
Abstract
Background
Shame is an emotional experience in health professions education, often contributing to burnout, isolation, and threats to professional identity. Self-compassion has been identified as a protective factor against shame. This study describes the development and evaluation of an elective designed to foster shame resilience and cultivate self-compassion among health professions students.
Methods
A 6-h elective, Fostering Connection and Shame Resilience Through Self-Compassion, was offered over 3 monthly 2-h sessions. Each session included a shared meal, abbreviated large-group conceptual learning, reflective writing, guided self-compassion practices, and small-group discussions. Participants completed the Self-Compassion Scale-Short Form (SCS-SF) at the beginning and end of the course and the Shame Frequency Questionnaire in Medical Students (SFQ-MS) at the end. A control group of nonparticipating medical students completed the SFQ-MS for comparison. An anonymous program evaluation survey was also conducted.
Results
Of 21 learners who completed both pre and post SCS-SF scales, statistically significant improvements were observed in 7 of 12 items and in 4 of 6 subscales (Self-Kindness, Self-Judgment, Common Humanity, and Mindfulness). The total self-compassion score increased from mild to moderate. On the SFQ-MS, 6 of 12 items showed statistically significant differences between the postelective group and matched controls. Program evaluation data indicated that 62% reported significantly greater awareness of shame, and 57% reported significantly increased openness to practicing self-compassion.
Conclusions
This elective represents an innovative approach to improving emotional resilience in learners, integrating experiential learning, interpersonal connection, and small-group learning. Findings suggest that even brief interventions can positively impact learners’ self-compassion and aspects of shame resilience. Curricula addressing these affective domains may offer valuable tools for enhancing well-being and professional identity formation in health professions education.
Keywords
Introduction
The trajectory of health professions education is inherently tied to lifelong learning, characterized not only by successes but also by exposure to failures and setbacks. In such challenging moments, shame—an often-unspoken, yet deeply influential emotion—can surface and significantly affect professional development. Shame, broadly defined as the feeling of being fundamentally flawed or deficient in the eyes of others, can intensify in the high-pressure, perfectionistic culture of healthcare training environments. 1 When left unaddressed, shame can hinder personal growth, disrupt professional relationships, and contribute to deleterious outcomes such as impaired empathy, social isolation, and burnout. 2 Encompassing emotional exhaustion, depersonalization, and reduced personal accomplishment, burnout remains a pressing concern within medical education, with evidence suggesting a link to experiences of shame. According to the 2025 Association of American Medical Colleges Medical School Graduation Questionnaire, 3 19.6% of graduates reported being publicly humiliated, and 36.9% reported being publicly embarrassed during medical school. Such experiences can foster internalized beliefs of inadequacy and isolation, undermining learners’ sense of belonging and professional identity, and may catalyze experiences of shame. 4 In our health professions journey, we are equipped with knowledge and tools to help others, but how do we heal ourselves? How do we move out of isolation and toward connection with others, learn emotional resilience, and constructively engage with an experience of shame in medical education?
Self-compassion, according to Dr Kristin Neff, is defined as Self-Kindness, Mindfulness, and recognition of Common Humanity.5,6 Emerging research supports self-compassion as a critical protective factor against the corrosive effects of self-conscious emotions such as shame. Self-compassion is associated with lower levels of shame and greater psychological resilience. 7 In high-pressure environments like healthcare, self-compassion can offer an internal mechanism for emotional regulation, enabling individuals to respond to our perceived failures with understanding and self-kindness rather than harsh self-criticism. 8 Self-care strategies, predominantly utilized outside of the clinical environment, such as exercise or creative pursuits, can be important for wellness. The benefit of self-compassion is that it offers immediate, on-the-job emotional support in moments of stress. Prior interventions aimed at fostering self-compassion among healthcare professionals have demonstrated reductions in burnout and secondary traumatic stress, along with increases in compassion satisfaction and job satisfaction. 9
Previously published interventions for addressing the experience of shame in medical students include structured educational seminars on shame resilience, 10 and courses with individual reflection. 11 Shame is an emotional experience that has also been reported among students in other health professions, including nursing. 12 Shame related to mental health concerns and self-compassion have been identified as key determinants of well-being among students in nursing, occupational therapy, social work, and counseling. Of note, self-compassion has emerged as the strongest predictor of overall mental health in this group of healthcare students. 13 However, interventions specifically employing self-compassion practices for constructively engaging in experiences of shame in health professions education have not been published.
This paper describes the development, implementation, and evaluation of a novel elective designed to equip healthcare trainees with the skills to recognize challenging emotions such as shame and engage in self-compassionate responses. This work offers an innovative educational model and provides a curricular experience that promotes not only knowledge acquisition, but also the development of reflective skills and emotional resilience. This study was completed to explore the following question: How does learning about the ways shame manifests throughout the health professions journey, engaging in small-group dialogue about these experiences, and applying evidence-based self-compassion practices influence health professions learners’ reported frequency of shame and levels of self-compassion?
Materials and Methods
Elective Overview
We developed a voluntary elective titled “Fostering Connection and Shame Resilience Through Self-Compassion” for health professions learners, aimed at equipping students with language and strategies to address difficult emotions encountered in the learning environment, particularly shame. The elective also sought to build students’ confidence and skill in practicing self-compassion, an evidence-based tool for emotional resilience.
This educational initiative was supported by a Josiah Macy Jr. Foundation President's Grant. The elective was structured as a 6-hour experience, divided into three 2-hour sessions occurring once monthly over a 3-month period beginning January 2025 and ending March 2025. This format was intentionally chosen to allow learners sufficient time between sessions to practice the exercises introduced. Based on the understanding that self-compassion can be strengthened through practice, the elective emphasized actionable skills that could be utilized both within preclinical and clinical environments and in personal contexts.
Participant Selection
Learners from various health professions within the UTHealth Houston system were invited to participate in the elective. Recruitment targeted students from the John P. and Kathrine G. McGovern Medical School, the UTHealth Houston Cizik School of Nursing, and the UTHealth Houston School of Dentistry. Outreach efforts included email invitations with flyers sent to school leadership for distribution, physical flyers posted around campus buildings associated with the 3 schools, and promotion through the McGovern Center for Humanities and Ethics webpage.
Participation in the elective was voluntary and not a requirement for any academic program. Consequently, the participant pool consisted of self-selected students who demonstrated an interest in dedicating additional time outside of the formal curriculum to engage with the concepts presented in the course. Participants were recruited from learners across health professions at UTHealth Houston. There were no exclusion criteria; all interested learners were eligible to participate.
Educational Content and Delivery
Each session of the elective was structured into 3 components: a dinner, a large-group didactic portion, and small-group discussions. A comprehensive outline of the structure and content for all 3 elective sessions is provided as a Facilitator Guide for Course Content (Supplemental Material 1). In addition to over a decade of personal study and practice in mindfulness, compassion, and self-compassion, the authors (RM and GM) have collectively completed a 2-year Mindfulness Meditation Teacher Certification Program, engaged in more than 360 hours of formal training, and delivered presentations on this domain at the local, national, and international levels. For all 3 sessions of the elective, the full content of the course as intended was taught by these 2 authors, who drew on their sustained personal practice and structured training to create an educational experience grounded in both evidence-based frameworks and lived understanding. The majority of the learners did not interact with the teachers outside of the course.
Dinner and Informal Connection
Each session began with a 30-min dinner, providing participants with an opportunity to connect and get to know one another in an informal setting. This approach aimed to foster a sense of community and increase comfort levels, thereby encouraging openness during subsequent small-group discussions.
Large-Group Didactic Sessions
Following dinner, the large-group sessions introduced conceptual frameworks related to shame, self-compassion, and resilience. The selected content on shame explored the various stages of a health professions learners’ journey where this complex emotion may emerge. As outlined in the facilitator guide, content addressed how shame can manifest during both preclinical and clinical training and may continue to influence individuals beyond graduation and into professional practice.
Learners engaged in experiential exercises such as reflective writing and guided self-compassion practices. These practices included audio exercises sourced from publicly available resources curated by Dr Kristin Neff (available at: https://self-compassion.org/self-compassion-practices/, accessed March 2025). 14
Emphasis was placed on informal, accessible self-compassion practices that could be utilized at the point of care. For example, practices such as placing a hand over one's heart and offering supportive inner dialogue through general self-compassion phrases were highlighted. This approach aligns with findings from a study by Neff et al, demonstrating that both formal meditation and informal self-compassion practices significantly contribute to increased self-compassion levels among participants. 8
Small-Group Discussions
After the didactic portion, students participated in small-group discussions facilitated by faculty familiar with the concepts discussed. These discussions provided a confidential environment for learners to reflect on how the session content related to their personal experiences and to foster connection via peer and faculty support. For each session, 5 discussion prompts were developed to encourage active engagement and meaningful dialogue. This format was intentionally chosen based on the observation that learners often feel more at ease discussing sensitive topics in smaller, more intimate groups.
Venue
The elective sessions were held on-campus in 2 large classrooms of the Texas Medical Center Library, providing a central location with an environment conducive for both large-group instruction and small-group interactions. The overall aim was to normalize shame-related conversations within healthcare training environments and to instill confidence in learners to respond empathically not only to others but also to themselves when encountering distress, feelings of inadequacy, or professional challenges.
Study Design
We developed a study protocol to assess the impact of the elective on learners’ self-compassion and to elucidate potential impact on learners’ experiences of shame. To protect participants’ identity, all responses were gathered anonymously via surveys completed on the QuestionPro platform and accessed through QR codes distributed to participants. All data gathered through surveys were fully anonymized to ensure the confidentiality and privacy of participants. All participants provided written consent by responding “Yes” to the first item of every survey: “I consent to participate in this survey voluntarily. I understand that my responses will remain anonymous and that I may withdraw at any time before submitting the survey.” Selecting “Yes” allowed participants to proceed, ensuring informed and voluntary participation. Institutional Review Board approval was provided by the Committee for the Protection of Human Subjects at UTHealth Houston (IRB # HSC-MS-24-1245).
To evaluate changes in self-compassion, participants completed the 12-item Self-Compassion Scale-Short Form (SCS-SF) 15 at the beginning and end of the elective. The SCS-SF is a simple, reliable, validated tool that is practical and has been used by researchers and clinicians to understand how persons respond to struggles. The SCS-SF assesses 6 components of self-compassion: Self-Kindness, Self-Judgment, Common Humanity, Isolation, Mindfulness, and Over-Identification (Supplemental material 2). Each item was rated on a 5-point Likert scale ranging from 1 (“Almost Never”) to 5 (“Almost Always”). Following the scoring guidelines by Neff et al, 16 items within the negatively worded subscales (Self-Judgment, Isolation, and Over-Identification) were reverse scored. Subscale means were then calculated, and a total self-compassion mean was obtained by averaging the 6 subscale means.
This study also aimed to identify the impact of the elective on health professions learners’ experiences of shame. The Shame Frequency Questionnaire in Medical Students (SFQ-MS), 17 a validated 12-item instrument developed by Bynum et al, was employed to assess the frequency of shame experiences among participants. The SFQ-MS was selected for its applicability across different educational contexts (eg, preclinical and clinical settings) and has been reported to be a psychometrically robust instrument. 17 Importantly, this tool was designed specifically to assess experiences of shame within medical education. The SFQ-MS was completed by the participants at the conclusion of the elective through an anonymous QuestionPro survey.
This design allowed for the assessment of the elective's effectiveness in reducing the reported frequency of shame among health professions students, providing insights into the potential benefits of incorporating self-compassion training into medical education curricula. Control group participants were recruited via an email invitation sent to medical students who were not enrolled in the elective. Students in the control group were matched to elective participants based on academic year to enhance comparability. Both the elective participants and the control group completed the same SFQ-MS, allowing for comparison of reported shame experiences between groups.
This study conformed to the DoCTRINE Guidelines 18 for reporting educational innovations in curriculum development found in the EQUATOR network. See Supplemental material 4 for the completed DoCTRINE Guidelines checklist.
Program Evaluation
In addition to completing the SCS-SF and the SFQ-MS, students in the elective were invited to complete an additional anonymous program evaluation survey. The full list of program evaluation survey questions used for analysis is available for review (Supplemental material 3). Utilizing a 5-point scale, participants were asked to characterize the impact of the elective on their awareness and understanding shame and how it influenced their ability to handle experiences of shame in their health professions journey in a constructive way, rather than letting them become debilitating. Additionally, they were asked how their openness to practicing self-compassion in challenging situations evolved after participating in this elective.
Statistical Analysis
Responses from the SCS-SF were analyzed to assess changes between pre- and postcourse surveys. For the self-compassion data, pre- and postscores of each item of the scale were evaluated. Additionally, mean scores were calculated for each of the 6 subscales, and an overall self-compassion score was computed by averaging these subscale means. As individual pre- and posttest responses could not be linked due to the anonymous nature of the surveys, a 1-way analysis of variance (ANOVA) was conducted to determine whether there were statistically significant differences in self-compassion scores before and after the intervention. All statistical analyses were performed using IBM SPSS. Descriptive statistics were used to summarize scores from the SCS-SF.
The SFQ-MS, as published, was originally presented on a 6-point scale (1 = never, 2 = once a month or less, 3 = a few times a month, 4 = once a week, 5 = a few times a week, 6 = nearly every day). As “never” on the scale would typically result in a score of 12 if “never” were selected on all 12 items, the SFQ-MS author agreed and recommended that use of the scale involve changing “never” to zero and renumbering the remaining item responses 1 to 5 (Bynum WE, MD, personal communication, March 2025). 19 As such, the data presented here for the post and control samples uses the revised point values on a 5-point scale (0 = never, 1 = once a month or less, 2 = a few times a month, 3 = once a week, 4 = a few times a week, 5 = nearly every day). The participants’ scores were compared to those of a control group comprised of medical students who did not participate in the elective. The control group was matched based on their academic year. Statistical analyses were conducted to determine any significant differences in shame frequency between the 2 groups. For the SFQ-MS data, a 1-way ANOVA was conducted to determine whether statistically significant differences in shame frequency were present between the posttest and the control group both for individual items of the questionnaire and total mean scores. Significance was set at the .05 standard alpha level. Equal variances were assumed based on the homogeneity of variance tests. Effect sizes are presented as epsilon-squared to control for positive bias.
Results
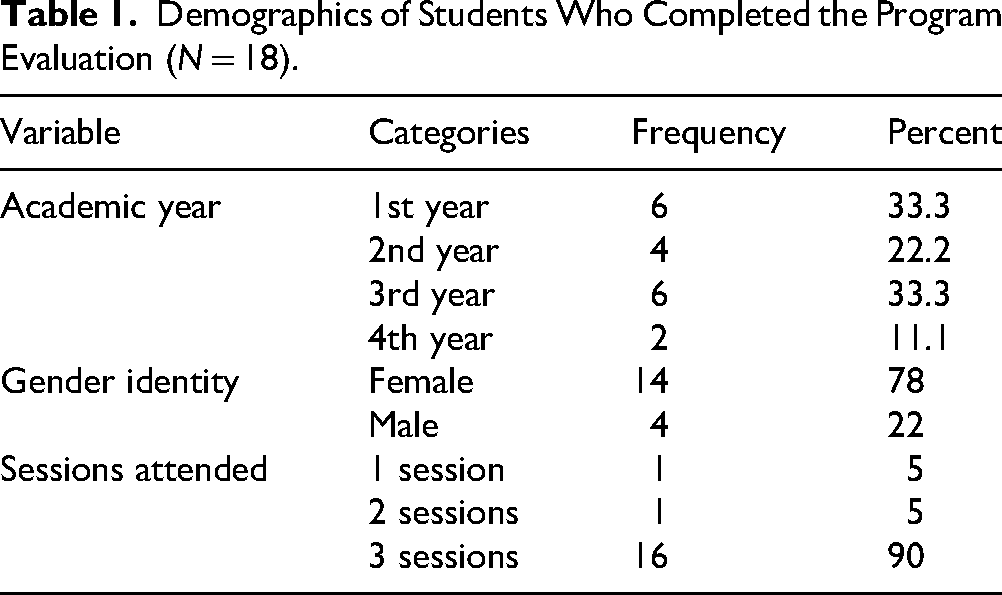
A total of 24 medical students enrolled in the course and 18 students completed the voluntary, anonymous program evaluation survey (75%). A total of 6 faculty facilitated small-group discussion in the elective, with representatives from the medical school (n = 5) and the nursing school (n = 1). Demographics for the 18 participants who agreed to complete the program evaluation are summarized in Table 1. Ninety percent of the participants attended all 3 sessions of the elective with the majority identifying as female.
Demographics of Students Who Completed the Program Evaluation (N = 18).
For the SCS-SF, 23 students completed the voluntary pretest, and 21 completed the voluntary posttest. Of these 21 students with time 1 and time 2 data, 16 completed all 3 sessions of the course. Statistically significant mean scores by individual items are summarized in Table 2. Results of the self-compassion analysis revealed statistically significant improvements in 7 of the 12 items of the SCS.
Pre- and Post-Self-Compassion Scale Scores by Item.

Analysis of SCS-SF subscales revealed statistically significant improvements in 4 of the 6 subscales: Self-Kindness, Self-Judgment, Common Humanity, and Mindfulness. Prior to the elective, the group's total mean self-compassion score was low and increased to moderate after the conclusion of the elective, according to a rubric created by Neff et al (Table 3). 16 These findings suggest that the intervention had a positive impact on participants’ self-compassion, as evidenced by significant improvements in several aspects of self-compassion as measured by the SCS-SF.
Mean Pre- and Posttest for Self-Compassion Subscales a .

The negative subscales Self-judgment, Isolation, and Over-identification were reverse-scored, such that higher postscores reflect lower levels of these negative traits. Consequently, an increase in mean scores from pre to postassessment indicates a positive change in the final self-compassion score.
For analysis of the SFQ-MS, the postelective group consisted of 19 students that completed the voluntary shame survey at the end of the course and the control group consisted of 25 students who had not received any instruction. Comparison of the SFQ-MS item-level and total means between the post and the control groups indicates statistically significant mean differences between the 2 groups on 6 of the 12 items, though not the total sample means (Table 4).
Mean Posttest and Control Group Scores on the Shame Frequency Questionnaire-Medical Students.

For the program evaluation, 61% of the participants indicated that they had a significant increase in their awareness and understanding of shame (Figure 1). In answer to the question, “How has your openness to practicing self-compassion in challenging situations evolved after participating in this elective,” 56% of the participants endorsed significant improvements (Figure 2). Among the participants who completed the program evaluation, 100% reported that the elective made a moderate or significant contribution to their personal and professional development (Figure 3). Furthermore, 57% of respondents indicated they were “extremely likely” to recommend the elective to their peers, suggesting a high level of perceived value and relevance.
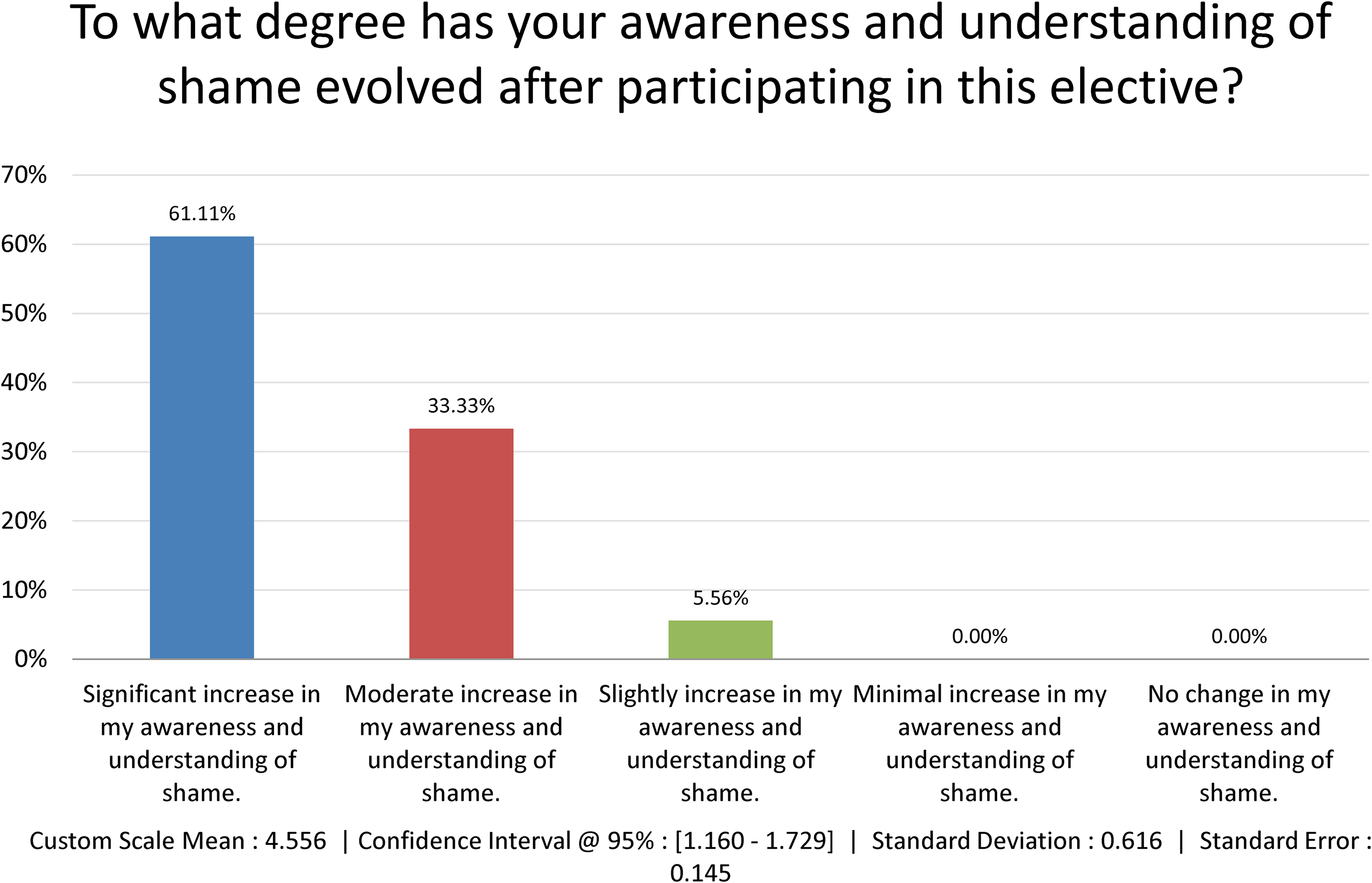
Program evaluation question: degree to which participants’ understanding of shame changed.

Program evaluation question: degree to which participants’ openness to practicing self-compassion changed.

Program evaluation question: degree to which the elective contributed to participants’ personal and professional growth.
Discussion
Prior interventions have explored shame resilience and used reflective approaches to navigate this complex emotion in medical education. Studies in other health professions show that shame and self-compassion can influence learner well-being, with self-compassion being a strong predictor of mental health. Educational interventions that specifically integrate self-compassion practices to address shame within health professions training have not yet been described.
This elective represents an innovative curricular design that integrates elements often overlooked in traditional health professions education: intentional connection-building, concise didactic teaching in large groups, reflective writing, and small-group dialogue. These components were purposefully selected to foster both cognitive engagement and emotional safety, concepts that are particularly important when addressing potentially vulnerable topics such as shame and self-compassion.
In contrast to conventional large-group, lecture-heavy formats, our elective emphasized relational connection from the outset. Beginning each session with a shared dinner created a communal atmosphere, helping to lower social barriers and build trust among participants. While providing a meal may not always be feasible, similar outcomes could be achieved through low-barrier strategies such as structured icebreakers, paired check-ins, or storytelling prompts. These connection points may be critical for allowing participants to feel psychologically safe before engaging in emotionally vulnerable discussions.
Time devoted to small-group dialogue emerged as a key strength of the elective. These sessions provided a safe space for participants to explore the potentially triggering topics of shame and self-compassion. Although no mental health professionals were involved, faculty facilitators with training in supporting sensitive discussions modeled courage by sharing their own vulnerable experiences with shame. This openness helped normalize shared challenges and reduce isolation among learners. The findings of this study align with those of Bynum et al, 10 in which speakers’ vulnerability and sharing of their own shame experiences were central to fostering psychological safety and meaningful small-group engagement.
The results of the SCS-SF analysis offer evidence that the elective had a positive effect on learners’ self-compassion. Statistically significant improvements were observed in 7 of the 12 items and in 4 of the 6 core subscales of the SCS-SF, namely, Self-Kindness, Self-Judgment, Common Humanity, and Mindfulness. These domains represent essential capacities for emotional regulation and resilience, particularly in the high-pressure contexts of clinical training. Of note, the group's average total score shifted from the low to the moderate range by the end of the elective, suggesting meaningful growth in self-compassion. These findings suggest that self-compassion can be taught and cultivated through brief, structured interventions, even within the constraints of a busy health professions curriculum. The findings in this study are consistent with prior research in which participants of a 3-day compassion-focused therapy workshop for healthcare professionals such as nurses and counselors demonstrated increased self-compassion and reduced self-critical judgment after brief training. 20 This shift is potentially relevant given that even modest increases in self-compassion have been linked to reductions in stress, burnout, and self-criticism in prior studies of healthcare professionals.8,9 Nearly all students who completed the posttest had attended all 3 sessions, highlighting the importance of sustained participation in reinforcing these skills.
In examining shame resilience, although the total mean scores on the SFQ-MS did not demonstrate a statistically significant difference between the elective and control groups, item-level analysis revealed statistically significant differences on 6 of the 12 items. These findings highlight the complexity of measuring affective and identity-related concepts such as shame. Of note, the items showing change reflect deeply internalized beliefs such as perceived professional adequacy, professional belonging, and fitness to practice. The presence of item-level differences, even in the absence of a total score change, suggests that targeted educational interventions may meaningfully shift learners’ self-perceptions in ways that are subtle yet significant, particularly in domains related to self-worth and professional identity.
Participants were not formally encouraged to engage in structured training outside the scheduled 3 sessions. However, given the self-motivated nature of the group to pursue learning in these topics, it is possible that some students chose to explore additional materials beyond the scope of the program. Learning about these concepts and increasing their awareness may have prompted some to further reflect on their experiences of shame and to apply self-compassion in navigating challenges along their health professions journey. This self-directed engagement would be viewed as a positive and welcomed impact.
A unique component of the elective was the inclusion of reflective writing, completed with pen and paper, in each session. In an era where much of medical education is screen-based and performance-driven, students rarely have opportunities to write for self-reflection. Narrative writing helped slow down the learning process, encouraged introspection, and offered a nonevaluative space for emotional processing.
This educational intervention offers a novel model for assessing the development of key professional competencies such as emotional awareness, self-compassion, and shame resilience. The domains may be underrepresented in traditional evaluations of medical education. By integrating qualitative feedback and validated tools like the SCS-SF and the SFQ-MS, this study captures shifts not only in learners’ knowledge but also in their attitudes toward themselves and their peers. The elective supports individualized learning and professional identity formation through structured self-reflection, group dialogue, and psychological safety. In this way, the curriculum demonstrates a practical and innovative approach to evaluating affective and interpersonal dimensions of health professions education.
Despite our intention to recruit a broad sample of health professions learners, the participant pool was comprised entirely of medical students. Recruitment efforts included emails to leadership at the nursing and dental schools, and placement of printed flyers in high-traffic areas across all 3 schools. Attendance from nursing and dental students was not achieved, but valuable lessons were learned. This highlights some of the ongoing challenges in fostering interprofessional engagement and breaking down the silos that persist within health professions education. To support more equitable participation in future iterations of the elective, more deliberate strategies may be needed such as inviting student ambassadors from each school to help promote the elective, offering information sessions to explain its interdisciplinary relevance, or co-developing sessions with faculty from other health professions schools. Integrating the elective more formally into cocurricular pathways or interprofessional education initiatives could also enhance its visibility and perceived value across programs. Addressing these barriers is essential if we aim to create learning environments that support well-being and resilience across the full spectrum of healthcare professions.
Conclusions
Taken together, the innovative structure of the elective, including brief large-group didactic sessions, handwritten reflective exercise, informal self-compassion practices, and small-group dialogue, represents a promising pedagogical model for engaging learners around emotional resilience and professional identity formation. The findings of this study suggest that even brief interventions can positively impact learners’ self-compassion and aspects of shame resilience. This elective demonstrates a feasible approach for integrating affective and relational competencies, such as shame resilience and self-compassion, into health professions curricula.
Limitations
This study did not include an a priori sample size calculation because participation in the elective workshop was voluntary. Consequently, the sample consisted of self-selected students who demonstrated an interest in dedicating additional time outside the formal curriculum to engage with the concepts presented in the course. This self-selection may limit generalizability and introduce selection bias.
The absence of a pretest SFQ-MS limited comparability of the posttest within the same group of participants. This was partially addressed by including a control sample that did not receive the elective course instruction. In this way, the control functioned like a pretest measure as would have been administered prior to course instruction.
Future Directions
With this investigation functioning as a proof of concept to educate, train, and foster new skill development in a sample of health professions students, the outcomes of this study align properly with the study design. However, now with this supporting evidence in place, a few improved processes and approaches can be considered for future investigations of this type.
Future efforts could focus on expanding interprofessional participation, exploring long-term impacts on learner well-being and professional identity, and further refining curricular strategies to support emotional growth alongside clinical competence.
Given the success of the course instruction in both improving self-compassion and reducing shame frequency through abbreviated large-group didactic intervention and ample time for small-group discussion, this could serve as a model for replication at a larger level and in different educational settings, such as graduate medical education. For instance, the number of courses could be increased, as could the number of sessions by expanding the content. As discussed in the limitations, the numbers of participants could also be increased for improved power to detect a statistically significant effect.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205261420679 - Supplemental material for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners
Supplemental material, sj-pdf-1-mde-10.1177_23821205261420679 for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners by Gioconda Mojica, Peggy Hsieh, Andrew J. Revell and Rex Marco in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205261420679 - Supplemental material for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners
Supplemental material, sj-pdf-2-mde-10.1177_23821205261420679 for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners by Gioconda Mojica, Peggy Hsieh, Andrew J. Revell and Rex Marco in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205261420679 - Supplemental material for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners
Supplemental material, sj-docx-3-mde-10.1177_23821205261420679 for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners by Gioconda Mojica, Peggy Hsieh, Andrew J. Revell and Rex Marco in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205261420679 - Supplemental material for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners
Supplemental material, sj-docx-4-mde-10.1177_23821205261420679 for Fostering Connection and Shame Resilience Through Self-Compassion: An Innovative Elective for Health Professions Learners by Gioconda Mojica, Peggy Hsieh, Andrew J. Revell and Rex Marco in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
Generative AI was not utilized for any portion of this submission.
Ethical Considerations
The study received approval from the Institutional Review Board (IRB) at UTHealth Houston and was determined to qualify for exempt status (HSC-MS-24-1245).
Consent to Participate
Written consent was obtained through the first item of every survey, which required participants to agree before proceeding.
Author Contributions
The authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge and express gratitude for the Josiah Macy Jr. Foundation for its generous support of this educational initiative via a President's Grant (P25-11). The views expressed in this article are of the authors’ and not an official position of the institution or funder.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.