
Abstract
Objective:
Diabetes is prevalent among hospitalized patients and there are multiple challenges to attaining glycemic control in the hospital setting. We sought to develop an inpatient glycemic management curriculum with stakeholder input and to evaluate the effectiveness of this educational program on glycemic control in hospitalized patients.
Methods:
Using the Six-Step Approach of Kern to Curriculum Development for Medical Education, we developed and implemented an educational curriculum for inpatient glycemic management targeted to internal medicine residents and hospitalists. We surveyed physicians (n = 73) and conducted focus group sessions (n = 18 physicians) to solicit input regarding educational deficits and desired format of the educational intervention. Based on feedback from the surveys and focus groups, we developed educational goals and objectives and a case-based curriculum, which was delivered over a 1-year period via in-person teaching sessions by 2 experienced diabetes physicians at 3 hospitals. Rates of hypoglycemia and hyperglycemia were evaluated among at-risk patient days using an interrupted time-series design.
Results:
We developed a mnemonic-based (SIGNAL) curriculum consisting of 10 modules, which covers key concepts of inpatient glycemic management and provides an approach to daily glycemic management: S = steroids, I = insulin, G = glucose, N = nutritional status, A = added dextrose, and L = labs. Following implementation of the curriculum, there was no difference in the rates of hyperglycemia in insulin-treated patients following the intervention; however, there was an increase in the rates of hypoglycemia defined as blood glucose (BG) ⩽ 70 mg/dL (5.6% vs 3.0%, P < .001) and clinically significant hypoglycemia defined as BG < 54 mg/dL (1.9% vs 0.8%, P = .01). There was poor penetration of the curriculum, with 60%, 20%, and 90% of the learning modules being delivered at the three participating hospitals, respectively.
Conclusions:
In this pilot study, a physician-targeted educational curriculum was not associated with improved glycemic control. Adapting the intervention to increase penetration and integrating the curriculum into existing clinical decision support tools may improve the effectiveness of the educational program on glycemic outcomes.
Introduction
Hyperglycemia requiring treatment with glucose-lowering medications is highly prevalent among hospitalized patients, affecting 20% to 40% of all inpatients. 1 Although diabetes is most often not their primary reason for admission, inpatient glucose control is important, as both hyperglycemia and hypoglycemia have been associated with worse clinical outcomes, including increased complications, length of stay, cost, and mortality.2-6 Hospital-based clinicians face many barriers to safely and effectively controlling blood glucose (BG) in their patients. Some of these barriers relate to patient factors that can affect glucose homeostasis, such as acute illness, change in renal or liver function, use of glucocorticoids, intravenous medications containing dextrose, and change in nutritional status (eg, nil per os [NPO]). Systems factors may also pose challenges for providers. Electronic medical record (EMR) systems vary in their ease of use, visual display of relevant clinical information (eg, glucose and insulin trends), and degrees of clinical decision support (eg, insulin order sets or insulin dosing algorithms). Moreover, hospital clinicians in various specialties may have differing degrees of training in or attitudes related to inpatient glucose management.7-10
Educational interventions have been developed and directed toward hospital-based physicians, advanced practitioners, and nurses to increase their knowledge of inpatient glucose management. Educational formats that have been developed in this area include lectures, written guidelines or algorithms, clinical decision support tools, workshops, computer-based modules, online interactive tutorials, case-based ward rounds, refresher courses, and interactive assessments. 11 Most of these studies have demonstrated effectiveness in increasing provider knowledge of inpatient glucose management and improving process measures (eg, adherence to clinical practice guidelines regarding the use of basal-bolus insulin therapy) 4 ; on the other hand, results have been mixed regarding the effectiveness of educational interventions on glycemic outcomes. 11
Components of educational interventions that have produced the most favorable clinical outcomes (beyond provider knowledge alone) include (1) greater hands-on experience within the target clinical context (eg, application of knowledge during supervised clinical rounds), 12 (2) provision of relevant clinical information at the point of care (eg, pocketcards with algorithms/guidelines), 13 (3) “active, participatory and situated learning” rather than passive acquisition of information, 11 (4) integration of educational content with electronic clinical decision support tools (eg, order sets),14,15 and (5) inclusion of continuing medical education in inpatient glycemic management as part of hospital quality planning. 11 A deficiency that has been noted in previous educational interventions is restricting the education to internal medicine physicians or residents in training only because inpatient glycemic management reaches a much broader group of clinicians in the hospital (eg, surgery, advanced practice clinicians).
At our institution, we developed a diabetes nursing “superuser” program, an educational intervention employing a scalable “train-the-trainer” approach led by experienced diabetes nurse practitioners to disseminate our hospital’s policies and protocols in inpatient glucose management.16,17 This educational intervention was one component of a centralized inpatient glucose management program, which achieved a significant and sustained (~20%) reduction in the incidence of inpatient hypoglycemia over a 3-year time period; however, rates of severe hyperglycemia were not significantly reduced. 16 We postulated that the differential impact of this intervention on hypoglycemia and hyperglycemia rates related to the fact that the hypoglycemia policy in our hospital is nurse driven, whereas hyperglycemia management is under the control of prescribers (eg, residents and hospitalists). As diabetes is often not the primary reason for hospitalization, providers likely experience situational unawareness 18 when managing inpatient glucose amid multiple other clinical conditions that may be deemed higher priority.
Recognizing that both knowledge deficits and situational unawareness likely contribute to prescriber therapeutic inertia, we sought to develop an educational curriculum that would provide not only clinical information (“what”) but also a systematic approach (“how”) to inpatient glucose management. In developing our curriculum, we drew from the high-reliability aviation industry, which employs “normal checklists” as part of every flight. 19 We sought to develop a mnemonic-based checklist that providers could use on a daily basis to minimize oversight of clinically important elements when making dosing decisions for inpatient glucose medications. A checklist-based intervention had been deployed in our intensive care units and was shown to significantly reduce the rates of catheter-related bloodstream infections. 20 We hypothesized that the delivery of clinical information structured around a mnemonic-based checklist would reduce rates of hypoglycemia and hyperglycemia. The proposed intervention was informed by previous successful interventions in inpatient glycemic management.
Methods
We sought to develop an inpatient glycemic management curriculum with stakeholder input and to evaluate the effectiveness of this educational program on glycemic control in hospitalized patients. This was a prospective observational study conducted at 2 academic medical centers (Johns Hopkins Hospital [JHH] and Johns Hopkins Bayview Medical Center [JHBMC]) and 1 community hospital (Howard County General Hospital [HCGH]) within the Johns Hopkins Health System. The study was approved by the Johns Hopkins Institutional Review Board. We used the Six-Step Approach of Kern to the development, implementation, and evaluation of our diabetes prescriber curriculum (Table 1). 21
Methods and key results based on the Six-Step Approach of Kern to curriculum development.

Abbreviations: CME, continuing medical education; EMR, electronic medical record.
Figures represent the number of times these themes were raised during focus groups.
Step 1: problem identification and general needs assessment and Step 2: targeted needs assessment and stakeholder engagement process
An overview of the general need for new approaches to delivering education relevant to inpatient glucose management has been summarized in our introduction. To identify local gaps in inpatient glucose management education, we administered a gap analysis survey to diabetes champions to each of the adult hospitals in our health system. 22 The diabetes champions were designated clinicians (physicians or nurses) who oversaw diabetes management and education at each hospital. This survey was developed with a broad representation of key stakeholders at each of our hospitals, assembled through the Diabetes Clinical Community of the Armstrong Institute for Patient Safety and Quality.22,23 A section of this survey was focused on professional education in inpatient glucose management, and respondents were asked to report whether education on individual topics at their hospital was mandatory, optional, or not offered. Results of the gap analysis tool were synthesized to identify the most prevalent gaps in inpatient glucose management education.
We developed a needs assessment survey for internal medicine residents and hospitalists. We asked participants to focus on the material content and to articulate effective presentation formats to enhance usability and tailor the materials and superuser training sessions to their local clinical context.
Following the needs assessment survey, we conducted 6 focus group sessions of 40- to 60-minute duration with clinician stakeholders: 4 residents and 1 hospitalist at JHH; 7 residents and 2 hospitalists at JHBMC; and 4 hospitalists at HCGH. Written informed consent was obtained from physician participants in focus group sessions, which were moderated by a senior project coordinator with extensive qualitative research experience with assistance from 2 investigators (S.H.G., N.M.). Sessions were taped and transcribed using the Ubiqus Reporting, Inc transcription service (New York, NY). We used the SAGE Publications Focus Group Kit and NVivo qualitative data analysis software (QSR International Pty Ltd, Version 10, 2012), 24 which our team has used for focus groups in other research studies. We used a grounded theory approach and identified emerging themes by reviewing the transcripts from the focus groups. The identification and verification process, marrying coding of data with the development of theoretical ideas, proceeded iteratively, until the analysis reached theoretical saturation. 25
Step 3: goals and objectives
Based on feedback from surveys and focus group sessions, 2 diabetes physicians developed overarching educational goals and objectives that encompassed the key elements of inpatient glycemic management, incorporating the topics identified as deficiencies for learners.
Step 4: educational strategies
Based on feedback from our physicians and literature showing that the incorporation of case-based education sessions into a hospital-wide glucose management program improved glycemic outcomes,13,26,27 we anticipated using case-based studies to achieve our learning objectives. In addition to clinical content, physicians indicated that they would value a decision-making approach to glucose management that could be employed on a daily basis for hospitalized patients. Accordingly, we sought to develop a mnemonic that would serve as a clinical decision aid or checklist at the point of care.
Step 5: implementation
We initially proposed to use a superuser educational approach for our clinicians, as this strategy had worked effectively for educating our nurses16,17; however, we intended to revise the method based on feedback from the surveys and the focus group sessions. To disseminate the curriculum, we developed posters and pocketcards with the curriculum mnemonic, which were placed in physician workrooms, and promoted the curriculum whenever delivering the content to end users (ie, during scheduled educational activities).
Two board-certified endocrinologists (S.H.G., N.M.) with expertise in hospital management of diabetes served as the primary trainers for the physician superusers. Initially, we proposed to hold quarterly case-based prescriber superuser workshops on relevant glucose management topics; however, based on feedback from the focus group sessions (Step 2), hospital physicians suggested more frequent sessions of shorter duration (eg, 1 hour or less), preferably incorporated into existing educational activities due to time constraints and competing clinical obligations. Thus, we adapted our approach and packaged the case studies into 15-minute “chalk talk-in-a box” sessions, which senior residents could deliver in brief teaching sessions during rounds. The set of topics and format satisfied several required core competencies of the American Board of Medical Specialties: medical knowledge, patient care, practice-based learning, and systems-based learning. We used a similar format for the hospitalist superuser training sessions and offered continuing medical education credit for the workshops.
Step 6: evaluation and feedback
We used an interrupted time-series design to evaluate the effectiveness of this educational intervention among adult, non-obstetrical patients with type 1 diabetes, type 2 diabetes, or acute hyperglycemia (in the absence of known diabetes). During the period of this study, there was a transition of the inpatient EMR system from Sunrise POE to EpicCare at JHH, whereas both JHBMC and HCGH hospitals had a consistent EMR (EpicCare) over the duration of the study.
Patient admissions were identified using International Classification of Diseases (ICD)-9 and ICD-10 codes from both EMR systems, depending on the date of admission: 250.01/E10.9 (type 1 diabetes controlled); 250.03/E10.65 (type 1 diabetes uncontrolled); 250.00/E11.9 (type 2 diabetes controlled); 250.02/E11.65 (type 2 diabetes uncontrolled); 790.21/R73.01 (impaired fasting glucose); 790.22/R73.02 (impaired glucose tolerance); 790.29/R73.09 (hyperglycemia); and V58.67/79.4 (insulin use without ICD-9 for ICD-10 diabetes code). We excluded patient admissions with the following diagnoses: 250.1x/E11.69 (diabetic ketoacidosis), 250.2x/E11.0x (hyperosmolar coma), and 250.3x/E11.641 (diabetes with other coma). Patient days were defined as calendar days from the date of admission.
The primary glycemic outcome measures are summarized below as recommended by the American Diabetes Association (ADA) 28 :
Hypoglycemia. Percentage of patient days with at least 1 hypoglycemic event during admission (moderate: ⩽70 mg/dL; clinically significant: <54 mg/dL; and severe: ⩽40 mg/dL) 29 ;
Hyperglycemia. Percentage of patient days with patient-day weighted mean BG in hyperglycemic range (glucose ⩾ 180 mg/dL). 16
Patient-day glycemic outcomes were evaluated as the numerator in 2 denominator populations: (1) insulin-treated patients and (2) patients with a diagnosis of diabetes mellitus. Insulin-treated patient days were defined as patients with or without diabetes who received at least 1 unit of any type of subcutaneous insulin on that calendar day. Diabetes patient days were defined as patient days with a diabetes diagnosis and at least 1 serum or fingerstick glucose measurement.
The implementation and evaluation period consisted of 3 phases: Phase 1 (–3 to 0 months; January 4, 2016 to June 30, 2016) was used to establish baseline glycemic outcomes; Phase 2 (0 to 12 months; July 1, 2016 to June 30, 2017) consisted of implementation and teaching of the curriculum; and Phase 3 (13 to 15 months; July 7, 2017 to September 30, 2017) was used to evaluate post-intervention glycemic outcomes. We chose to assess glycemic outcomes over 3 months post-intervention because (1) we previously found that hypoglycemia levels declined over 3 months following our nursing superuser education on this topic16,17 and (2) our power calculations indicated that this timeframe would provide adequate patient days (>90% power) based on the number of admissions (n = 500) to observe significant (20%) differences in rates of glycemic measures pre-intervention and post-intervention. Laboratory and medication data were extracted from the relevant EMRs (POE or EpicCare) by 2 experienced teams of software engineers. For the JHBMC and HCGH hospitals, all data were extracted from EpicCare.
Descriptive statistics were used to tabulate the results from the focus group sessions and surveys. For evaluation of the glycemic outcomes, chi-square analysis was used to compare rates of hypoglycemic and hyperglycemic outcomes during Phase 1 and Phase 3 time periods. A 2-sided P-value of <.05 was considered statistically significant. All statistical analyses were performed using Stata Statistical Software: Release 15 (StataCorp LLC, College Station, TX).
Results
Table 1 summarizes the key findings at each step of the curriculum development approach of Kern.
Step 1: problem identification and Step 2: targeted needs assessment
Our gap analysis revealed a lack of standardized training of health care professionals in inpatient diabetes management within our health system. 22 Although inpatient diabetes education was generally considered a priority in nursing staff education, physicians received less frequent and variable degrees of education in this area. Not surprisingly, educational initiatives on the topic differed among academic vs community hospitals, with less exposure to formal inpatient glucose management education at the latter.
Clinician surveys
We attended 2 internal medicine resident academic meetings and 3 hospitalist faculty meetings, during which 73 physicians completed the needs assessment survey. Generally, the respondents found the existing prescriber decision support tools for inpatient glucose management very useful, but they identified the need for additional information in the following areas: (1) management of hypoglycemia and its risk factors, (2) management of pre-mixed (ie, 70/30) insulins, (3) management of insulin pumps, (4) correction of severe hyperglycemia, and (5) transitioning to home regimen at hospital discharge. Respondents also identified several ambiguous terms in the existing algorithms and requested more precise definitions for (1) elderly person, (2) liver disease, and (3) kidney disease, all of which are risk factors for hypoglycemia. Respondents requested that the existing decision support tools add the following topics: (1) management of NPO status, (2) preoperative management, (3) new oral antidiabetic agents and outpatient management tips, (4) glucose management in end-stage renal disease, (5) management of steroid-induced hyperglycemia, (5) management in gastroparesis, and (6) guidance for ordering hemoglobin A1C in the hospital.
With respect to the desired format of diabetes decision support tools, respondents ranked the following formats from most to least desired: mobile phone app with electronic PDF (54.8%), no change to existing printed booklet (42.5%), link in EMR and insulin order set (34.2%), and web-based eLearning (12.3%).
With respect to the desired format of a case-based curriculum, the following formats were ranked from most to least desired as follows: web-based cases (38.3%), simulation-based cases (36.9%), in-person discussion (17.8%), print case study booklet (13.6%), and pre-recorded webinar/video (9.6%).
The internal medicine residents requested that more inpatient glucose lectures be incorporated into their existing academic conference time and that formal training be provided during their residency orientation. Residents of JHH currently use a digital handbook as a reference and they requested that the inpatient diabetes clinical decision support aids be incorporated into this resource. The residents also requested that the proposed curriculum be made available on the health system’s electronic learning (eLearning) platform and that protected time be built into their residency program so that they could complete this at early stages in their training.
Focus group sessions
Many of the themes that emerged in these focus group sessions aligned with the summary feedback from the needs survey responses and are summarized in Table 1. Focus groups included 5 to 6 participants.
Step 3: goals and objectives
Our goals and learning objectives were rooted in the “basal-nutritional-correctional” insulin concept, which reflects evidence-based, physiologic insulin delivery 30 for hospitalized patients. Applying this concept to challenging hospital-based patient scenarios (ie, tube feedings, steroids, insulin pumps, etc) was incorporated into our learning objectives. A separate learning objective was developed for hyperglycemic emergencies given the complex physiology and management for these patients compared with general medical or surgical ward patients. Finally, although we do not expect hospital-based clinicians to have expertise in insulin pump management, we thought it important that they have a basic familiarity of insulin pumps for patient safety.
Step 4: educational strategies
Based on our stakeholder input, we updated and finalized our curriculum objectives and decided to maintain the existing pocket cards (which were universally desired) as part of our educational toolkit. To accommodate the concerns about extra time commitments outside of structured educational and meeting times, we worked in collaboration with the Residency Program Director at JHH and JHBMC and the Director of the Hospitalist Program at HCGH to incorporate the inpatient diabetes superuser educational curriculum into existing educational forums to reach a broader audience and achieve deeper penetration of the diabetes curriculum to the entire physician group. The sessions were designed as shorter, more frequent 1-hour sessions rather than the 2-hour superuser sessions that were originally proposed.
In addition to clinical content, we developed a mnemonic (SIGNAL), designed to serve as a checklist for clinicians in making day-to-day decisions in inpatient glucose management for hospitalized patients. The components of the mnemonic are summarized in Table 2. This mnemonic and the educational curriculum based on which it was built were centered around an aviation theme, emphasizing the shared importance of checklists in the 2 high-risk industries of health care and aviation. The SIGNAL approach is introduced at the start of each learning module and is directly applied in each case to reinforce this systematic approach to glucose management through repetition.
“SIGNAL” mnemonic.

Step 5: implementation
In collaboration with an educational strategy and design organization, Bottom Line Performance, Inc, we developed an electronic toolkit, in the form of an e-magazine that includes all of the prescriber diabetes educational materials that are now hosted on our internal server (http://signal.jhmi.edu) (Figure 1A). The SIGNAL curriculum consists of 10 learning modules (Table 3).

(A) SIGNAL eToolkit main page and (B) SIGNAL case studies.
“SIGNAL” curriculum modules.

Each course consists of a facilitator guide, PowerPoint presentation, participant worksheet, pocketcards, teaching cards (eg, insulin types, drug names, diabetes supplies), case study descriptions (Figure 1B), and case study mock EMR data. One module was completed per 1-hour session. To encourage spontaneous case-based teaching by residents, a filter was created allowing cases to be identified based on keyword search (eg, steroids, hypoglycemia). Case studies and answers were used during the teaching sessions and were available following each in-person session.
During the intervention period, 6, 2, and 9 of the 10 SIGNAL learning modules were delivered in-person at JHH, JHBMC, and HCGH, respectively. Our goal was to deliver 9 of 10 modules over the 1-year intervention period, which was only achieved at 1 site. At JHH and JHBMC, the learners included third year medical students and post-graduate year (PGY) 1-3 internal medicine residents (approximately n = 70 and n = 30, respectively). We were unable to deliver all of the modules at these 2 housestaff sites, despite enthusiasm from both residency program directors, due to other Accreditation Council for Graduate Medical Education (ACGME) curriculum requirements. At HCGH, learners were internal medicine hospitalists and approximately 8 to 10 individuals attended each session. We were unable to track the number of modules received by individual providers due to their rotating schedules over the course of the year and it is unlikely that any of our providers received all of the modules.
Step 6: evaluation
Figure 2A and B shows the pre-intervention and post-intervention glycemic outcomes data for insulin-treated and diabetes patient days, respectively. The pre-intervention period (Phase 1) included 1511 insulin-treated patient days of 720 patient admissions and 2159 diabetes patient days of 736 patient admissions. The post-intervention period (Phase 3) included 1564 insulin-treated patient days of 819 patient admissions and 2377 diabetes patient days of 884 patient admissions. Among insulin-treated patient days, there was no difference in the rate of hyperglycemia following the intervention; however, there was an increase in the rates of hypoglycemia defined as BG ⩽ 70 mg/dL (5.6% vs 3.0%, P < .001) and clinically significant hypoglycemia defined as BG < 54 mg/dL (1.9% vs 0.8%, P = .01). There was no difference in the rate of severe hypoglycemia (⩽40 mg/dL). A similar pattern was observed among diabetes patient days, with no notable difference in rates of hyperglycemia following the intervention, and an increase in rates of BG ⩽ 70 mg/dL (4.7% vs 2.9%, P < .01).
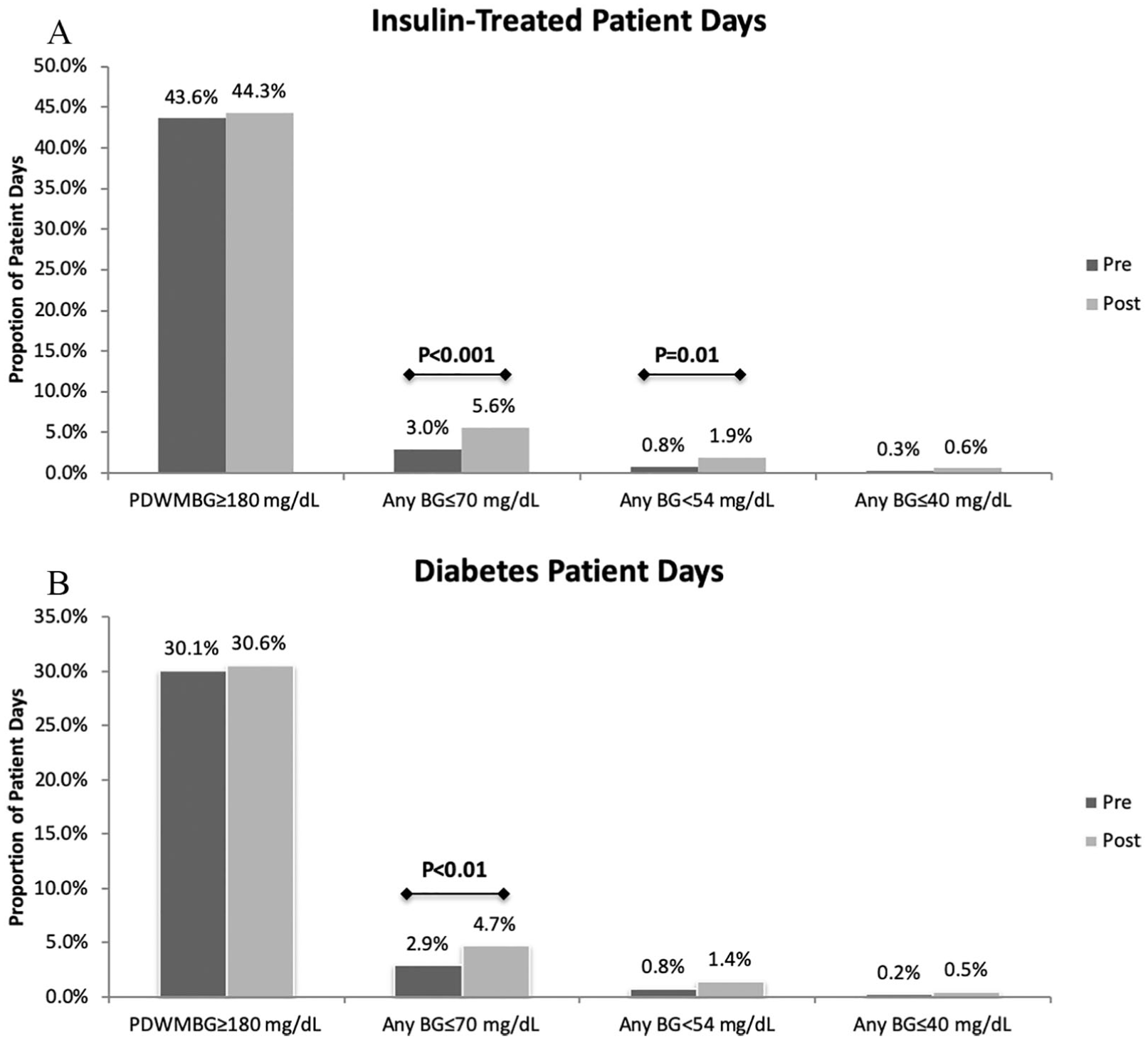
Glycemic outcomes among insulin-treated patient days (A) and diabetes patient days (B). Statistically significant differences are indicated with P-values. BG indicates blood glucose; PDWMBG, patient-day weighted mean blood glucose.
It is important to note that, during the study period, there was a substantial change in the inpatient glucose management order sets and decision support tool at JHH, the largest hospital in our health system and in this study. During the transition to our new EMR, a best practice advisory alert that advises providers to consider reducing insulin doses when a patient’s nutritional status changes to NPO was inadvertently eliminated. There were otherwise no major systems changes that occurred during the study period. Notably, our inpatient diabetes management service structure and processes remained consistent throughout the intervention and evaluation period. The clinicians on the patient diabetes management services were not informed of the results of this study while it was still ongoing, as this could have influenced practice change and confounded the results.
Discussion
In this pilot study, we engaged stakeholders to develop an inpatient glycemic management curriculum for physicians. Following implementation of the case-based mnemonic curriculum, there was no effect on the rates of hyperglycemia among hospitalized patients treated with insulin therapy or patients with diabetes; however, there was a small but statistically significant increase in the rates of hypoglycemia in the post-intervention period compared with baseline. We suspect that the lack of effectiveness of our educational intervention on glycemic outcomes may be attributable to poor penetration of the intervention and that the increased rates of hypoglycemia were related to loss of a critical clinical decision support tool (insulin NPO alert) during the study period, rather than the intervention itself.
Educational interventions related to inpatient glycemic management have shown mixed but generally favorable results on clinical outcomes. In a recent review of 16 educational programs in this area, 14 studies reported at least 1 clinical process or outcome measure, whereas 7 reported glycemic outcomes. 11 Among the 7 studies reporting glycemic outcomes, 3 showed reductions in rates of hyperglycemia with a concomitant increase in rates of hypoglycemia,12,31,32 3 showed a reduction in rates of hyperglycemia with no change in rates of hypoglycemia,13,33,34 and 1 study showed no effect on either hyperglycemia or hypoglycemia. 14 The educational formats in these studies included daily endocrine rounds with endocrine faculty, lectures/workshops, personal digital assistant (PDA), print algorithms, interactive discussions applying practice recommendations, games, case-based diabetes ward rounds, and refresher courses. Despite the lack of glycemic outcomes in this study, a previous intervention at our institution focused on nursing education demonstrated reductions in rates of hypoglycemia with no effect on hyperglycemia. 16
Several factors have been identified as features related to successful educational opportunities for clinical practice improvement in inpatient diabetes: (1) “active, situated, and participatory interactions of learners in workplace,” (2) “instruction needs to reach a large population of learners,” (3) “integration with clinical decision support strategies,” and (4) “education should be adopted as a formal component of hospitals’ quality planning.” 11 By creating a simple mnemonic that providers can use to promote recall and application of relevant information at the point of care (ie, when adjusting insulin medications), we believe that our curriculum presents an active and situated learning opportunity; however, we believe that poor penetration of the curriculum hindered opportunities for practice improvement.
Based on stakeholder feedback, we attempted to deliver these case-based learning modules during regularly scheduled academic/administrative conferences; however, at one of our hospitals (JHBMC), only 3 to 5 general internal medicine residents rotate through an ambulatory course at a given time and the duration of these courses is several weeks per group; the lecture series for these courses is already established to fulfill ACGME requirements such that at most any given group of residents would only be able to receive 1 to 2 SIGNAL modules among other general ambulatory topics. Similarly, the attendance at academic conferences at JHH was variable due to call schedules and duty hour rules, thus ensuring that a given resident received all of the SIGNAL modules was impractical. We found it generally easier to deliver the SIGNAL course to hospitalists at a community hospital, as the group was smaller and there was less turnover compared with residents who shift from multiple inpatient or outpatient experiences during their residency program. However, even among hospitalists, the penetration was inadequate to accurately assess glycemic outcomes.
As with all time-series studies, this study could not exclude confounding due to co-interventions or other events that occur during or around the time of the intervention. In fact, we suspect that secular confounding did influence glycemic outcomes: loss of an existing informatics alert to prevent hypoglycemia in NPO patients, which occurred during transition from our previous to current inpatient EMR during the study period, may have resulted in increased rates of hypoglycemia as providers failed to proactively reduce insulin doses in patients who were made NPO. However, there were no other major systems changes related to the delivery of care for hospitalized patients with diabetes during this time period that could have confounded our results. Nonetheless, one approach to addressing confounding in time-series designs is to include a control group, which we will consider for future studies. Alternatively, a per-protocol analysis where patient’s glycemic outcomes are compared based on whether providers completed vs did not complete the SIGNAL program could be used to isolate the impact of the educational intervention.
In light of the lessons learned from this pilot study, we are currently reformatting the curriculum into smaller education sessions that will be available on our eLearning system. With buy-in from the residency program directors, we will advocate that the curriculum be added as a required component of internal medicine residency training and included in our health system’s eLearning platform, allowing tracking of completion by providers to correlate learning to glycemic outcomes. Finally, we are considering translating the SIGNAL mnemonic into a clinical decision support tool embedded in the EMR to facilitate clinical decision making. Considering the high prevalence of diabetes in hospitalized patients and the potential for adverse outcomes related to poor glucose management, developing an educational intervention that translates into improved clinical outcomes is an important quality improvement goal for health systems.
Footnotes
Acknowledgements
The authors wish to acknowledge Drs Lisa A Cooper and Peter J Pronovost for their assistance during the study design planning phase. Consent for publishing the findings of the focus group sessions was secured from focus group participants. IRB approval was obtained to conduct the surveys without informed consent given the anonymized and deidentified reporting of results.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: S.H.G. and N.M. were supported by the National Institute of Diabetes and Digestive and Kidney Diseases through Grant Nos R34DK105460 and 1K3DK111986, respectively.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NM and SHG designed the study, developed the intervention, collected the data, analyzed the data, and wrote the manuscript. HB developed the intervention and contributed to the writing of the manuscript. LB conducted the qualitative components of the study and reviewed the manuscript. BSP, SF, and SS collected the outcomes data and reviewed the manuscript. SL performed the statistical analysis and reviewed the manuscript.