
Abstract
Anatomy Academy is a simultaneous service-learning experience for preprofessional school undergraduate students and preclinical professional students acting as classroom paraprofessional teachers (Mentors), and engaged-learning experience for fourth to sixth grade elementary school children (Students). Using didactic and kinesthetic active learning teaching strategies in small-group classroom environments, Mentors taught anatomy, physiology, and nutrition concepts to Students. In this study of the program’s early years (2012-2014), overall objectives of improving Mentors’ pedagogical confidence; and Students’ science interest, science knowledge, and exercise self-efficacy were assessed. Mentors showed (89% response of 595 surveyed) improvement in content delivery (P < .001), student engagement (P < .001), classroom management (P < .001), and professionalism (P = .0001). Postprogram Mentor reflections were categorized into 7 major themes that demonstrated personal growth through the service-learning opportunity: (1) realization of an ability to make a difference in the world now; (2) acknowledgment of the importance of listening in teaching; (3) recognition that lives can and will change with “a little love”; (4) insight into the effectiveness of guiding Students through material rather than lecturing; (5) awareness of the value of respect in the learning environment; (6) cognizance of the power of individualized attention to motivate Students; and (7) reflection of one’s own personal growth through the open influence of Students. Students showed (88% response of 1259 surveyed) improvement in science knowledge (P = .014) and exercise self-efficacy (P = .038), but not science interest (P = .371). Thus, while Students are learning more science and becoming more aware of their health, we need to be more overt in our presence as scientists in the educational arena.
Keywords
Introduction
Teaching in medicine takes on multiple forms, but 2 predominate: teaching in the historical context of medical education as an apprenticeship-based endeavor, and the teaching that occurs near-constantly between medical professionals and their patients.
Formalized teaching structures in the preclinical years equip students with prerequisite knowledge necessary for entering the clinical setting. During the clinical years, resident, fellow, and attending physicians integrate patient cases with salient teaching points. In addition, on a daily basis, physicians and medical students teach patients about pathophysiology, preventive health, and disease management.
With these multiple responsibilities in mind, the Liaison Committee on Medical Education (LCME) has determined that those in teaching positions, including resident and fellow physicians, should be “prepared for their roles in teaching and assessment.” 1 Yet a 2011 letter to the editor by Shariq and other medical student colleagues highlights the need for “enhancing the teaching skills of medical students.” Unfortunately, competing educational priorities and low value perception have been identified as major limitations to implementing courses and programs dedicated to establishing teaching skills in medical professionals.2,3 Given the lack of requirement for physicians to receive formal or informal training in pedagogy before or during residency, a need exists to equip future physicians with the tools necessary to become effective teachers as well as to address the barriers against incorporating teaching instruction. A small niche (less than 10%) of medical students can elect for a “teaching distinction tract,” if offered at their school, to prepare them for a career in medical education. 4 The issue is not isolated to the field of medicine. Other health professions students find themselves in the same drought of teaching opportunities and, while there are some opportunities for service-learning engagement, current programs rarely focus on application of teaching skills, but instead, still notably, expose students to diverse and underserved community initiatives.5,6
Service learning in higher education
The exposure that preprofessional and professional students receive when participating in service learning provides an opportunity to apply the knowledge and principles taught during their formal education. It also often allows interaction with underserved and diverse socioeconomic communities, which will expand students’ abilities to empathize with and communicate with individuals from diverse backgrounds. The LCME requires that medical schools encourage students to be involved with community-identified concerns, and through that service, they are involved in the preparation and reflection on “relationships among their participation in the activity, their medical school curriculum, and their roles as citizens and medical professionals.” 7 Opportunities for service off campus allow for students to learn in situations that would otherwise be very difficult to recreate or simulate in the classroom. Interprofessional teamwork and collaboration is emphasized and valued by students from multiple allied health disciplines as they serve together in the community. 8
A review of published accounts of service learning in medical education posited academic learning and professional development, personal development, and enhanced citizenship and social responsibility as the overarching outcomes of student involvement. 9 Celebration of student efforts and positive reinforcement through posters, awards, and potential publication are top ways of encouraging involvement, as top-ranked medical students are less likely to participate in service-learning opportunities opting for more traditional scientific research. 10 Despite the positive evidence surrounding service learning, not all students have a positive experience, which might be more coupled with the vision and organization of the program, than the experience itself. 11 When considering the many programs that have been established, teaching focused service learning is definitely the exception and not the rule, despite opportunities available at various universities. 12
Teaching focused service-learning and outreach programs
The need for improved teaching skills of physicians and other allied health professionals can be evidenced by the aforementioned deficiencies and other anecdotal experiences by medical students, residents, and even patients. While many teaching programs exist for undergraduates pursuing education, little exposure is offered to students in science or preprofessional career tracks, although the occasional project can be found. 13 Some medical schools have recognized this deficiency and have initiated a variety of training programs for their residents tasked with the responsibility of teaching and guiding medical students. 14 Other medical schools offer student-run clinics to increase clinical reasoning and interprofessional behaviors. 15 Dandavino et al highlight the importance of training medical students as teachers for establishing doctors with better communication. This can lead to better learning, for both doctor and patient, and ultimately a better future for the health care profession and industry. 16 One way some medical schools have addressed the issue is through “peer-teaching” initiatives for senior students to teach select topics in short sessions to underclassmen, often during Anatomy.17,18 A review of the literature revealed 19 studies (from nearly 400) that addressed the topic of peer teaching and showed the same model of senior students teaching peers or lowerclassmen, nearly exclusively in medicine. 19 The opportunity and need for training the student as the teacher are particularly apparent in allied health professions, with great potential for interprofessional applications, as well as flipped classroom teaching modalities. 20 In most of these (near) peer-teaching initiatives, the content and activities are still developed by current faculty, and then delivered by the students, or in the case of the flipped classroom, delivered online, and discussed in small group. In addition, due to the level of content delivered (medical or professional level), it is possible that many students would be more focused on the accuracy of material than development of pedagogical skills. Finally, another common method of higher education outreach is practitioner-scientists investigating improved methods of education; however, these are often limited in their breadth of impact and have minimal student involvement.21,22 Furthermore, the ultimate goal of these research studies is aimed at assessing and improving education at the elementary through high-school level, and while noble and necessary, this does not fill the need of teaching those skills to medical students or professionals. 23 Unfortunately, the majority of universities and graduate medical education programs simply do not require, let alone offer, these types of teaching training programs to the majority of their medical students.
Nonteaching focused outreach and service programs
Much more common are outreach programs focused on providing a service to a specific demographic, age group, or discipline without either a focus on improving teaching skills of university students, or even including university students at all. These types of programs are necessary to provide a service to the community but fail to achieve an impactful learning experience by the volunteers, if there are any volunteers. Many programs aim at impacting the deficit of STEM interest by a “train and equip” method, where university professors give workshops to K-12 teachers, enabling the K-12 teachers to impact STEM interest. 23-25 These teacher workshops are helpful for illuminating the optimum delivery of content to those teachers but do not reveal much about the students taught by those teachers, and do not allow for participation and growth of the students of the university professors running the workshops. 26 Many outreach programs focus on providing a service to the community, but there is seldom vision or occasion to include mentorship into the existing models. Failing to include undergraduate and graduate students in teaching the content and interacting with the audience reduces the potential growth of the student volunteers and potentially minimizes the impact of the students receiving the service. Using university-level students as volunteer teachers provides a larger paraprofessional resource for schools while simultaneously enhancing the communication and teaching skills of the volunteers. 27 In addition, the students receiving the service are benefited by lower student to teacher ratios and the opportunity to connect with someone who can serve as a young adult role model. This opportunity is what Anatomy Academy sought to capitalize on to enhance the learning experience of both the university mentors and the elementary students.
A program called “Anatomy Academy” was formulated and implemented in the Summer of 2012 to provide opportunities for professional students-in-training at the David Geffen School of Medicine at UCLA (DGSOM), Brigham Young University (BYU), University of Utah School of Medicine (UUSOM), and Utah Valley University (UVU) to engage in teaching roles in the anatomical and health sciences disciplines early in the course of their education. Anatomy Academy allows preprofessional school undergraduate students and professional students to serve as classroom paraprofessional teachers (Mentors) and simultaneously practice and improve their teaching skills for the subjects of anatomy, physiology, and nutrition over the course of 6 to 7 weeks, once a week, to children between 4th and 6th grade (Students). Likewise, Students were exposed to contextual, integrated science and health through engaged-learning activities. As a service-learning opportunity, Anatomy Academy is designed to augment, not compete with, other educational priorities for Mentors in undergraduate and professional school curricula. As an engaged-learning opportunity, Anatomy Academy is taught either during the science or physical education/health instructional periods of the elementary or middle-school schedule or as an after-school program.
Service-learning theoretical frameworks applicable to Anatomy Academy
Formalized service-learning opportunities in higher education involve a partnership between a university and elementary and middle schools through which Mentors apply personal experience-based knowledge and newly acquired classroom-based knowledge in a contextual, engaged-learning environment. In this partnership, faculty can act in advisory or mediator roles to help Mentors meet learning objectives.
A number of theoretical frameworks exist for the establishment of service-learning opportunities, most notably the philanthropic model,28,29 civic engagement model,30,31 and com-munitarian model.32,33 In short, in the philanthropic model, universities fulfill a social responsibility by helping students learn skills for their own moral and epistemological development.28,29 In the civic engagement model, universities advocate for partnerships and provide resources necessary to help faculty and students acquire transformational skills to become agents for social change.30,31 In the communitarian model, universities are microcosms for their communities. Faculty and Mentors are partners in learning multidisciplinary skills that focus on improving interpersonal relationships and citizenship, which thereby improves the community.32,33
Within the aforementioned 3 major theoretical frameworks of service learning, many different combinations of service-learning conceptual frameworks can exist. Anatomy Academy is designed as an experiential learning program, within the conceptual framework of cognitive development theory34-36 and constructivist epistemology 37 that learning is naturally accomplished in an active, purposeful environment. 38
Specifically, with regard to cognitive development theory, the Anatomy Academy curriculum places 8-10 Students in a small group to work with 2 Mentors. The learning environment provides a high teacher to student ratio to facilitate dynamic conversations: Mentors encourage Students to interact with one another as they hear didactic information, explore knowledge through interactive activities, and work together to understand the application of knowledge to common clinical conditions (i.e. the relationship between emphysema and lung microanatomy). Activities are typically multimodal—visual, auditory, and kinesthetic—which lends to the highly engaged environment.
With regard to constructivist epistemology, the Anatomy Academy curriculum includes a large-group activity with all Students working together or in their teams to solve or simulate concepts. For instance, the cardiovascular lesson large-group activity involves Students and Mentors simulating movement of red blood cells (students) exchanging carbon dioxide (blue gym ball) for oxygen (red gym ball) in the simulated lungs, or vice versa in the simulated body tissues. This particular activity plays out like a large obstacle course outdoors or in a gymnasium. Each school site performs this activity differently because Students and Mentors construct the simulation uniquely.
Service-learning options and requirements vary at DGSOM, BYU, UUSOM, and UVU. The following reasons listed for participation in service-learning opportunities extend beyond assumed inherent humanitarian motivation. At the DGSOM, students are highly encouraged to participate in service-learning opportunities, but are not required to do so. For students enrolled in Human Anatomy at BYU, or Honors Biology at UVU, participation in Anatomy Academy fulfills a class service-learning requirement. Anatomy Academy is 1 of 2 options for BYU anatomy students. Since 2012, participation has increased from approximately 25 students in a semester, to an average of 100 students per semester in a class of 400 students. All UVU Honors Biology students in a class of 12 are required to participate each semester. Students at UUSOM were required to fulfill a minimum of 64 community service hours, 32 of which must be classified as “vital,” defined as supervised service hours. Anatomy Academy is categorized as a “vital” service opportunity. From among both preclinical medical classes of 105 students each, approximately 30% participated in each semester.
Anatomy Academy objectives
We have identified 2 main objectives for our university and elementary school clients: (1) provide a service-learning pedagogical opportunity for preprofessional and professional students; (2) integrate science and health curricula at elementary schools to improve science knowledge, science interest, and exercise self-efficacy through engaged-learning activities.
To meet our objectives of helping preprofessional undergraduate and preclinical professional students gain confidence in teaching medical concepts, 3 service-learning goals were implemented: (1) to learn, synthesize, and distill medical concepts to a fourth- to sixth-grade education level; (2) to engage socioeconomically disadvantaged Students in Title 1 schools (more than 40% of students receive free or reduced lunch) and nondisadvantaged students in non-Title 1 schools and; (3) to establish a high teacher to student ratio of 2 Mentors per 4 to 8 Students that establishes effective small groups that cater to student-specific teaching and learning styles.
To meet the objective of improving science knowledge, science interest, and exercise self-efficacy, we established a highly engaging small-group, engaged-learning curriculum that consisted of the following attributes: (1) a Mentor to Student ratio of approximately 2 to 8; (2) a didactic instructional period during which Mentors taught Students anatomy, physiology and nutrition; (3) a kinesthetic instructional period during which Mentors and Students applied concepts learned during the didactic period through a large-group activity (such as an obstacle course or kinesthetic object lesson).
Materials and Methods
Setting and participants
The Anatomy Academy program was initially implemented from 2012 to 2014 at 12 elementary and middle schools in the Greater Los Angeles, CA and Salt Lake City, UT areas through interdisciplinary partnerships with the DGSOM (Los Angeles, CA), BYU (Provo, UT), UVU (Orem, UT), and UUSOM (Salt Lake City, UT). Partner schools were chosen primarily based on the interest of teachers and Principals/Directors to provide their Students with additional or augmented instruction in science and physical education. The 12 participating schools (see Table 1) included (* indicates a Title 1 school) *Stella Middle Charter Academy (Los Angeles, CA), Salt Lake Arts Academy (SLC, UT), Canyon Rim Academy (West Jordan, UT), Harvest Elementary (Saratoga Springs, UT), *Franklin Elementary (Provo, UT), Freedom Academy (Provo, UT), *Greenwood Elementary (American Fork, UT), *Mana Academy Charter School (West Valley, UT), *Hillcrest Elementary (Orem, UT), *Cherry Hill Elementary (Orem, UT), Odyssey Charter School (American Fork, UT), and Sego Lily Elementary (Lehi, UT). Among these schools, Anatomy Academy is actively implemented in a total of 30 classrooms, with an average enrollment of 30 students per class.
List of schools that participated in Anatomy Academy from 2012 to 2014.
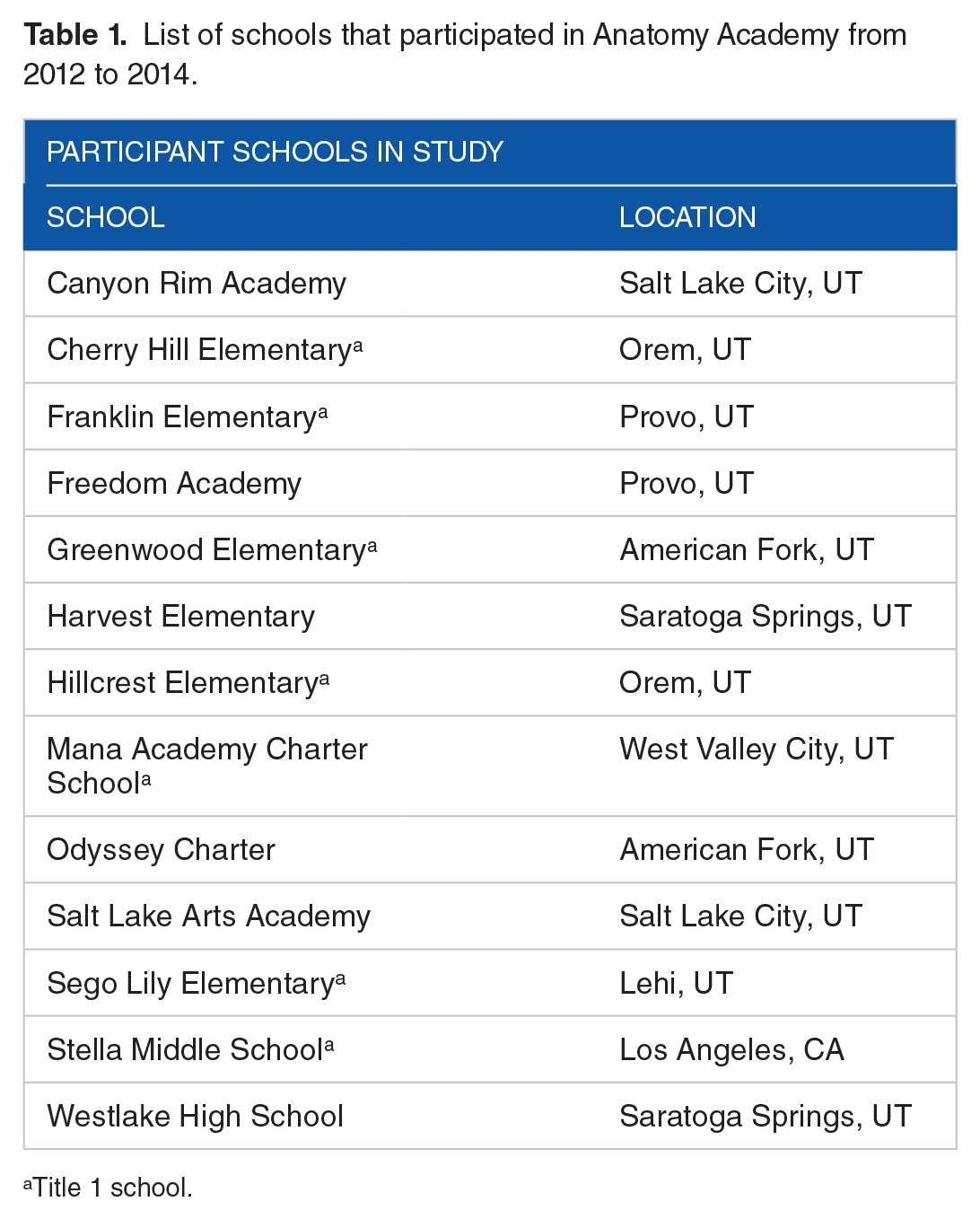
Title 1 school.
Preprofessional and preclinical students at these institutions served as Mentors. Coordinators were recruited from the ranks of experienced Mentors.
To become a Mentor, university students completed an application that requested demographic information and schedule availability. Although Mentors were not expected to have extensive experience in describing clinical conditions or completely understanding classroom discipline, reasonable answers to the following additional questions in the application were required as follows:
Please describe (in approximately one paragraph) why you are applying to be an Anatomy Academy Mentor.
Please describe (in approximately one paragraph) how you would describe the concept of the “carotid pulse” to a fifth grader.
Please describe (in approximately one paragraph) how you would manage a disruptive student.
To become a Coordinator, experienced Mentors completed an application that included demographic information, schedule availability, previous experience as a Mentor, suggestions for improving Anatomy Academy, and finally the following classroom-management questions:
Please describe (in approximately one paragraph) how you would inspire your Mentors to be creative in their pedagogy, use the heart lesson as an example.
Please describe (in approximately one paragraph) how you would manage a Student who refuses to participate.
Anatomy Academy is an institutional review board (IRB)-approved program at all participating universities. At the initiation of Anatomy Academy, Faculty served as Coordinators. Mentors were recruited through formalized classroom enrollment as a service-learning requirement or option. Mentors ranged in experience from first-year undergraduate students in preprofessional health care tracks to second-year medical, dental, or nursing advanced degree students. The 290 male (48.7%) and 305 female Mentors (51.3%) self-reported good academic standing (Grade Point Average [GPA] is not checked, but the classes from which Mentors are recruited require demonstrated academic rigor) and rarely repeated the program, since they were recruited through a service-learning requirement for their class, major, or professional school. Those who continued in the program from semester to semester typically became Coordinators. Each Mentor was given a pseudo-random, 5 to 7 digit Anatomy Academy ID that was used in place of an identifier for the surveys and the reflections. Presurveys and postsurveys and reflections were matched using this unique identifier. Coordinators did not take the Mentor surveys.
Elementary and middle-school children were recruited through participating classes. To participate in the research study, parents signed a consent form, and their children signed an assent form. If either parent or child does not sign the consent or assent form, respectively, the child was not included in the study. However, in order to ensure that all children felt included during the Anatomy Academy activities, no one was excluded from the learning activities regardless of whether they participated in the study components. Indeed, Anatomy Academy at all of the aforementioned schools was an integral part of each class’ curriculum. The teachers always remained in the classroom and were asked to intervene in cases of severe misbehavior, but otherwise played a minimal role in the program, besides scheduling and communication with coordinators. Each Student was assigned a pseudo-random, 5 to 7 digit Anatomy Academy ID that was used in place of an identifier for the surveys. Presurveys and postsurveys were matched using this unique identifier.
Program description—training
Anatomy Academy aimed to provide Mentors with opportunities to develop teaching skills, as well as to provide elementary and middle-school students with introduction to anatomy, physiology, and nutrition concepts. This was accomplished using a hierarchy of leadership. University Faculty who implemented the service-learning activity at their institution trained or assisted with the training of Coordinators in a 2-hour session. During the training session, Coordinators learned the administrative mechanics of coordinating the Anatomy Academy lessons with the school partners—classroom teacher and principal/director. This included distribution of parent consent and child assent, assigning Anatomy Academy ID numbers, and coordinating the distribution of preprogram and postprogram surveys. In as much as each school, and teacher, had preferred methods for distributing the research forms, the role of Coordinator was extraordinarily important. In addition, Coordinators learned how to manage Mentor teams. This included providing Mentors support for teaching their group of children and assisting with discipline when necessary.
With assistance from Coordinators, university faculty provided a 3-hour training for the Mentors at least 2 weeks before the Anatomy Academy program was launched each semester. Mentors were provided with a packet of information that included the following materials prior to the training:
Description of the Anatomy Academy program.
Mentor expectations.
Mentor consent form.
Mentor preprogram self-evaluation survey (the postevaluation survey was administered by the Coordinators at the conclusion of Anatomy Academy at the end of the semester).
Principles of classroom management.
Parent consent form.
Student assent form.
Student surveys.
The Anatomy Academy curriculum and supplies.
During the training, Mentors were guided through the entire packet of materials by the Faculty. Coordinators assisted the Faculty during the description of the curriculum by providing ideas for implementing the principles of each lesson to the Mentors on their team.
Program description—curriculum
The Anatomy Academy curriculum focused on 7 organ systems: musculoskeletal, cardiovascular, pulmonary, upper gastrointestinal, lower gastrointestinal, peripheral nervous, and central nervous. Depending on school schedules, Coordinators had the option of combining peripheral and central nervous system lessons. The copyrighted curriculum is available upon request, but a summary of the upper gastrointestinal lesson, as an example, is provided in Figure 1. Each Anatomy Academy lesson is delivered once a week for 6 to 7 weeks during a 1-hour instructional period in the classroom (Figure 2).
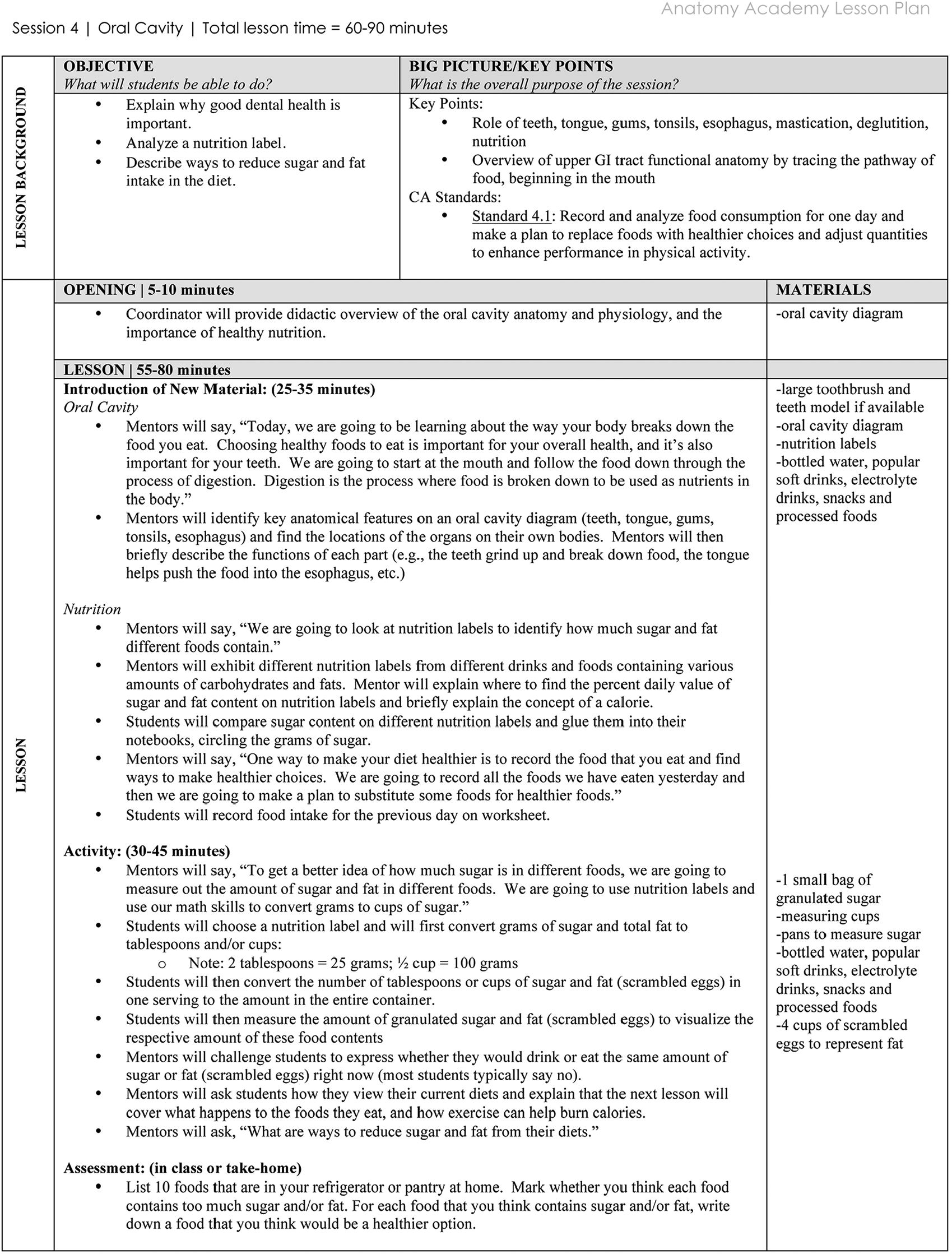
An example Anatomy Academy lesson. This lesson depicts the upper gastrointestinal lesson, which focuses on oral health and nutrition. Each Anatomy Academy lesson includes suggested total and activity allocation Time, Objectives, Big picture/key points (based on State of California physical education standards), Opening, Lesson, and Materials.

Anatomy Academy in action: (a) Coordinators and Mentors teaching Students how to convert grams of sugar on food labels into cups, then visualizing the number of cups of sugar in various foods and drinks at Stella Middle Charter Academy. (b) Mentors and Students performing jumping jacks while breathing through straws to demonstrate the effect of emphysema on cardiovascular performance at Stella Middle Charter Academy. (c) Students examining gastrointestinal organs of a mouse during the field trip to UCLA. Note the facial expressions. (d) Demonstration of cardiovascular anatomy using an ultrasound during the field trip to UCLA. Please refer to http://youtu.be/r6bN073FGOs to view the full Anatomy Academy Video, a recent BYU feature of the program at http://education.byu.edu/news/2013/07/15/the-science-of-hands-on-learning/, and a radio conversation with Julie Rose of Top of Mind at https://www.byuradio.org/episode/2e80e368-63c4-4f15-8f76-7e1cc947b6b4?playhead=2412&autoplay=true.
On the first day of Anatomy Academy, Mentors and Students worked together to establish learning goals and behavioral expectations. In a typical classroom of 30 Students, the Coordinator managed approximately 5 teams of 2 Mentors. The Mentors have the liberty to decide how to teach the curriculum to their Students. Thus, the high teacher-to-student ratio allows for a needs-based engaged-learning environment. Anatomy Academy videos and a radio conversation with Julie Rose of Top of Mind demonstrate the engaged-learning environment: Stella Middle Charter Academy Brigham Young University, McKay School of Education feature of Anatomy Academy
http://education.byu.edu/news/2013/07/15/the-science-of-hands-on-learning/
Radio conversation with Julie Rose of Top of Mind https://www.byuradio.org/episode/2e80e368-63c4-4f15-8f76-7e1cc947b6b4?playhead=2412&autoplay=true.
At the beginning of each 1-hour instructional session, the classroom Coordinator provided a short, 5-minute whole-group “introduction to new material.” This allowed the Coordinators to model effective teaching practice for the Mentors. Mentors then worked in a small-group format for approximately 25 minutes, guiding their Students through the individual lesson plans, and interjecting active learning approaches to concepts. Each lesson plan consisted of a guided practice and application activity (Figure 1). During the last 30 minutes of each lesson, the Coordinator and Mentors worked together to implement a large-group activity. Depending on the lesson, activities typically involved some sort of kinesthetic activity. In the case of the example lesson provided in Figure 1, the large-group activity consisted of Mentors guiding their Students through the reading of nutrition labels found on packaged drinks and foods and the respective measurement of sugar and fat content (see Anatomy Academy videos cited above).
In summary, after a short introduction by the Coordinator, Mentors teach Students the base curriculum for approximately the first half of the instructional period. Mentors typically teach concepts through the use of coloring sheets, journal entries, computer applications and activities, and physical activities. Then, during the second half of the instructional period, the Coordinator organized the large-group activity in which all small groups participate together.
Coordinators were responsible for communicating lesson topics, and activity plans with Mentors in the days before each session and were prepared to step into the mentor role should the need arise. Mentors could rely on Coordinators for student behavior issues, content questions, and scheduling problems. Coordinators communicated directly with the school teachers and administration for scheduling of sessions, which was sometimes a very fluid process. After each session, the coordinators were responsible for distributing the reflection questions.
The Anatomy Academy curriculum was structured to primarily focus on State of California and State of Utah physical education standards, but Mentors guided the Student participants to employ a variety of skills from multiple content areas.39,40 For instance, Students used math skills to convert grams of sugar to tablespoons in certain foods during the example lesson on the upper gastrointestinal System (Figure 1).
Assessments
To evaluate the outcomes of interest for Anatomy Academy, quantitative self-assessments were collected. First, Mentors completed a preprogram and postprogram self-assessment of their teaching skills as well as a postprogram assessment (Appendix 1). The areas assessed were as follows: content delivery, student engagement, classroom management, and professionalism. Second, a postparticipation survey was completed by all Mentors, which was administered after each instructional session. Responses were collected through Qualtrics. Each Mentor recorded their responses using their Anatomy Academy ID. Mentors were asked the following reflection prompts:
What did you learn about yourself from the experience of working as an Anatomy Academy mentor?
How might this make you a better person (apart from your career goals)? Compare yourself at the end of a given week to the beginning of the week, and at the end of the program compared to the beginning of the program.
How have you changed/developed?
What have you learned through the experience of working with kids?
What will you take with you into your future career?
Please use specific examples where appropriate or necessary.
Third, Students completed content-validated preprogram and postprogram multiple choice science knowledge quiz (Appendix 2); and 5-point Likert-type-style surveys on science interest (Appendix 3) and exercise self-efficacy (Appendix 4). Responses included “strongly disagree,” “disagree,” “neither agree nor disagree,” “agree,” and “strongly agree” that were depicted using commonly used and ubiquitously available smiley Likert-type-scale faces.
Statistical analysis
Preprogram and postprogram Mentor self-reported confidence in teaching abilities was analyzed using a Mann-Whitney test in SPSS (version 20; IBM Corp., Armonk, NY), (Appendix 1). Mentor answers to self-reflection questions were analyzed using grounded theory thematic analysis in 2 steps: a cursory word frequency calculation was performed, which led to thematic categorization. For major identified themes, we subcategorized responses according to Fink’s Taxonomy of Significant Learning. 41
Student performance on their respective preprogram and postprogram assessments was also analyzed using a paired t-test.
Results
Mentors—self-evaluation of teaching abilities
Of the 595 Mentors surveyed, 89% completed both the preprogram and postprogram self-evaluation rating on content delivery, student engagement, classroom management, and level of professionalism.
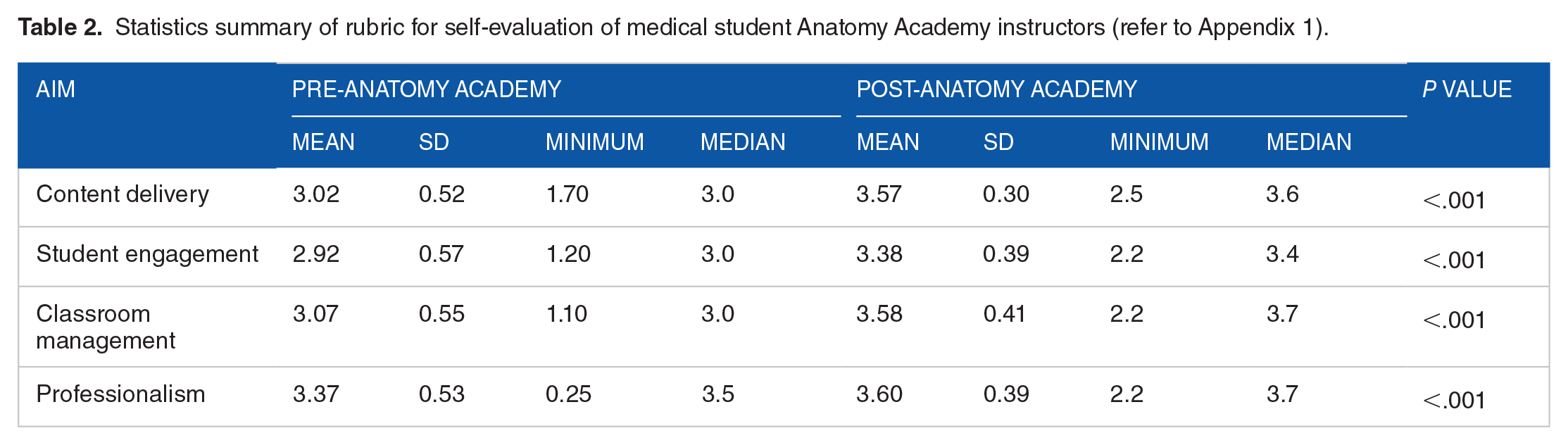
More than half of the Mentors self-reported improvement on all 4 aspects of teaching. Specifically, Mentors reported a subjective improvement in all Aims of content delivery (P < .001), student engagement (P < .001), classroom management (P < .001), and professionalism (P < .001; Table 2).
Statistics summary of rubric for self-evaluation of medical student Anatomy Academy instructors (refer to Appendix 1).
Mentors—post-Anatomy Academy reflections
We analyzed reflection responses from Mentors who also completed the self-evaluation of their teaching. A cursory word frequency analysis of all the responses revealed 3 major themes that Mentors learned from their experience in Anatomy Academy: Experience, Application, and Love. In addition, 7 subthemes were identified to help categorize the personal growth demonstrated through the service-learning opportunity (Fink’s Significant Learning taxonomy domains are listed in parentheses): (1) realization of an ability to make a difference in the world now (human dimension and caring); (2) acknowledgment of the importance of listening in teaching (learning how to learn); (3) recognition that lives can and will change with “a little love” (human dimension and caring); (4) insight to the effectiveness of guiding Students through material rather than lecturing (foundational knowledge, application, integration, and learning how to learn); (5) awareness of the value of respect in the learning environment (human dimension, caring, learning how to learn); (6) cognizance of the power of individualized attention to motivate Students (human dimension, caring, and learning how to learn); and (7) reflection of one’s own personal growth through the open influence of Students (foundational knowledge, application, integration, human dimension, caring, and learning how to learn). We present representative excerpts from Mentor reflections for each question asked. Children’s names in the quotes have been changed to pseudonyms. Quotes were selected that encompassed as many of the 6 Fink’s Significant Learning taxonomy domains as possible. After each quote, the Fink’s Significant Learning taxonomy domains specific to the quote are listed in parentheses.
What did you learn about yourself from the experience of working as an Anatomy Academy mentor?
“As I look back retrospectively on my participation in Anatomy Academy, I realize that I have gained more from this experience than I had expected. I went into it with the goal of teaching fifth graders about anatomy, hopefully instilling in them an interest in science. I came out of it with the realization that I had also learned from these kids—it wasn’t just about teaching them about the trachea or the intestinal tract, but it was also about being a role model and mentor figure in their young lives . . . The role of an Anatomy Academy Mentor is not just to teach the facts of physiological science, but also includes providing emotional and mental support to help a child in his or her developing years. As an Anatomy Academy mentor, I have learned that it really is up you to make the most out of a volunteer experience. Knowing that the time I gave had impacted at least one child’s life in a positive way makes all the work and effort worthwhile.” (Foundational Knowledge, Application, Integration, Human Dimension, Caring, Learning How to Learn)
How might this make you a better person (apart from your career goals)? Compare yourself at the end of a given week to the beginning of the week, and at the end of the program compared to the beginning of the program
“This experience has made me into a better person because I am now more aware of how fortunate I am of being able to receive a quality education. It has made me feel that I have to give back to my community and help the children of underserved communities not only because they deserve it, but also because our future resides within them.” (Human Dimension, Caring) “Working as a mentor taught me the trials and tribulations that an educator faces on a daily basis. There were times when I thought I had the lesson plan well thought out, had all my material in order, and was ready to go only to find out about a change of plans. Teaching itself is a very dynamic process, and I learned that I could be a pretty flexible and resourceful individual. I had to adjust my plans at times to ensure that the students had a sound understanding of the material . . . Anatomy Academy taught me about patience, compassion, and empathy. In the beginning, I felt like an educator to the students. I was the teacher, and they were the students. Toward the end of the Academy, the mentor-mentee relationship was more established. It was less so much me just lecturing them, but I was able to relate to them and have them share with me their stories, what they thought about school and their goals for the future. I became a supporter in their futures and wanted to impart my experiences and anything I wished I had known at their age to them.” (Foundational Knowledge, Application, Integration, Human Dimension, Caring, Learning How to Learn)
How have you changed/developed?
“After Anatomy Academy, my whole perspective on children changed. I was more or less indifferent to kids before the week started. Sure they’re cute or whatever, but what can they actually do? Little I thought. But after watching these fifth graders learn health and science with enthusiasm, I couldn’t help but see an efficacious future in every single one. They all have the potential to learn and do great things, and no bit of resource or encouragement should be withheld.” (Human Dimension, Caring) “Being an Anatomy Academy mentor, I have gained a lot both personally and professionally from the experience. One of the biggest lessons I’ve learned from this was the importance of effective communication—a skill that is absolutely essential for success in almost every aspect of life. In order to teach physiology concepts to 5th grade students, I was often forced to step outside the box and come up with creative ways to not only help them understand, but in an effort to help them remember them.” (Foundational Knowledge, Application, Integration, Learning How to Learn)
What have you learned through the experience of working with kids?
“The day after we did the lesson about sugar, ‘Brian’ and ‘Catie’ both brought water instead of Gatorade. After we talked about nutrition facts and nutrition labels everyone got a break. During the break, they were given fruit snacks and juice. Because the Mentors were given these as well, I was about to go straight to opening mine and eating them, but then I looked up. Literally every single kid in the Silver Panthers [the group name of this particular team of Mentors and 5th grade students] was turning their juice boxes over and reading the nutrition labels. Not one of them opened their packets right away. I was so incredibly impressed. I knew then I had to be careful. I had to remember to practice what I teach, and to never underestimate the potential of these children.” (Foundational Knowledge, Application, Integration, Human Dimension, Caring, Learning How to Learn) “Working with these kids really opened my eyes to the ability they have to learn. However, in order to keep that attention on learning it must be mixed with activities that are both fun but challenging. I was amazed at the profound questions they asked. ‘Eddie’ asked at one point, ‘Why can I hear my own voice in my head when I am not talking, but thinking a sentence?’ Many times I could answer similar questions but for a question such as this, it required the help of a faculty member or Coordinator. Having them there was an invaluable asset. Through this experience I realized that the children can view things in much different context, or viewpoints, even more profoundly than I could.” (Foundational Knowledge, Application, Integration, Human Dimension, Caring, Learning How to Learn)
What will you take with you into your future career?
“It was important to keep things fun and interesting for them, but also follow the structure of the lesson plan. I found that as I connected the lesson to each one individually and asked them each direct questions that it would hold their attention. At one point ‘Doug’ was very distracted from either playing outside, having just eaten lunch, or a combination of the two. He did not want to listen and almost nothing we did could bring him to participate with the group. The next day I resolved to do better. My fellow Mentor and I stumbled upon his love for soccer and especially a player named Christiano Ronaldo. We connected it to the lesson throughout the day always bringing back soccer or Ronaldo to what we were asking him about or teaching. He responded much more readily and remained focused as we moved on and focused on other students. It was really amazing how it helped. I think that this is a principle that can be applied to more age groups than just 5th graders.” (Human Dimension, Caring) “I aspire to become a pediatrician and thinking about my role as a physician to children, I realize that not only will their health be in my hands, but also I will be a role model and facilitator in their lives. I will be a part of the support system in their lives.” (Human Dimension, Caring, Learning How to Learn)
Students
Of the 1259 Students surveyed across all participating school sites, 88% responded to both preprogram and postprogram surveys of science knowledge, science interest, and exercise self-efficacy. Significant improvement in science knowledge (P = .014), and in self-reported exercise self-efficacy (P = .038), but not science interest (P = .371) was found.
Discussion
Mentors
Through the planning and implementation of Anatomy Academy, we aimed to provide Mentors with opportunities to learn and develop basic teaching skills that could be applied in their future roles as teachers in the medical setting. The results of the program evaluation indicate that Mentors recognized improvement in their own basic teaching skills, including delivering content, engaging Students, managing a classroom, and demonstrating professionalism. Furthermore, the 7 major themes identified show that exposure to a service-learning program like Anatomy Academy can inform student’s perspectives on personal growth and the ability to impact the world through small acts like listening, respect, and attention.
Anatomy Academy Mentors learn how to communicate complex medical information to a level appropriate for elementary school children, prepare and deliver lessons on anatomy, physiology, and nutrition that help children understand the importance of establishing and maintaining a healthy lifestyle, teach groups of children in didactic and active learning environments, serve as role models for pursuing higher education, demonstrate the utmost professional demeanor, and become exposed to an experiential learning environment that results in immediate change in Students’ self-efficacy. Thus, Mentors are exposed to at least 1 aspect of all 6 core Accreditation Council for Graduate Medical Education (ACGME) competencies, respectively, in one volunteer setting: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, systems-based practice. 42
With an increasing focus on the physician as a teacher to other physicians-in-training and to patients, it is essential to provide preprofessional and professional students with teaching opportunities early in the course of their education. To accomplish this, we developed and implemented a program to teach students the fundamentals of teaching in the preprofessional and professional years of higher education. Teaching these students to become effective teachers themselves has implications for both medical education and patient care, as medical professionals will be more adept at teaching one another as well as teaching their patients.
Students
We have received overwhelming, informal, positive feedback from elementary and middle-school Students, their parents, and teachers. In one anecdotal story received from a Mentor, a Student expressed immediate shock and distaste for a popular drink he consumed daily, after participating in the upper gastrointestinal system lesson on sugar content. From that moment on, he vowed never to drink that product again. In another story from a parent, she caught her child measuring portions of healthy food for his lunch box in accordance with the lesson on lower gastrointestinal system, in which the children learn the importance of eating a balanced diet. Our Mentors and Coordinators receive stories like these consistently each semester.
Limitations and lessons learned
Given the impact the program has on elementary and middle-school children, we were surprised to discover that science interest was not improving as a result of the program, even though science knowledge and exercise self-efficacy improved greatly. In our evaluation of the program, we realized that we are not training Mentors to explicitly identify as “scientists.” Indeed, many Students expressed that they feel like they are just having fun during Anatomy Academy and are not really in school (which is a testament to the effectiveness of the engaged-learning model). The same can be said for how Students relate to their Mentors. We need to address this in future trainings. However, as an example, one Student did express interest in becoming an engineer because his Mentor shared his career goal of becoming an engineer. Explicitly educating Students through active and engaging programs will continue to promote and advance all STEM disciplines in their young minds. 43
From 2012 to 2014, Anatomy Academy experienced rapid growth from 2 initial schools to a total of 12 schools. The importance of a community partnership between elementary schools and preprofessional and professional schools cannot be overstated. One of our salient observations that need formalized experimental analysis was the immediate impact Anatomy Academy had on Students attending underserved schools in diverse communities. Although the learning experience was also rich at socioeconomically advantaged schools, Mentors at underserved schools expressed elation at the thirst for knowledge that Students expressed. Students and their teachers looked forward to the day when Anatomy Academy Mentors would visit, and likewise were saddened at the conclusion of the 6 to 7-week program. The model of infusing volunteer human resources into schools with limited access to learning resources in general was very well-received by school administrators, teachers, and students alike.
Although all 6 of Fink’s Significant Learning taxonomy domains were experienced by Mentors and Students during the course of Anatomy Academy, the 7 major themes emanating from our grounded theory analysis revealed that human dimension, caring, and learning how to learn were domains in which Mentors received the most epiphanies. These results indicate that service learning helps preprofessional and preclinical students learn, understand, and apply important intangible lessons that might be difficult to acquire in a typical brick-and-mortar classroom lecture. Service learning helps solidify the importance of gaining and understanding knowledge in the context of learning as a philosophy.
Conclusions
The benefits of Anatomy Academy have been multifaceted. Elementary age students can learn through engaged-learning pedagogies and enjoy the material while doing so. The importance of improving professional, communication, and teaching skills in medical professionals is readily apparent, and Anatomy Academy is one of the emerging paradigms to accomplish that. Finally, perhaps the greatest impact of a service-learning program is the educational experience paradigm shift and personal growth that takes place through exposure to demanding and novel teaching and learning situations.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Appendix 4
Acknowledgements
The authors acknowledge the following funding sources for Anatomy Academy: The Albert Schweitzer Fellowship; Monica Salinas Fellowship; Brigham Young University, Mentored Research Environment Grants (College of Nursing, and David O. McKay College of Education); Brigham Young University, David O. McKay Scholarly and Creative Works Grant; and Utah Valley University, Engaged Learning Grant. The authors thank all of our school partner sites, but especially Stella Middle Charter Academy (Los Angeles, CA) and Principal Elysa Vargas for being the first to support the vision of Anatomy Academy. They also thank our inaugural mentors, Anisha Banda, Alex Chang, Heajung Lee, Monica Martinez, Elizabeth Shue, Kevin Steed, and Christine Thang. From them, hundreds of mentors have followed in their footsteps, and thousands of children have started on the path toward a healthy lifestyle.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MMD – Anatomy Academy Co-Founder, experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
KO – Anatomy Academy Co-Founder, experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
JP – Anatomy Academy Co-Founder, experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
KS– Anatomy Academy Associate Director, experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
NS – Experimental design, IRB, data acquisition, data analysis, manuscript writing, manuscript editing
AT – Data acquisition, data analysis, manuscript writing, manuscript editing
AM – Data acquisition, data analysis, manuscript writing, manuscript editing
JMC – Data acquisition, data analysis, manuscript writing, manuscript editing
EW – Data acquisition, data analysis, manuscript writing, manuscript editing
MES – Experimental design, IRB, data acquisition, data analysis, manuscript writing, manuscript editing
DAM – Experimental design, IRB, data acquisition, data analysis, manuscript writing, manuscript editing
GS – Experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
GR – Experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
JL – Experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
HAWA – Experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing
JJW – Anatomy Academy Co-Founder, Anatomy Academy Director, experimental design, IRB, grant writing, data acquisition, data analysis, manuscript writing, manuscript editing