
Abstract
Introduction:
Patient safety (PS) is one of the most important priorities in modern healthcare systems. Unfortunately, PS education is limited in many medical school curricula. Our objective was to implement an innovative curriculum to introduce third-year medical students on their pediatric clerkship to PS concepts and domains, and to provide a safe environment to discuss lapses in PS that they identified while caring for patients.
Methods:
At the start of the pediatric clerkship, students were introduced to the curriculum, instructed to identify a lapse of PS, and to submit a description and analysis of the lapse using the SAFE framework (S = Safety concern, A = Action taken, F = Failure, linked to safety domains, E = Effects on patient outcome). Two sessions, 90-mins each, were conducted every clerkship during which there was a brief didactic presentation, each student presented their case, and the case discussed by students and faculty.
Results:
Over 19 months, 75 students participated. The most common PS themes identified were Communication (57% of cases), Human factors (39%), and System issues (37%). Anonymous written feedback was obtained; learners reported improved knowledge and ability to identify lapses in PS and to propose potential solutions to prevent similar future events. They expressed a desire for additional PS and quality improvement education.
Discussion:
Our results show that third-year medical students are able to identify lapses in PS and able to propose solutions. This aligns with the Association of American Medical Colleges (AAMC) goals of entrustable professional activities (EPA) 13. We intend to expand the curriculum to other third-year core clerkships.
Keywords
Introduction
Critical lapses in patient safety (PS) were highlighted in 1999 by the Institute of Medicine (IOM) landmark report on PS, “To Err is Human: Building a Safer Health System.” 1 The IOM estimated that between 44 000 and 98 000 patients die every year from preventable medical errors. Since then, PS and quality improvement (QI) movements have transformed the healthcare culture in this country with significant impact on medical education across the spectrum from undergraduate medical education to graduate medical education and beyond. Newer estimates suggest that medical errors may play an even larger role in patient deaths. In 2016, Makary et al reported that approximately 251 454 deaths yearly result from medical errors. Medical errors therefore are estimated to cause 9.5% of deaths in the United States annually, making it the third leading cause of death, after cardiac disease and cancer. 2 Knowledge about PS is critical to physicians in training to promote future excellence in patient care.
The need for education in PS has been recognized by accreditation bodies including the Accreditation Council for Graduate Medical Education (ACGME) and the Association of American Medical Colleges (AAMC). However, PS curricula vary substantially throughout undergraduate and graduate medical education. The ACGME has adopted the concept of resident and residency program evaluation based on showing competency in a series of milestones, and undergraduate medical education (UGME) has used the similar concept of entrustable professional activities (EPAs). Institutions sponsoring residency programs are evaluated by the Clinical Learning Environment Review (CLER) program which has six focus areas, including PS and healthcare quality. The ACGME Common Program Requirements 3 require resident training in PS and healthcare quality for initial and continued accreditation of a residency training program. The AAMC has also recommended that this learning be evident in the medical school curriculum and has included identifying systems failure and contributing to the culture of safety and improvement as one of the 13 Core EPAs for entering residency. 4
The literature on PS curricula for medical students is limited. A survey in 2012 found that less than half of medical schools had a formal PS curriculum. 5 Another study found that students rate their own safety skills highly yet have many misconceptions about PS, highlighting the need for new approaches to curricula. 6 A survey of medical students suggested that they rate real-life examples of PS events highly in respect to learning about PS, 7 and similar work strongly suggests that students prefer to learn from case-based safety events. 8 However, reports of specific PS curricula are scarce in the literature9,10 and many are didactic, module, or simulation based.11,12 Therefore, our curriculum was designed to incorporate the students’ real patient care experiences, recognizing that PS education may be more meaningful when placed in the context of firsthand clinical care.
Based on the need to improve PS education to meet the above identified goals, we designed a PS curriculum targeting third-year medical students. Our campus is part of a multi-campus medical school distributed over a large geographic area. Students complete the first year of basic science education at one of the regional campuses and then move to our campus to complete the remaining 3 years of training. Students are introduced to PS concepts during the second year of medical school training. During the M2 year, students are encouraged to complete modules from the Institute for Healthcare Improvement (IHI) 13 and participate in longitudinal PS sessions. The IHI modules are an online program that contains both introductory and advanced education on PS and QI. The longitudinal sessions consist of panel discussions, simulations, and didactics that highlight various topics including team communication, root cause analysis, and human factors. The purpose of our curriculum is to provide a foundation of PS early in the clinical education curriculum, so that learners can display proficiency in the care domain of PS as they progress through training. Therefore, we targeted learners who are in their first year of direct patient care and introduced the curriculum in pediatrics, a core clerkship taken by all students.
Methods
Curricular design: SAFE framework
We designed an educational intervention and novel framework to analyze PS events during the Pediatric Clerkship using Kolb’s Model for Experiential Learning. 14 Building on the principles of Kolb’s model, the SAFE framework provides a structure to help learners formulate their experience, reflect, and analyze the impact on PS (Figure 1). A literature search was used to help identify the key components required to report patient safety concerns. The components of SAFE are Safety concern (description of the case), Action taken (what happened as a result), Failure (causes of the event, linked to predefined safety domains), and Effects (effect of the event on the patient or team). This simple framework was felt to be intuitive and easily used by students as part of their first introduction to PS events, in contrast to other methods of event analysis that are designed for more advanced learners. We developed SAFE as a simple acronym to use to discuss the components of a PS event, while similar acronyms exist as PS tools (such as those promoted by TeamSTEPPS) 15 , to our knowledge this approach has not previously been applied to medical education.

Outline of the SAFE framework and safety domain structure used for case discussion.
Curriculum: PS morning report
Students were introduced to PS morning report, using the SAFE framework, as part of the orientation to the pediatric clerkship. The clerkship is 8 weeks long and split equally between 4-week outpatient and inpatient experiences. Two safety morning report sessions were held per clerkship, one midway through and one near the end of the rotation. This was done so that students who were on the inpatient portion first could present a case at the midway point, and those on the inpatient portion second could present at the end; however, there was no requirement that the case be from the inpatient setting. Each student presented one case. Utilizing two sessions was beneficial as there are 10-12 students per clerkship, and the team could cover about 5-6 case discussions per 90-min session. Approximately 1 week prior to each session, students were sent a reminder email with supporting documents (example patient write-ups, the SAFE framework outline, and a curriculum outline). The morning report was used for formative purposes only, even though participation in the session was mandatory.
Session learning objectives included (1) teaching students to identify actual and potential errors in patient care; (2) discuss the domains of PS using the SAFE framework with student-identified patient cases; (3) identify methods or system improvements to overcome these safety issues; and (4) foster a safe and supportive learning environment.
Prior to each session, the students were expected to identify and write up a patient encounter in which they were either concerned about PS or where an adverse event occurred in either the inpatient or outpatient setting using the SAFE framework. The format of each session was a short didactic session on a key safety concept followed by a discussion of the PS cases. The first didactic session focused on an overview of PS, the different types of medical error, and the importance of communication in preventing medical error. The second didactic reviewed the importance of and strategies for disclosure of medical errors to patients and families. The didactics supplement the case discussion and as such were intentionally not presented prior to the student’s write up of their case.
Faculty with expertise and skills in PS and QI helped facilitate the case discussion and provide feedback to the students on key learning points and issues within each case. Faculty are interdisciplinary and come from the departments of Medicine, Pediatrics, and Emergency Medicine. Each of the faculty has been involved in developing PS and quality curriculum for their respective residency programs.
Evaluation tools
Students completed an 11-item questionnaire at the completion of the clerkship. The items were to be rated on a 1-5 Likert-type scale with 1 being strongly disagree and 5 being strongly agree. Students could add any free text feedback at the end of the questionnaire.
Data analysis
We tracked the number and types of safety domains identified by both students and faculty during the sessions. These were analyzed descriptively as shown in the results. For quantitative analysis, the Wilcoxon signed-rank test was used to compare the number of domains identified per case between students and faculty.
Results
Our curriculum was started in February 2015 and we analyzed the curriculum in September 2016. Data were examined for 75 patient cases written by third-year medical students during their Pediatric Clerkship.
In total, 63 of 75 students completed the feedback form (Table 1). We found that there was a general positive response to the sessions. Students tended to disagree that their prior PS training was limited (question 1), which is consistent with the other safety curricula at our medical school as outlined above. Students also reported that after the sessions, they could better recognize a medical error or adverse event and recognize the role of communication in preventing these errors. The students felt strongly that the session provided a safe and supportive learning environment to discuss PS (question 5). In general, the sessions received positive feedback from the clinical learners.
Student feedback on the curriculum (N = 63).
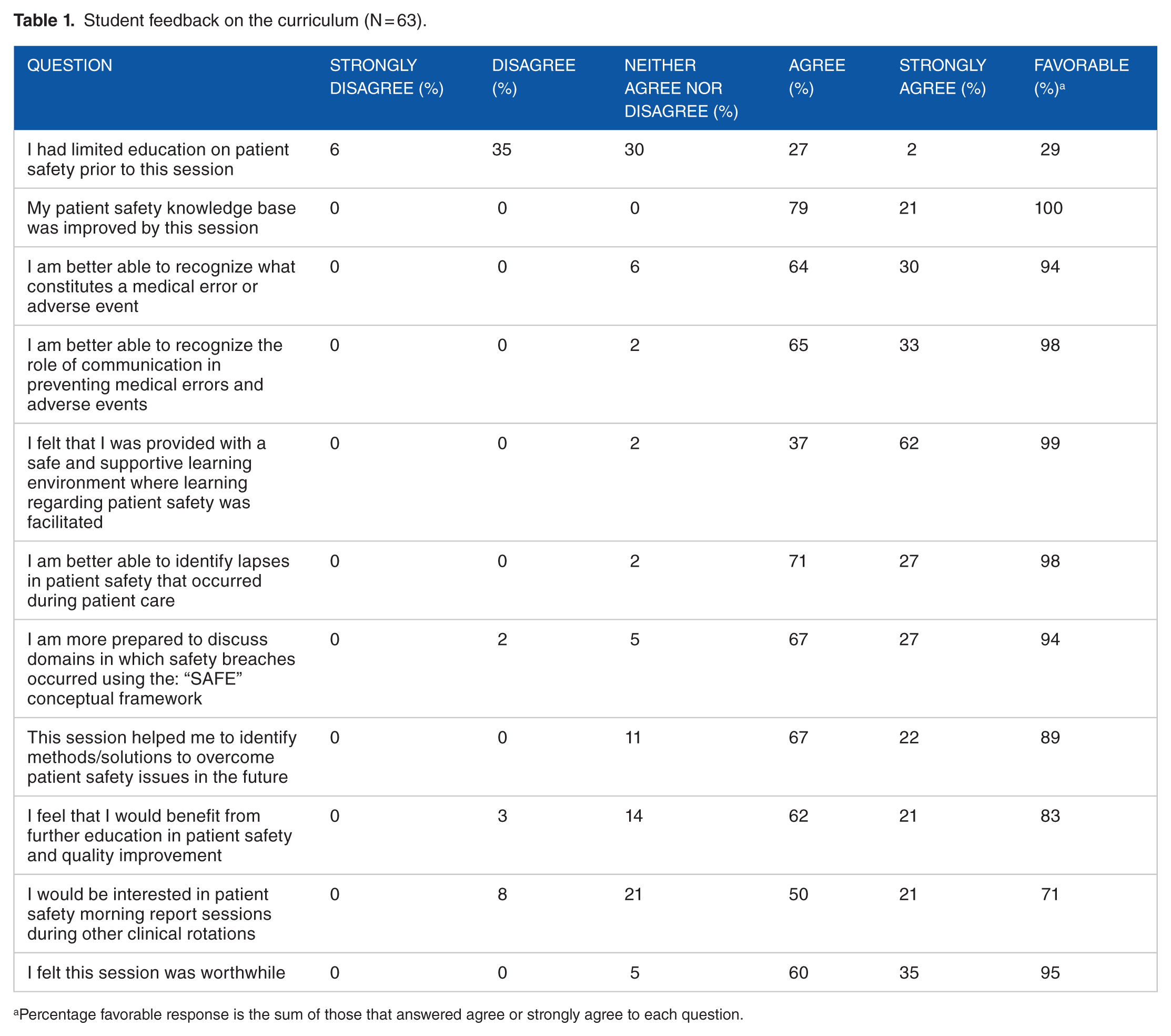
Percentage favorable response is the sum of those that answered agree or strongly agree to each question.
We also compared student-identified safety domains (see SAFE Framework in Figure 1) to domains identified by consensus of the curriculum faculty who reviewed each student case. Student- and faculty-identified domains were similar in distribution (Figure 2); communication was the highest identified domain present in 57% and 64% of the cases (student and faculty, respectively). Faculty cited system factors and patient and caregiver engagement more often than students. We also compared how often students and faculty were in agreement on whether each domain contributed to a PS case (Figure 3). Agreement was highest in communication and lowest in human factors. Faculty consensus on average identified 2.4 domains per case, while students identified only 1.9 domains (P = .0007, Wilcoxon signed-rank test). In some cases, student-identified domains that faculty did not feel were warranted; removing those domains from the analysis, the student mean decreased to 1.4 domains per case (P < .0001 compared with faculty mean, Wilcoxon signed-rank test; note that all student-identified domains were included in the data in the figures).
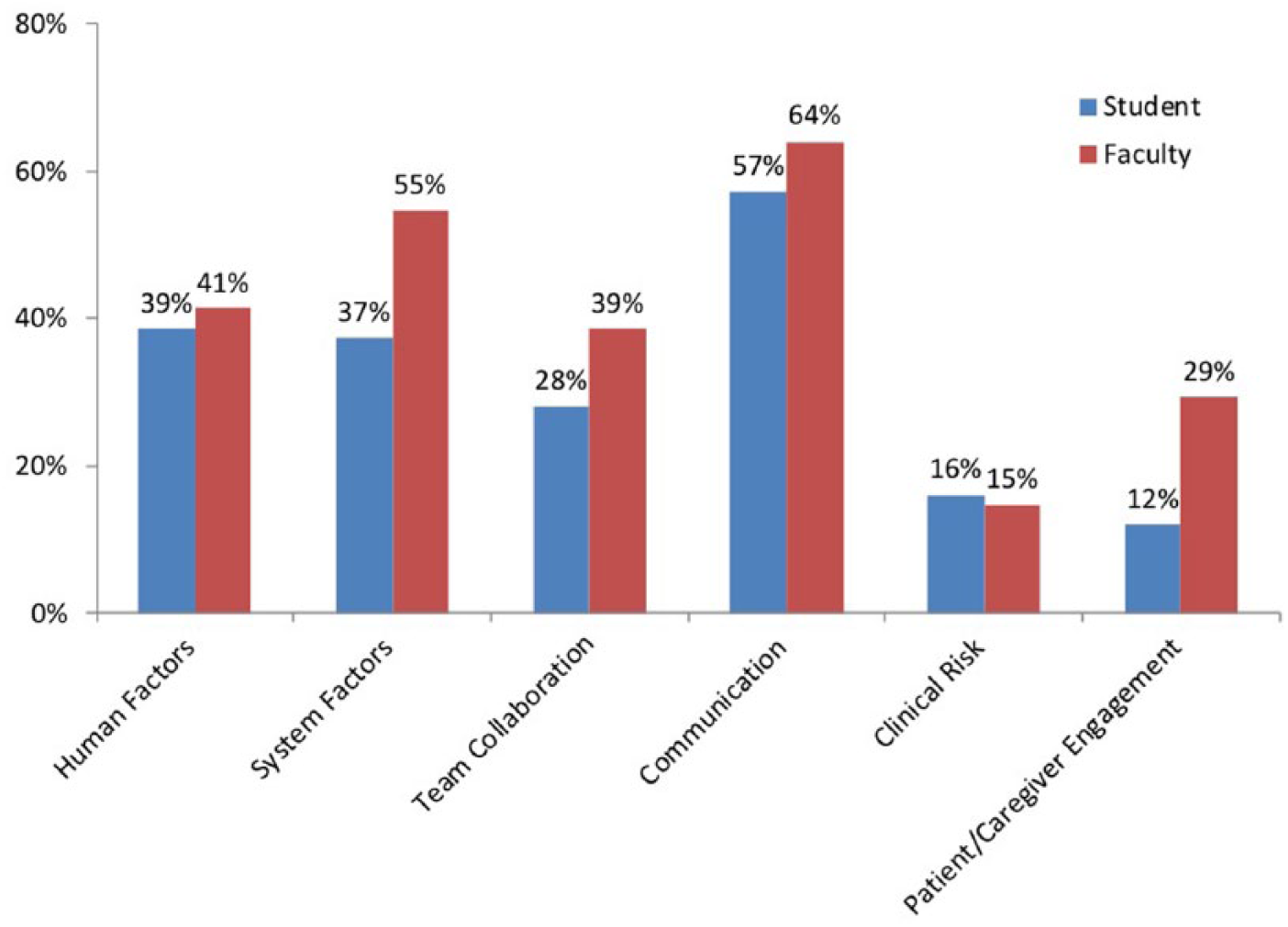
Analysis of cases by safety domain. Percentage of cases in which the safety domain was identified as contributing is shown. Multiple domains can be identified for each case. Student-identified domains are in blue and faculty-identified domains are in red. N = 75 cases.

Student and faculty agreement about safety domains. Percentage of cases in which both faculty and students were in agreement about whether or not the domain contributed to the case. N = 75 cases.
Discussion
Patient Safety Morning Report is a novel curriculum integrated with real case scenario discussions, identification of specific safety domains, and brainstorming of potential solutions to prevent similar safety errors in the future. This curriculum laid a pathway for students to become PS liaisons, and opportunity to initiate discussion about PS in the early clinical years. It helped students to voice safety concerns and identify possible domains involved. Interestingly, our curriculum assumed that each student would be able to identify at least one safety lapse to discuss, and since starting we have never had a student who was unable to bring a case for discussion. This highlights the ubiquity of PS issues and medical students’ ability to recognize them. We feel this curriculum will serve as a starting point for students to recognize PS events and become more vocal about them, helping develop a positive safety culture in the hospital.
Given the positive feedback from the participants, we infer that education on PS is meaningful to students in the early clinical years. Based on the feedback we received, we met the objectives of the curriculum, which were to identify lapses in PS and discuss the safety domains. Interestingly, students did not identify both systems factors and patient/caregiver engagement as contributing domains as often as faculty (Figure 2). This is consistent with prior work that found that medical students are more confident about clinical aspects of PS (eg, hand hygiene) than contextual aspects (eg, systems factors). 16 These findings may be explained by the lack of clinical exposure for early third-year students, and our curriculum can help them recognize the importance of these domains in preventing adverse events. However, our data are limited as we did not assess students’ baseline knowledge regarding PS and their responses on the survey may be influenced by prior knowledge or other cognitive biases. Students had prior access to the IHI modules, but these were not required and the percentage of students completing them was not tracked, so learners may have had variable previous exposure to PS concepts that affected our results. The goal of the sessions was not to improve knowledge, rather to enable students to feel comfortable discussing PS in a safe environment; nevertheless, pairing our curriculum with a knowledge-based program could be beneficial in future work. The differences between faculty- and student-identified domains suggest a need for improvement in our students’ knowledge base as well and could similarly serve as an avenue for future curriculum development.
During case discussion, we also highlight the importance of reporting the error to the hospital safety event monitoring system, as this will improve the clinical environment and ensure necessary steps are taken to prevent similar errors in future. Safety event reporting is stressed by both the AAMC 4 and ACGME 3 as an integral part of the education and clinical training of physicians. This curriculum is designed upon and directly connects to AAMC’s EPA 13 and can be implemented at other institutions to meet this educational objective. While we did not have a formal system in place for reporting of events that students identified if not already done so by the primary medical team, if an event seemed serious enough, our faculty would ensure a report had been placed or the event otherwise addressed. Students were not required to report events or to follow up on events in any way; instead, this was the faculty’s informal responsibility after the case discussion, most commonly done by contacting the unit or medical team involved to make sure appropriate actions were taken. In these instances, we emphasized to the students that they would not be associated with our follow-up or tied to the event in any way. This discussion further served to emphasize the benefits of a positive safety culture. Fortunately, we did not find our students hesitant in reporting cases or concerned about potential negative consequences of reporting.
Students appreciated the safe learning environment to discuss lapses in PS, and the training they received to become PS advocates in their early clinical years. Overall, the positive feedback from the students and specific comments, such as “I appreciate the non-judgmental environment to discuss medical safety situations to prepare us if, and when, we encounter them later in practice,” indicate the success of the curriculum. In the future, we see this curriculum expanding to include different clerkships, focusing on different types of errors and adverse events pertinent to each specialty (eg, procedural errors during surgical rotations, diagnostic errors, and high value care during medical rotations). Our survey results indicated enthusiasm for expansion of the curriculum, as 71% of students agreed or strongly agreed that they would be interested in having a similar session in other clinical clerkships. Evaluation of our curriculum also occurred during the UGME Pediatric Clerkship review, and specific feedback was that the “SAFE patient safety case study and discussion session was praised highly by the students, and indeed the focus group agreed that this should become a common feature in all core clerkships or at least a minimum of three of the core clerkships, so as to maintain a focus on safety throughout the M3 year.” We envision a longitudinal curriculum starting with introduction and didactics for students during pre-clinical years and more case-based discussions during clinical years. This curricular framework can also be modified and expanded for use at other medical facilities to use with their learners at both undergraduate and graduate levels of training.
Footnotes
Acknowledgements
The authors would like to acknowledge the Research Open Access Publishing (ROAAP) Fund of the University of Illinois Chicago for financial support towards the open access publishing fee for this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
MA declares that she is a shareholder in CGN Global. There are no other potential conflicts of interest to disclose.
Author Contributions
MB, VKE, RW, GW, and MA developed the curriculum. MB, VKE, and RW implemented the curriculum, and KH later joined as faculty. All authors contributed to data analysis/interpretation and manuscript preparation.