for underserved communities. Table 1 lists mean ages for both cohorts and results from the t test.
Ages for cohorts 1 and 2.

Abbreviation: BMI, body mass index.
Results from student’s t test showed a significant difference in mean ages and in mean BMIs between the 2 cohorts.
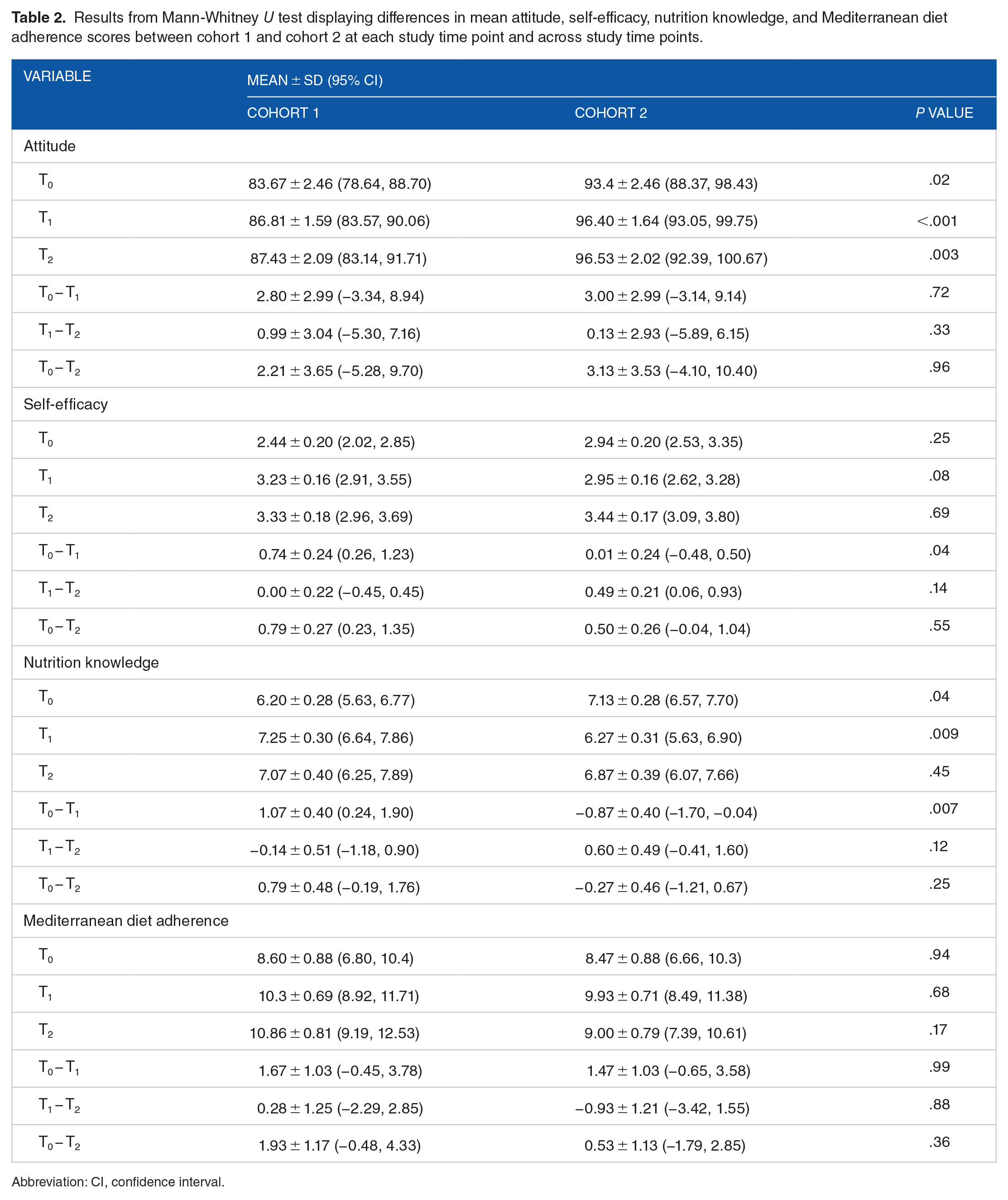
The attitude scale (α = 0.78), self-efficacy scale (α = 0.96), knowledge scale (α = 0.70), and Mediterranean diet scale (α = 0.63) all demonstrated accepted reliability. At T0, there was a significant difference between cohort 1 and cohort 2 in mean attitude scores (P = .02), with cohort 2 having higher scores. There was also a significant difference in mean nutrition knowledge scores (P = .04), with cohort 2 having higher scores. There was no significant difference in mean self-efficacy scores (P = .25) or mean Mediterranean diet adherence (P = .94) between cohorts 1 and 2. At T1, there was a significant difference between cohort 1 and cohort 2 in mean attitude scores (P < .001), with cohort 2 showing higher nutrition scores. There was also a significant difference in mean nutrition knowledge (P = .009), with cohort 1 showing higher nutrition scores. Self-efficacy scores were trending toward significance, with cohort 1 showing higher self-efficacy (P = .08), and no significant difference in mean Mediterranean diet adherence (P = .68). At T2, there was a significant difference between cohort 1 and cohort 2 in mean attitude scores (P = .003), with cohort 1 showing higher attitudes, but no significant difference in mean self-efficacy scores (P = .69), mean nutrition knowledge scores (P = .45), or mean Mediterranean diet adherence (P = .17).
When examining changes in mean scores of cohorts 1 and 2 from T0 − T1, there was a significant difference in self-efficacy (P = .0441) and nutrition knowledge (P = .0069), but no significant difference in changes in mean attitude scores (P = .7200) or mean Mediterranean diet adherence (P = .9917). From T1 − T2, there were no significant differences in changes of mean attitude scores (P = .3332), nutrition knowledge (P = .1206), Mediterranean diet adherence (P = .8884), or self-efficacy (P = .1424). From T0 − T2, there were no significant differences in changes of mean attitude scores (P = .9571), self-efficacy (P = .5537), nutrition knowledge (P = .2495), or Mediterranean diet adherence (P = .3577). However, from T0 − T1 and T0 − T2, the nutrition knowledge scores of cohort 2 showed a decrease (−0.87 ± 0.40, 95% confidence interval [CI] −1.70, −0.04, and −0.27 ± 0.46, 95% CI −1.12, 0.67, respectively). In addition, a decrease in Mediterranean diet scores was seen from T1 − T2 in cohort 2 (−0.93 ± 1.21, 95% CI −3.42, 1.55), but from T0 − T2, there was an overall increase (0.53 ± 1.13, 95% CI −1.79, 2.85). Table 2 displays results from Mann-Whitney U analysis at each time point and across study time points.
Results from Mann-Whitney U test displaying differences in mean attitude, self-efficacy, nutrition knowledge, and Mediterranean diet adherence scores between cohort 1 and cohort 2 at each study time point and across study time points.
Abbreviation: CI, confidence interval.
Discussion
This study investigated the differences in outcomes between currently practicing and aspiring health professionals in implementation of a culinary medicine, hands-on curriculum that used the learn-first, practice second model. It was hypothesized that there would be no differences between cohort 1 (currently practicing) and cohort 2 (aspiring) in their nutrition knowledge, attitudes, self-efficacy, and Mediterranean diet adherence throughout the duration of the study. At baseline, T0, there were no significant differences in any of the measured variables except attitudes and nutrition knowledge, where we observed cohort 2 to have higher scores in both. This could be attributed to the fact that Mediterranean diet awareness is increasing, and nutrition knowledge among younger generations has shown to be overall greater.28,29 At T1, which was the conclusion of the online learning and before the cultural immersion, difference in mean self-efficacy scores was trending toward significance, and mean nutrition knowledge scores were significantly different, with cohort 1 showing higher scores in both domains. This could indicate that cohort 1 had a greater benefit from the online course. At T2, which was at the conclusion of the cultural immersion, no significant differences in mean scores between the cohorts were observed, possibly indicating that the immersion was equally beneficial for both cohorts.
When examining differences in mean changes of scores across the study, it was observed that cohort 1 had a statistically significant greater increase in self-efficacy and nutrition knowledge from T0 − T1, reinforcing the possibility of cohort 1 having a greater benefit from the online course. No other significant changes were seen in any of the measures from T1 − T2 and T0 − T2. At the conclusion of the study, we saw higher nutrition knowledge and Mediterranean diet adherence in cohort 1, but higher self-efficacy in cohort 2. However, the differences were not statistically significant.
There are several possible explanations as to why we saw greater increases in nutrition knowledge and self-efficacy in cohort 1 than in cohort 2. According to adult learning theory, adults prefer responsibility for their learning and desire self-direction. 30 The online course relies on self-management for learning, and the older age of cohort 1 may have been more equipped to do so. In addition, adult learning theory states that adults have a greater volume of experiences, which can be a resource for learning, have internal motivation, and prefer learning that is life centered. 30 It is possible that because cohort 1 was older, had more experiences to relate to, and more internal motivation, they had more effective learning in the online course. It was observed that by the conclusion of the study, there were no significant differences in mean scores of any of the measures, suggesting the overall effect of the curriculum was equal in both cohorts. The use of experiential learning was integral to this study. Experiential learning theory states that learning reflects a continuing process, and relies on immediate personal experience, the context and surroundings in which the learning occurs, and creating meaning for the learner. 31 Tangible experiences, such as cooking activities and participation in observational learning from experts, were the backbone of the curriculum in the cultural immersion and reinforced the previously learned concepts from the online course, such as nutrition needs for type 2 diabetes. The combination of concrete experiences and abstract concepts are key for experiential learning. 31 It was observed that the use of experiential learning and the learn-first, practice second model was effective for both cohorts in improving nutrition attitudes, self-efficacy, and Mediterranean diet adherence. However, only the currently practicing health professionals had an increase in nutrition knowledge from T0 − T2, whereas the aspiring health professionals showed a decrease in knowledge.
There are several limitations to this study. There were overall small sample sizes in each cohort. This was largely due to budget and space limitations for the cultural immersion. There was also a difference in the time between the course ending and the immersion occurring between 2 groups, and the greater gap between these times in cohort 2 may have caused a decrease in the knowledge gained from the course due to not being required to study the material for a month between these time points. This was due to scheduling conflicts with the lodging facilities and planned activities in Italy, requiring the immersion to be moved to several weeks later than planned. In addition, not all health professionals and students have the financial means and schedule flexibility to participate in an immersion like this. The financial barrier poses several limitations. Sustainability and scalability of this program is a potential issue due to these costs. In addition, the fact that participants had personal investment in the immersion may have led them to more enthusiastically participate, potentially affecting results. Furthermore, translating the concepts of the Mediterranean diet to the health-disparate Appalachian population may be difficult. However, within the curriculum, comparisons to Appalachian culture were made, and throughout the course and immersion, participants were prompted to apply how they would translate Mediterranean concepts to counseling Appalachian patients through their personal journaling. The results from the qualitative portion of this study analyzing the journal data are published elsewhere. 32 Currently, there is no long-term follow-up to determine how the curriculum may have changed the behaviors and practices of participants in their professional and personal lives. Future work will aim to investigate how to lower the costs of the program and determine the long-term impacts of this curriculum.
Determining if implementing this curriculum is more effective in currently practicing or aspiring health professionals has several important implications. First, we were able to establish that it is possible to teach individuals who are no longer enrolled in a formal institution about nutrition as medicine and the Mediterranean diet. This is important because as nutrition and culinary medicine are increasingly implemented in medical and other health professional schools, currently practicing health professionals are left without these resources. The use of online and experiential learning for these individuals like in this study is a viable option to enhance the nutrition knowledge, attitudes, and self-efficacy of health professionals and therefore potentially enhance the effectiveness of their care. Second, providing this effective opportunity to undergraduate, aspiring health professionals is important to establish a foundation of nutritional and culinary knowledge to equip them as they continue their education and apply the learned concepts. Finally, depending on time, involved institutions, resources, access to participants, and other factors, it may be more feasible to implement this curriculum with 1 cohort over the other, and establishing the effectiveness in both cohorts is important to ensure that whichever age group is plausible can be worthwhile.
Conclusion
This study investigated whether implementing the learn-first, practice second model in a culinary medicine cultural immersion would yield differences between currently practicing health professionals and aspiring health professionals in their changes in nutrition knowledge, attitudes, and self-efficacy. Results showed that overall, there were no differences in mean scores from study beginning to end, suggesting that the complete effect of the online course and cultural immersion was similar between the 2 cohorts. While the financial barrier is a significant limitation, future work can determine how to make this curriculum more cost-effective while maintaining its core components. Providing unique and dynamic learning opportunities such as this for both current and future health professionals can effectively improve their nutrition knowledge, attitudes, and self-efficacy and possibly, in turn, their patient care.
Footnotes
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by WV Agricultural and Forestry Experiment Station (WVA00689 and WVA00721) and West Virginia University Office of Global Affairs
Author Contributions
M.D.O., R.A.W., and R.L.H. created study design and collected the data. R.A.W. and R.L.H. analyzed the data. M.D.O. and R.A.W. wrote the first draft with contributions from R.L.H. All authors reviewed subsequent drafts and approved the final manuscript.