
Abstract
Vaccine hesitancy is an increasing and urgent global public health challenge. Medical students’ encounters with vaccine-hesitant parents, however, remain incidental and unexplored. During pre-clinical training, the vaccine-hesitant parents are typically represented through impersonal text-based cases, lists of their concerns, and sometimes a virtual patient. However, in reality, vaccine-hesitant parents have many health beliefs and arguments that are accompanied with intense emotions, and students remain unaware and unprepared for them. This study is an experimental pilot test in stimulating the medical students’ understanding of, and ability to respond to, vaccine-hesitant parents’ beliefs and questions. An arts-based video scenario and a writing exercise are used to demonstrate a rich case of vaccine hesitancy, including a simulated dialogue between a parent and a student. The study invites vaccine-hesitant parents to ask questions to medical students, then it incorporates these questions in a video scenario and subsequently invites the students to answer these questions as junior doctors. The study examines how the peer group discussion after the video viewing resembles a hospital breakroom conversation and how the written dialogue with a vaccine-hesitant parent simulates a consultation-room encounter.
Keywords
Introduction
Lack of confidence in vaccines is a growing phenomenon, as vaccines are perceived unsafe and unnecessary by groups of individuals especially in the developed countries. 1 The determinants of vaccine hesitancy are complex, and to be able to deal with it would require understanding of its diverse context-specific causes. 2 A large portion of medical students and residents, however, feel insufficiently trained in vaccine-safety communication and poorly prepared to respond to vaccine hesitancy.3–5 Accordingly, as poor doctor-patient communication is considered one of the factors contributing to the rejection of vaccines, 6 the SAGE Working Group for Vaccine Hesitancy calls for appropriate training for medical and health care students concerning encounters with vaccine-hesitant individuals. 7 In existing studies on vaccine communication training, video-based cases or writing exercises are generally not included as education modes on vaccine hesitancy. There does however emerge innovative vaccine hesitancy curricula, which involve videos as well as role-playing simulations. 8 Furthermore, some medical schools employ virtual reality applications to train students or residents to encounter a vaccine-hesitant parent. 9 However, the actual parents’ voices are typically not heard in the classroom.
The current vaccine hesitancy problem-based scenario employed as a part of third-year medical students’ prevention study module in the University of Tampere Faculty of Medicine and Life Sciences is a 2-sentence, text-based description without any visual material. The scenario involves a mother and a baby (the father is absent), and it identifies their ages and the mother’s education but excludes aspects such as their emotional state when in the consultation room: A 28-year-old nutritionist mother is in a children’s health care center with her 6-week-old child and wants to talk about the child’s future vaccination. The mother has wondered if it would be better for a child to go through the children’s infectious diseases so that their resistance would develop naturally.
Although such a minimalistic scenario can form a foundation for multiple kinds of encounters, it also creates an illusion of an emotionally neutral situation and is likely to seem easier to the student than a dialogue with an actual parent. Furthermore, whereas the current scenario introduces (indirectly) merely one argument for hesitancy, the appreciation of a ‘natural’ development of the immune system, in reality, the variety of beliefs behind vaccine hesitancy is much greater. In addition, the scenario of vaccine hesitancy differs from most of the problem-based learning (PBL) scenarios, as it presents a clinical encounter in the absence of patient’s symptoms or problems. In typical PBL case, the students work together to understand a single patient’s medical problems. 10 However, in case of vaccine hesitancy, many parents do not experience having a problem at all; their non-compliance is mostly a problem for the physician.
Although the use of video sometimes simplifies complex concepts, 11 in the intervention described in this article, the purpose is to demonstrate the complexity of a situation that may appear unrealistically simple as a written case. Furthermore, it is a case that cannot be solved with only clinical information or skills. The arts-based video in this intervention represents a rich narrative case by realistically portraying the complexity of patient presentation and interaction, stimulating the students’ holistic awareness of vaccine hesitancy. It is here considered that understanding the perspectives of the people for whom immunization services are intended is essential in forming a meaningful dialogue with them. 12 The study describes and evaluates the intervention, as it parallels 2 different modalities of relating to vaccine hesitancy: a group discussion following a video viewing and an individual (albeit dialogical) writing exercise.
Methods
Intervention description
One third-year medical student PBL tutor group (f = 3, m = 6), tutored by one of this paper’s authors (J.T.L.), was recruited for this experimental pilot study. A study coordinator had placed the students in the PBL groups independently of this study; thus, the students were randomly selected. J.T.L. was invited to participate in this project as he had pre-existing interest in arts-based methods for medical education and experience of employing performative exercises in particular. The study was conducted as part of the prevention study unit and particularly as a case about vaccine hesitancy. The students had not received previous training in vaccine communication, although they have been exposed to some pre-clinical communication training as part of their vertically integrated spiral curriculum. All the students gave their informed consent. The video Conversations with vaccine-critical parents was viewed in 2 parts (9 and 7 minutes), during 2 different PBL sessions. The structured group discussions (45 and 30 minutes) were conducted accordingly during 2 separate PBL sessions on August 22 and 26, 2016. The tutorial discussions were structured with open-ended questions. These included identifying reasons for vaccine hesitancy the video included (and excluded), as well as the types of information and health care relationships the parents were currently lacking. In addition, the discussion invited the students to share their personal attitudes towards vaccine hesitancy. The discussions were audio-recorded and transcribed verbatim. The steps in the intervention are visualized in Figure 1.
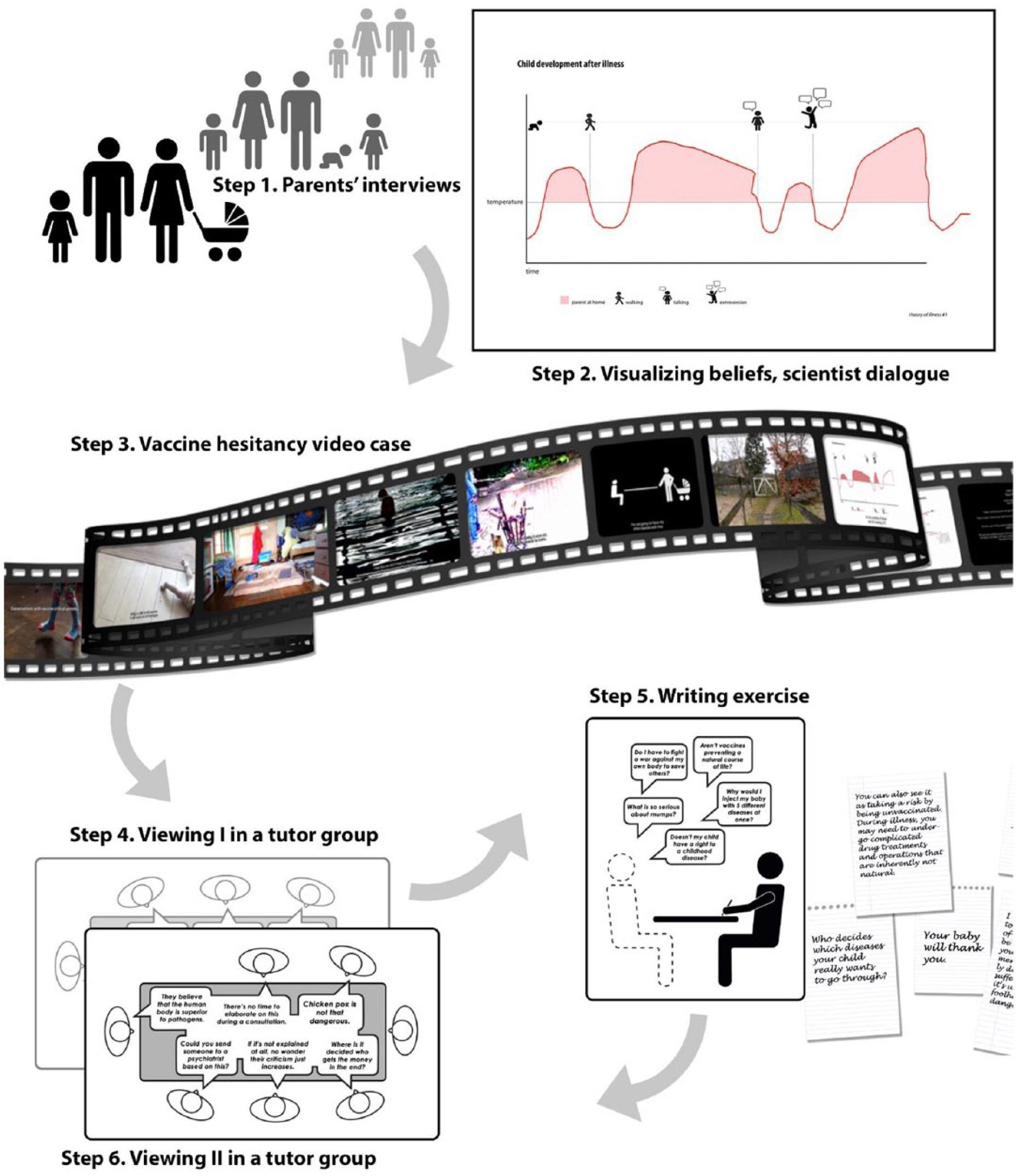
Steps in the intervention.
The writing exercise was to be completed at home between the 2 in-person sessions. In this exercise, the students were invited to answer 7 of the parents’ questions presented in the video, playing the role of a physician. The students had 3 days to complete the exercise, and they were free to search the literature if they felt answering the questions required doing so. As part of the intervention evaluation, the study compares these individual answers with the themes that emerged in the group discussions.
Conversations with vaccine-critical parents
As part of the video-making process preceding this video pilot study, one of the authors (K.K.) interviewed 9 vaccine-critical parents in the Netherlands and Finland in 2015 and 2016. The parents were recruited through K.K.’s social network, inviting both mothers and fathers of all levels of hesitancy from delay or selection to total refusal. Their health beliefs were not known before the interviews, but these were identified in the interview (analysis) instead. During these interviews, the parents were not only invited to elaborate on their views on immunization but also their experiences in children’s health care system. In addition, each parent was invited to pose a question about immunization to a medical student and donate home video footage of their children for the film. The purpose was not only to create a video that simulates clinical encounters but also to appreciate the parents as whole persons and learn about their particular health beliefs as a necessary foundation to encounter them meaningfully in the future. Furthermore, the video’s purpose was not to arm the students with convincing counterarguments against the parents’ beliefs. The video intentionally digs deeper into such beliefs by visualizing and deconstructing them, considering that only by gaining understanding of these and tolerance for the emotions that they raise, can the students begin to think of constructive communication strategies.
As the parents were kept anonymous and not filmed during the interviews, the home video footage was inquired to create a visual composition for the first part of the film. The home video footage thus did not contain any narratives that would have been included in the interview analysis. There are several reasons for the parents’ anonymity. First, as their visual appearance has no clinical relevance in the case, their portrayal would risk creating stereotypes of how ‘such parents’ look like. Second, the main purpose of the video is to expand the student’s perception of the parents beyond the consultation room (view), thus ‘seeing’ them as whole persons instead of talking heads. In the absence of the parents’ faces the video stimulates the students’ focus on the nuances of what is being said. Third, vaccine hesitancy is a volatile topic that raises strong emotions. This study prioritizes the participant safety in that by agreeing to an openhearted controversial interview, the participants will not be subjected to a risk of receiving negative reactions afterwards.
The film is trilingual (English, Dutch, Finnish), allowing the parents to speak in their native language, and is subtitled in English, which is a standard mode of translation in broadcasting both in the Netherlands and Finland. As part of the arts-based data analysis, K.K. identified the parents’ main health beliefs and created diagrammatic representations to be discussed with senior scientist Johan Holst from the Norwegian Institute of Public Health. All these aspects (parents’ interviews with their home videos and health belief diagrams with a scientist’s perspective) are included in the video.
K.K. created the video during May-August 2016, following several discussions with another study author (K.H.). The video has 3 main parts: (1) the parents’ everyday lives, which form a central visual aspect and an important authenticity factor in the film; (2) health care encounters, based on the parents’ actual experiences; and (3) parents’ beliefs explored through diagrammatic visualizations and an artist-scientist dialogue.
The video supports learning about vaccine hesitancy in the following ways:
Stimulating students to take the case seriously by the presence of authentic vaccine-hesitant parents.
Introducing a variety of health beliefs and arguments supporting vaccine hesitancy.
Demonstrating (reasons for) failed vaccine-hesitancy encounters in health care.
Presenting a non-linear and ethically complex case that cannot be solved with only strict medical information.
Role-modeling a vaccine professional who is reflexive and does not show frustration.
Theoretical background for the video case
The video case connects to the views of medical humanities and narrative medicine, 13 building on aspects of Bakhtin’s dialogic theory. 14 It challenges the monologic and linear qualities in narratives currently produced in medical practice and education. A linear perception of the body and health, for instance, is considered a prevailing problem in health care, 15 manifesting in narrative formulas as ‘the patient becomes ill; patient is cured by physician expert; patient is restored to preillness state’. 16 Moreover, while doctor-patient interaction is characteristically polyphonic, being imbued with the voices of all who are related to it, 17 the medicine is typically characterized by a ‘monological mindset’. 18 This results, for instance, in doctors being criticized for not recognizing others’ perspectives. 13 Simultaneously, although the doctor’s diagnostic task involves reduction of polyphony, ie, different opinions, beliefs, and fears, the monologic context of biomedical theory risks discarding the patient as a person. 17
One of the main educational functions of the video is to introduce the student to everyday lives and beliefs of a particular patient population with all their messiness and contradictions, in a non-linear chapter-like structure instead of a dramatic narrative. This is an unusual approach to creating video scenarios. While tolerance for ambiguity has been recognized as one of the fundamental skills in developing an antiauthoritarian professional identity, 19 many existing video scenarios reorganize the chaotic real-life events into well-ordered linear narratives with expected endings. 20
Although videos are used for various educational purposes, and with different pedagogic techniques, there can, however, be distinguished videos addressing ‘softer’ aspects of medicine, such as ethical dilemmas, and the clinical patient cases to be diagnosed in PBL. Yet, instead of keeping such curricular facets separate, there is a need for integrative approaches that merge the humanities-related aspects of medicine with the conventional focus of diagnosis and problem-solving. 21 As opposed to elective humanities teaching delivered by nonmedical teachers, alas, often dismissed by the students as irrelevant, 22 this video is developed for the core medical curriculum, to be delivered in small-group settings by the clinical educators. Moreover, this intervention uses transformative learning theory according to which the students are stimulated to reflect their knowledge and attitudes in situations that deliberately challenge their views. 23 The video viewing in particular employs the so-called movie clip teaching methodology, in which students are invited to share and contemplate the insights and feelings evoked by the film and relate them to their peers’ responses. 24
Evaluation of the video case
The video displays a range of authentic vaccine-hesitant parents’ arguments, aiming to increase the students’ ability to encounter them. Instead of focusing on one vaccine-hesitant individual, as the text-based case does, the video maps a specific sub-culture population: well-educated vaccine-hesitant parents (7 mothers, 2 fathers) without religious arguments. Some of the issues put forward by the parents have been recognized in previous studies as well. For instance, the perceived benefits of illness have been identified as one of the key reasons for vaccine hesitancy among those following an anthroposophical lifestyle. 25 Many studies, however, do not identify concrete narratives under abstract categories such as ‘personal beliefs’ or ‘philosophical reasons’. 26 The video case introduces actual parents’ stories that demonstrate such umbrella categories, some of them being identified in the previous phase of this study only. 27 The specificities of the parents’ lives are here considered important in demonstrating the ‘realness’ of the phenomenon and in motivating the students. Thus, while many video cases exclude the patient’s everyday life and its psychosocial aspects, focusing on medical interviews in the examination room only, 28 this video gives voice to the parent’s lifeworld 29 and opens the door visually to their homes and everyday activities.
Collaboration with senior scientist Johan Holst was initiated by K.K. in 2015 during an interdisciplinary international multi-year project on vaccines <Immune Nations>. For a meaningful artist-scientist collaboration, it is essential that the collaborators share authentic interest towards each other’s fields and tolerate differing views on vaccines. Such collaborators can hardly be found by random. Thus, although the pilot study was conducted in Finland, the vaccine researcher’s nationality does not play a significant role here. It is rather his willingness both for a respectful meaning-making of the parents’ beliefs and the arts-based methodology that are crucial. Furthermore, as vaccine hesitancy increases in many developed countries, and the parents included represent several nationalities, the video is relevant and applicable in many different countries.
Collaborative data analysis after video viewing
Immediately after the 2 PBL sessions in which the video was viewed and discussed, K.K. and J.T.L. conducted collaborative data analysis sessions, sharing their immediate observations and interpretations. K.H. participated in the second collaborative analysis session, interpreting the emerging themes from the existing curriculum viewpoint. These sessions resulted thus in identification of the main themes in the data, and they were audio-recorded for memory aid. Collaborative data analysis is here considered fruitful, if not a necessity, as the authors represent different disciplinary fields. Subsequently, followed by multiple re-readings of the group discussion transcripts, the data are thematically coded and tabulated by K.K. according to various different point of views, and attitudes/communicative strategies the students initiated to make sense of vaccine hesitancy with their peers.
Writing exercise
The exercise involved the following questions, extracted from the parents’ interviews:
Why does my baby need tetanus and hepatitis B vaccines?
What is so serious about a mumps?
Why does my baby get so many vaccines at one time? In real life, you never get 5 diseases at the same time.
Doesn’t my child have the right to go through children’s infectious diseases? These support mental and physical development.
Do I have to fight a war against my own body to save others?
I want to live as natural life as possible. How does ‘natural’ relate to vaccination?
Is the purpose of life, according to medicine, to live as long as possible?
The students were instructed to answer from their role as a physician, imagining as if the parent would be sitting across them. There were 2 main aspects examined in the students’ answers, forming thus the guiding principles in their analysis: (1) whether the student addressed the parent in second person and in a professional role and (2) the strategies used in addressing the parent’s concern. Both the group discussion analysis and the analysis of the written exercise identify the used point of views and tone of voices, ie, the students’ ability to respond to vaccine hesitancy from different ‘registers’.
Theoretical background for the writing exercise
The dialogical writing exercise, like the preceding video, intends to stimulate an expansion of the monological mindset of medicine, 18 manifesting in, for instance, bombardment of clinical information or harsh judgment of the parent’s decisions. Furthermore, in the study design, it was anticipated that the group discussion has a different function than writing, acknowledging that talking about a patient with peers and talking to a patient privately are different aspects of the medical profession. Previous studies have, in fact, suggested that students give more thought to their written responses as opposed to group discussions. 30 The framework for the writing exercise is inspired by philosopher Martin Buber’s word pairs ‘I-You’ and ‘I-It’ and how these may take place in a dialogue with a vaccine hesitant parent. 31 The purpose of writing here is to bring the medical student face to face with a patient 32 and to acknowledge the parent as a person. This is in line with many students’ needs for ‘learning the human side of medicine’. An eloquent expression of this need is Messinger and Chin-Yee’s 33 exploration of Buber’s ‘I-You’ and ‘I-It’ and how these parallel different modes of caring for patients. The writing exercise aims to address the vaccine-hesitant parent as ‘You’ instead of ‘It’ as a condition or a collection of labels. In addition, next to ‘It’ as a medical condition, the exercise distinguishes ‘I’ as a physician from ‘It’ as the ‘voice of medicine’, manifesting in communication that is relying exclusively on the biomedical model. 34
This imaginary face-to-face encounter is initiated during the vaccine-critical parents’ interviews, when each of the parents addresses the student-physician as ‘You’ with their questions. These questions are implemented in the writing exercise, either remaining formulated the same way as the parents initially asked them or reformulated into questions from their most predominant statements. The video purposefully does not provide a physician role model for an immunization encounter. Specifically, one of the writing exercise’s central aims is to activate the student to explore aspects of their existing attitudes and communication and to reflect how these may affect their encounters with vaccine-hesitant parents.
Evaluation of the writing exercise
Only the first 3 of the parents’ questions in this study related directly to vaccines and infectious diseases. The other 4 questions were concerning lifestyle choices, child’s rights, ownership of one’s body, and the definition of ‘natural’ and eventually the physician’s/medicine’s role in the human life cycle. The questions are asked with different emotional intensities, both by mothers and fathers. Therefore, answering these questions requires multiple communication strategies. This is in line with previous studies that have suggested that a single mode for vaccine communication fails to appreciate a spectrum of the parents’ different cognitive decision-making styles. 35
Although the group discussion often proceeds quickly as the participants respond to one another, the writing exercise allows time to carefully consider the answer, including thinking what the parent would find important to hear and what kind of professional one wants to portray. Writing allows the student to practice answering a variety of vaccine-critical questions and to explore various communication strategies in their professional role. The purpose was, however, not to practise these questions within the normative structures for medical encounters, nor to distill a particular anti-vaccine argument from a longer narrative. Instead, the exercise is experimental in that it jumps directly (after the video viewing) into what is considered the core of the parent’s concern. This allows an exposure for a multitude of different anti-vaccine arguments with little repetitive writing sections. However, the exercise is not training the student for yet another critical skill: beginning and ending an encounter with a non-compliant patient.
Results
Group discussions: making sense of vaccine hesitancy with peers
The group discussion develops several perspectives in learning about vaccine hesitancy. In the first instance, the discussion enables peers to vent their frustrations, including black humour, and to clearly take the role of a future vaccine advocate. However, after this initial phase, the students begin to develop alternate perspectives and explanations for vaccine hesitancy, having a strong need to make sense of it. In search of learning objectives, they admit lacking knowledge of the governmental immunization programme and many infectious diseases. In terms of their future practice, the students already anticipate a lack of resources (time) to address the parents’ concerns. This leads to understanding the frustration many physicians are displaying to their vaccine-hesitant patients, even though this is not an optimal way of communication. The group discussions, however, also acknowledge various counterarguments related to immunization. For instance, the students share their questions about the opaque role of the pharmaceutical industry and the necessity of certain new vaccines. Furthermore, there emerges an understanding for an individual parent perspective: if parents lose their child because of a vaccine side effect, the idea of herd immunity does not comfort them.
Responding to parents’ desire for a ‘natural life’
The group discussion excerpt below illustrates the students’ meaning-making on the parents’ desire to live a so-called natural life. The students found this aspect to be extremely strong in the parents’ arguments and were surprised to hear the radical views certain parents introduced, particularly when a mother talked about ‘acceptance’ of natural selection and believing in destiny. Thus, the video stimulates the students to ask follow-up questions, which are then offered to their peer group, as an attempt to make sense of the origins of the parents’ non-compliance: Student 4: One of them really emphasised that they are living this kind of natural life, so just where do they draw its boundaries? Student 5: Yeah, like are they using any medication for instance? Student 7: Is using a seatbelt in traffic bad because it can save you from a fatal accident? So, those people [who face an accident] are supposed to die then? Student 2: There weren’t safety belts before either. Student 7: So, all the prevention is then unnecessary? Student 2: So basically, all the healthcare services . . . are blocking natural selection.
Changing perspectives: physician-parent-pharma
In this part of the group discussion, the students generated various viewpoints that expressed understanding the controversy around vaccines. They pondered, for instance, the necessity of the chicken pox vaccine, previous mistakes in vaccine production, and the impossibility in accepting the risks from a misfortunate parent’s viewpoint. They also recognize the role of the provider’s poor communication in growing vaccine hesitancy while simultaneously anticipating a hurried practice and the incapability of addressing the problem: Student 5: I believe that many of the vaccine-hesitant parents care about their child, and that’s why they are so worried about what is injected in their child. But if it is not explained at all, then I’m not surprised that their vaccine-criticism just grows. Student 7: The physician may not have patience when there are so many hippies like that, so they are just fed up. Student 2: Also, like during a normal consultation, there aren’t possibilities to elaborate on that situation . . . Student 7: Yeah, hurry and all. Student 5: Of course, there’s been misunderstandings or mistakes in some drug or vaccine production that have caused harmful effects. Student 6: Well, you can’t say that ‘we are now rescuing a million lives here, but your child died because of this vaccine, sorry’. That’s, of course, hard to understand for the parent.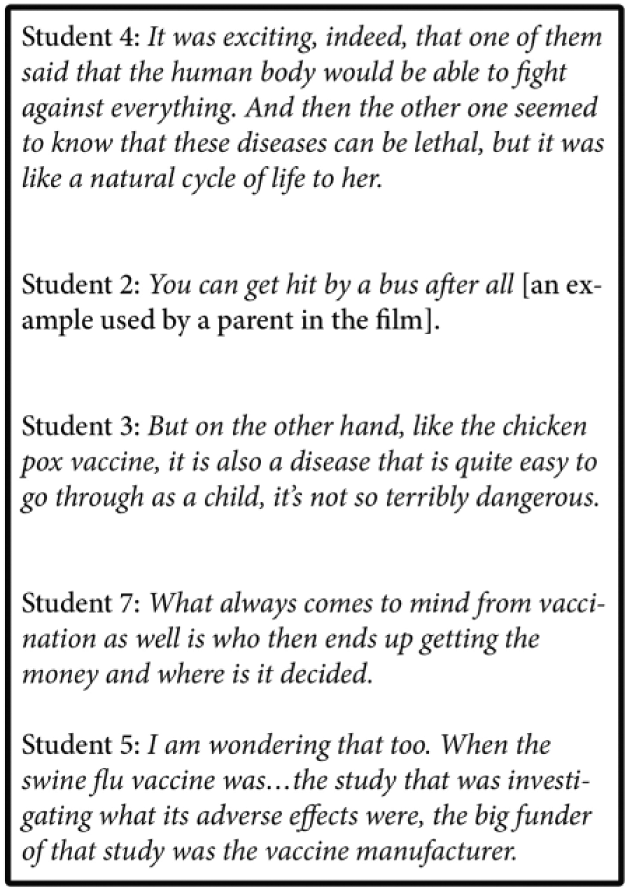
Writing exercise: simulated encounter with a vaccine-hesitant parent
There emerged 3 main modes of communication in the students’ answers: (1) addressing the parent and child as persons: talking in second person, acknowledging the parents’ rhetoric, asking counter questions and even involving self-disclosure; (2) delivering impersonal medical information in a passive voice; and (3) answering with sarcasm and disrespecting the parent.
Addressing the whole person/lifeworld
Most students (n = 6) were, to various degrees, able to address the parent as a whole person, responding to them in a dialogue form, taking cues from what the parents had said and making links to their lifeworlds. For instance, in responding to many parents’ wish to live a natural life, one student creatively reminds them of the possibility of other unnatural medical interventions if they contract a vaccine-preventable disease. Other students, realizing how important ‘natural’ life is for the parents, reminded them that vaccines stimulate the body’s natural reactions: Parent: I want to live as natural life as possible. How does ‘natural’ relate to vaccination? Student: Of course, there haven’t been vaccines from the beginning of times, so they may seem unnatural. However, [. . .] during illness, you may need to undergo complicated drug treatments and operations that are inherently unnatural, but they may save your life. Thus, preventing the illness with vaccines is smart.
Some parents’ questions involved strong metaphors, such as fighting a war against one’s own body. Several students (n = 5) acknowledged this parent-used rhetoric, and the student connected it to the body’s natural functioning, tried to replace it with a milder expression, or elicited more information what the parent meant: Parent: Do I have to fight a war against my own body to save others? S1: Our system runs ‘war’ all the time against various pathogens. Vaccination, therefore, seeks to help one’s own body to ‘war’ against fully-functioning pathogens. S2: War is a bit heavy term. In the end, vaccines merely cause a kind of a memory trace in your body. S3: Would you like to tell me why taking vaccines feels like war against your own body?
Some students generated dialogue by presenting counter questions (n = 3). This was often done in a combination with other strategies, such as advocating for the child, a persuasion strategy used to represent the child’s viewpoint (n = 3): Parent: Doesn’t my child have the right to go through children’s infectious diseases? These support mental and physical development. S1: The child is unable to take a stand on the vaccines she has received, and because many of the vaccine-preventable diseases are life-threatening or even lethal, I think it is justified to see the well-being of the child first. S2: [. . .] Who decides what diseases your child really wants to go through?
Voice of medicine
Few students (n = 2) answered the parent with only science-based information about vaccines and infectious diseases. These answers were written in passive voice, instead of addressing the parent as ‘You’ or the doctor as ‘I’. Such answers do not function as an invitation for a dialogue but instead appear as a medical monologue channelled through the physician’s mouth. In fact, these answers could have been copy-pasted from another information source (and likely were). Thus, the student here represents exclusively the voice of medicine. In these dialogues, the student does not even form an ‘I-It’ relationship (non-ideal). Instead, they create an even worse doctor-patient relationship of ‘It-It’, the ‘voice of medicine’ talking to a ‘medical condition’.
The answer below entirely ignores the parent’s question about the child’s right to a disease and its perceived benefits and makes a top-down commentary, leaving little space to continue the dialogue: Student: It is unnecessary for a child to suffer a disease, against which the national vaccination programme has an effective, free vaccine that is found safe. The vaccine will provide protection against the disease, which can have dangerous complications. However, the parent is entitled to refuse to take the vaccine for the child.
Ignoring professionalism
One of the students responded to the parents’ concerns and questions with disrespecting sarcasm. Although this student was the only one in the writing exercise purposefully restraining from professionalism, in the group discussion, few others expressed understanding for physicians who take their frustration out on patients. The excerpt below shows a response to a parent’s wish to live a ‘natural’ life: Student: Sure, one can live in the Stone Age if they want to. Life expectancy in the Stone Age was about 20 years.
Discussion
This pilot study explores a video case and a subsequent group discussion, and a writing exercise, as a means to expand the students’ understanding of health beliefs behind vaccine hesitancy, and stimulate the students’ ability to encounter the parents as whole persons. Most students respond differently to vaccine hesitancy in the classroom than in their written homework. Given all the perspectives and modes of communicating, the group discussion seems to function as a hospital breakroom, in which the physicians can momentarily drop the professional role and share their thoughts and experiences as a ‘whole person’. Such discussions allow the thinking and emotions that are not intended to be expressed in the patient encounter, no matter how valuable these may be for other reasons. The notion of ‘hospital breakroom’ is here used as a metaphor for a peer-to-peer debriefing environment, as most of the immunization consultations take place in primary care settings instead of a hospital. In those settings, the ‘whole person’ debriefing may take place in hallways, during lunch, or in between the patients in the consultation room.
Aside from the emotional reactions towards the non-compliant parents, the group discussions unveiled that some students have doubts about the necessity of certain vaccines, about how the governmental decides which vaccines are made and about the role of the pharmaceutical industry. Thus, such students share concerns with the vaccine-hesitant parents and may not be able to gain the parents’ trust due to their own ambivalence about certain aspects of vaccines. Medical educators should not assume that students adopt the ‘voice of medicine’ about vaccines uncritically without addressing their own concerns and making the underlying power relations transparent. In this regard, the group discussion has an important function in allowing a peer-to-peer conversation, where personal thoughts and emotions can be expressed more freely, simulating future hospital breakroom discussions with colleagues. This project, however, identifies a need for further studies of how the students’ attitudes and beliefs about vaccines develop during their educational trajectory.
In the writing exercise, the students are invited to form an ‘I-You’ relationship between themselves as a junior doctor and a vaccine-hesitant parent from the video case. This exercise simulates a face-to-face patient encounter, inviting the student to imagine the parent is sitting in the consultation room with them. Several students elicited the parents’ concerns through counter questions, which is considered a helpful strategy for addressing vaccine hesitancy. 6 However, according to the criteria used in this study, which is the engagement in a humane ‘I-You’ health care dialogue and the acknowledgement of the parents’ concerns in their lifeworld, 3 out of the 9 students failed. They either ignored the patient as a whole person or their own professional role, or both. There may be several reasons for restraining from the invited dialogue form and ignoring the parents’ lifeworld. For instance, the students feel insecure when addressing an assertive parent directly, feeling it would be too confrontational. In fact, existing in the ‘I-You’ relationship and entering the patient’s world can be much more uncomfortable than existing in the ‘I-It’ connection. 32 Furthermore, in the Finnish language, while the passive is relatively common, the hidden subject is used particularly when expressing something uncomfortable. 36 In addition, some students may associate an impersonal and science-focused style of communication with being professional, resulting in an ‘It-It’ relationship. Although conveying medical information is an essential part of vaccine communication, some physicians may not develop a broader communication repertoire. Many health care providers, in fact, operate primarily from such an analytical style, focusing on science-based facts and statistics, 37 whereas studies show that, in terms of vaccine refusal, merely providing more information is counterproductive. 6
One student demonstrated consistently sarcastic responses in a group as well as the written exercise. Although it may be unlikely that he would use such a communication mode in an actual encounter, his frustration seemed to prevent practicing professional behaviour. Such response is not an exception however. In fact, students have previously reported being challenged by their private emotional reactions, mostly anger, towards vaccine-hesitant parents. 38 Unfortunately, this cannot be solely blamed on the students’ immaturity and lack of clinical experience. As most parents shared experiences of frustrated and angry health care professionals, it seems a relevant concern that the caregivers are not able or willing to hide their negative reactions. Results in this study thus indicate a need for communication training with vaccine-hesitant parents, as well as discussions about the role of the patient’s lifeworld in clinical encounters. This is in line with studies identifying an ability to ‘listen to the patients’ health beliefs non-judgmentally’ as one of the necessary learning objectives in a suggested pre-service vaccinology curriculum. 39 Students would thus benefit from training that helps them to transition from the ‘hospital breakroom’ to the ‘consultation room’ and to find an appropriate balance between their personal and professional voices.
After completing the study sessions, the students were invited to share their experiences on this pilot in a short concluding conversation. Several students noted that the involvement of the actual vaccine-hesitant parents in the video case made the situation more authentic and made the students realize they are likely to encounter similar parents in the future. When asked how they had experienced the writing exercise, few students told specifically having imagined being a physician and restraining from expressing frustration or from using professional jargon. This had caused them think how to formulate their answers, knowing that ‘naturalness’, for instance, is an important issue for the parents.
Several aspects of this study have limitations and call for further development. One of the key weaknesses of the study is in its evaluation design: the intervention only compares the 2 learning modalities within with each other but does not involve a control group. The reason for this is that the study was a preliminary step needed to test a concept previously unfamiliar in medical education. The authors plan to conduct a more in-depth study with larger sample size and control groups. In terms of assessment, the written assignments were not marked, as the PBL modules do not include marking in the Tampere medical school. In fact, in this initial pilot phase of the study, it was considered relevant to gather authentic responses to design possible further development and assessment criteria for the exercise, instead of the students thinking of what would be desirable answers. Ideally, the study would have proceeded with a group reflection on the students’ written answers. The authors intend to send a follow-up email with a selection of anonymous answers and a short feedback for the tutor group.
As the study surprisingly identifies some gaps in students’ confidence in vaccines, the authors will include these findings in the discussion about the prevention curriculum development. The vaccine hesitation study was organized at the beginning of an integrated study unit ‘Prevention’ where vaccinations are one of the main objectives. The hesitation study was organized during the first week of the unit at the same time when the students were initiating their studies on vaccination. Therefore, they at this point did not present full professional knowledge on the issues. Some of them also did not have critical attitude towards false beliefs presented by some parents. In future research, one consideration is to place the processing of vaccine hesitancy challenges at the end of the integrated unit. One of the lessons learned relates thus to the placement of the vaccine hesitancy intervention. The placement of intervention at the beginning of the ‘Prevention’ unit might not have been ideal. The authors, however, argue that one can only know this by trying it out. It is also clear that this topic should be present also at the end clinical stage of the curriculum and in the specialization programme for general medicine and pediatrics.
There are no easy answers to the challenge that vaccine hesitancy presents to the medical education at all levels. It is important to provide the students with opportunities to encounter opinions that they might experience as intellectually dissatisfying and harmful to the patient and the society. The students should have diverse possibilities to practice dialogue in such instances knowing that the results might more often than not be disappointing. This study aims to offer one alternative for that purpose. The authors speculate that when developing the exercise and its assessment further, an approach that combines the above-mentioned communication skills with clinical aspects of immunization may be the most appropriate for primary care training, instead of focusing merely on one or the other.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study is part of Kaisu Koski’s Academy Research Fellow project, Video scenarios in medical education: Polyphony and non-linearity in audio-visual doctor-patient narratives, funded by the Academy of Finland 2015-2020 (decision number 285118). The film Conversations with vaccine-critical parents was completed as part of the International Collaboration for Capitalizing on Cost-Effective and Life-Saving Commodities (i4C), which is funded through the Research Council of Norway’s Global Health & Vaccination Program (GLOBVAC Project #234608). The Medical Education Ethics Committee in the Faculty of Medicine and Life Sciences in University of Tampere approved this study. The video link can be requested for educational purposes:
Author Contributions
KK conceived and designed the intervention and planned it with KH. KK conducted the intervention with JTL. All authors discussed the results. KK wrote the manuscript with support from JTL and KH.