
Abstract
Problem:
Medical school curriculum continues to search for methods to develop a conceptual educational framework that promotes the storage, retrieval, transfer, and application of basic science to the human experience. To achieve this goal, we propose a metacognitive approach that integrates basic science with the humanistic and health system aspects of medical education.
Intervention:
During the week, via problem-based learning and lectures, first-year medical students were taught the basic science underlying a disease. Each Friday, a patient with the disease spoke to the class. Students then wrote illness scripts, which required them to metacognitively reflect not only on disease pathophysiology, complications, and treatments but also on the humanistic and health system issues revealed during the patient encounter. Evaluation of the intervention was conducted by measuring results on course exams and national board exams and analyzing free responses on the illness scripts and student course feedback. The course exams and National Board of Medical Examiners questions were divided into 3 categories: content covered in lecture, problem-based learning, or patient + illness script. Comparisons were made using Student t-test. Free responses were inductively analyzed using grounded theory methodology.
Context:
This curricular intervention was implemented during the first 13-week basic science course of medical school. The main objective of the course, Scientific Principles of Medicine, is to lay the scientific foundation for subsequent organ system courses. A total of 150 students were enrolled each year. We evaluated this intervention over 2 years, totaling 300 students.
Outcome:
Students scored significantly higher on illness script content compared to lecture content on the course exams (mean difference = 11.1, P = .006) and national board exams given in December (mean difference = 21.8, P = .0002) and June (mean difference = 12.7, P = .016). Themes extracted from students’ free responses included the following: relevance of basic science, humanistic themes of empathy, resilience, and the doctor-patient relationship, and systems themes of cost, barriers to care, and support systems.
Lessons learned:
A metacognitive approach to learning through the use of patient encounters and illness script reflections creates stronger conceptual frameworks for students to integrate, store, retain, and retrieve knowledge.
Introduction
Cognitive integration of basic science with clinical experience improves diagnostic reasoning. 1 An illness script is a schema by which clinicians integrate information to understand a clinical presentation and link formal knowledge with experiential clinical encounters. 2 Expert clinicians often depend on this method to make memory connections that aid in recognizing possible differential diagnoses.3,4 Medical students do not usually get this training until third year of medical school during clinical rotations. We propose that illness scripts can be used early in medical school training, in basic science courses. By linking science to the human experience, a metacognitive approach can reinforce conceptual scaffolding with personal, emotional connections.
The 4 main pillars of medical education at our institution are scientific knowledge, clinical practice, humanities, and health systems.5,6 Although the exact themes may vary between institutions, the challenge many medical schools face is finding an effective way to integrate similar themes into their curriculum.7,8 Although some courses may easily lend themselves to such integration, 9 other courses, for example those heavy in the basic sciences, find it difficult. Our research analyzes the use of illness scripts to integrate humanistic and health system issues in the basic science course, Scientific Principles of Medicine (SPM).
Illness scripts were first introduced into the medical literature by Professor Clancey 10 in the 1980s. These scripts were designed as an educational tool for clinical rotations. Students would describe a disease’s pathogenesis, presentation, diagnosis, and treatment and then correlate this information to a specific, real-life patient they observed during their rotation. Scripts are believed to facilitate information storage in long-term memory which can then be activated by trainees at subsequent encounters either on a test or in a clinical setting. 11 In other words, they guide student information selection, memorization, and interpretation. 12 The effectiveness of this tool is supported by today’s current medical educational theory, which suggests that students learn material through gists and schema rather than pure memorization of facts and figures. 13 Indeed, learning medicine in this manner prepares students to become expert clinicians 14 because medical diagnoses are an explanation and correlation of symptoms made on the basis of biomedical knowledge. 15 Integrating basic science with clinical sessions is felt to increase understanding and application of the scientific material. 16
The first objective of this article is to compare the understanding and retention of medical knowledge learned through the 3 educational methods used in the SPM class: lecture-based pedagogy, constructivist learning with problem-based learning (PBL), and the metacognitive approach with patient encounters and illness scripts. We used the results of the SPM midterm and final exams to represent short-term learning and the results of the standardized National Board of Medical Examiners (NBME) exam 3 and 8 months later to represent learning retention and retrieval.
The second objective of this article was to explore the ability of patient encounters and illness scripts to integrate clinical medicine, humanities, and health systems into a basic science course. Humanities and health systems education are crucial themes for a well-rounded medical education.17–19 Integrating these themes into a basic science course can be challenging. To address this problem, free response humanities and health system sections were added to the illness scripts. The free responses were inductively analyzed using grounded theory methodology.
Methods
The data used in this study were approved as part of the education research registry, which was approved by the College of Medicine Institutional Review Board (#STUDY00000123).
Each year from August through October, 150 first-year medical students take SPM, a basic science course whose main objective is to lay the scientific foundation for the subsequent organ system blocks. SPM is 13 weeks in duration. There is a formative midterm assessment and a summative final assessment composed of multiple-choice and short answer responses.
The SPM curriculum is organized by week. Each week covers 2 active-learning PBLs for 2 hours every Monday, Wednesday, and Friday. There are 2 hours of lecture each day from Monday through Thursday. On Friday, a 1-hour integration/review session with questions and answers is followed by a 1-hour patient encounter (Figure 1). The patient encounter is mandatory, it is not videotaped, students dress professionally and wear their white coats, computers are closed, note taking is discouraged, and listening and interacting is encouraged. The patients who speak have an illness that was discussed either in PBL or in lecture. For example, 1 week in PBL, students learned about the cystic fibrosis transmembrane regulator (CFTR) protein and sodium-chloride-water transport. On Friday, a patient with cystic fibrosis spoke to the class. An illness script regarding this encounter was due by Sunday evening. The illness script was formatted with the textbook version in column 1 and the patient version in column 2 (Figure 2). The categories addressed in each version were pathophysiology, presentation, diagnosis, treatment, humanistic take-away, and health systems issues.

Weekly SPM schedule template. PBL indicates problem-based learning; SPM, Scientific Principles of Medicine.

Example of illness script.
Patients had the following illnesses: celiac disease, cystic fibrosis, diabetes mellitus, multidrug-resistant infection, HIV, lynch syndrome, myasthenia gravis, osteogenesis imperfecta, glycogen storage disease, muscular dystrophy, and phenylketonuria. Often spouses, family, the patient’s physician, or nurse-coordinator accompanied the patient. The patient was given the opportunity to describe how they were diagnosed, the life adjustments that were required to live with their condition, and the issues that arose during treatment. Time was allotted for questions from the student audience.
The results of this study are presented in a sequential exploratory mixed-methods approach.
Qualitative data from 300 students over 2 years were acquired via written student illness scripts which included the free response sections addressing humanism and health systems and the end of the course student feedback. The scripts were evaluated with a thematic analysis approach. 20 Team members developed ideas about patterns and meanings. One team member developed a codebook by randomly selecting 15 representative illness scripts from each of the patient sessions over the 2 years and assigning codes to repetitive ideas. The team extrapolated from the literature that approximately 12 field interviews were sufficient to obtain data saturation. 21 ATLAS.ti 8.0 software was used to manage the data. Once verified, codes were grouped into themes according to similarities. Using the newly developed codebook, 2 other team members each independently coded sections of relevant text from the 15 random illness scripts. Updating and changing the codebook was done among the 3 members until consensus was achieved and theoretical saturation was reached.
Quantitative data was obtained over 2years from 300 students, 4 SPM exams, and 4 practice NBME exams. The SPM midterm and final exams were administered 6 and 13 weeks into the course, respectively. We considered the SPM exams a measurement of short-term memory. The exams were 60% multiple choice questions and 40% short answer responses. The NBME exams were administered in December, 2 months after the SPM course ended, and June, 8 months after SPM. We considered the NBME exams results to be an indicator of more long-term memory. The NBME exams were 100% multiple choice questions. Students took the NMBE exams as Step 1 practice, with no additional preparation.
A team member, blinded from exam question scores, identified the category of each exam question’s content. Each question on the SPM and NBME exams was selected into 1 of 3 categories based on where the content was taught during the SPM course: lecture only, PBL only, or patient + illness script. The SPM exam data are given as the class total correct cumulative points. The NBME data are given as the percentage of students who answered the question correctly. For statistical analysis, the lecture based questions served as the standard baseline. Averages were compared using a paired student’s t-test with significance defined as p<0.05. Mean differences compared to the lecture group were then calculated with a confidence interval set at 95%.
Results
Qualitative results revealed 7 main themes: patients make the basic science relevant, empathy and awareness, patient resilience, the doctor-patient relationship, cost of care, barriers to care, and support systems.Tables 1 to 3 outline the themes that were derived from the qualitative free response portion of the illness scripts matched with representative quotes.
Qualitative theme of relevance with representative quotes.

Abbreviation: PKU, phenylketonuria.
Qualitative humanities themes with representative quotes.
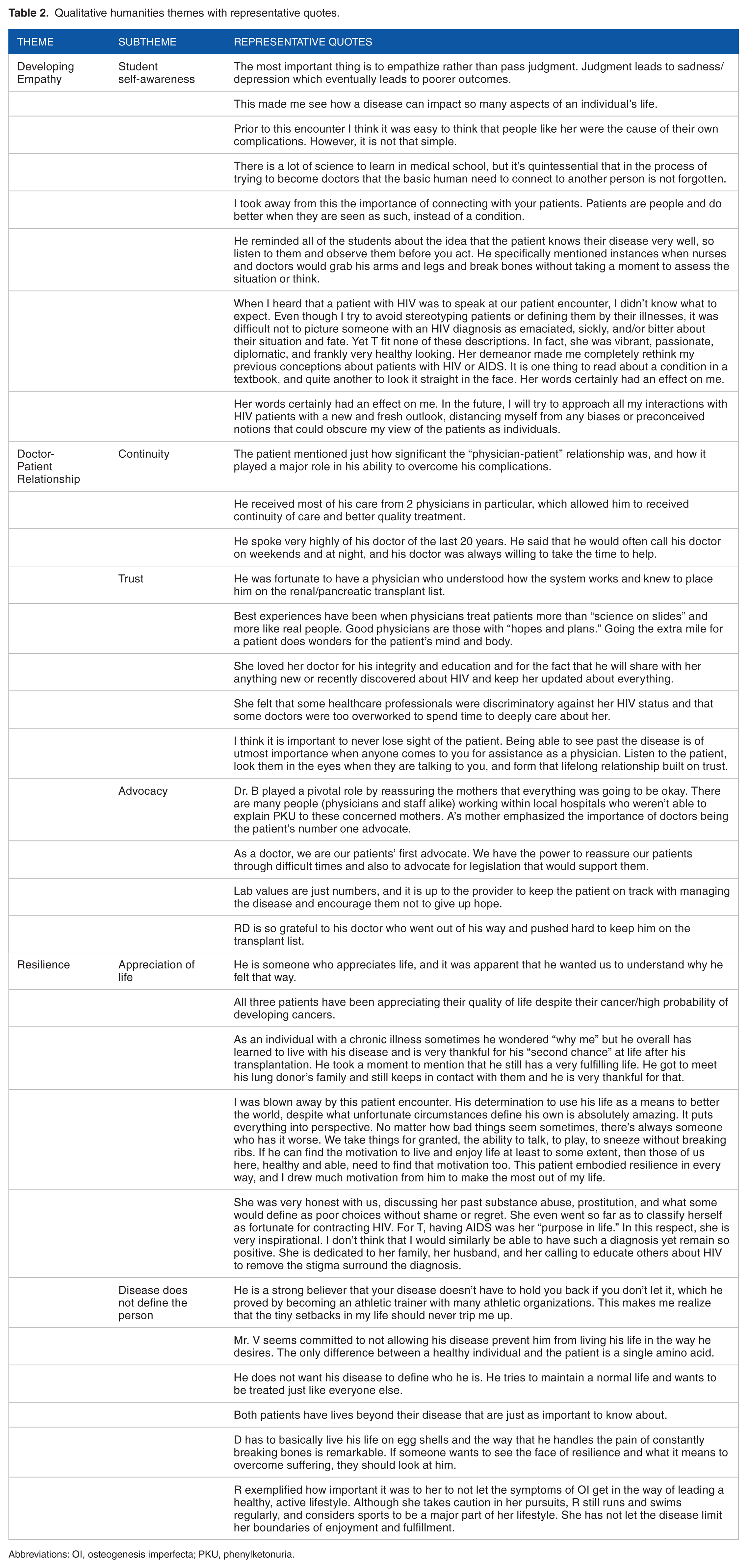
Abbreviations: OI, osteogenesis imperfecta; PKU, phenylketonuria.
Qualitative health system themes with representative quotes.
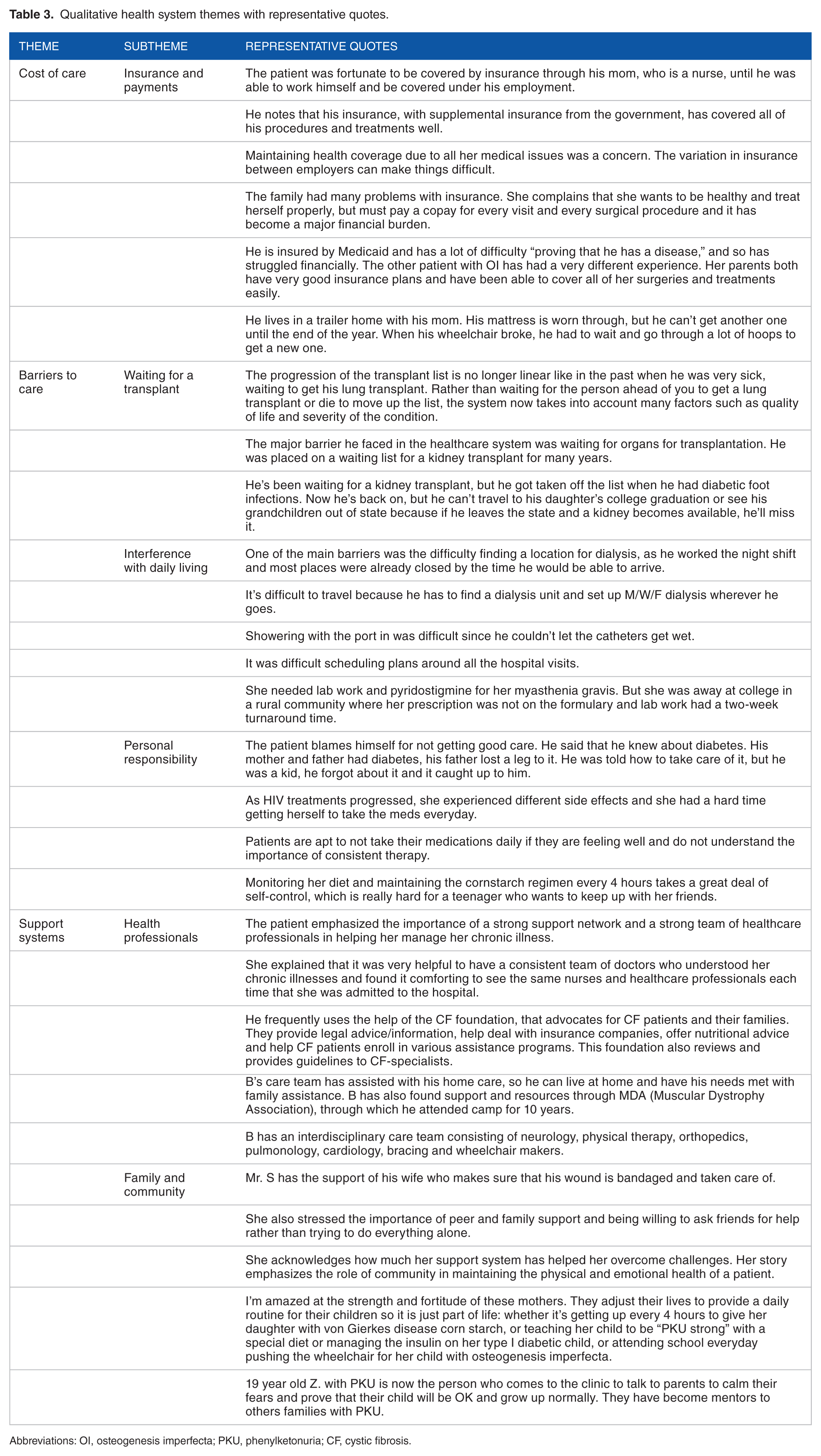
Abbreviations: OI, osteogenesis imperfecta; PKU, phenylketonuria; CF, cystic fibrosis.
The quantitative data revealed that patient + illness script SPM questions were answered significantly more correctly than lecture questions. PBL question results were not significantly different than lecture question results on the SPM exams. Both PBL and patient + illness script NBME questions were answered correctly more often than lecture questions in both the December and June exams. The patient + illness script questions scored better than the PBL questions. As would be expected, the average percent correct for all question categories declined over time. There was a 7% to 16% decrease in all test scores from the December exam to the June exam, 6 months later.
Discussion
John Dewey the father of pragmatist teaching theory believed that “School should be less about preparation for life and more like life itself.”22,23 Although we set out to address 2 objectives, the first: best methods for learning retention and retrieval and the second: integrating humanities and health sciences into a basic science medical school course, we completed this research project with a more complete understanding that these objectives are not separate entities but are one integrated objective. The multiple learning contexts used in the SPM course created a conceptual framework that enhanced abstraction of relevant features, promoted transfer to new situations, and improved retrieval and application of knowledge.
What we found was that each of our learning methods added a new beam of support to our students’ educational scaffolding. Lectures, considered a “banking model” where faculty make deposits that students receive, lay down the foundation of factual knowledge. 24 First-year students, novices to medicine, tend to approach this learning style with memorization and surface level understanding committed to short-term memory, frequently failing to extract the meaning and relevance of the information. Next, we added on the constructivist approach with PBLs, where students are at the center of learning; where they create their own knowledge. With this approach, students explore, investigate, make connections, and collaborate.25,26 What we added, that most medical schools fail to do, is the final beam to complete the scaffolding, metacognition. Through our patient encounters and illness scripts, we discovered that students developed internal conversations reconciling their preconceived notions with new knowledge, connecting and applying knowledge, as John Dewey 23 would say, to “life itself.”
We learned from the free response section of the illness scripts that the human element experienced in the patient encounter created an emotional connection to the subject matter (Tables 1 to 3). We know that emotion stimulates an entire system of cerebral connections involving memory consolidation, memory encoding and formation, and memory retention.27,28 Patients told very personal and often emotional stories to which we saw students empathize with and reflect upon. Adding the illness scripts prompted the students to reflect on and write about the human experience, the medical science and the health systems that led to that experience. But most importantly, the students reflected on how they will approach such an experience as a future physician.
As seen in Table 4, adding on PBL (constructivist learning method) improved test scores especially in the retrieval from long-term memory, compared to lecture based only. Although the literature is mixed regarding specific grade differences between PBL and lecture (ie, students with a PBL-based curriculum do not necessarily score higher on standardized exams compared with students with a lecture-based curriculum), the idea that PBL increases long-term knowledge retention and enhances self-directed learning is well founded.29,30 Adding on the level of metacognition with the patient encounters/illness scripts, we see an even better effect on both short-term and long-term knowledge retrieval. There is currently limited research on live patient encounters with illness scripts and learning retention in basic science classes. Scripts increase clinical reasoning and performance, but their effect on exams is relatively unstudied.3,31 Our results demonstrate that students transferred their learning from the conceptual framework in SPM that included PBL and patient encounters/illness scripts to questions asked on a national standardized test. We believe that this additional layer of emotional-humanistic metacognition focuses the students’ attention to better understand, integrate, store, retrieve, transfer, and apply their learning.
Test scores divided by content: lecture based, PBL based, and patient/illness script based.

Abbreviations: CI, confidence interval; NBME, National Board of Medical Examiners; PBL, problem-based learning; SPM, Scientific Principles of Medicine.
Not only did this added layer of metacognition in our educational framework improve test scores, it was enjoyable. Student feedback was unanimously positive with frequent comments that the patient encounter was their favorite part of SPM and that they looked forward to it every Friday. After moving on from SPM, students inquire, why doesn’t every course have a Friday patient encounter? Students also appreciate that they are not to take notes and that they are to listen and interact. The patient portion of the illness scripts comes from the memory of the event, what they recall, not what they wrote notes about. On class feedback, the most common remark was that the patient encounter made their week of studies relevant to their purpose of becoming a doctor.
Limitations to this study include the differences in quantitative data points. In all exams, there were more lecture-content questions than PBL or patient/illness script content questions. Unfortunately, this limitation was unavoidable since more testable content is packed into 1 hour of lecture than 1 hour of PBL or 1 hour with a patient. Since it is impossible to bring a patient in for every illness studied each week, it is important to find a patient who embodies the essence of the week.
Patients who have taught in our class for a number of years now return with stories about their more recent hospitalizations. These patients feel fulfilled when the team of white coats exits the hospital room but a medical student lingers behind to personally thank the patient for his or her presentation in the SPM class years earlier and inform the patient that he or she is still remembered. Future studies plan to not only analyze if students keep these illness scripts and find them helpful when seeing such patients on clinical rotations or for studying for the board exams years later but also to look at the effects that patient encounters have upon the patients themselves.
In conclusion, this study supports the concept that applying metacognition through the use of patient encounters and illness scripts can be successfully employed in a basic science medical school class. Reflecting upon a patient’s experience not only promotes learning connections and retrieval of knowledge but also enhances integration of clinical medicine, humanities, and health systems into a basic science curriculum.
Footnotes
Acknowledgements
The authors alone are responsible for the content and writing of the article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Eileen F Hennrikus, MD devised and implemented the curricular design. All authors were involved in the analysis and interpretation of the curricular design, and writing and editing the manuscript.