
Abstract
Objective:
To evaluate the effects of a nutrition education programme conducted during health education lessons on students’ adherence to the Mediterranean Diet (MD) and their body mass index (BMI).
Design:
Quasi-experimental pre-test/post-test research design: two study conditions (intervention and control groups).
Setting:
Two urban schools, the 11th and 21st primary schools in Limassol, Cyprus.
Method:
Two hundred and thirty-five fifth- and sixth-grade students participated in the programme. One hundred and fifteen were in the intervention group school (the 11th primary school), and 120 were in the control group school (the 21st primary school). Students in the intervention school participated in nine 80-minute lessons during the health education class. The curriculum focused on the MD and included cooking activities, food tasting and parental involvement. The primary outcomes were subsequent adherence to the MD, nutritional knowledge, self-efficacy physical activity and BMI.
Results:
Following the implementation of the intervention, the intervention group showed a significant increase in nutritional knowledge, self-efficacy and adherence to the MD (p < .001). The intervention group also had significantly higher nutritional knowledge and MD Quality Index scores than the control group (p < .001). However, no effect was observed on children’s BMI (p > .05).
Conclusion:
The intervention successfully improved children’s dietary habits in the intervention group by increasing adherence to the MD, but it did not affect their BMI. The results show some promise for addressing poor nutrition through education.
Keywords
Introduction
Adopting healthy eating habits is a key goal of health promotion programmes, given their crucial role in combatting non-communicable diseases such as obesity (Cerf, 2021; World Health Organization, 2016). Implementing health promotion programmes for children is vital as dietary habits formed in childhood are likely to persist throughout adulthood (Mikkilä et al., 2005).
Schools are ideal settings in which to implement health promotion programmes due to the large number of children and the potential for interventions in different aspects of school life, including in the curriculum (Sahota et al., 2001). In schools, preventive lifestyle interventions, such as improving the nutritional value of children’s food, have been shown to improve nutritional behaviours significantly (Steyn et al., 2009). Success factors for school-based interventions include a nutrition-based curriculum taught by trained teachers, a parental involvement component, a programme lasting more than 5 months in duration and with a solid foundation in behavioural theory (Murimi et al., 2017; Rana and Alvaro, 2010; Steyn et al., 2009).
One theoretical approach widely used in health promotion is social cognitive theory (Conner and Norman, 2015). Social cognitive theory addresses both the personal and social structural determinants of health (Bandura, 1998) and identifies critical factors influencing behaviour (Conner and Norman, 2015). Core determinants of health-related behaviour include knowledge, perceived self-efficacy outcome expectations, clear goals and a focus on perceived facilitators as well as social and structural impediments (Bandura, 2004). Social cognitive theory has been effectively utilised in developing and implementing interventions to improve health-related behaviours such as nutrition (Bagherniya et al., 2017; Hall et al., 2015) among preschool (Nixon et al., 2012) and primary school children (Bashirian et al., 2021; Hall et al., 2015) in school settings.
The Mediterranean Diet (MD) is a healthy eating pattern that includes a high consumption of plant-based foods, such as fruit, vegetables, whole-grain bread, cereals, pulses and nuts. Olive oil is a key component of this diet, and meat is only consumed a few times each month, with a preference for lamb, poultry, rabbit or fish. Yoghurt and cheese are made widely available, and milk consumption is lower compared with current intakes in Spain (Serra-Majem et al., 2004). The MD has been associated with lower rates of mortality (Trichopoulou et al., 2003), lower body weight (Buckland et al., 2008) and beneficial effects for the prevention and the management of childhood diseases such as asthma and allergies (Chatzi and Kogevinas, 2009; Razquin and Martinez-Gonzalez, 2019), as well as adult-onset cardiovascular disease (Willett, 2006), metabolic syndrome, cancer, Parkinson’s disease and Alzheimer’s disease (Sofi et al., 2008). Intervention programmes promoting adherence to the MD have been implemented in adults to prevent and manage cardiovascular diseases (Serra-Majem et al., 2006) and cancer (Hernáez and Estruch, 2019; Mentella et al., 2019) and in children to promote healthy lifestyles (Piana et al., 2017).
The dietary habits of children and adolescents in Cyprus are often of poor quality (Lazarou et al., 2009), resulting in rising obesity rates (Pigeot et al., 2009; Savva et al., 2014). Compared with eight European countries participating in the
It is crucial therefore to improve the dietary habits of Cypriot children through effective interventions. Following the educational reforms of 2011–2012 and the introduction of health education into the school curriculum, opportunities arose to develop such an intervention in the form of a nutritional education programme. However, no textbooks or evaluated materials were present in the Health Education curriculum at that time, except several thematic units assigned for teaching at each grade level, opposing the published literature’s suggestion about the procedure that must be followed for effective development and evaluation of health promotion programmes (Drapeau et al., 2016; Warren et al., 2003).
The main goal of this study therefore was to develop, implement and evaluate a nutrition intervention programme to increase adherence to the MD through health education lessons given to fifth- and sixth-grade (10–12 years old) children. This study was one of the first programmes to implement and evaluate the uptake of, and adherence to, an MD among children – brought about by school health education lessons. More specifically, the study sought to investigate whether children’s higher adherence to an MD can impact their body mass index (BMI).
Methods
Study design, participants and procedure
The study was conducted in two public primary schools in Limassol, Cyprus. Health education teachers were invited to participate in the recruitment of schools, and two large primary schools (the 11th and 21st primary schools of Limassol) agreed to join the study, with one randomly assigned as the intervention group (the 11th primary school) (A) and the other (the 21st primary school) assigned as the control (B). School A received the programme, and school B received regular teaching. Altogether, 235 fifth- and sixth-grade students aged 10–12 years old in the 2 schools were involved in the study. In school A, 115 children participated, and in school B, 120 children formed the control group.
Pre- and post-programme questionnaires were used to identify any differences between the groups regarding adherence to an MD, nutritional knowledge, self-efficacy and physical activity. Anthropometric data on weight, height and body mass index (BMI, kg/m2) were collected before and after programme implementation. Data collection took place during September 2015 and March 2016. The questionnaires were administered by a trained nutritionist (KM), who was a member of the research team.
The study protocol was approved and conducted according to the guidelines of the Cyprus Ministry of Education, Culture, Sport and Youth (Approval No. 7.15.09.2). The permission of the participating schools’ principals and the written agreement of the parents/guardians of the participating students was obtained after principals and parents had been fully informed about the study objectives and methods.
Intervention
The intervention took place between October 2015 and March 2016 as part of health education lessons, which take place every 2 weeks and last for 80 minutes. It was delivered by the health education teacher at the intervention school. Health education teachers in both schools were trained nutritionists.
Educational material supportive of the intervention was developed in line with the project’s needs. It included informational leaflets and interactive nutrition education activities, including food tasting and preparing simple healthy snacks. These activities have been shown to improve nutrition quality and self-efficacy in food preparation (Larson et al., 2009; Nation et al., 2003).
The intervention programme itself consisted of 9 lessons delivered over a 6-month period as part of the home economics classroom. Both boys and girls participate equally in these classes. Each lesson was devoted to a specific topic, including the MD pyramid, MD food groups, the recommended consumption of each food group and its relationship to health outcomes, breakfast choices and reading food labels.
The first lesson introduced the MD diet and the MD pyramid. The following six lessons focused on a different MD food group each time and were divided into four parts. First, children tried new foods from the food group under study (e.g. when studying the fruit group, they tasted various fresh, dried and preserved fruit). Second, they learned about the nutritional benefits of the food group (e.g. by exploring the health benefits of eating fruit regularly). Third, they prepared a simple and healthy snack related to the food group (e.g. a fruit salad) and set a fortnightly goal (e.g. eating at least two to three different kinds of fruit every day). Fourth, they discussed their progress and ways to overcome the challenges they encountered. In the last two lessons, students were taught how to prepare nutritious breakfasts and healthy snacks as an alternative to unhealthy packaged foods.
Families in the intervention group received an informational newsletter throughout the programme, while the parents and guardians in the control group received no additional feedback beyond the consent form. The newsletter outlined the programme’s goals and significance for children’s health, emphasising the importance of cooperation for success. It also included suggestions for encouraging the child to achieve nutrition goals, making target food groups available and accessible and modelling good nutrition habits. A final newsletter sent to parents and guardians of children at the intervention school provided information on programme implementation and results. Furthermore, each child in the intervention group received a personal goal-setting leaflet as part of programme implementation. Every 2 weeks, they wrote down their nutrition goals for the period concerned and had their parents or guardians sign it to encourage shared responsibility and increase the likelihood of success.
In the control school, the health education teacher simply delivered the health education lessons included in the formal health education curriculum. The fifth and sixth grade curriculum includes four lessons that focus on healthy eating and food groups and include a focus on knowledge and cooking activities, but without family involvement.
Measurement
Questionnaire
A questionnaire distributed to children was used to assess the programme. It consisted of five parts: adherence to an MD, nutrition knowledge, self-efficacy, physical activity and sociodemographic information. A nutritionist, a research team member (KM) administered the questionnaire to the children in each school, reading each section and explaining any unfamiliar words. Afterward, the children completed the defined sections.
The first part of the questionnaire assessed adherence to an MD using the Mediterranean Diet Quality Index for children and adolescents (KIDMED). The KIDMED is an index which validates adherence to Mediterranean dietary patterns (Serra-Majem et al., 2004). The index ranges from 0 to 12 and is based on responses to a 16-question test. Questions/statements that do not support adherence to the MD like ‘I eat sweets more than 2 times daily’ are assigned a value of −1, and those which support adherence to the MD such as ‘I eat two fruits daily’ are given +1. The sum of the values achieved enables the child’s response to be classified at one of three levels: (1) ⩾8, optimal MD; (2) 4–7, improvement needed to adjust intake to Mediterranean patterns and (3) ⩽3, very low diet quality.
The second part of the questionnaire assessed nutritional knowledge by means of 11 dichotomous (yes/no) items, with each correct answer receiving a score of +1. The maximum possible score is 11. The nutrition knowledge part included statements concerning the health benefits of the MD and its food groups, as well as their recommended consumption. Some examples of the questionnaire items are: ‘Eating one fruit or vegetable a day is enough to provide all the necessary nutrients for the body’. ‘Using olive oil is highly beneficial for health as it protects a range of diseases’.
The third part of the questionnaire assessed self-efficacy through eight statements about the child’s confidence in performing specific nutrition-related actions. Response categories were not at all, a little, fairly, much and too much. Examples of the statements are ‘If I set a goal about my diet e.g., eat more fruit, I will find ways to achieve it’ and ‘I can make myself a simple healthy snack like a sandwich or salad’. Values from 1 to 5 were given for each statement (1 = not at all, a little = 2, fairly = 3, much = 4 and 5 = very much). The total score was the sum of these values, with the maximum score being 40. This part was developed after studying the work of Contento et al. (2002) who describe the main types of questions for measuring self-efficacy, as well as the University of California Fruit and Vegetable Questionnaire (Townsend and Kaiser, 2007), part of which assesses self-efficacy.
The fourth part of the questionnaire assessed physical activity using part of the survey used in the Physical Activity, Nutrition and Allergies in Children Examined in Athens (PANACEA) study conducted in Athens, Greece (Priftis et al., 2007). Children completed a questionnaire rating how often in the week they participated in 18 different physical activities such as walking, cycling, running, playing football and so on for at least 20–40 minutes each time, on a scale of 0 (0 days) to 7 (7 days a week). Each activity is given a score from 0 to 7 based on weekly engagement.
The fifth part of the questionnaire assessed demographic characteristics such as sex, grade (fifth or sixth), age, country of birth, accommodation status (living with whom) and parents’ educational level.
The research team developed parts 2 and 3 to evaluate self-efficacy and nutrition knowledge and part 5 to assess demographic characteristics. Parts 1 and 4 on the contrary were adapted from previous research conducted on Greek-speaking populations of the same age group.
The children’s questionnaire was assessed for its validity. It was distributed to 35 fifth- and sixth-grade children in the 21st primary school of Limassol, 1 school year before programme implementation, and no problems were identified with understanding and completion. It was also tested for reliability using a retest method with a 2-week space. It was completed by 72 fifth- and sixth-grade children at the same school and was validated using Cronbach’s alpha. Both internal and external reliability were above .70 for all parts.
BMI
The height and weight of each student were measured by a trained nutritionist from the research team in the health service office at the respective schools. BMI was evaluated using a stadiometer provided by the School Health Service, which was consistent across both schools. Height was measured in centimetres and weight was measured in kilograms, with the first decimal place included for weight (e.g. 50.4 kg). BMI was calculated for each child by dividing their weight by the square of their height (kg/m²).
Data analysis
Descriptive analysis in terms of means, standard deviations and percentages was conducted for the variables examined in the total sample. A mixed-way ANOVA was used to evaluate changes within and between groups at the beginning and end of the programme. Schools/groups were fixed factors and time was the factor with repeated measures. Dependent variables included the MD Quality Index (MD index), nutritional knowledge score, self-efficacy, BMI and physical activity. Paired t-tests were used for within-group tests, while t-tests for independent samples were used for between-group tests. Non-parametric Mann–Whitney tests were used to analyse non-normally distributed data. Data were analysed using SPSS version 23.0.
Findings
At the start of the study, before the nutrition intervention, there were no significant differences between the intervention and the control group, in age, gender, country of origin, accommodation status and parents’ educational level. Table 1 summarises baseline participant characteristics.
Comparison of baseline sociodemographic characteristics between the intervention group and the control group.
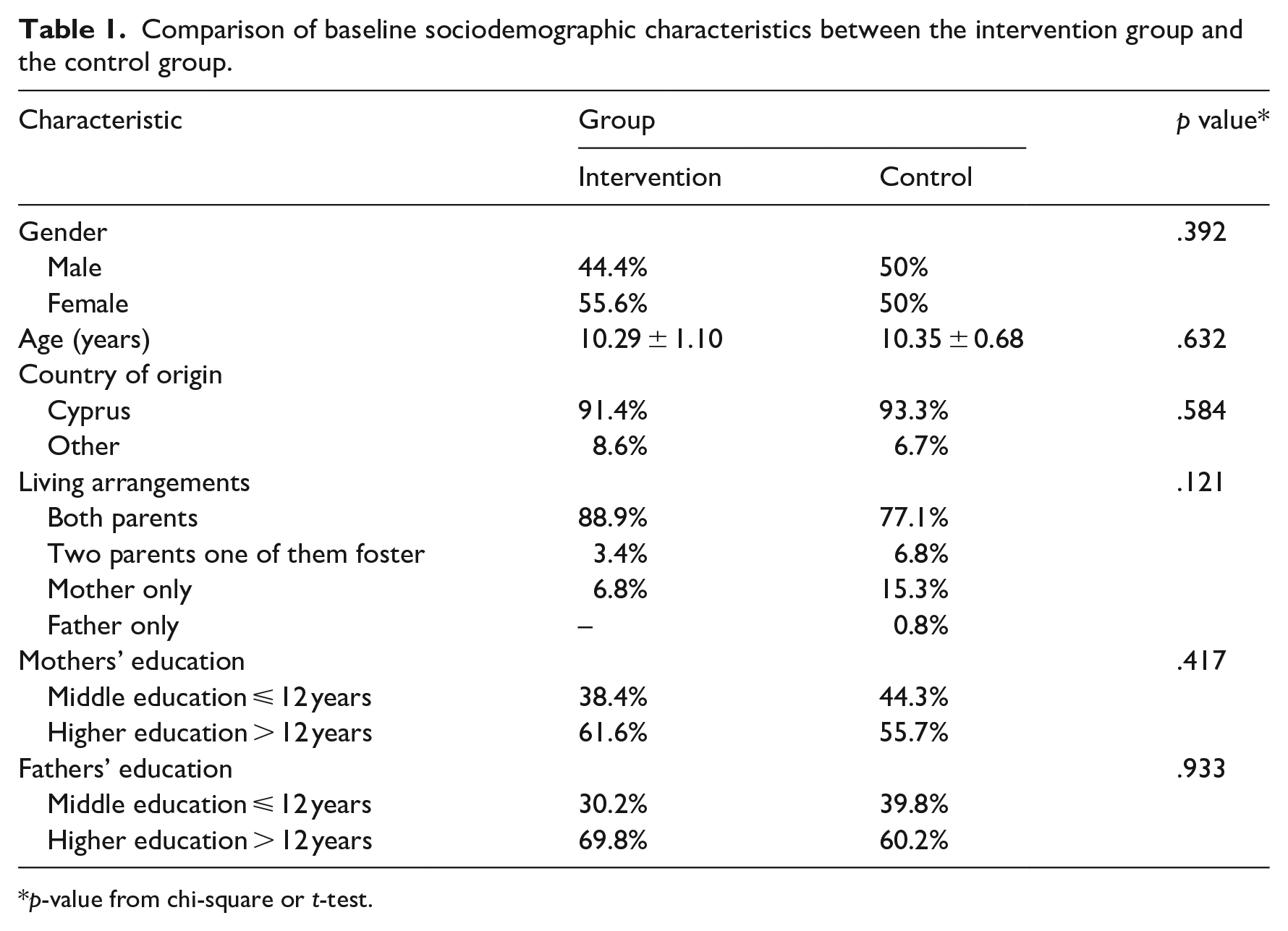
p-value from chi-square or t-test.
Average scores for outcome measures
Changes in children’s behaviour can be expressed through average scores of nutritional knowledge, MD index, self-efficacy and physical activity as presented in Table 2. The last two columns of Table 2 with the p-values refer to the comparison between the two groups before and after the implementation of the intervention programme.
Average scores and results in the main parts of the children’s questionnaire before and after the intervention, within and between groups.
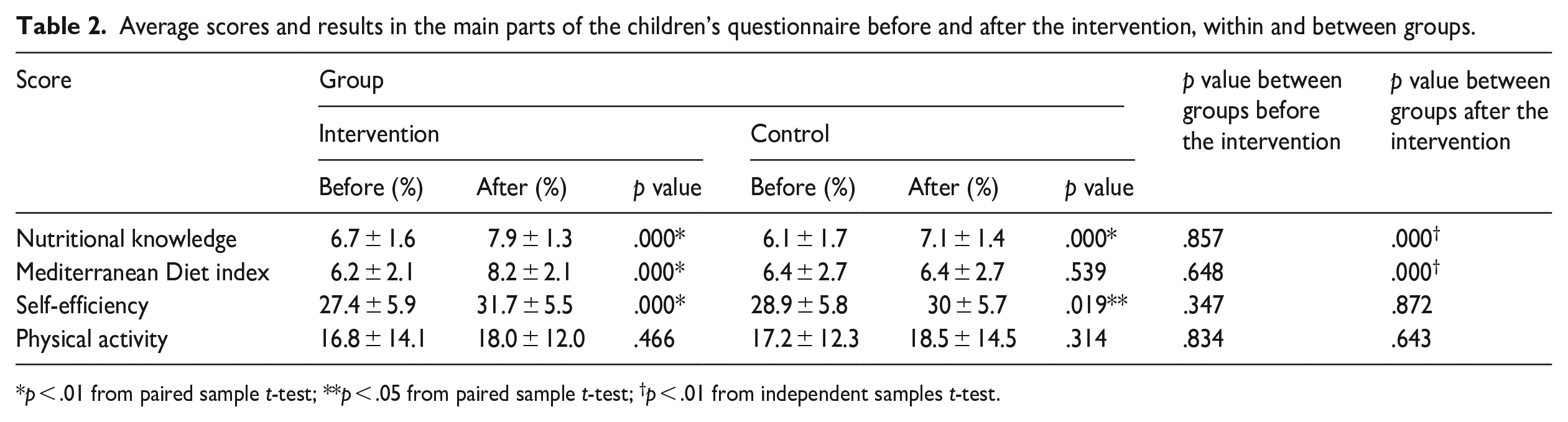
p < .01 from paired sample t-test; **p < .05 from paired sample t-test; †p < .01 from independent samples t-test.
Adherence to the MD
The MD index divides adherence to an MD in three ways, as detailed earlier. Table 3 compares adherence to an MD diet in the intervention and control groups. There was a significant increase in level 3 responses among intervention group children, showing high MD adherence. Conversely, control group children decreased over time in level 1 and level 3 responses, resulting in medium (level 2) MD adherence for most children. Comparing before and after values for the MD index using the Chi-square test, it was found that the change was significant for the intervention group but not for the control group.
Adherence to Mediterranean Diet (MD) according to the MD index before and after the intervention.
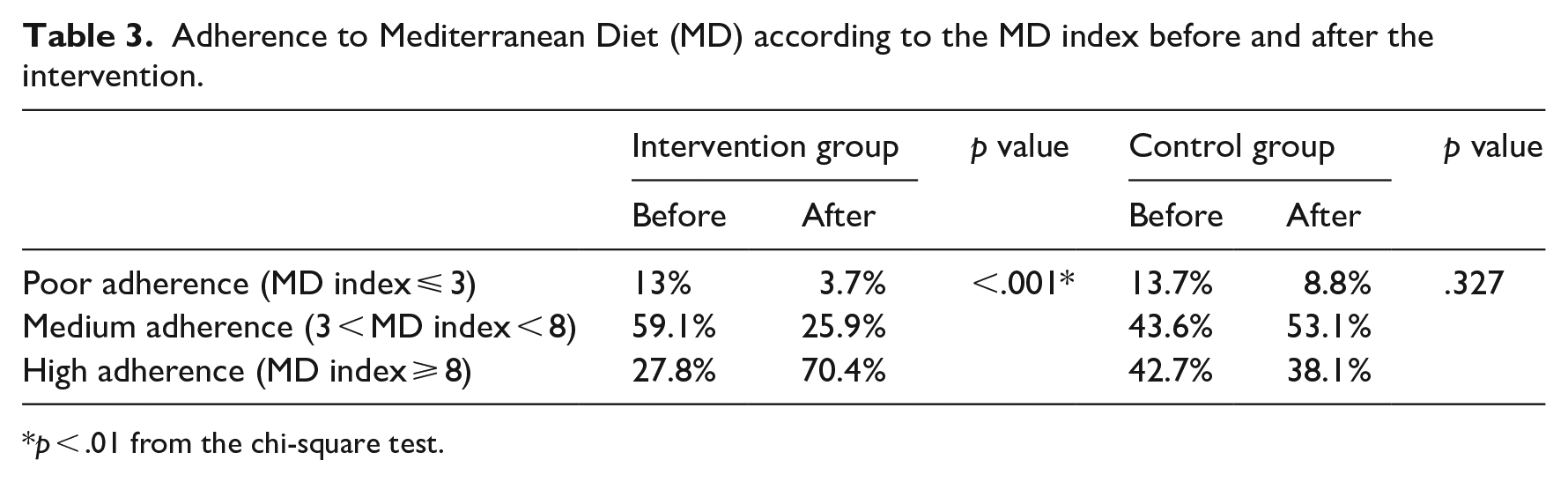
p < .01 from the chi-square test.
In Table 4, we report on the consumption of various food groups, within groups, before and after the intervention. Most of the intervention group members reported positive changes, thus the significant increase in this group’s total MD index score at the end of the intervention. More specifically, there was an increase in the consumption of fruit, vegetables, fish, dry nuts, olive oil and dairy products and a decrease in the use of baked products, sweets and fast food – no changes were observed in the consumption of legumes, pasta, rice and cereals at breakfast time. In the control group, we observed an increase in the consumption of daily fruit or juice and dry nuts at the end of the intervention. These changes, however, had no significant impact on the total score for the MD index in the control group at the second evaluation which was conducted at the end of the study.
Positive answers to each statement of the Mediterranean Diet (MD) index questionnaire before and after the intervention.
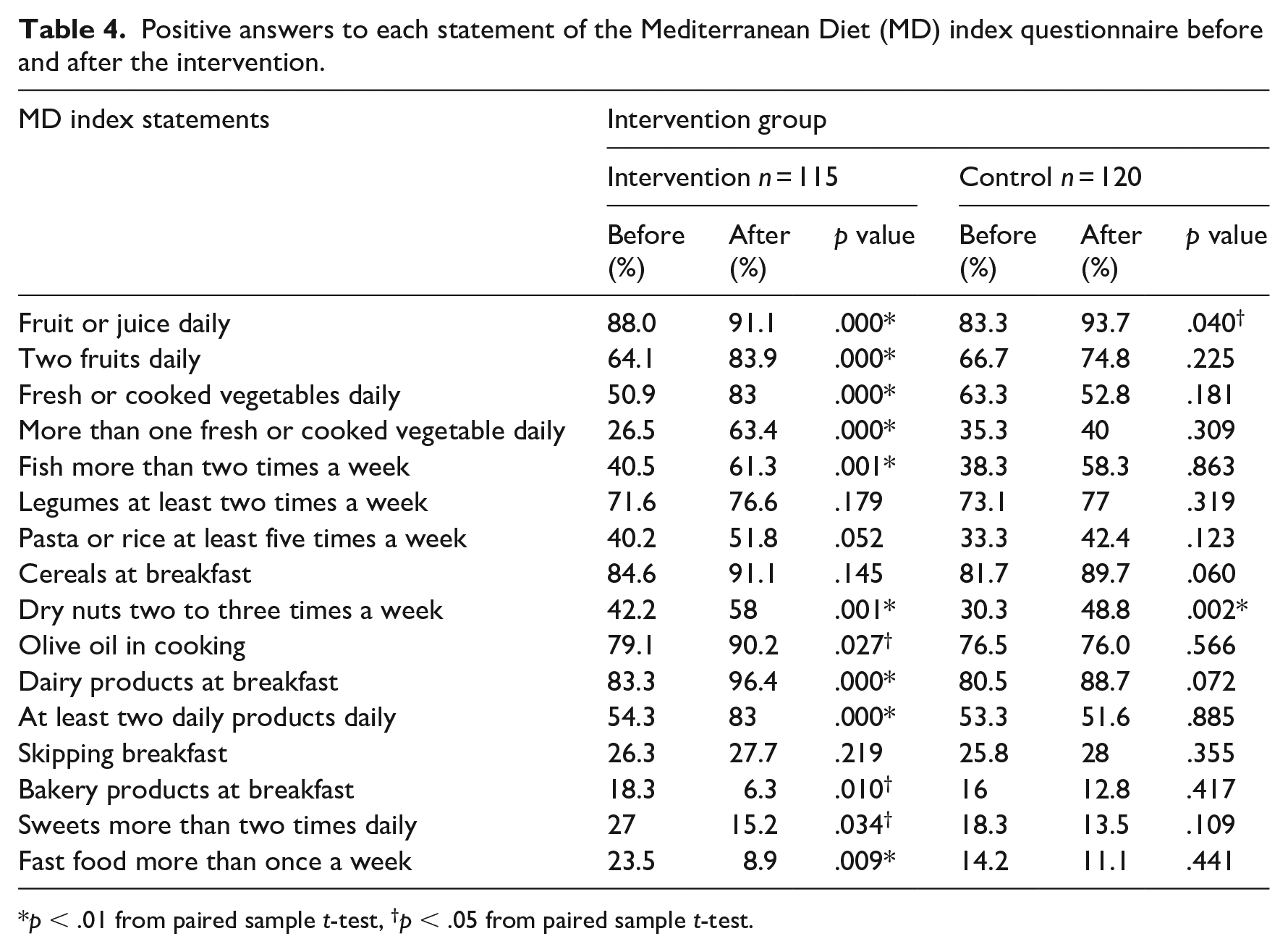
p < .01 from paired sample t-test, †p < .05 from paired sample t-test.
Children’s anthropometric characteristics
The comparison of height and weight of all participants showed no significant differences between the repeated measures. Similarly, there was no significance in BMI between the two groups. The comparison of height, weight and BMI between the two groups assessed by the repeated measures showed no significant differences. However, there was an increase in the height and weight of all participants between the start and end of the study, likely due to rapid development at this age. Table 5 shows the anthropometric characteristics of children before and after the intervention.
Anthropometric characteristics of children before and after the intervention.
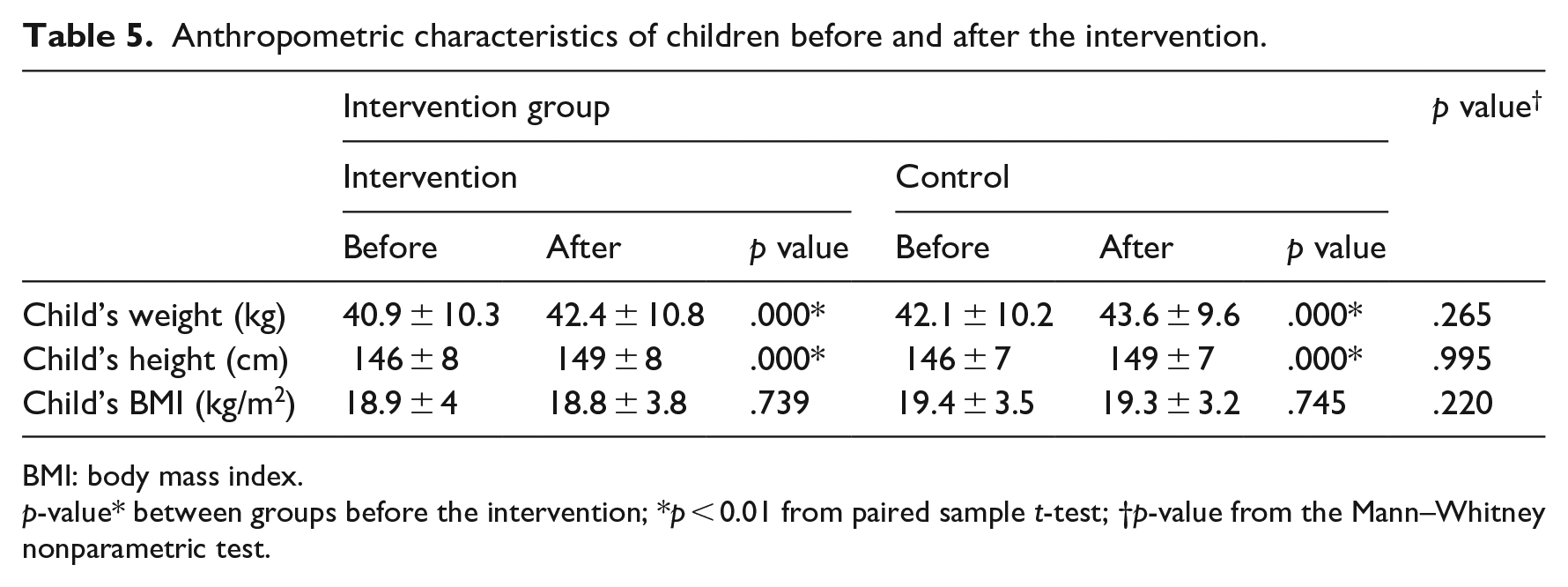
BMI: body mass index.
p-value* between groups before the intervention; *p < 0.01 from paired sample t-test; †p-value from the Mann–Whitney nonparametric test.
Discussion
This paper describes the short-term effects of a nutrition intervention programme aiming to increase adherence to the MD among fifth- and sixth-grade elementary students through health education lessons and associated parental support. The programme showed success as the MD index score increased significantly only in the intervention group, creating a notable difference between groups that was not evident in the initial evaluation. This improvement was associated with significant changes in intervention group nutrition habits at the end of the programme. More specifically, there was a substantial increase in the consumption of fruit, vegetables, dairy products, fish and olive oil and a significant decrease in the consumption of sweets and fast food.
These positive results are in line with the findings of Piana et al. (2017) who also reported an increase in the MD index to primary school children after the implementation of a 4-month multicomponent intervention. Our positive results in changing nutrition-related behaviour are also in line with the findings of other nutrition intervention programmes delivered through the curriculum as part of nutrition education lessons (Fahlman et al., 2008; Ochoa-Avilés et al., 2017) as well as interventions involving the Cypriot elementary school population (Perikkou et al., 2013).
Based on the MD index scores, most children showed moderate adherence to an MD at the start of the programme in both groups. However, at the final evaluation, the vast majority of the intervention group children showed high adherence to the MD, while no significant changes were observed in the control group, with most children showing only moderate adherence to the MD, similar to the first evaluation.
We noticed a significant increase in knowledge at the end of the programme in both groups but only in the intervention group was there a positive change in nutrition habits. The weak link between knowledge and behaviour is well documented and exists in other intervention programmes where a significant increase in student’s knowledge does not lead to any clear-cut behaviour change (see, for example, Prelip et al., 2012).
The same is true of self-efficacy. At the end of the programme, there was a significant increase in both groups’ self-efficacy, but only the intervention group displayed nutrition habit changes. Although self-efficacy is considered a key factor in behaviour change (Bandura, 2004), the achievement of a change in dietary behaviour change requires a ‘continuum of factors working together’ (Rolling and Hong, 2016: 1).
This study investigated whether a higher adherence of children to an MD would improve their BMI. In this study, there was no significant difference in the children’s BMI between or within groups. This could be attributed to the fact that it is one-dimensional, and the target in this study was an improvement in the quality of children’s nutrition. No activities targeted an increase in physical activity. According to some researchers (Evans et al., 2015; Wang et al., 2015), BMI improvement is more likely when children simultaneously engage in good nutrition and physical activities. Delivering a multi-dimension programme such as this, however, would require the involvement of many teachers, something not feasible in a study involving health education teachers alone.
Importantly, an improvement in children’s BMI could occur in the future. According to some researchers, adherence to an MD does not have a direct connection to a lower BMI (Buckland et al., 2008; Trichopoulou et al., 2005), but people who have high adherence to such a diet are less likely to become obese (Razquin et al., 2010; Schröder, 2007), with likely knock-on effects for BMI later in life.
Limitations
The study has some limitations that must be noted. The sample was derived from only two primary schools in one city; therefore, they are not representative of the children’s population in that city or in Cyprus, and no generalisation of the findings results can occur. Moreover, there was no follow-up after the end of the programme, and the questionnaires used were self-administered. Future evaluations need to identify medium- to longer-term consequences and assess change in a more detailed manner with a focus on other obesity indices such as waist-to-height ratio and body fat percentages.
Conclusion
This programme is the first intervention that has aimed to increase adherence in MD to primary school children in Cyprus through health education lessons, by enriching the current curriculum and engaging parents.
Findings suggest that both parents and schools have a critical role to play in creating healthy environments and facilitating the development of healthy habits and skills related to nutrition in children. By collaborating with each other, they can establish a supportive framework that motivates children to adopt and sustain healthy dietary habits.
Interventions of the kind implemented here may have longer-term benefits. Based on the findings of this study, we suggest incorporating nutrition education into the school curriculum and developing policies that promote healthy eating habits. To enhance efficacy and possible effectiveness, future programmes might emphasise the importance of the MD as a part of the national heritage.